
Effect of Malignancy on Semen Parameters

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
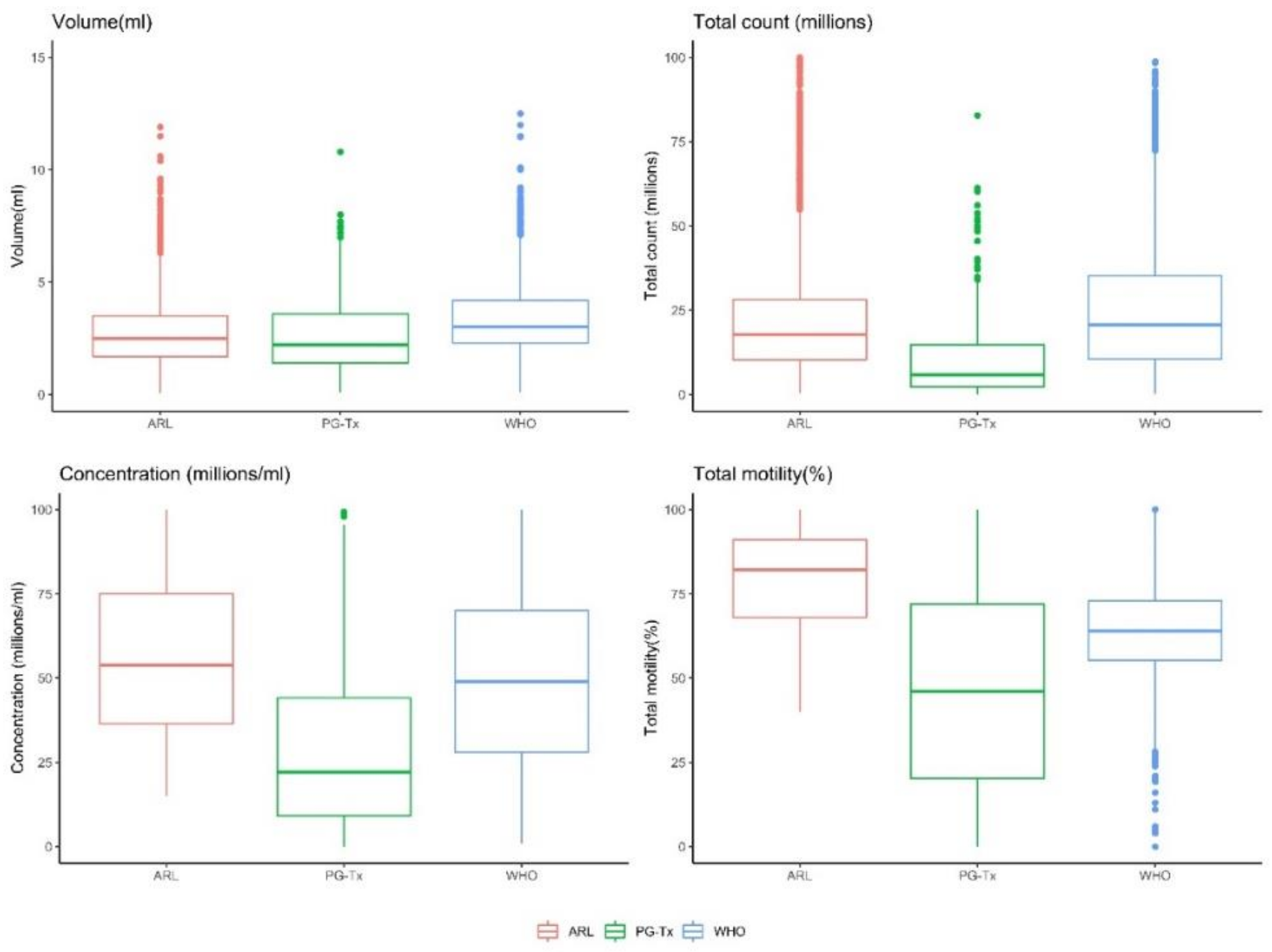
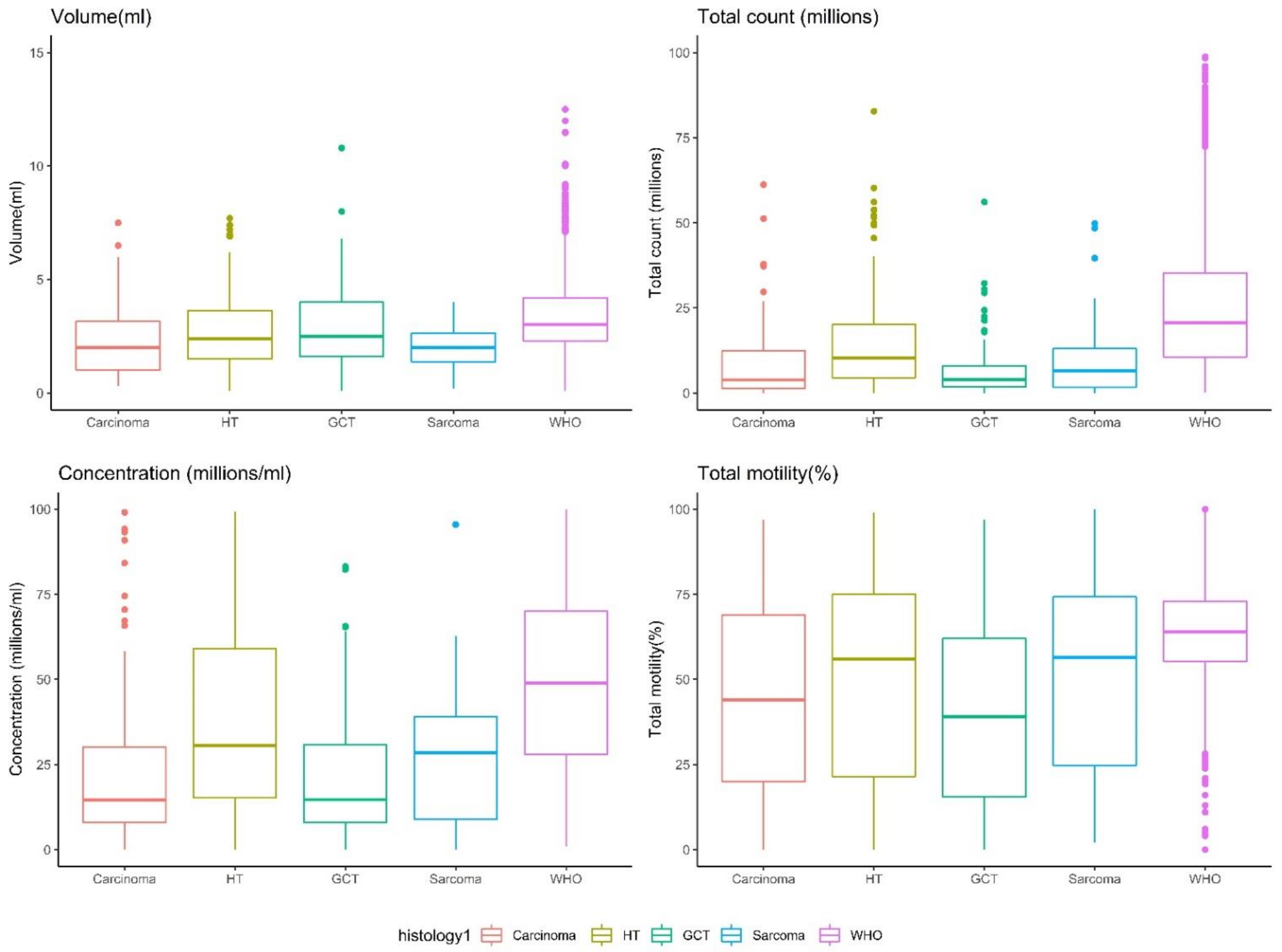
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Trottmann, M.; Becker, A.J.; Stadler, T.; Straub, J.; Soljanik, I.; Schlenker, B.; Stief, C.G. Semen quality in men with malignant diseases before and after therapy and the role of cryopreservation. Eur. Urol. 2007, 52, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Padron, O.F.; Sharma, R.K.; Thomas, A.J.; Agarwal, A. Effects of cancer on spermatozoa quality after cryopreservation: A 12-year experience. Fertil. Steril. 1997, 67, 326–331. [Google Scholar] [CrossRef]
- Pourmasumi, S.; Sabeti, P.; Rahiminia, T.; Mangoli, E.; Tabibnejad, N.; Talebi, A.R. The etiologies of DNA abnormalities in male infertility: An assessment and review. Int. J. Reprod. Biomed. 2017, 15, 331–344. [Google Scholar] [CrossRef] [PubMed]
- MacKenna, A.; Crosby, J.; Huidobro, C.; Correa, E.; Duque, G. Semen quality before cryopreservation and after thawing in 543 patients with testicular cancer. JBRA Assist. Reprod. 2017, 21, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Hamano, I.; Hatakeyama, S.; Nakamura, R.; Fukuhara, R.; Noro, D.; Tanaka, T.; Yoneyama, T.; Yamamoto, H.; Yoneyama, T.; Hashimoto, Y.; et al. Differences in semen characteristics between patients with testicular cancer and other malignancies using various cut-off values. Int. J. Urol. 2018, 25, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Caponecchia, L.; Cimino, G.; Sacchetto, R.; Fiori, C.; Sebastianelli, A.; Salacone, P.; Marcucci, I.; Tomassini, S.; Rago, R. Do malignant diseases affect semen quality? Sperm parameters of men with cancers. Andrologia 2016, 48, 333–340. [Google Scholar] [PubMed]
- Xu, R.; Centola, G.M.; Tanrikut, C. Genitourinary cancer patients have worse baseline semen parameters than healthy sperm bankers. Andrology 2019, 7, 449–453. [Google Scholar] [CrossRef]
- Bizet, P.; Saias-Magnan, J.; Jouve, E.; Grillo, J.M.; Karsenty, G.; Metzler-Guillemain, C.; Perrin, J. Sperm cryopreservation before cancer treatment: A 15-year monocentric experience. Reprod. Biomed. Online 2012, 24, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Carlsen, E.; Andersson, A.-M.; Petersen, J.H.; Skakkebaek, N.E. History of febrile illness and variation in semen quality. Hum. Reprod. 2003, 18, 2089–2092. [Google Scholar] [CrossRef]
- Van der Kaaij, M.A.E.; Heutte, N.; van Echten-Arends, J.; Raemaekers, J.M.M.; Carde, P.; Noordijk, E.M.; Christophe, F.; Tomas, J.; Eghbali, H.; Brice, P.; et al. Sperm quality before treatment in patients with early stage Hodgkin’s lymphoma enrolled in EORTC-GELA Lymphoma Group trials. Haematologica 2009, 94, 1691–1697. [Google Scholar] [CrossRef]
- Sieniawski, M.; Reineke, T.; Josting, A.; Nogova, L.; Behringer, K.; Halbsguth, T.; Fuchs, M.; Diehl, V.; Engert, A. Assessment of male fertility in patients with Hodgkin’s lymphoma treated in the German Hodgkin Study Group (GHSG) clinical trials. Ann. Oncol. 2008, 19, 1795–1801. [Google Scholar] [CrossRef]
- Rueffer, U.; Breuer, K.; Josting, A.; Lathan, B.; Sieber, M.; Manzke, O.; Grotenhermen, F.J.; Tesch, H.; Bredenfeld, H.; Koch, P.; et al. Male gonadal dysfunction in patients with Hodgkin’s disease prior to treatment. Ann. Oncol. 2001, 12, 1307–1311. [Google Scholar] [CrossRef]
- Xavier, R.; de Carvalho, R.C.; Fraietta, R. Semen quality from patients affected by seminomatous and non-seminomatous testicular tumor. Int. Braz. J. Urol. 2021, 47, 495–502. [Google Scholar] [CrossRef]
- Sposito, C.; Camargo, M.; Tibaldi, D.S.; Barradas, V.; Cedenho, A.P.; Nichi, M.; Bertolla, R.P.; Spaine, D.M. Antioxidant enzyme profile and lipid peroxidation products in semen samples of testicular germ cell tumor patients submitted to orchiectomy. Int. Braz. J. Urol. 2017, 43, 644–651. [Google Scholar] [CrossRef] [Green Version]
- Dias, T.R.; Agarwal, A.; Pushparaj, P.N.; Ahmad, G.; Sharma, R. Reduced semen quality in patients with testicular cancer seminoma is associated with alterations in the expression of sperm proteins. Asian J. Androl. 2020, 22, 88–93. [Google Scholar]
- Cheng, C.Y.; Mruk, D.D. The blood-testis barrier and its implications for male contraception. Pharmacol. Rev. 2012, 64, 16–64. [Google Scholar] [CrossRef] [Green Version]
- Pallotti, F.; Pelloni, M.; Faja, F.; Di Chiano, S.; Di Rocco, A.; Lenzi, A.; Lombardo, F.; Paoli, D. Semen quality in non-Hodgkin lymphoma survivors: A monocentric retrospective study. Hum. Reprod. 2021, 36, 16–25. [Google Scholar] [CrossRef]
- Williams, D.H.; Karpman, E.; Sander, J.C.; Spiess, P.E.; Pisters, L.L.; Lipshultz, L.I. Pretreatment semen parameters in men with cancer. J. Urol. 2009, 181, 736–740. [Google Scholar] [CrossRef]
- Hallak, J.; Mahran, A.; Chae, J.; Agarwal, A. Poor semen quality from patients with malignancies does not rule out sperm banking. Urol. Res. 2000, 28, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Van Casteren, N.J.; Boellaard, W.P.A.; Romijn, J.C.; Dohle, G.R. Gonadal dysfunction in male cancer patients before cytotoxic treatment. Int. J. Androl. 2010, 33, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Amirjannati, N.; Sadeghi, M.; Hosseini Jadda, S.H.; Ranjbar, F.; Kamali, K.; Akhondi, M.A. Evaluation of semen quality in patients with malignancies referred for sperm banking before cancer treatment. Andrologia 2011, 43, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmon-Divon, M.; Shrem, G.; Balayla, J.; Nehushtan, T.; Volodarsky-Perel, A.; Steiner, N.; Son, W.-Y.; Dahan, M.H. An age-based sperm nomogram: The McGill reference guide. Hum. Reprod. 2020, 35, 2213–2225. [Google Scholar] [CrossRef]
- Cooper, T.G.; Noonan, E.; von Eckardstein, S.; Auger, J.; Baker, H.W.G.; Behre, H.M.; Haugen, T.B.; Kruger, T.; Wang, C.; Mbizvo, M.T. World Health Organization reference values for human semen characteristics. Hum. Reprod. Update 2010, 16, 231–245. [Google Scholar] [CrossRef]
- Campbell, M.J.; Lotti, F.; Baldi, E.; Schlatt, S.; Festin, M.P.R.; Björndahl, L.; Toskin, I.; Barratt, C.L.R. Distribution of semen examination results 2020—A follow up of data collated for the WHO semen analysis manual 2010. Andrology 2021, 9, 817–822. [Google Scholar] [CrossRef]
- Hazra, A.; Gogtay, N. IJD® module on biostatistics and research methodology for the dermatologist—Module editor: SAUMYA panda. Indian J. Dermatol. 2016, 61, 251–260. [Google Scholar] [CrossRef]
- rapidtable.com. Pie Chart Maker. 2022. Available online: https://www.rapidtables.com/tools/pie-chart.html (accessed on 17 February 2022).
- Brannigan, R.E.; Fantus, R.J.; Halpern, J.A. Fertility preservation in men: A contemporary overview and a look toward emerging technologies. Fertil. Steril. 2021, 115, 1126–1139. [Google Scholar] [CrossRef]
- Gandini, L.; Lombardo, F.; Salacone, P.; Paoli, D.; Anselmo, A.P.; Culasso, F.; Dondero, F.; Lenzi, A. Testicular cancer and Hodgkin’s disease: Evaluation of semen quality. Hum. Reprod. 2003, 18, 796–801. [Google Scholar] [CrossRef] [Green Version]
- Meirow, D.; Schenker, J.G. Cancer and male infertility. Hum. Reprod. 1995, 10, 2017–2022. [Google Scholar] [CrossRef]
- Bahadur, G.; Ozturk, O.; Muneer, A.; Wafa, R.; Ashraf, A.; Jaman, N.; Patel, S.; Oyede, A.W.; Ralph, D.J. Semen quality before and after gonadotoxic treatment. Hum. Reprod. 2005, 20, 774–781. [Google Scholar] [CrossRef] [Green Version]
- Degl’Innocenti, S.; Filimberti, E.; Magini, A.; Krausz, C.; Lombardi, G.; Fino, M.G.; Rastrelli, G.; Maggi, M.; Baldi, E. Semen cryopreservation for men banking for oligospermia, cancers, and other pathologies: Prediction of post-thaw outcome using basal semen quality. Fertil. Steril. 2013, 100, 1555–1563. [Google Scholar] [CrossRef]
- Di Bisceglie, C.; Bertagna, A.; Composto, E.R.; Lanfranco, F.; Baldi, M.; Motta, G.; Barberis, A.M.; Napolitano, E.; Castellano, E.; Manieri, C. Effects of oncological treatments on semen quality in patients with testicular neoplasia or lymphoproliferative disorders. Asian J. Androl. 2013, 15, 425–429. [Google Scholar] [CrossRef] [Green Version]
- Nagler, H.M. Male factor infertility: A solitary semen analysis can never predict normal fertility. Nat. Rev. Urol. 2011, 8, 16–17. [Google Scholar] [CrossRef]
- Borges, E., Jr. Total motile sperm count: A better way to rate the severity of male factor infertility? JBRA Assist. Reprod. 2016, 20, 47–48. [Google Scholar] [CrossRef]
- Guzick, D.S.; Overstreet, J.W.; Factor-Litvak, P.; Brazil, C.K.; Nakajima, S.T.; Coutifaris, C.; Carson, S.A.; Cisneros, P.; Steinkampf, M.P.; Hill, J.A.; et al. Sperm morphology, motility, and concentration in fertile and infertile men. N. Engl. J. Med. 2001, 345, 1388–1393. [Google Scholar] [CrossRef]
- Buck Louis, G.M.; Sundaram, R.; Schisterman, E.F.; Sweeney, A.; Lynch, C.D.; Kim, S.; Maisog, J.M.; Gore-Langton, R.; Eisenberg, M.L.; Chen, Z. Semen quality and time to pregnancy: The Longitudinal Investigation of Fertility and the Environment Study. Fertil. Steril. 2014, 101, 453–462. [Google Scholar] [CrossRef] [Green Version]
- Slama, R.; Eustache, F.; Ducot, B.; Jensen, T.K.; Jørgensen, N.; Horte, A.; Irvine, S.; Suominen, J.; Andersen, A.G.; Auger, J.; et al. Time to pregnancy and semen parameters: A cross-sectional study among fertile couples from four European cities. Hum. Reprod. 2002, 17, 503–515. [Google Scholar] [CrossRef] [Green Version]
- Ayala, C.; Steinberger, E.; Smith, D.P. The influence of semen analysis parameters on the fertility potential of infertile couples. J. Androl. 1996, 17, 718–725. [Google Scholar]
- Keihani, S.; Verrilli, L.E.; Zhang, C.; Presson, A.P.; Hanson, H.A.; Pastuszak, A.W.; Johnstone, E.B.; Hotaling, J.M. Semen parameter thresholds and time-to-conception in subfertile couples: How high is high enough? Hum. Reprod. 2021, 36, 2121–2133. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
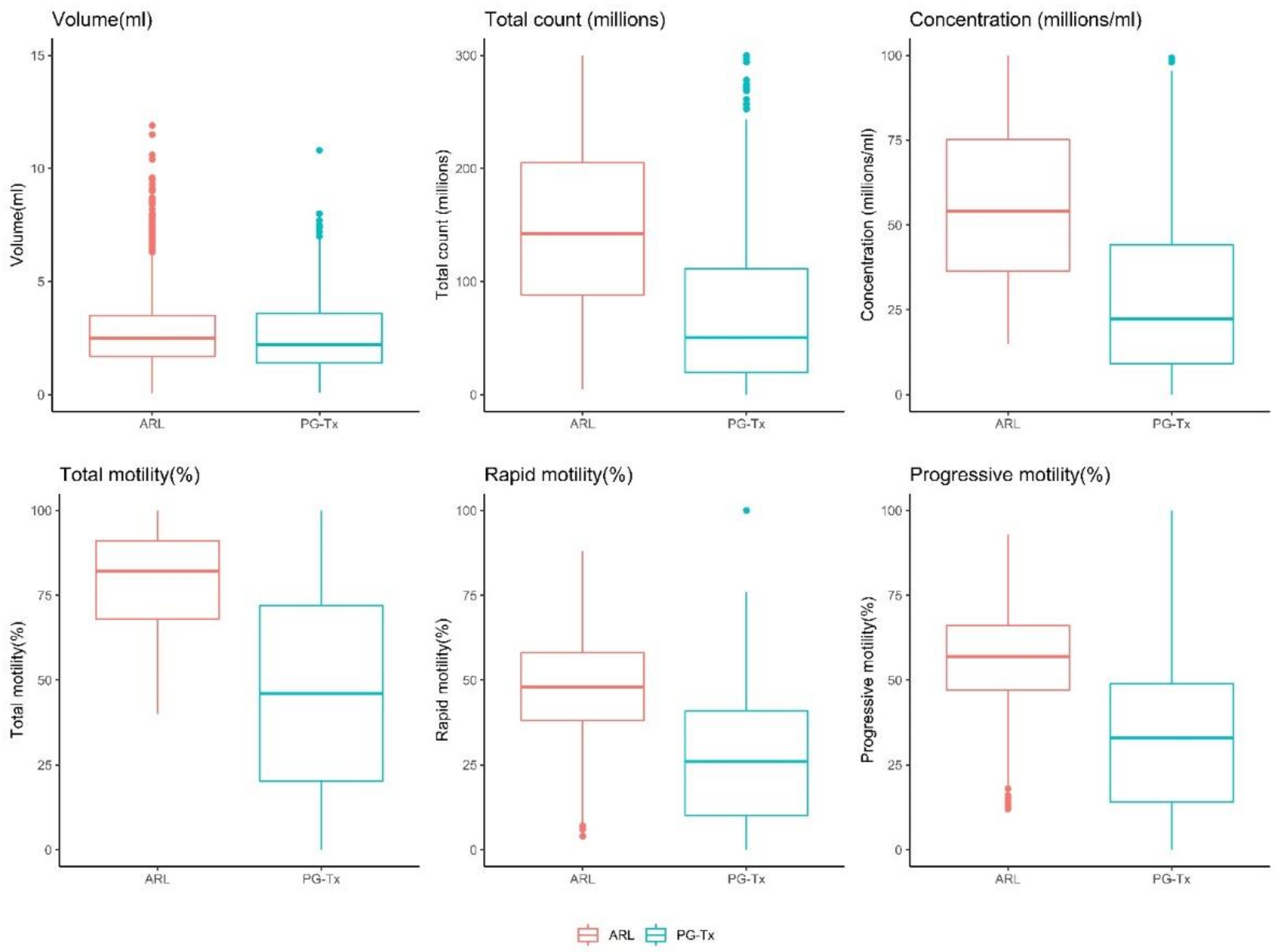
| Beta | 95% CI | p | R2 | |
|---|---|---|---|---|
| Volume * | −12.1% | −16.3%, −8.6% | <0.001 | 0.02 |
| Concentration * | −65.6% | −68.3%, −62.8% | <0.001 | 0.10 |
| Total count (millions) * | −72.7% | −75.0%, −69.0% | <0.001 | 0.09 |
| Total motility (%) | −33 | −34.9, −31.1 | <0.001 | 0.15 |
| Rapid motility (%) | −22.2 | −23.8, −20.6 | <0.001 | 0.10 |
| Progressive Motility (%) | −24.7 | −26.3, −23.1 | <0.001 | 0.09 |
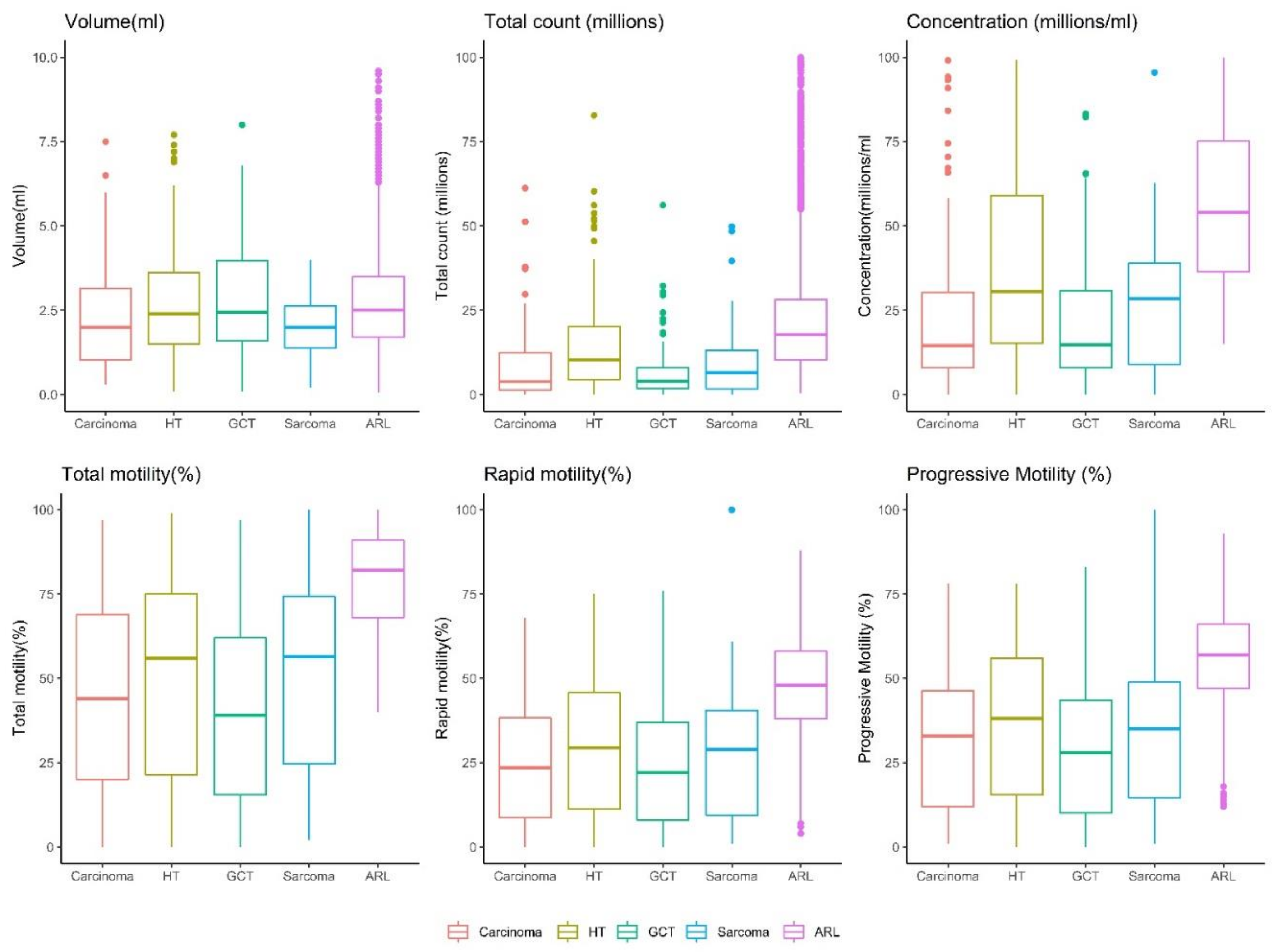
| Semen Parameter | Cancer Type | Beta | 95% CI | p |
|---|---|---|---|---|
| Total count (millions) * | Carcinoma | −73.3% | −78.3%, −67.2% | <0.001 |
| Hematological cancer | −57.6% | −63.8%, −50.4% | <0.001 | |
| Germ cell tumor | −82.7% | −85.4%, −79.4% | <0.001 | |
| Sarcoma | −76.8% | −82.4%, −69.3% | <0.001 | |
| Volume (mL) * | Carcinoma | −11.6% | −19.4%, −3.11% | <0.01 |
| Hematological cancer | −12.4% | −18.4%, −5.9% | <0.001 | |
| Germ cell tumor | −7.4% | −14.3%, −0.007% | <0.05 | |
| Sarcoma | −27.3% | −35.9%, −17.6% | <0.001 | |
| Concentration (mil/mL) * | Carcinoma | −69.4% | −74%, −64.1% | <0.001 |
| Hematological cancer | −48.5% | −54.5%, −41.7% | <0.001 | |
| Germ cell tumor | −78.8% | −81.5%, −75.7% | <0.001 | |
| Sarcoma | −57.9% | −66.2%, −47.5% | <0.001 | |
| Total motility (%) | Carcinoma | −33.3 | −37.2, −29.4 | <0.001 |
| Hematological cancer | −28.7 | −31.7, −25.7% | <0.001 | |
| Germ cell tumor | −38.7 | −42, −35.4 | <0.001 | |
| Sarcoma | −31.2 | −36.5, −25.8 | <0.001 | |
| Rapid motility(%) | Carcinoma | −22.5 | −25.9, −19.2 | <0.001 |
| Hematological cancer | −19.8 | −22.3, −17.2 | <0.001 | |
| Germ cell tumor | −24.4 | −27.3,−21.6 | <0.001 | |
| Sarcoma | −23.4 | −27.9,−18.9 | <0.001 | |
| Progressive Motility (%) | Carcinoma | −24.4 | −27.8, −21 | <0.001 |
| Hematological cancer | −21.7 | −24.3, −19.1 | <0.001 | |
| Germ cell tumor | −28.1 | −31, −25.2 | <0.001 | |
| Sarcoma | −26.2 | −30.8, −21.6 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrem, G.; Azani, L.; Feferkorn, I.; Listovsky, T.; Hussaini, S.; Farber, B.; Dahan, M.H.; Salmon-Divon, M. Effect of Malignancy on Semen Parameters. Life 2022, 12, 922. https://doi.org/10.3390/life12060922
Shrem G, Azani L, Feferkorn I, Listovsky T, Hussaini S, Farber B, Dahan MH, Salmon-Divon M. Effect of Malignancy on Semen Parameters. Life. 2022; 12(6):922. https://doi.org/10.3390/life12060922
Chicago/Turabian StyleShrem, Guy, Liat Azani, Ido Feferkorn, Tamar Listovsky, Sofia Hussaini, Benjamin Farber, Michael H. Dahan, and Mali Salmon-Divon. 2022. "Effect of Malignancy on Semen Parameters" Life 12, no. 6: 922. https://doi.org/10.3390/life12060922