

Urinary Collectrin (TMEM27) as Novel Marker for Acute Kidney Injury
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods and Patients
2.1. Study Design
2.2. Study Population
2.3. ELISA Testing
2.4. Data Processing and Statistical Analyses
3. Results
3.1. Study Population
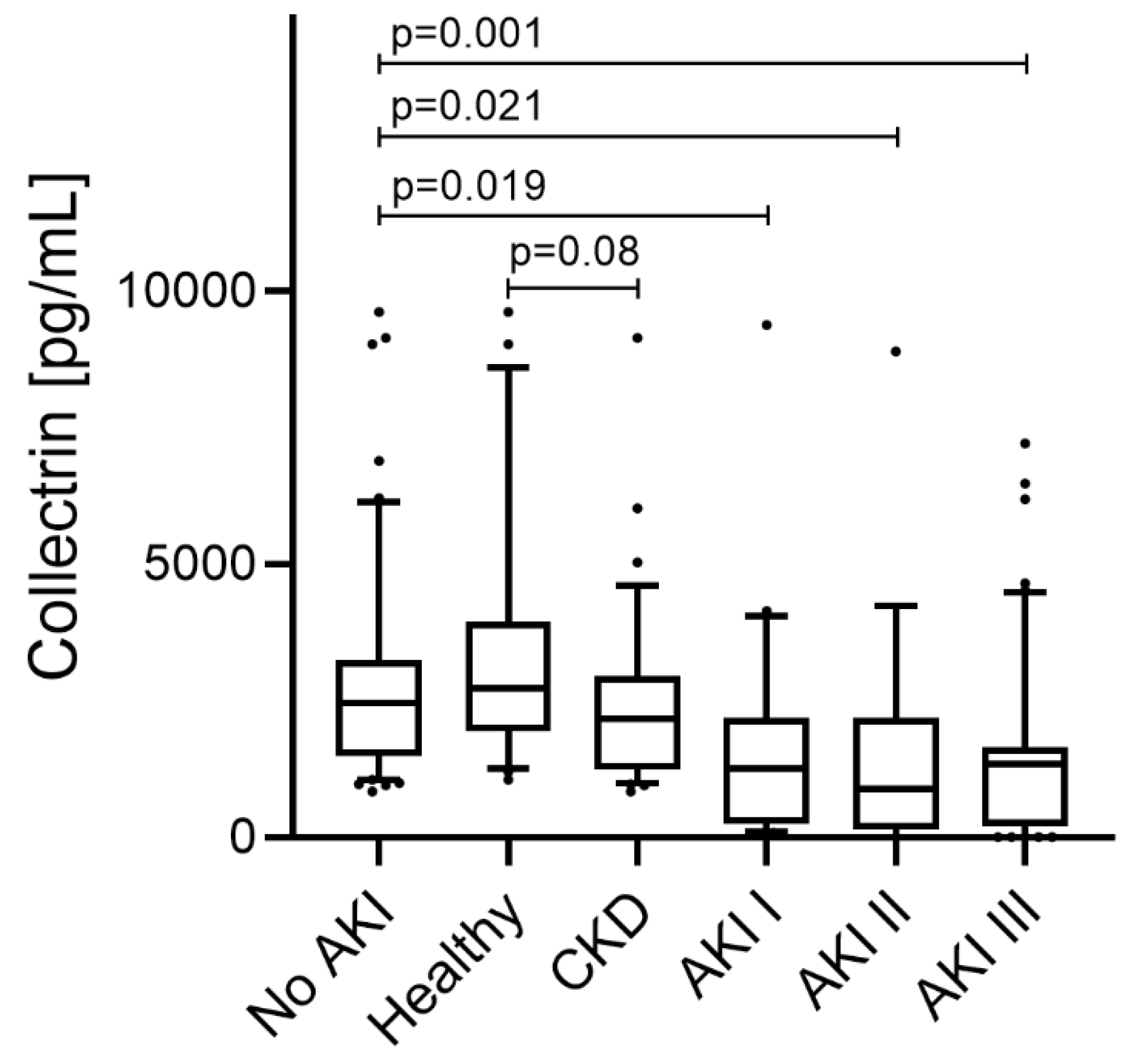
3.2. Urinary Collectrin Values Depending on Kidney Function
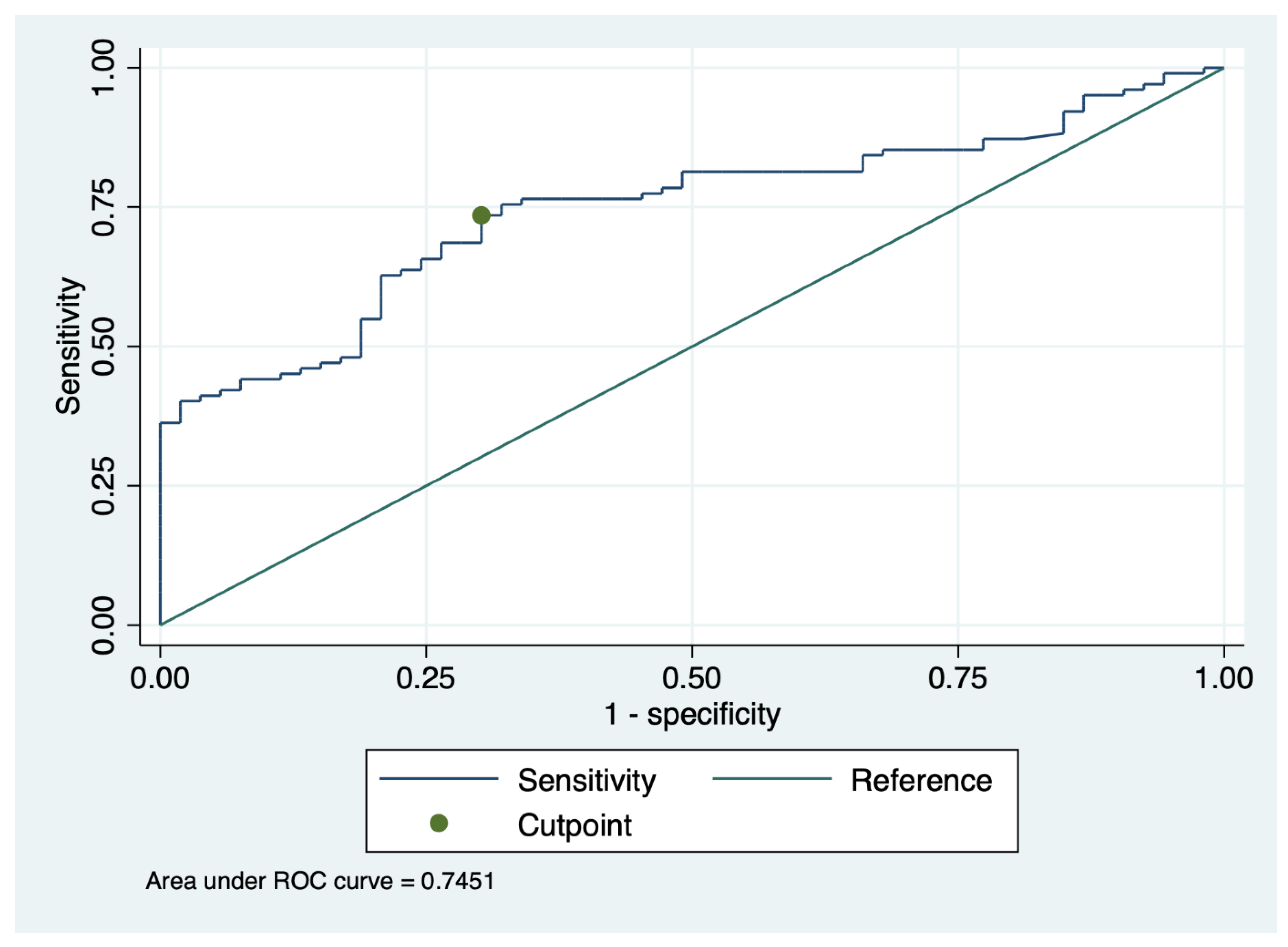
3.3. Sensitivity and Specificity of Urinary Collectrin for Diagnosis of AKI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef] [PubMed]
- Guzzi, L.M.; Bergler, T.; Binnall, B.; Engelman, D.T.; Forni, L.; Germain, M.J.; Gluck, E.; Göcze, I.; Joannidis, M.; Koyner, J.L.; et al. Clinical use of [TIMP-2]•[IGFBP7] biomarker testing to assess risk of acute kidney injury in critical care: Guidance from an expert panel. Crit. Care 2019, 23, 225. [Google Scholar] [CrossRef] [PubMed]
- Bonventre, J.V.; Yang, L. Cellular pathophysiology of ischemic acute kidney injury. J. Clin. Investig. 2011, 121, 4210–4221. [Google Scholar] [CrossRef] [PubMed]
- Han, W.K.; Bailly, V.; Abichandani, R.; Thadhani, R.; Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): A novel biomarker for human renal proximal tubule injury. Kidney Int. 2002, 62, 237–244. [Google Scholar] [CrossRef]
- Bernardi, M.H.; Wagner, L.; Ryz, S.; Puchinger, J.; Nixdorf, L.; Edlinger-Stanger, M.; Geilen, J.; Kainz, M.; Hiesmayr, M.J.; Lassnigg, A. Urinary neprilysin for early detection of acute kidney injury after cardiac surgery: A prospective observational study. Eur. J. Anaesthesiol.|EJA 2021, 38, 13–21. [Google Scholar] [CrossRef]
- Bennett, M.; Dent, C.L.; Ma, Q.; Dastrala, S.; Grenier, F.; Workman, R.; Syed, H.; Ali, S.; Barasch, J.; Devarajan, P. Urine NGAL Predicts Severity of Acute Kidney Injury After Cardiac Surgery: A Prospective Study. Clin. J. Am. Soc. Nephrol. 2008, 3, 665–673. [Google Scholar] [CrossRef]
- Soto, K.; Coelho, S.; Rodrigues, B.; Martins, H.; Frade, F.; Lopes, S.; Cunha, L.; Papoila, A.L.; Devarajan, P. Cystatin C as a Marker of Acute Kidney Injury in the Emergency Department. Clin. J. Am. Soc. Nephrol. 2010, 5, 1745. [Google Scholar] [CrossRef]
- Parikh, C.R.; Abraham, E.; Ancukiewicz, M.; Edelstein, C.L. Urine IL-18 is an early diagnostic marker for acute kidney injury and predicts mortality in the intensive care unit. J. Am. Soc. Nephrol. 2005, 16, 3046–3052. [Google Scholar] [CrossRef]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; et al. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit. Care 2013, 17, R25. [Google Scholar] [CrossRef]
- Pajenda, S.; Ilhan-Mutlu, A.; Preusser, M.; Roka, S.; Druml, W.; Wagner, L. NephroCheck data compared to serum creatinine in various clinical settings. BMC Nephrol. 2015, 16, 206. [Google Scholar] [CrossRef] [Green Version]
- Gonzales, P.A.; Pisitkun, T.; Hoffert, J.D.; Tchapyjnikov, D.; Star, R.A.; Kleta, R.; Wang, N.S.; Knepper, M.A. Large-scale proteomics and phosphoproteomics of urinary exosomes. J. Am. Soc. Nephrol. 2009, 20, 363–379. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Page, E.K.; Knechtle, S.J. Urine proteomics in kidney transplantation. Transplant. Rev. 2014, 28, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Shao, C.; Wei, L.; Duan, J.; Wu, S.; Li, X.; Li, M.; Sun, W. An individual urinary proteome analysis in normal human beings to define the minimal sample number to represent the normal urinary proteome. Proteome Sci. 2012, 10, 70. [Google Scholar] [CrossRef] [PubMed]
- Marimuthu, A.; O’Meally, R.N.; Chaerkady, R.; Subbannayya, Y.; Nanjappa, V.; Kumar, P.; Kelkar, D.S.; Pinto, S.M.; Sharma, R.; Renuse, S.; et al. A comprehensive map of the human urinary proteome. J. Proteome Res. 2011, 10, 2734–2743. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wada, J.; Hida, K.; Tsuchiyama, Y.; Hiragushi, K.; Shikata, K.; Wang, H.; Lin, S.; Kanwar, Y.S.; Makino, H. Collectrin, a collecting duct-specific transmembrane glycoprotein, is a novel homolog of ACE2 and is developmentally regulated in embryonic kidneys. J. Biol. Chem. 2001, 276, 17132–17139. [Google Scholar] [CrossRef]
- Danilczyk, U.; Sarao, R.; Remy, C.; Benabbas, C.; Stange, G.; Richter, A.; Arya, S.; Pospisilik, J.A.; Singer, D.; Camargo, S.M.; et al. Essential role for collectrin in renal amino acid transport. Nature 2006, 444, 1088–1091. [Google Scholar] [CrossRef]
- Kleta, R.; Gahl, W.A. Collecting evidence: The case of collectrin (Tmem27) and amino acid transport. Am. J. Physiol.-Renal Physiol. 2007, 292, F531–F532. [Google Scholar] [CrossRef]
- Malakauskas, S.M.; Quan, H.; Fields, T.A.; McCall, S.J.; Yu, M.J.; Kourany, W.M.; Frey, C.W.; Le, T.H. Aminoaciduria and altered renal expression of luminal amino acid transporters in mice lacking novel gene collectrin. Am. J. Physiol.-Renal Physiol. 2007, 292, F533–F544. [Google Scholar] [CrossRef]
- Singer, D.; Camargo, S.M. Collectrin and ACE2 in renal and intestinal amino acid transport. Channels 2011, 5, 410–423. [Google Scholar] [CrossRef]
- Mount, D.B. Collectrin and the kidney. Curr. Opin. Nephrol. Hypertens. 2007, 16, 427–429. [Google Scholar] [CrossRef]
- Zhang, Y.; Wada, J.; Yasuhara, A.; Iseda, I.; Eguchi, J.; Fukui, K.; Yang, Q.; Yamagata, K.; Hiesberger, T.; Igarashi, P.; et al. The role for HNF-1beta-targeted collectrin in maintenance of primary cilia and cell polarity in collecting duct cells. PLoS ONE 2007, 2, e414. [Google Scholar] [CrossRef] [PubMed]
- Buqaileh, R.; Saternos, H.; Ley, S.; Aranda, A.; Forero, K.; AbouAlaiwi, W.A. Can cilia provide an entry gateway for SARS-CoV-2 to human ciliated cells? Physiol. Genom. 2021, 53, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N.; Group, K.A.G.W. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Liu, X. Classification accuracy and cut point selection. Stat. Med. 2012, 31, 2676–2686. [Google Scholar] [CrossRef]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef]
- Simon, N.; Hertig, A. Alteration of Fatty Acid Oxidation in Tubular Epithelial Cells: From Acute Kidney Injury to Renal Fibrogenesis. Front. Med. 2015, 2, 52. [Google Scholar] [CrossRef]
- Akpinar, P.; Kuwajima, S.; Krützfeldt, J.; Stoffel, M. Tmem27: A cleaved and shed plasma membrane protein that stimulates pancreatic beta cell proliferation. Cell Metab. 2005, 2, 385–397. [Google Scholar] [CrossRef]
- Huang, L.; Belousova, T.; Chen, M.; DiMattia, G.; Liu, D.; Sheikh-Hamad, D. Overexpression of stanniocalcin-1 inhibits reactive oxygen species and renal ischemia/reperfusion injury in mice. Kidney Int. 2012, 82, 867–877. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Subjects without AKI (n = 53) | Subjects with AKI (n = 102) | p-Value |
|---|---|---|---|
| Age (years) | 54.3 ± 15.4 | 57.6 ± 17.4 | 0.25 |
| Gender–number (%) | |||
| -Male | 25 (47) | 60 (59) | 0.18 |
| -Female | 28 (53) | 42 (41) | |
| Unit of admission–number (%) | |||
| -Intensive care unit | 14 (26) | 19 (19) | 0.30 |
| Coexisting or prior illness–number (%) | |||
| -Arterial hypertension | 32 (60) | 71 (70) | |
| -Diabetes mellitus | 10 (19) | 30 (29) | 0.21 |
| -Cardiovascular disease | 20 (38) | 45 (44) | 0.18 |
| -Congestive heart failure | 9 (17) | 15 (15) | 0.49 |
| -Glomerulonephritis | 3 (6) | 10 (10) | 0.82 |
| Acute Kidney Injury [23]–number (%) | 0.54 | ||
| -No AKI | 53 (100) | ||
| -AKI stage I | 27 (26) | ||
| -AKI stage II | 18 (18) | ||
| -AKI stage III | 57 (56) | ||
| AKI aetiology–number (%) | |||
| -Infection-related | 44 (43) | ||
| -Hypovolemic state | 19 (19) | ||
| -Postrenal/obstructive | 6 (6) | ||
| -Intrinsic | 31 (30) | ||
| -Undefined | 2 (2) |
| Healthy Subjects | CKD | AKI I | AKI II | AKI III | p-Value | |
|---|---|---|---|---|---|---|
| Number of study participants | 21 | 32 | 27 | 18 | 57 | |
| Characteristics | ||||||
| -Age (years) | 46.1 ± 15.5 | 59.7 ± 13.0 | 56.9 ± 20.9 | 57.7 ± 16.1 | 58.0 ± 16.2 | 0.45 |
| -Gender—male number (%) | 9 (43) | 16 (50) | 14 (52) | 8 (44) | 38 (67) | 0.14 |
| Laboratory parameters | ||||||
| -Urine protein/creatinine ratio (mg/g) | 190 ± 9 | 1680 ± 2273 | 1356 ± 1447 | 953 ± 841 | 1718 ± 3446 | 0.21 |
| -Urine albumin/creatinine ratio (mg/g) | 20 ± 10 | 1159 ± 1701 | 668 ± 809 | 475 ± 556 | 868 ± 1722 | 0.99 |
| -HbA1c | 5.62 ± 0.16 | 5.86 ± 1.03 | 5.80 ± 1.13 | 5.87 ± 0.45 | 5.79 ± 0.93 | 0.73 |
| Baseline renal function parameters | ||||||
| -Baseline serum creatinine (mg/dL) | 0.64 ± 0.15 | 2.35 ± 1.35 | 1.47 ± 0.86 | 1.36 ± 0.64 | 1.39 ± 0.80 | 0.52 |
| -Baseline eGFR (mL/min) | 113.21 ± 18.87 | 37.94 ± 24.88 | 56.27 ± 32.91 | 60.23 ± 33.47 | 62.88 ± 29.98 | 0.46 |
| Biomarker for acute kidney injury | ||||||
| -Minimum urine collectrin levels (pg/mL) | 3468 ± 2452 | 2453 ± 1706 | 1630 ± 1956 | 1616 ± 2148 | 1576 ± 1686 | 0.001 |
| Variable | Regression Coefficient (95% CI) with Minimum Collectrin Adjusted a | p-Value |
|---|---|---|
| Gender (male) | 0.143 (−0.421 to 0.707) | 0.62 |
| Age (years) | −0.018 (−0.035 to −0.002) | 0.03 |
| Baseline eGFR (mL/min) | −0.004 (−0.014 to 0.006) | 0.41 |
| Peak C-reactive protein (mg/dL) | 0.005 (−0.024 to 0.033) | 0.74 |
| Peak white blood count (G/L) | 0.016 (−0.022 to 0.055) | 0.41 |
| Need for ICU admission | −0.760 (−1.534 to 0.015) | 0.06 |
| History of renal transplantation | −0.468 (−1.084 to 0.148) | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pajenda, S.; Wagner, L.; Gerges, D.; Herkner, H.; Tevdoradze, T.; Mechtler, K.; Schmidt, A.; Winnicki, W. Urinary Collectrin (TMEM27) as Novel Marker for Acute Kidney Injury. Life 2022, 12, 1391. https://doi.org/10.3390/life12091391
Pajenda S, Wagner L, Gerges D, Herkner H, Tevdoradze T, Mechtler K, Schmidt A, Winnicki W. Urinary Collectrin (TMEM27) as Novel Marker for Acute Kidney Injury. Life. 2022; 12(9):1391. https://doi.org/10.3390/life12091391
Chicago/Turabian StylePajenda, Sahra, Ludwig Wagner, Daniela Gerges, Harald Herkner, Tamar Tevdoradze, Karl Mechtler, Alice Schmidt, and Wolfgang Winnicki. 2022. "Urinary Collectrin (TMEM27) as Novel Marker for Acute Kidney Injury" Life 12, no. 9: 1391. https://doi.org/10.3390/life12091391