
The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Preoperative Workup and AVF Technique
2.4. AVF Maturation
2.5. Study Outcomes
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Murad, M.H.; Elamin, M.B.; Sidawy, A.N.; Malaga, G.; Rizvi, A.Z.; Flynn, D.N.; Casey, E.T.; McCausland, F.R.; McGrath, M.M.; Vo, D.H.; et al. Autogenous versus Prosthetic Vascular Access for Hemodialysis: A Systematic Review and Meta-Analysis. J. Vasc. Surg. 2008, 48, 34S–47S. [Google Scholar] [CrossRef] [PubMed]
- Almasri, J.; Alsawas, M.; Mainou, M.; Mustafa, R.A.; Wang, Z.; Woo, K.; Cull, D.L.; Murad, M.H. Outcomes of Vascular Access for Hemodialysis: A Systematic Review and Meta-Analysis. J. Vasc. Surg. 2016, 64, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Al-Jaishi, A.A.; Liu, A.R.; Lok, C.E.; Zhang, J.C.; Moist, L.M. Complications of the Arteriovenous Fistula: A Systematic Review. J. Am. Soc. Nephrol. JASN 2017, 28, 1839–1850. [Google Scholar] [CrossRef] [PubMed]
- Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Arbănași, E.M.; Kovács, I.; Horváth, E.; Suciu, B.A.; Hosu, I.; Russu, E. Uncommon Surgical Management by AVF between the Great Saphenous Vein and Anterior Tibial Artery for Old Radiocephalic AVF Failure. Life 2022, 12, 529. [Google Scholar] [CrossRef]
- Russu, E.; Muresan, A.V.; Arbanasi, E.M.; Nedelea, D.; Suciu, B.A.; Arbanasi, E.M.; Kaller, R. Polytetrafluorethylene Prosthesis Interposition in Vascular Access. Mater. Plast. 2022, 59, 1–8. [Google Scholar] [CrossRef]
- Schmidli, J.; Widmer, M.K.; Basile, C.; de Donato, G.; Gallieni, M.; Gibbons, C.P.; Haage, P.; Hamilton, G.; Hedin, U.; Kamper, L.; et al. Editor’s Choice—Vascular Access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2018, 55, 757–818. [Google Scholar] [CrossRef]
- Kopple, J.D. National Kidney Foundation K/DOQI Clinical Practice Guidelines for Nutrition in Chronic Renal Failure. Am. J. Kidney Dis. 2001, 37, S66–S70. [Google Scholar] [CrossRef]
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am. J. Kidney Dis. 2020, 75, S1–S164. [Google Scholar] [CrossRef]
- Woodside, K.J.; Bell, S.; Mukhopadhyay, P.; Repeck, K.J.; Robinson, I.T.; Eckard, A.R.; Dasmunshi, S.; Plattner, B.W.; Pearson, J.; Schaubel, D.E.; et al. Arteriovenous Fistula Maturation in Prevalent Hemodialysis Patients in the United States: A National Study. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2018, 71, 793–801. [Google Scholar] [CrossRef]
- Robbin, M.L.; Greene, T.; Allon, M.; Dember, L.M.; Imrey, P.B.; Cheung, A.K.; Himmelfarb, J.; Huber, T.S.; Kaufman, J.S.; Radeva, M.K.; et al. Prediction of Arteriovenous Fistula Clinical Maturation from Postoperative Ultrasound Measurements: Findings from the Hemodialysis Fistula Maturation Study. J. Am. Soc. Nephrol. 2018, 29, 2735–2744. [Google Scholar] [CrossRef] [Green Version]
- Ravani, P.; Brunori, G.; Mandolfo, S.; Cancarini, G.; Imbasciati, E.; Marcelli, D.; Malberti, F. Cardiovascular Comorbidity and Late Referral Impact Arteriovenous Fistula Survival: A Prospective Multicenter Study. J. Am. Soc. Nephrol. JASN 2004, 15, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Tordoir, J.; Canaud, B.; Haage, P.; Konner, K.; Basci, A.; Fouque, D.; Kooman, J.; Martin-Malo, A.; Pedrini, L.; Pizzarelli, F.; et al. EBPG on Vascular Access. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. -Eur. Ren. Assoc. 2007, 22 (Suppl. S2), ii88–ii117. [Google Scholar] [CrossRef] [PubMed]
- Roubicek, C.; Brunet, P.; Huiart, L.; Thirion, X.; Leonetti, F.; Dussol, B.; Jaber, K.; Andrieu, D.; Ramananarivo, P.; Berland, Y. Timing of Nephrology Referral: Influence on Mortality and Morbidity. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2000, 36, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Avorn, J.; Winkelmayer, W.C.; Bohn, R.L.; Levin, R.; Glynn, R.J.; Levy, E.; Owen, W. Delayed Nephrologist Referral and Inadequate Vascular Access in Patients with Advanced Chronic Kidney Failure. J. Clin. Epidemiol. 2002, 55, 711–716. [Google Scholar] [CrossRef]
- Kaygin, M.A.; Halici, U.; Aydin, A.; Dag, O.; Binici, D.N.; Limandal, H.K.; Arslan, Ü.; Kiymaz, A.; Kahraman, N.; Calik, E.S.; et al. The Relationship between Arteriovenous Fistula Success and Inflammation. Ren. Fail. 2013, 35, 1085–1088. [Google Scholar] [CrossRef]
- Usman, R.; Jamil, M.; Abbassi, H. Association between Raised Serum C-Reactive Protein and Arteriovenous Fistula Failure. J. Islamabad Med. Dent. Coll. 2016, 5, 157–160. [Google Scholar]
- Wongmahisorn, Y. Role of Neutrophil-to-Lymphocyte Ratio as a Prognostic Indicator for Hemodialysis Arteriovenous Fistula Failure. J. Vasc. Access 2019, 20, 608–614. [Google Scholar] [CrossRef]
- Sarioglu, O.; Capar, A.E.; Belet, U. Relationship of Arteriovenous Fistula Stenosis and Thrombosis with the Platelet–Lymphocyte Ratio in Hemodialysis Patients. J. Vasc. Access 2020, 21, 630–635. [Google Scholar] [CrossRef]
- Stirbu, O.; Gadalean, F.; Pitea, I.V.; Ciobanu, G.; Schiller, A.; Grosu, I.; Nes, A.; Bratescu, R.; Olariu, N.; Timar, B.; et al. C-Reactive Protein as a Prognostic Risk Factor for Loss of Arteriovenous Fistula Patency in Hemodialyzed Patients. J. Vasc. Surg. 2019, 70, 208–215. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Mureșan, A.V.; Coșarcă, C.M.; Kaller, R.; Bud, T.I.; Hosu, I.; Voidăzan, S.T.; Arbănași, E.M.; Russu, E. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Impact on Predicting Outcomes in Patients with Acute Limb Ischemia. Life 2022, 12, 822. [Google Scholar] [CrossRef]
- Taurino, M.; Aloisi, F.; Del Porto, F.; Nespola, M.; Dezi, T.; Pranteda, C.; Rizzo, L.; Sirignano, P. Neutrophil-to-Lymphocyte Ratio Could Predict Outcome in Patients Presenting with Acute Limb Ischemia. J. Clin. Med. 2021, 10, 4343. [Google Scholar] [CrossRef] [PubMed]
- Appleton, N.D.; Bailey, D.M.; Morris-Stiff, G.; Lewis, M.H. Neutrophil to Lymphocyte Ratio Predicts Perioperative Mortality Following Open Elective Repair of Abdominal Aortic Aneurysms. Vasc. Endovasc. Surg. 2014, 48, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Ntalouka, M.P.; Nana, P.; Kouvelos, G.N.; Stamoulis, K.; Spanos, K.; Giannoukas, A.; Matsagkas, M.; Arnaoutoglou, E. Association of Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratio with Adverse Events in Endovascular Repair for Abdominal Aortic Aneurysm. J. Clin. Med. 2021, 10, 1083. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liu, H.; Wang, Q.; Cheng, Z.; Sun, S.; Zhang, Y.; Sun, X.; Wang, Z.; Ren, L. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Are Effective Predictors of Prognosis in Patients with Acute Mesenteric Arterial Embolism and Thrombosis. Ann. Vasc. Surg. 2018, 49, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Taşoğlu, I.; Çiçek, O.F.; Lafcı, G.; Kadiroğulları, E.; Sert, D.E.; Demir, A.; Cavus, U.; Colak, N.; Songur, M.; Hodo, B. Usefulness of Neutrophil/Lymphocyte Ratio as a Predictor of Amputation after Embolectomy for Acute Limb Ischemia. Ann. Vasc. Surg. 2014, 28, 606–613. [Google Scholar] [CrossRef]
- Lareyre, F.; Carboni, J.; Chikande, J.; Massiot, N.; Voury-Pons, A.; Umbdenstock, E.; Jean-Baptiste, E.; Hassen-Khodja, R.; Raffort, J. Association of Platelet to Lymphocyte Ratio and Risk of 30-Day Postoperative Complications in Patients Undergoing Abdominal Aortic Surgical Repair. Vasc. Endovasc. Surg. 2019, 53, 5–11. [Google Scholar] [CrossRef]
- Drugescu, A.; Roca, M.; Zota, I.M.; Costache, A.-D.; Gavril, O.I.; Gavril, R.S.; Vasilcu, T.F.; Mitu, O.; Esanu, I.M.; Roca, I.-C.; et al. Value of the Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio in Predicting CPET Performance in Patients with Stable CAD and Recent Elective PCI. Med. Kaunas Lith. 2022, 58, 814. [Google Scholar] [CrossRef]
- Russu, E.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Voidăzan, S.; Arbănași, E.M.; Coșarcă, C.M. The Predictive Role of NLR and PLR in Outcome and Patency of Lower Limb Revascularization in Patients with Femoropopliteal Disease. J. Clin. Med. 2022, 11, 2620. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef]
- Woziwodzka, K.; Dziewierz, A.; Pawica, M.; Panek, A.; Krzanowski, M.; Gołasa, P.; Latacz, P.; Burkat, M.; Kuźniewski, M.; Krzanowska, K. Neutrophil-to-Lymphocyte Ratio Predicts Long-Term All-Cause Mortality in Patients with Chronic Kidney Disease Stage 5. Folia Med. Cracov. 2019, 59, 55–70. [Google Scholar] [CrossRef]
- Kato, S.; Abe, T.; Lindholm, B.; Maruyama, S. Neutrophil/Lymphocyte Ratio: A Promising Prognostic Marker in Patients with Chronic Kidney Disease. Inflamm. Cell Signal. 2015, 2, 132–137. [Google Scholar] [CrossRef]
- Altunoren, O.; Akkus, G.; Sezal, D.T.; Ciftcioglu, M.; Guzel, F.B.; Isiktas, S.; Torun, G.I.; Uyan, M.; Sokmen, M.F.; Sevim, H.A.; et al. Does Neutrophyl to Lymphocyte Ratio Really Predict Chronic Kidney Disease Progression? Int. Urol. Nephrol. 2019, 51, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Solak, Y.; Yilmaz, M.I.; Sonmez, A.; Saglam, M.; Cakir, E.; Unal, H.U.; Gok, M.; Caglar, K.; Oguz, Y.; Yenicesu, M.; et al. Neutrophil to Lymphocyte Ratio Independently Predicts Cardiovascular Events in Patients with Chronic Kidney Disease. Clin. Exp. Nephrol. 2013, 17, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Pan, L.; Yang, M. Preoperative Elevated Neutrophil-to-Lymphocyte Ratio (NLR) and Derived NLR Are Associated with Poor Prognosis in Patients with Breast Cancer. Medicine 2018, 97, e13340. [Google Scholar] [CrossRef]
- Chen, J.-H.; Zhai, E.-T.; Yuan, Y.-J.; Wu, K.-M.; Xu, J.-B.; Peng, J.-J.; Chen, C.-Q.; He, Y.-L.; Cai, S.-R. Systemic Immune-Inflammation Index for Predicting Prognosis of Colorectal Cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef]
- Topkan, E.; Besen, A.A.; Ozdemir, Y.; Kucuk, A.; Mertsoylu, H.; Pehlivan, B.; Selek, U. Prognostic Value of Pretreatment Systemic Immune-Inflammation Index in Glioblastoma Multiforme Patients Undergoing Postneurosurgical Radiotherapy Plus Concurrent and Adjuvant Temozolomide. Mediat. Inflamm. 2020, 2020, 4392189. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Zhang, J.; Xiao, X.; Wu, Y.; Yang, J.; Zou, Y.; Zhao, Y.; Yang, Q.; Liu, F. Prognostic Nutritional Index as a Predictor of Diabetic Nephropathy Progression. Nutrients 2022, 14, 3634. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Hung, S.-C. Geriatric Nutritional Risk Index Is Associated with Unique Health Conditions and Clinical Outcomes in Chronic Kidney Disease Patients. Nutrients 2019, 11, 2769. [Google Scholar] [CrossRef]
- Ruperto, M.; Barril, G. Nutritional Status, Body Composition, and Inflammation Profile in Older Patients with Advanced Chronic Kidney Disease Stage 4–5: A Case-Control Study. Nutrients 2022, 14, 3650. [Google Scholar] [CrossRef]
- Sim, J.H.; Jun, I.-G.; Moon, Y.-J.; Jeon, A.R.; Kim, S.-H.; Kim, B.; Song, J.-G. Association of Preoperative Prognostic Nutritional Index and Postoperative Acute Kidney Injury in Patients Who Underwent Hepatectomy for Hepatocellular Carcinoma. J. Pers. Med. 2021, 11, 428. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.-H.; Bang, J.-Y.; Kim, S.-H.; Kang, S.-J.; Song, J.-G. Association of Preoperative Prognostic Nutritional Index and Postoperative Acute Kidney Injury in Patients with Colorectal Cancer Surgery. Nutrients 2021, 13, 1604. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Roy-Chaudhury, P. Advances and New Frontiers in the Pathophysiology of Venous Neointimal Hyperplasia and Dialysis Access Stenosis. Adv. Chronic Kidney Dis. 2009, 16, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Brahmbhatt, A.; Remuzzi, A.; Franzoni, M.; Misra, S. The Molecular Mechanisms of Hemodialysis Vascular Access Failure. Kidney Int. 2016, 89, 303–316. [Google Scholar] [CrossRef]
- Hu, H.; Patel, S.; Hanisch, J.J.; Santana, J.M.; Hashimoto, T.; Bai, H.; Kudze, T.; Foster, T.R.; Guo, J.; Yatsula, B.; et al. Future Research Directions to Improve Fistula Maturation and Reduce Access Failure. Semin. Vasc. Surg. 2016, 29, 153–171. [Google Scholar] [CrossRef]
- Ahbap, E.; Sakaci, T.; Kara, E.; Sahutoglu, T.; Koc, Y.; Basturk, T.; Sevinc, M.; Akgol, C.; Kayalar, A.O.; Ucar, Z.A.; et al. Neutrophil-to-Lymphocyte Ratio and Platelet-Tolymphocyte Ratio in Evaluation of Inflammation in End-Stage Renal Disease. Clin. Nephrol. 2016, 85, 199–208. [Google Scholar] [CrossRef]
- Turkmen, K.; Erdur, F.M.; Ozcicek, F.; Ozcicek, A.; Akbas, E.M.; Ozbicer, A.; Demirtas, L.; Turk, S.; Tonbul, H.Z. Platelet-to-Lymphocyte Ratio Better Predicts Inflammation than Neutrophil-to-Lymphocyte Ratio in End-Stage Renal Disease Patients. Hemodial. Int. 2013, 17, 391–396. [Google Scholar] [CrossRef]
- Li, P.; Xia, C.; Liu, P.; Peng, Z.; Huang, H.; Wu, J.; He, Z. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Evaluation of Inflammation in Non-Dialysis Patients with End-Stage Renal Disease (ESRD). BMC Nephrol. 2020, 21, 511. [Google Scholar] [CrossRef]
- Yaprak, M.; Turan, M.N.; Dayanan, R.; Akın, S.; Değirmen, E.; Yıldırım, M.; Turgut, F. Platelet-to-Lymphocyte Ratio Predicts Mortality Better than Neutrophil-to-Lymphocyte Ratio in Hemodialysis Patients. Int. Urol. Nephrol. 2016, 48, 1343–1348. [Google Scholar] [CrossRef]
- Zhu, F.; Yao, Y.; Ci, H.; Shawuti, A. Predictive Value of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio for Primary Patency of Percutaneous Transluminal Angioplasty in Hemodialysis Arteriovenous Fistula Stenosis. Vascular 2021, 17085381211039672. [Google Scholar] [CrossRef]
- Umeres-Francia1, G.; Rojas-Fernández, M.; Añazco, P.H.; Benites-Zapata, V. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as a Risk Factor for Mortality in Peruvian Adults with Chronic Kidney Disease. Ren. Replace. Ther. 2021, 8, 30. [Google Scholar] [CrossRef]
- Duan, S.; Sun, L.; Zhang, C.; Wu, L.; Nie, G.; Huang, Z.; Xing, C.; Zhang, B.; Yuan, Y. Association of Platelet-to-Lymphocyte Ratio with Kidney Clinicopathologic Features and Renal Outcomes in Patients with Diabetic Kidney Disease. Int. Immunopharmacol. 2021, 93, 107413. [Google Scholar] [CrossRef]
- Brito, G.M.C.; Fontenele, A.M.M.; Carneiro, E.C.R.L.; Nogueira, I.A.L.; Cavalcante, T.B.; Vale, A.A.M.; Monteiro, S.C.M.; Salgado Filho, N. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in Nondialysis Chronic Kidney Patients. Int. J. Inflamm. 2021, 2021, e6678960. [Google Scholar] [CrossRef] [PubMed]
- Catabay, C.; Obi, Y.; Streja, E.; Soohoo, M.; Park, C.; Rhee, C.M.; Kovesdy, C.P.; Hamano, T.; Kalantar-Zadeh, K. Lymphocyte Cell Ratios and Mortality among Incident Hemodialysis Patients. Am. J. Nephrol. 2017, 46, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Yoshitomi, R.; Nakayama, M.; Sakoh, T.; Fukui, A.; Katafuchi, E.; Seki, M.; Tsuda, S.; Nakano, T.; Tsuruya, K.; Kitazono, T. High Neutrophil/Lymphocyte Ratio Is Associated with Poor Renal Outcomes in Japanese Patients with Chronic Kidney Disease. Ren. Fail. 2019, 41, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Neuen, B.L.; Leather, N.; Greenwood, A.M.; Gunnarsson, R.; Cho, Y.; Mantha, M.L. Neutrophil–Lymphocyte Ratio Predicts Cardiovascular and All-Cause Mortality in Hemodialysis Patients. Ren. Fail. 2016, 38, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Wang, S.; Zhang, G.; Xiong, R.; Li, H. High Neutrophil-to-Lymphocyte Ratio Is a Significant Predictor of Cardiovascular and All-Cause Mortality in Patients Undergoing Peritoneal Dialysis. Kidney Blood Press. Res. 2018, 43, 490–499. [Google Scholar] [CrossRef]
- Zhang, L.; Nie, Y.; Guo, M.; Wang, L.; Shi, Y.; Jiang, X.; Ding, X.; Xu, X.; Ji, J. Neutrophil to Lymphocyte Ratio as a Predictor of Long-Term Outcome in Peritoneal Dialysis Patients: A 5-Year Cohort Study. Blood Purif. 2021, 50, 772–778. [Google Scholar] [CrossRef]
- Erdem, E.; Kaya, C.; Karataş, A.; Dilek, M.; Akpolat, T. Neutrophil to Lymphocyte Ratio in Predicting Short-Term Mortality in Hemodialysis Patients. J. Exp. Clin. Med. 2013, 30, 129–132. [Google Scholar] [CrossRef]
- An, X.; Mao, H.-P.; Wei, X.; Chen, J.-H.; Yang, X.; Li, Z.-B.; Yu, X.-Q.; Li, Z.-J. Elevated Neutrophil to Lymphocyte Ratio Predicts Overall and Cardiovascular Mortality in Maintenance Peritoneal Dialysis Patients. Int. Urol. Nephrol. 2012, 44, 1521–1528. [Google Scholar] [CrossRef]
- Zhu, X.; Li, G.; Li, S.; Gong, Z.; Liu, J.; Song, S. Neutrophil-to-lymphocyte Ratio and Red Blood Cell Distribution Width-to-platelet Ratio Predict Cardiovascular Events in Hemodialysis Patients. Exp. Ther. Med. 2020, 20, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Kordzadeh, A.; Chung, J.; Panayiotopoulos, Y.P. Cephalic Vein and Radial Artery Diameter in Formation of Radiocephalic Arteriovenous Fistula: A Systematic Review. J. Vasc. Access 2015, 16, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.R.; Farber, M.A.; Marston, W.A.; Dinwiddie, L.C.; Keagy, B.A.; Burnham, S.J. Prediction of Wrist Arteriovenous Fistula Maturation with Preoperative Vein Mapping with Ultrasonography. J. Vasc. Surg. 2002, 36, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Parmar, J.; Aslam, M.; Standfield, N. Pre-Operative Radial Arterial Diameter Predicts Early Failure of Arteriovenous Fistula (AVF) for Haemodialysis. Eur. J. Vasc. Endovasc. Surg. 2007, 33, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.; Ward, R.; Taylor, J.; Selvakumar, S.; How, T.V.; Bakran, A. Factors Associated with Early Failure of Arteriovenous Fistulae for Haemodialysis Access. Eur. J. Vasc. Endovasc. Surg. 1996, 12, 207–213. [Google Scholar] [CrossRef]
- Wilmink, T.; Corte-Real Houlihan, M. Diameter Criteria Have Limited Value for Prediction of Functional Dialysis Use of Arteriovenous Fistulas. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 572–581. [Google Scholar] [CrossRef]
- Khavanin Zadeh, M.; Gholipour, F.; Naderpour, Z.; Porfakharan, M. Relationship between Vessel Diameter and Time to Maturation of Arteriovenous Fistula for Hemodialysis Access. Int. J. Nephrol. 2012, 2012, 942950. [Google Scholar] [CrossRef]
- Barutcu Atas, D.; Tugcu, M.; Asicioglu, E.; Velioglu, A.; Arikan, H.; Koc, M.; Tuglular, S. Prognostic Nutritional Index Is a Predictor of Mortality in Elderly Patients with Chronic Kidney Disease. Int. Urol. Nephrol. 2022, 54, 1155–1162. [Google Scholar] [CrossRef]
- Wada, H.; Dohi, T.; Miyauchi, K.; Jun, S.; Endo, H.; Doi, S.; Konishi, H.; Naito, R.; Tsuboi, S.; Ogita, M.; et al. Relationship between the Prognostic Nutritional Index and Long-Term Clinical Outcomes in Patients with Stable Coronary Artery Disease. J. Cardiol. 2018, 72, 155–161. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients n = 125 | Maturation n = 88 | Non-Maturation n = 37 | p-Value (OR; CI 95%) |
|---|---|---|---|---|
| Mean age ± SD (min–max) | 61.64 ± 13.81 (21–84) | 60.32 ± 14.82 (21–84) | 64.75 ± 10.58 (37–84) | 0.03 |
| Male sex no. (%) | 76 (60.80%) | 55 (62.5%) | 21 (56.76%) | 0.54 (0.78; 0.36–1.71) |
| Comorbidities and Risk Factors | ||||
| AH, no. (%) | 102 (81.6%) | 71 (80.68%) | 31 (83.78%) | 0.68 (1.23; 0.44–3.43) |
| AF, no. (%) | 34 (27.2%) | 22 (25%) | 12 (32.43%) | 0.39 (1.44; 0.62–3.33) |
| CHF, no. (%) | 47 (37.6%) | 24 (27.27%) | 23 (62.16%) | 0.0004 (4.38; 1.94–9.88) |
| IHD, no. (%) | 83 (66.4%) | 55 (62.5%) | 28 (75.68%) | 0.15 (1.86; 0.78–4.43) |
| MI, no. (%) | 55 (44%) | 36 (40.91%) | 19 (51.35%) | 0.28 (1.52; 0.70–3.30) |
| T2D, no. (%) | 52 (41.6%) | 26 (29.55%) | 26 (70.27%) | 0.0001 (5.63; 2.43–13.06) |
| CVA, no. (%) | 40 (32%) | 25 (28.41%) | 15 (40.54%) | 0.18 (1.78; 0.76–3.83) |
| PAD, no. (%) | 32 (25.6%) | 20 (22.73%) | 12 (32.43%) | 0.25 (1.63; 0.69–3.81) |
| Tobacco, no. (%) | 43 (34.4%) | 27 (30.68%) | 16 (43.24%) | 0.11 (1.90; 0.85–4.25) |
| Obesity, no. (%) | 27 (21.6%) | 21 (23.86%) | 6 (16.22%) | 0.34 (0.61; 0.22–1.68) |
| Laboratory Data | ||||
| Hemoglobin g/dL, median [Q1–Q3] | 13.79 [12.89–14.97] | 13.88 [12.89–14.97] | 13.67 [12.5–14.6] | 0.23 |
| Hematocrit %, median [Q1–Q3] | 42.11 [39.1–45] | 42.45 [39.11–45.21] | 41.43 [37–44.5] | 0.13 |
| Neutrophils × 103/µL, median [Q1–Q3] | 5.43 [3.92–7.04] | 4.9 [3.74–6.5] | 6.56 [5.43–8.66] | <0.0001 |
| Lymphocytes × 103/µL, median [Q1–Q3] | 1.38 [1.05–1.89] | 1.56 [1.12–2.07] | 1.07 [0.88–1.3] | <0.0001 |
| Monocyte × 103/µL, median [Q1–Q3] | 0.66 [0.51–0.95] | 0.66 [0.55–0.92] | 0.69 [0.45–0.97] | 0.44 |
| PLT × 103/µL, median [Q1–Q3] | 219 [170–270] | 212.5 [166.5–272.5] | 227 [173–265] | 0.21 |
| Glucose mg/dL, median [Q1–Q3] | 107 [91.9–143.5] | 102.85 [91.57–144.95] | 110 [92.9–134] | 0.32 |
| Cholesterol mg/dL, median [Q1–Q3] | 171.8 [145.4–214.9] | 170.8 [143.9–219.45] | 187.2 [154–208.4] | 0.32 |
| Triglyceride mg/dL, median [Q1–Q3] | 117.6 [87.3–159.6] | 121.1 [88.87–165] | 107 [84.1–137.1] | 0.21 |
| GFR (mL/min/1.73 m2), median [Q1–Q3] | 10.19 [5.88–21.59] | 11.16 [5.94–20.03] | 9.25 [5.26–21.81] | 0.29 |
| Serum albumin mg/dL, median [Q1–Q3] | 3.57 [3.13–3.96] | 3.78 [3.45–4.1] | 2.93 [2.63–3.21] | <0.0001 |
| Serum calcium mg/dL, median [Q1–Q3] | 8.62 [7.89–9.26] | 8.86 [8.22–9.50] | 7.90 [6.77–8.82] | <0.0001 |
| Serum phosphorous mg/dL, median [Q1–Q3] | 4.76 [3.32–5.74] | 3.80 [3.18–5.06] | 6.74 [5.77–7.83] | <0.0001 |
| PNI, median [Q1–Q3] | 43.10 [37–46.85] | 46.25 [41.78–49.55] | 34.55 [32.3–37.2] | <0.0001 |
| Ca-P product, median [Q1–Q3] | 39.34 [29.32–50.66] | 32.51 [27.30–42.93] | 51.48 [48.16–59.55] | <0.0001 |
| CRP mg/dL, median [Q1–Q3] | 2.02 [1.85–2.15] | 1.97 [1.83–2.05] | 2.15 [2.12–2.17] | <0.0001 |
| NLR, median [Q1–Q3] | 3.58 [2.41–5.67] | 2.86 [2.2–4.34] | 5.9 [5.31–8.18] | <0.0001 |
| PLR, median [Q1–Q3] | 140.59 [107.4–208.39] | 129.96 [103.17–174.17] | 208.39 [139.8–269.79] | <0.0001 |
| SII, median [Q1–Q3] | 823.59 [436.91–1277.02] | 641.99 [410.26–999.93] | 1294.63 [963.3–1907.42] | <0.0001 |
| Type of AVF | ||||
| RC-AVF, no. (%) | 64 (51.2%) | 47 (53.41%) | 17 (45.95%) | 0.44 (0.74; 0.34–1.60) |
| Radial artery diameter, median [Q1–Q3] | 2.4 [2.08–3] | 2.8 [2.3–3.25] | 2.05 [1.9–2.2] | <0.0001 |
| Cephalic vein diameter, median [Q1–Q3] | 2.8 [2.1–4.22] | 3.3 [2.5–4.6] | 2.1 [1.9–2.3] | <0.0001 |
| BC-AVF, no. (%) | 61 (48.8%) | 41 (46.59%) | 20 (54.05%) | 0.44 (1.34; 0.62–2.91) |
| Brachial artery diameter, median [Q1–Q3] | 3.5 [2.5–4.5] | 3.8 [3.1–5] | 2.5 [2.32–2.67] | <0.0001 |
| Cephalic vein diameter, median [Q1–Q3] | 3.4 [2.1–5.8] | 4.2 [3.4–6.5] | 2.1 [1.8–2.32] | <0.0001 |
| Outcomes | ||||
| Early thrombosis, no. (%) | 22 (17.6%) | - | 22 (43.24%) | 0.0001 |
| Mortality, no. (%) | 10 (8.0%) | 3 (3.41%) | 7 (18.92%) | 0.008 (6.61; 1.60–27.21) |
| Outcome | All Patients n = 125 | RC-AVF n = 64 | BC-AVF n = 61 | p-Value |
|---|---|---|---|---|
| Six-week maturation, no. (%) | 88 (70.4%) | 47 (73.43%) | 41 (67.21%) | 0.44 |
| Early thrombosis, no. (%) | 22 (17.6%) | 9 (14.06%) | 13 (61.31%) | 0.29 |
| Mortality, no. (%) | 10 (8%) | 4 (6.25%) | 6 (9.83%) | 0.46 |
| Overall maturation, no. (%) | 109 (87.2%) | 51 (79.68%) | 58 (95.08%) | 0.01 |
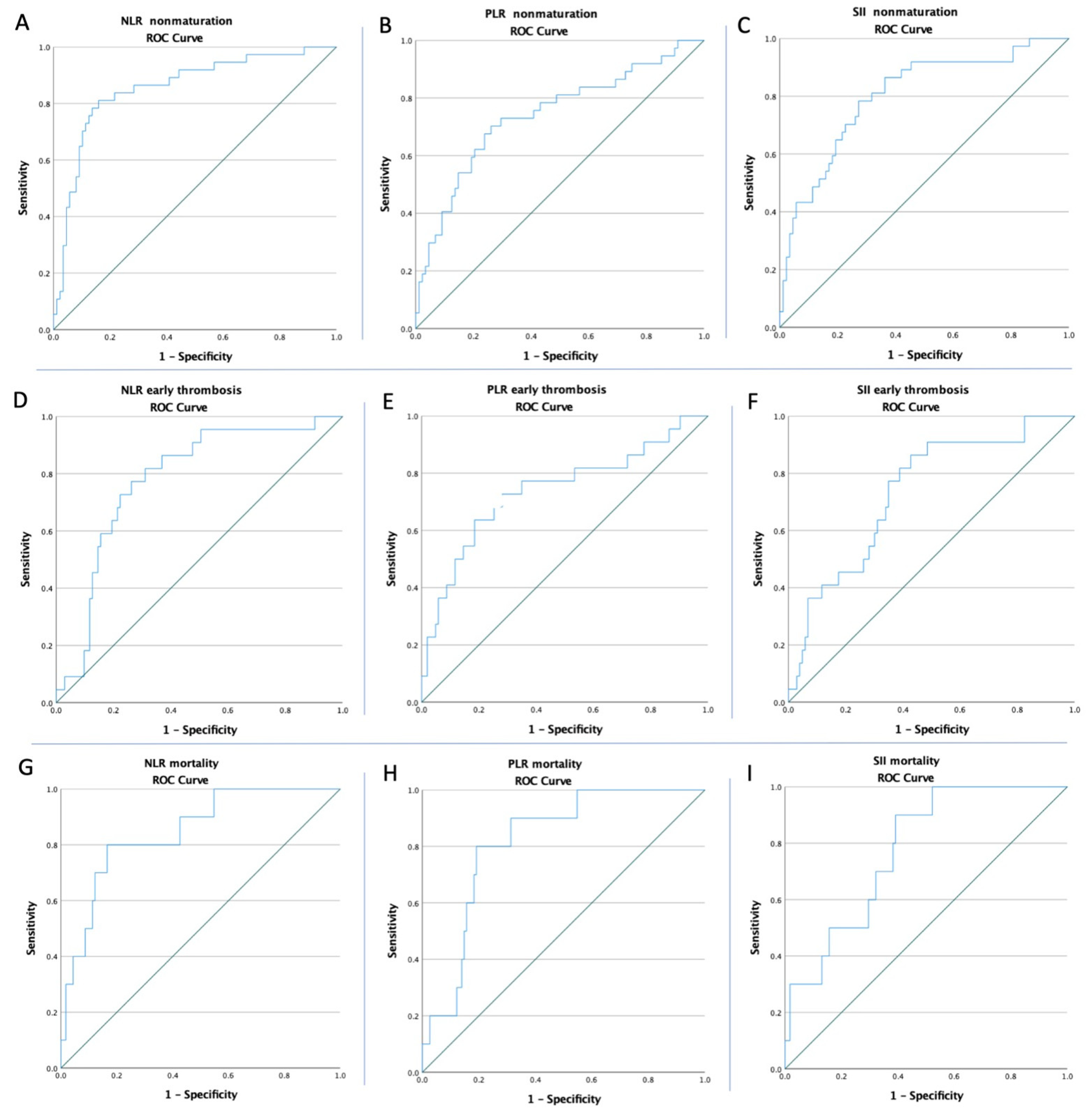
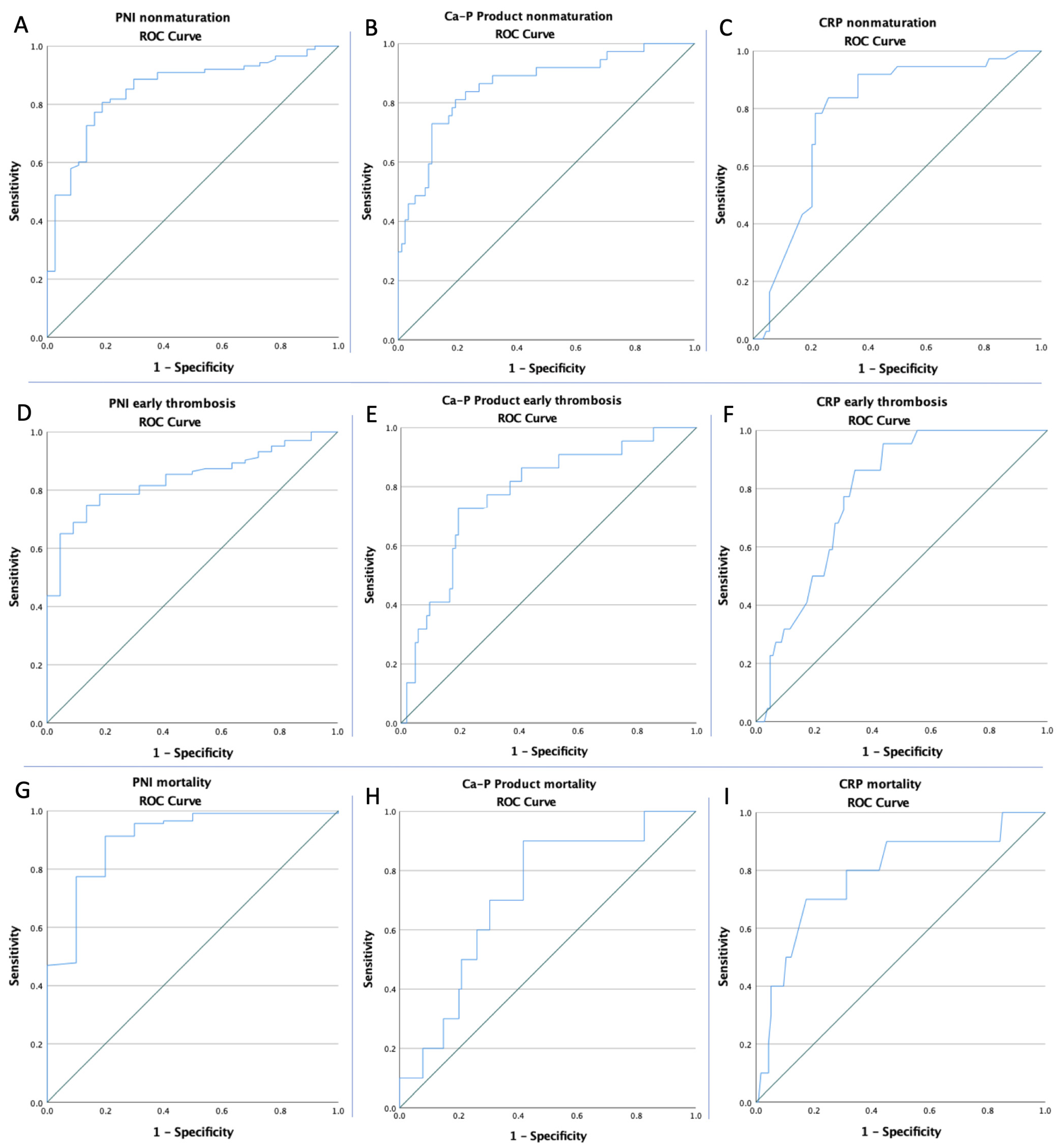
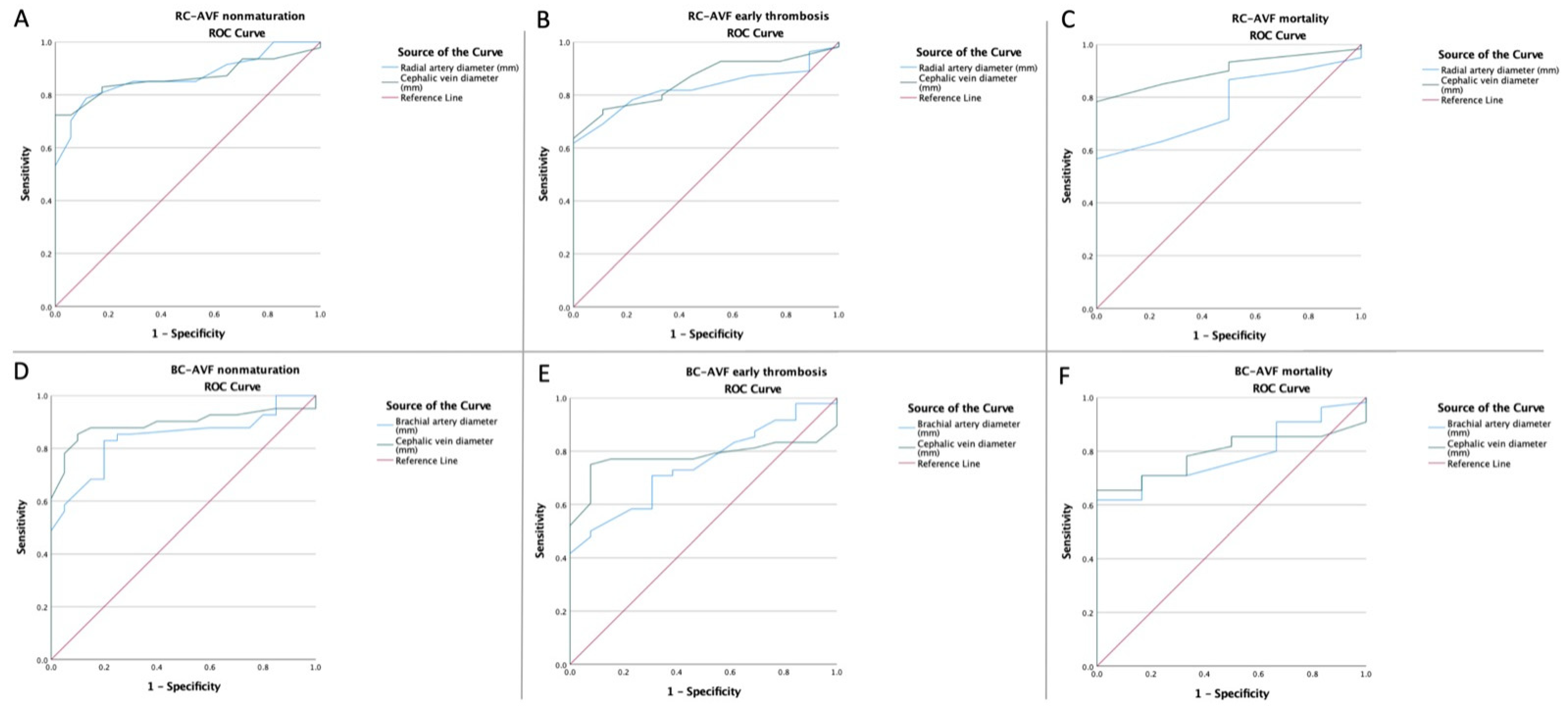
| Variables | Cut-Off | AUC | Std. Error | 95% CI | Sensitivity | Specificity | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Non-Maturation | ||||||||
| NLR | 4.90 | 0.856 | 0.039 | 0.780–0.932 | 81.1% | 84.1% | <0.0001 | |
| PLR | 172.29 | 0.740 | 0.051 | 0.639–0.841 | 70.3% | 73.9% | <0.0001 | |
| SII | 954.54 | 0.802 | 0.044 | 0.716–0.888 | 78.4% | 72.7% | <0.0001 | |
| PNI | 40.59 | 0.852 | 0.036 | 0.780–0.923 | 80.7% | 81.1% | <0.0001 | |
| Ca-P product | 47.36 | 0.859 | 0.038 | 0.784–0.934 | 81.1% | 80.7% | <0.0001 | |
| CRP | 2.07 | 0.785 | 0.043 | 0.700–0.871 | 83.8% | 73.9% | <0.0001 | |
| RC-AVF | RA diameter | 2.25 | 0.869 | 0.044 | 0.783–0.956 | 78.7% | 88.2% | <0.0001 |
| CV diameter | 2.55 | 0.866 | 0.044 | 0.779–0.953 | 72.3% | 99.05% | <0.0001 | |
| BC-AVF | BA diameter | 2.95 | 0.841 | 0.050 | 0.742–0.940 | 82.9% | 80% | <0.0001 |
| CV diameter | 2.70 | 0.894 | 0.043 | 0.810–0.978 | 85.4% | 90% | <0.0001 | |
| Early Thrombosis | ||||||||
| NLR | 4.90 | 0.780 | 0.050 | 0.681–0.878 | 77.3% | 73.8% | <0.0001 | |
| PLR | 181.72 | 0.739 | 0.066 | 0.611–0.868 | 72.7% | 71.8% | <0.0001 | |
| SII | 859.22 | 0.736 | 0.056 | 0.626–0.845 | 81.8% | 61.2% | 0.001 | |
| PNI | 38.65 | 0.839 | 0.038 | 0.766–0.913 | 78.6% | 81.8% | <0.0001 | |
| Ca-P product | 49.67 | 0.777 | 0.054 | 0.671–0.883 | 72.7% | 80.6% | <0.0001 | |
| CRP | 2.07 | 0.785 | 0.042 | 0.702–0.869 | 86.4% | 66% | <0.0001 | |
| RC-AVF | RA diameter | 2.35 | 0.826 | 0.052 | 0.725–0.927 | 61.8% | 100% | 0.002 |
| CV diameter | 2.35 | 0.857 | 0.049 | 0.761–0.952 | 74.5% | 88.9% | 0.001 | |
| BC-AVF | BA diameter | 2.95 | 0.784 | 0.065 | 0.621–0.876 | 70.8% | 69.2% | 0.006 |
| CV diameter | 2.70 | 0.780 | 0.058 | 0.667–0.894 | 75% | 99.3% | 0.002 | |
| Mortality | ||||||||
| NLR | 5.83 | 0.846 | 0.059 | 0.730–0.962 | 80% | 83.5% | <0.0001 | |
| PLR | 212.89 | 0.817 | 0.053 | 0.713–0.922 | 80% | 80.9% | 0.001 | |
| SII | 949.71 | 0.777 | 0.061 | 0.656–0.897 | 90% | 60.9% | 0.004 | |
| PNI | 33.20 | 0.904 | 0.052 | 0.803–1.000 | 91.3% | 80% | 0.01 | |
| Ca-P product | 41.36 | 0.714 | 0.075 | 0.566–0.862 | 90% | 58.3% | 0.02 | |
| CRP | 2.15 | 0.785 | 0.081 | 0.626–0.943 | 70% | 82.6% | 0.001 | |
| RC-AVF | RA diameter | 2.35 | 0.771 | 0.071 | 0.611–0.931 | 56.7% | 100% | 0.07 |
| CV diameter | 2.15 | 0.902 | 0.044 | 0.815–0.989 | 78.3% | 100% | 0.007 | |
| BC-AVF | BA diameter | 2.70 | 0.786 | 0.066 | 0.656–0.917 | 70.9% | 83.3% | 0.02 |
| CV diameter | 2.45 | 0.792 | 0.059 | 0.677–0.907 | 70.9% | 83.3% | 0.01 | |
| Non-Maturation | Early Thrombosis | Mortality | |
|---|---|---|---|
| Low NLR vs. high NLR | 74/81 (91.36%) vs. 14/44 (31.88%) p < 0.0001 OR: 22.65 CI: (8.32–61.67) | 5/81 (6.17%) vs. 17/44 (38.64%) p < 0.0001 OR: 9.57 CI: (3.21–28.45) | 2/97 (2.06%) vs. 8/28 (28.57%) p = 0.0004 OR: 19 CI: (3.74–96.27) |
| Low PLR vs. high PLR | 65/76 (85.55%) vs. 23/49 (46.94%) p < 0.0001 OR: 9.66 CI: (3.88–24.07) | 6/80 (7.50%) vs. 16/45 (35.55%) p = 0.0003 OR: 6.80 CI: (2.42–19.09) | 2/95 (2.10%) vs. 8/30 (26.67%) p = 0.0006 OR: 16.90 CI: (3.35–85.24) |
| Low SII vs. high SII | 64/72 (88.89%) vs. 24/53 (44.28%) p < 0.0001 OR: 9.66 CI: (3.88–24.07) | 4/67 (5.97%) vs. 18/58 (31.03%) p = 0.0009 OR: 7.08 CI: (2.23–22.46) | 1/71 (1.40%) vs. 9/54 (16.67%) p = 0.01 OR: 14.0 CI: (1.71–114.29) |
| Low PNI vs. high PNI | 16/46 (34.78%) vs. 72/79 (91.14%) p < 0.0001 OR: 0.05 CI: (0.01–0.13) | 15/40 (37.50%) vs. 7/85 (8.23%) p = 0.0002 OR: 0.14 CI: (0.05–0.40) | 8/19 (42.11%) vs. 2/106 (1.89%) p < 0.0001 OR: 0.02 CI: (0.005–0.14) |
| Low Ca-P product vs. High Ca-P product | 69/78 (88.46%) vs. 19/47 (40.43%) p < 0.0001 OR: 11.29 CI: (4.56–27.97) | 6/89 (6.74%) vs. 16/36 (44.44%) p < 0.0001 OR: 11.06 CI: (3.84–31.86) | 1/69 (1.47%) vs. 9/57 (15.79%) p = 0.01 OR: 12.75 CI: (1.56–103.99) |
| Low CRP vs. high CRP | 63/71 (88.73%) vs. 25/54 (46.30%) p < 0.0001 OR: 9.13 CI: (3.67–22.68) | 3/71 (4.23%) vs. 19/54 (35.19%) p = 0.0001 OR: 12.30 CI: (3.40–44.43) | 3/94 (3.19%) vs. 7/31 (22.58%) p = 0.002 OR: 8.84 CI: (2.12–36.79) |
| RC-AVF | Non-Maturation | Early Thrombosis | Mortality |
| Low RA diameter vs. high RA diameter | 10/25 (40%) vs. 37/39 (94.87%) p = 0.0009 OR: 14.6 CI: (3.02–70.60) | 8/30 (26.67%) vs. 1/34 (2.94%) p = 0.02 OR: 0.08 CI: (0.009–0.71) | 4/30 (13.33%) vs. 0/34 (0%) p = 0.10 OR: 0.08 CI: (0.004–1.65) |
| Low CV diameter vs. high CV diameter | 13/29 (44.82%) vs. 34/35 (97.14%) p = 0.0001 OR: 27.75 CI: (5.42–141.98) | 8/22 (36.36%) vs. 1/42 (2.38%) p = 0.004 OR: 0.04 CI: (0.004–0.37) | 4/17 (23.52%) vs. 0/47 (0%) p = 0.02 OR: 0.03 CI: (0.001–0.62) |
| BC-AVF | Non-Maturation | Early Thrombosis | Mortality |
| Low BA diameter vs. high BA diameter | 7/23 (30.43%) vs. 34/38 (89.47%) p < 0.0001 OR: 19.42 CI: (4.96–76.05) | 9/23 (39.13%) vs. 4/38 (10.52%) p = 0.01 OR: 0.18 CI: (0.04–0.69) | 5/21 (23.80%) vs. 1/40 (2.50%) p = 0.02 OR: 0.08 CI: (0.008–0.75) |
| Low CV diameter vs. high CV diameter | 6/24 (40%) vs. 35/37 (94.59%) p < 0.0001 OR: 52.5 CI: (9.60–286.89) | 11/24 (45.83%) vs. 3/37 (8.10%) p = 0.001 OR: 0.10 CI: (0.02–0.43) | 5/21 (23.80%) vs. 1/40 (2.50%) p = 0.02 OR: 0.08 CI: (0.008–0.75) |
| Non-Maturation | Early Thrombosis | Mortality | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | ||
| CHF | 4.38 | 3.88–24.07 | <0.001 | 3.71 | 1.41–9.71 | 0.008 | 1.11 | 0.29–4.18 | 0.87 | |
| MI | 1.52 | 0.70–3.30 | 0.28 | 1.67 | 0.66–4.22 | 0.27 | 1.30 | 0.35–4.73 | 0.69 | |
| T2D | 5.63 | 2.43–13.06 | <0.001 | 3.82 | 1.43–10.21 | 0.008 | 0.93 | 0.24–3.47 | 0.91 | |
| Tobacco | 1.72 | 0.77–3.80 | 0.17 | 1.45 | 0.54–3.61 | 0.48 | 0.45 | 0.09–2.22 | 0.32 | |
| RC-AVF | High RA diameter | 0.03 | 0.007–0.18 | <0.001 | 0.05 | 0.006–0.48 | 0.009 | 0.19 | 0.01–1.97 | 0.16 |
| High CV diameter | 0.02 | 0.003–0.19 | <0.001 | 0.04 | 0.005–0.37 | 0.004 | 0.04 | 0.009–0.75 | 0.04 | |
| BC-AVF | High BA diameter | 0.05 | 0.01–0.20 | <0.001 | 0.18 | 0.04–0.69 | 0.01 | 0.08 | 0.009–0.75 | 0.02 |
| High CV diameter | 0.01 | 0.003–0.10 | <0.001 | 0.02 | 0.003–0.23 | 0.001 | 0.08 | 0.009–0.75 | 0.02 | |
| High NLR | 22.65 | 8.32–61.67 | <0.001 | 9.57 | 3.21–28.45 | <0.001 | 19.0 | 3.75–96.27 | <0.001 | |
| High PLR | 6.68 | 2.85–15.63 | <0.001 | 6.80 | 2.42–19.09 | <0.001 | 16.90 | 3.35–85.24 | <0.001 | |
| High SII | 9.66 | 3.88–24.07 | <0.001 | 7.08 | 2.23–22.46 | <0.001 | 14.0 | 1.71–114.28 | 0.01 | |
| High PNI | 0.05 | 0.02–0.14 | <0.001 | 0.15 | 0.05–0.40 | <0.001 | 0.02 | 0.005–0.14 | <0.001 | |
| High Ca-P Product | 17.89 | 6.73–47.60 | <0.001 | 11.06 | 3.84–31.86 | <0.001 | 12.56 | 1.54–102.48 | 0.01 | |
| High CRP | 14.60 | 5.39–39.49 | <0.001 | 12.30 | 3.40–44.43 | <0.001 | 8.84 | 2.12–36.79 | 0.003 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; Voidăzan, S.; Arbănași, E.M.; Horváth, E.; Suciu, B.A.; Hosu, I.; Halmaciu, I.; Brinzaniuc, K.; et al. The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure. Life 2022, 12, 1447. https://doi.org/10.3390/life12091447
Kaller R, Arbănași EM, Mureșan AV, Voidăzan S, Arbănași EM, Horváth E, Suciu BA, Hosu I, Halmaciu I, Brinzaniuc K, et al. The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure. Life. 2022; 12(9):1447. https://doi.org/10.3390/life12091447
Chicago/Turabian StyleKaller, Réka, Emil Marian Arbănași, Adrian Vasile Mureșan, Septimiu Voidăzan, Eliza Mihaela Arbănași, Emőke Horváth, Bogdan Andrei Suciu, Ioan Hosu, Ioana Halmaciu, Klara Brinzaniuc, and et al. 2022. "The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure" Life 12, no. 9: 1447. https://doi.org/10.3390/life12091447