
Epiglottopexy Is a Treatment of Choice for Obstructive Sleep Apnea Caused by a Collapsing Epiglottis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Clinical Evaluation
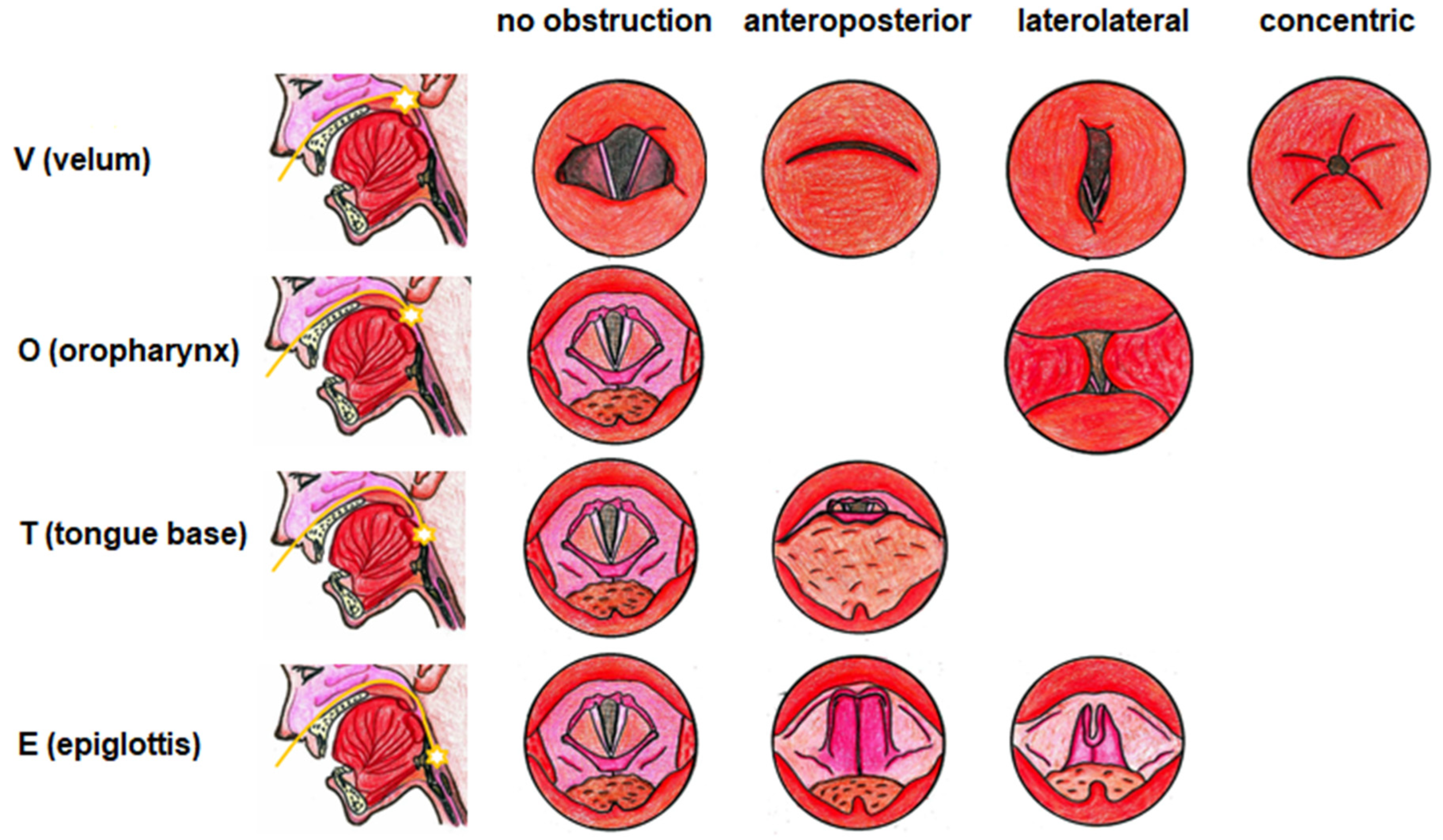
2.5. Drug-Induced Sleep Endoscopy
2.6. Positive Airway Pressure Titration during the Sleep Endoscopy
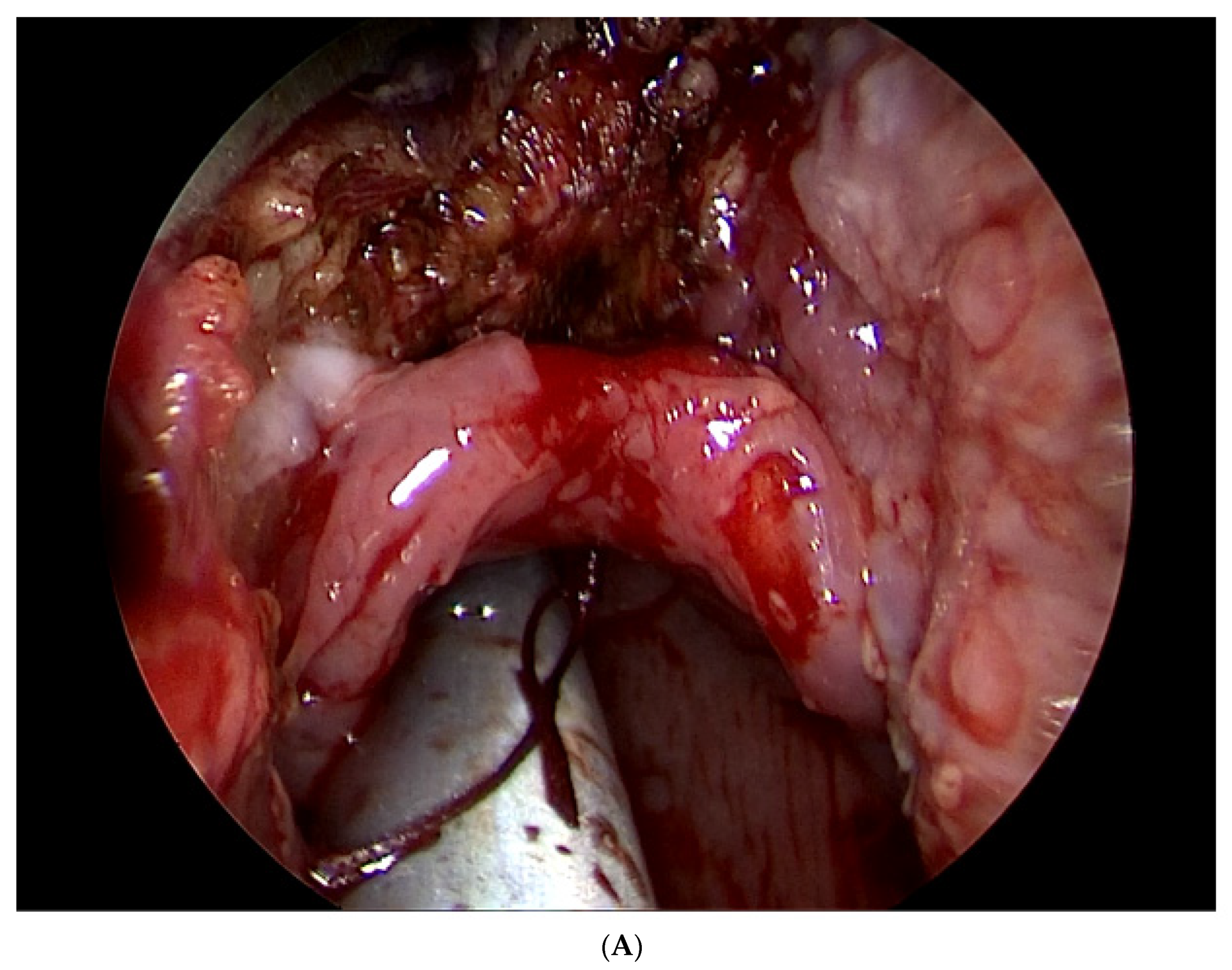
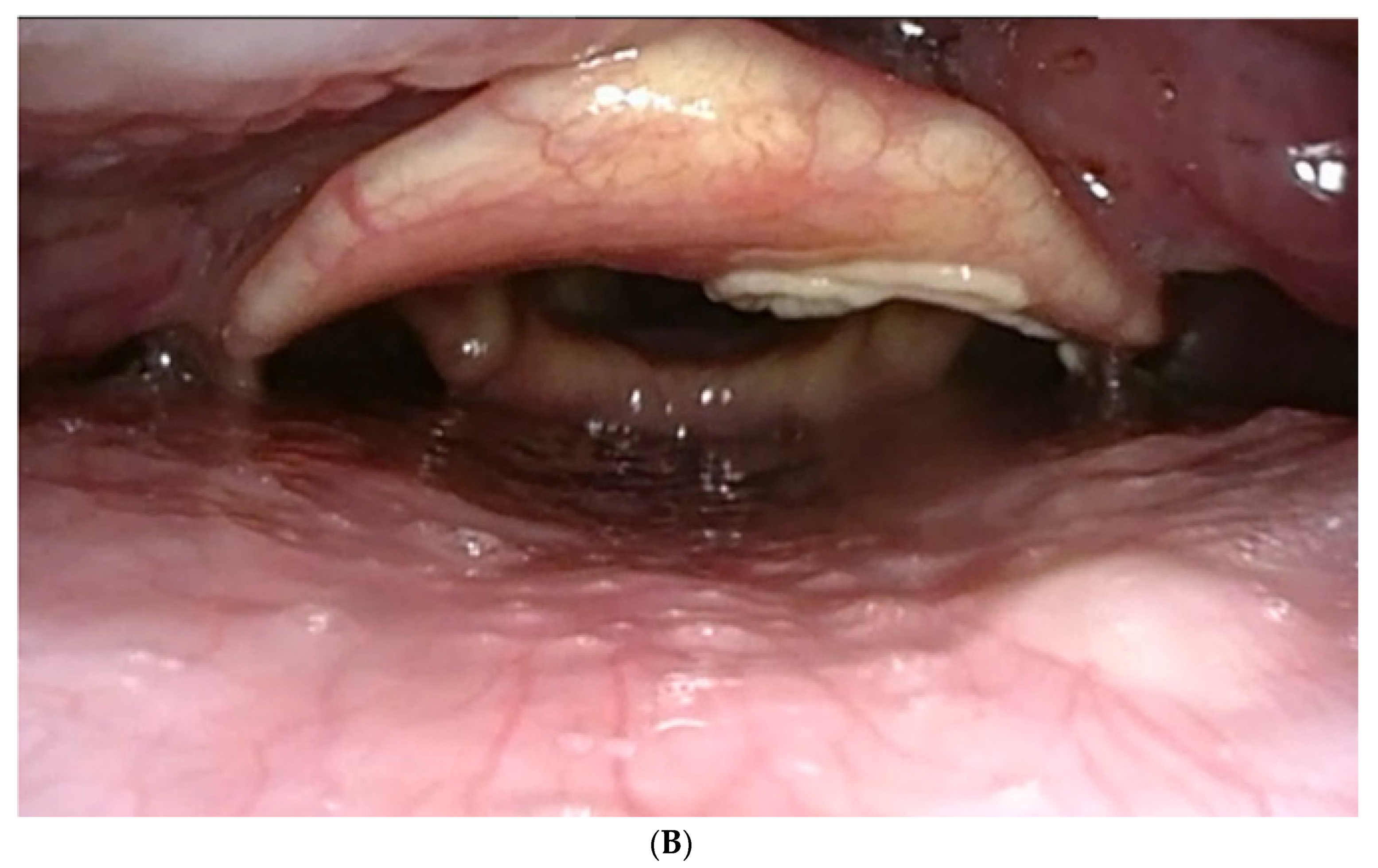
2.7. Surgical Technique
2.8. Postoperative Care
2.9. Follow-Up
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dedhia, E.C.; Rosen, C.A.; Soose, R.J. What is the role of the larynx in adult obstructive sleep apnea? Laryngoscope 2014, 124, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Torre, C.; Camacho, M.; Liu, S.Y.; Huon, L.K.; Capasso, R. Epiglottis collapse in adult obstructive sleep apnea: A systematic review. Laryngoscope 2016, 126, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Roustan, V.; Barbieri, M.; Incandela, F.; Missale, F.; Camera, H.; Braido, F.; Mora, R.; Peretti, G. Transoral glossoepiglottopexy in the treatment of adult obstructive sleep apnoea: A surgical approach. Acta Otorhinolaryngol. Ital. 2018, 38, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Kwon, E.O.; Jung, S.Y.; Al-Dilaijan, K.; Min, J.Y.; Lee, K.H.; Kim, S.W. Is Epiglottis Surgery Necessary for Obstructive Sleep Apnea Patients with Epiglottis Obstruction? Laryngoscope 2019, 129, 2658–2662. [Google Scholar] [CrossRef]
- Pavwoski, P.; Shelgikar, A.V. Treatment options for obstructive sleep apnea. Neurol. Clin. Pract. 2017, 7, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Waters, T. Alternative interventions for obstructive sleep apnea. Clevel. Clin. J. Med. 2019, 86, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Chaidas, K.; Garas, G.; Amlani, A. Outcome of TORS to tongue base and epiglottis in patients with OSA intolerant of conventional treatment. Sleep Breath. 2016, 20, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Bourolias, C.; Hajiioannou, J.; Sobol, E.; Velegrakis, G.; Helidonis, E. Epiglottis reshaping using CO2 laser: A minimally invasive technique and its potent applications. Head Face Med. 2008, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Kezirian, E.J.; Hussey, H.M.; Brietzke, S.E.; Cohen, S.M.; Davis, G.E.; Shin, J.J.; Weinberger, D.G.; Cabana, M.D. Hypopharyngeal surgery in obstructive sleep apnea: Practice patterns, perceptions, and attitudes. Otolaryngol. Head Neck Surg. 2012, 147, 964–971. [Google Scholar] [CrossRef]
- Yung-Chuan Liu, S.; Riley, R.W.; Yu, M.S. Surgical algorithm for obstructive sleep apnea: An update. Clin. Exp. Otorhinolaryngol. 2020, 13, 215–224. [Google Scholar] [CrossRef]
- Hybášková, J.; Jor, O.; Novák, V.; Matoušek, P.; Komínek, P. Možné využití spánkové endoskopie pro zvýšení efektivity léčby (operační i neoperační) u pacientu s obstrukční spánkovou apnoí. Česk Slov. Neurol. N 2017, 113, 428–433. [Google Scholar] [CrossRef]
- De Vito, A.; Cammaroto, G.; Chong, K.B.; Carrasco-Llatas, M.; Vicini, C. Drug-Induced Sleep Endoscopy: Clinical Application and Surgical Outcomes. Healthcare 2019, 7, 100. [Google Scholar] [CrossRef]
- Mickelson, S.A.; Rosenthal, L. Midline glossectomy and epiglottidectomy for obstructive sleep apnea syndrome. Laryngoscope 1997, 107, 614–619. [Google Scholar] [CrossRef]
- Fernández-Julián, E.; García-Pérez, M.A.; García-Callejo, J.; Ferrer, F.; Martí, F.; Marco, J. Surgical planning after sleep versus awake techniques in patients with obstructive sleep apnea. Laryngoscope 2014, 124, 1970–1974. [Google Scholar] [CrossRef]
- Koutsourelakis, I.; Safiruddin, F.; Ravesloot, M.; Zakynthinos, S.; de Vries, N. Surgery for obstructive sleep apnea: Sleep endoscopy determinants of outcome. Laryngoscope 2012, 122, 2587–2591. [Google Scholar] [CrossRef]
- Weaver, T.E.; Grunstein, R.R. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef]
- Camacho, M.; Certal, V.; Capasso, R. Comprehensive review of surgeries for obstructive sleep apnea syndrome. Braz. J. Otorhinolaryngol. 2013, 79, 780–788. [Google Scholar] [CrossRef]
- Kezirian, E.J.; Weaver, E.M.; Yueh, B.; Deyo, R.A.; Khuri, S.F.; Daley, J.; Henderson, W. Incidence of serious complications after uvulopalatopharyngoplasty. Laryngoscope 2004, 114, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Haavisto, L.; Suonpää, J. Complications of uvulopalatopharyngoplasty. Clin. Otolaryngol. Allied Sci. 1994, 19, 243–247. [Google Scholar] [CrossRef]
- Verse, T.; Pirsig, W. Age-related changes in the epiglottis causing failure of nasal continuous positive airway pressure therapy. J. Laryngol. Otol. 1999, 113, 1022–1025. [Google Scholar] [CrossRef]
- Kent, D.T.; Rogers, R.; Soose, R.J. Drug-induced sedation endoscopy in the evaluation of OSA patients with incomplete oral appliance therapy response. Otolaryngol. Head. Neck Surg. 2015, 153, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Sung, C.M.; Jang, H.B.; Kim, H.C.; Lim, S.C.; Yang, H.C. Patients with epiglottic collapse showed less severe obstructive sleep apnea and good response to treatment other than continuous positive airway pressure: A case-control study of 224 patients. J. Clin. Sleep Med. 2021, 17, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Azarbarzin, A.; Marques, M.; Sands, S.A.; de Beeck, S.O.; Genta, P.R.; Taranto-Montemurro, L.; de Melo, C.M.; Messineo, L.; Vanderveken, O.M.; White, D.P.; et al. Predicting epiglottic collapse in patients with obstructive sleep apnoea. Eur. Respir. J. 2017, 50, 1700345. [Google Scholar] [CrossRef]
- De Almeida, F.R.; Lowe, A.A.; Tsuiki, S.; Otsuka, R.; Wong, M.; Fastlicht, S. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J. Clin. Sleep Med. 2005, 1, 143–152. [Google Scholar] [CrossRef]
- Sung, C.M.; Kim, H.C.; Yang, H.C. The clinical characteristics of patients with an isolate epiglottic collapse. Auris Nasus Larynx 2020, 47, 450–457. [Google Scholar] [CrossRef]
- Cassano, M. Endoscopic coblator-assisted epiglottoplasty in “obstructive sleep apnoea syndrome” patients. Clin. Otolaryngol. 2017, 42, 1112–1114. [Google Scholar] [CrossRef]
- Oluwasanmi, A.F.; Mal, R.K. Diathermy epiglottectomy: Endoscopic technique. J. Laryngol. Otol. 2001, 115, 289–292. [Google Scholar] [CrossRef]
- Lin, H.S.; Rowley, J.A.; Badr, M.S.; Folbe, A.J.; Yoo, G.H.; Victor, L.; Mathog, R.H.; Chen, W. Transoral robotic surgery for treatment of obstructive sleep apnea-hypopnea syndrome. Laryngoscope 2013, 123, 1811–1816. [Google Scholar] [CrossRef]
- Catalfumo, F.J.; Golz, A.; Westerman, S.T.; Gilbert, L.M.; Joachims, H.Z.; Goldenberg, D. The epiglottis and obstructive sleep apnoea syndrome. J. Laryngol. Otol. 1998, 112, 940–943. [Google Scholar] [CrossRef]
- Sorrenti, G.; Piccin, O.; Mondini, S.; Ceroni, A.R. One-phase management of severe obstructive sleep apnea: Tongue base reduction with hyoepiglottoplasty plus uvulopalatopharyngoplasty. Otolaryngol. Head Neck Surg. 2006, 135, 906–910. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Preoperative BMI | Preoperative AHI | Preoperative ESS | Preinclusion Failed Therapy | Awake Examination Findings (Obstruction) | DISE Findings (Obstruction) | Opening PAP Pressure (hPa) | Postoperative BMI | Postoperative AHI | Postoperative ESS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 22 | 25.48 | 46.5 | 15 | PAP | Tonsils | Epiglottis | >18 | 25.15 | 1.3 | 5 |
| 2 | 50 | 30.88 | 33 | 16 | PAP UPPP | Tongue base | Epiglottis Tongue base | >18 | 31.25 | 5.3 | 4 |
| 3 | 44 | 29.32 | 8.3 | 11 | - | Soft palate Tongue base | Epiglottis | >18 | 28.76 | 4.8 | 4 |
| 4 | 58 | 31.1 | 46.5 | 20 | PAP | Soft palate Tongue base | Epiglottis, Tongue base | >18 | 31.15 | 28 | 12 |
| 5 | 49 | 26.59 | 18.3 | 18 | - | Soft palate Tongue base | Epiglottis Tongue base | >18 | 25.48 | 6.1 | 6 |
| 6 | 48 | 27.65 | 28.83 | 19 | PAP | Soft palate Tongue base | Epiglottis, Tongue base | >18 | 28.88 | 11.7 | 4 |
| 7 | 32 | 28.47 | 25.74 | 15 | PAP | Soft palate Tongue base | Epiglottis Tongue base | >18 | 29.32 | 10.2 | 3 |
| 8 | 41 | 26.2 | 23.99 | 15 | PAP | Soft palate | Epiglottis Tongue base | >18 | 29.7 | 10.8 | 6 |
| 9 | 38 | 32 | 11 | 13 | - | Soft palate Tongue base | Epiglottis | >18 | 31.67 | 9 | 2 |
| 10 | 55 | 28 | 17.1 | 14 | - | Soft palate Tongue base | Epiglottis Tongue base | >18 | 26.54 | 7.7 | 4 |
| Median (Min; Max) | ||||
|---|---|---|---|---|
| Preoperative | Postoperative | Difference | p * | |
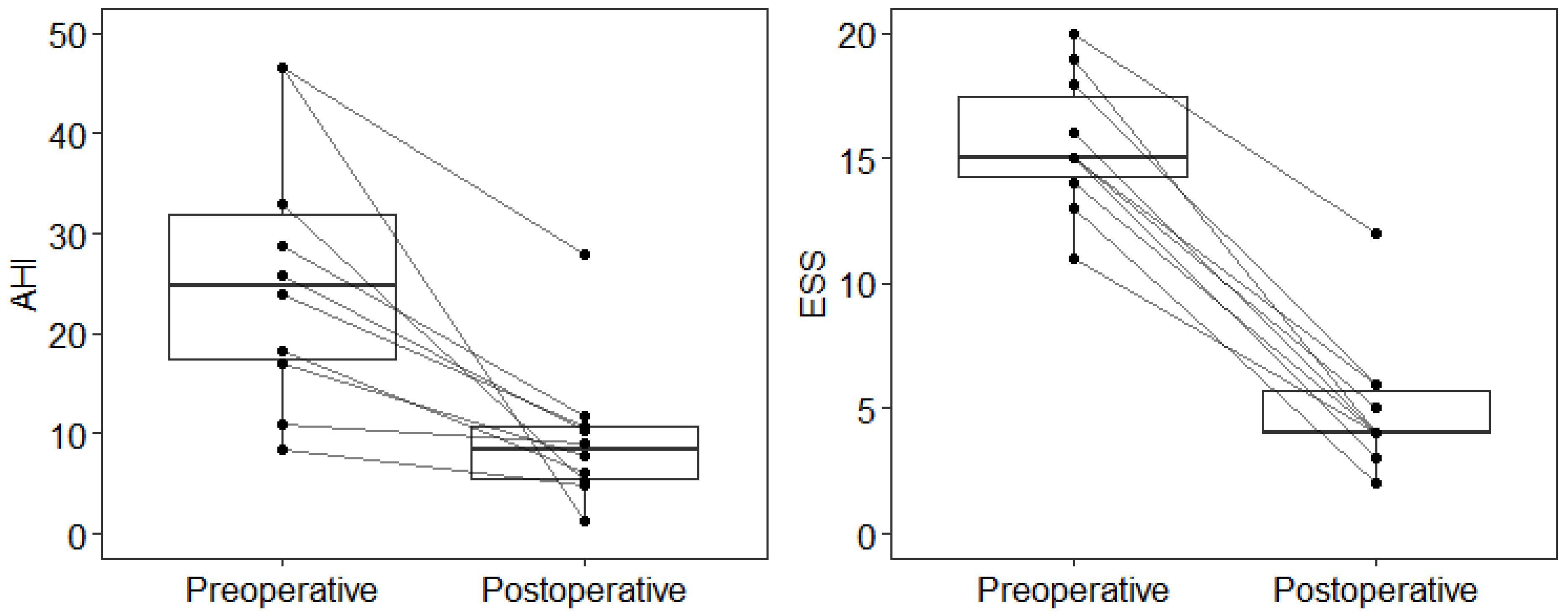
| AHI | 24.9 (8.3; 46.5) | 8.4 (1.3; 28.0) | 14.4 (2.0; 45.2) | <0.001 |
| ESS | 15 (11; 20) | 4 (2; 12) | 11 (7; 15) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masárová, M.; Formánek, M.; Jor, O.; Novák, V.; Vrtková, A.; Matoušek, P.; Komínek, P.; Zeleník, K. Epiglottopexy Is a Treatment of Choice for Obstructive Sleep Apnea Caused by a Collapsing Epiglottis. Life 2022, 12, 1378. https://doi.org/10.3390/life12091378
Masárová M, Formánek M, Jor O, Novák V, Vrtková A, Matoušek P, Komínek P, Zeleník K. Epiglottopexy Is a Treatment of Choice for Obstructive Sleep Apnea Caused by a Collapsing Epiglottis. Life. 2022; 12(9):1378. https://doi.org/10.3390/life12091378
Chicago/Turabian StyleMasárová, Michaela, Martin Formánek, Ondřej Jor, Vilém Novák, Adéla Vrtková, Petr Matoušek, Pavel Komínek, and Karol Zeleník. 2022. "Epiglottopexy Is a Treatment of Choice for Obstructive Sleep Apnea Caused by a Collapsing Epiglottis" Life 12, no. 9: 1378. https://doi.org/10.3390/life12091378