
Proprioceptive Neuromuscular Facilitation-Based Physical Therapy on the Improvement of Balance and Gait in Patients with Chronic Stroke: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Inclusion/Exclusion Criteria for Studies
2.3. Screening Process
2.4. Methodological Quality and Risk of Bias Assessment
2.5. Data Extraction and Analysis
3. Results
3.1. Study Selection
3.2. Quality Appraisal and Risk of Bias
3.3. Participant Characteristics
3.4. Participant Inclusion Criteria
3.5. Interventions Administered
3.6. Outcome Measures
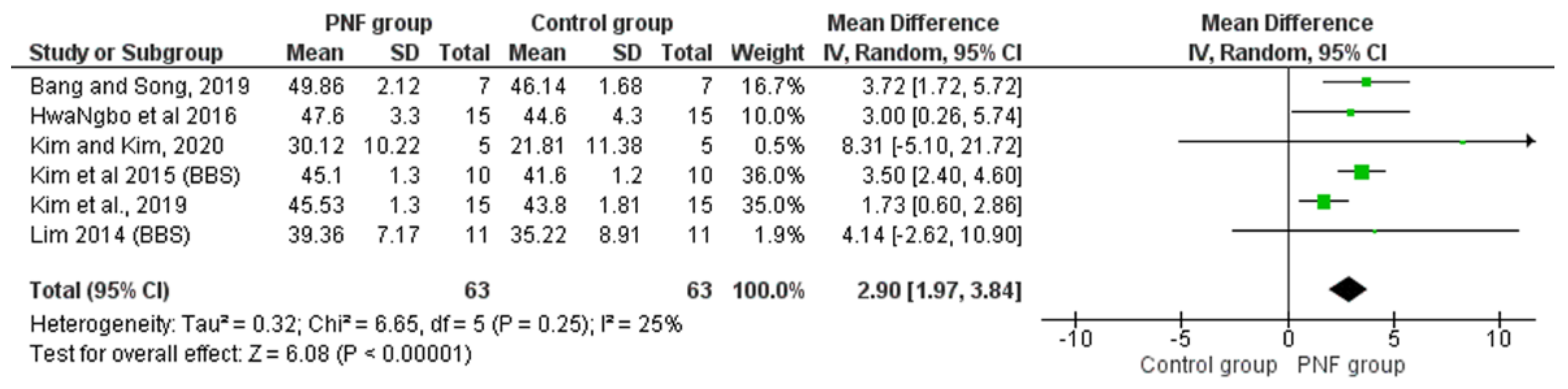
3.6.1. Balance
Berg Balance Scale
Functional Reach Test
Timed up and Go Test
3.6.2. Gait
10-Meter Walking Test
4. Discussion
4.1. Limitations of Included Studies
4.2. Strengths and Weaknesses of This Review
4.3. Implications for Clinical Practice and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adamson, J.; Beswick, A.; Ebrahim, S. Is stroke the most common cause of disability? J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2004, 13, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Bushnell, C.; Bettger, J.P.; Cockroft, K.M.; Cramer, S.C.; Edelen, M.O.; Hanley, D.; Katzan, I.L.; Mattke, S.; Nilsen, D.M.; Piquado, T.; et al. Chronic stroke outcome measures for motor function intervention trials: Expert panel recommendations. Circ. Cardiovasc. Qual. Outcomes 2015, 8 (Suppl. 3), S163–S169. [Google Scholar] [CrossRef] [Green Version]
- Kollen, B.; van de Port, I.; Lindeman, E.; Twisk, J.; Kwakkel, G. Predicting improvement in gait after stroke: A longitudinal prospective study. Stroke 2005, 36, 2676–2680. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.L.; Kesar, T.M.; Ting, L.H. Motor module generalization across balance and walking is impaired after stroke. J. Neurophysiol. 2019, 122, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Briggs, R.; O’Neill, D. Chronic stroke disease. Br. J. Hosp. Med. 2016, 77, C66–C69. [Google Scholar] [CrossRef]
- Beyaert, C.; Vasa, R.; Frykberg, G.E. Gait post-stroke: Pathophysiology and rehabilitation strategies. Neurophysiol. Clin. 2015, 45, 335–355. [Google Scholar] [CrossRef]
- Jamal, K.; Leplaideur, S.; Rousseau, C.; Chochina, L.; Moulinet-Raillon, A.; Bonan, I. Disturbances of spatial reference frame and postural asymmetry after a chronic stroke. Exp. Brain Res. 2018, 236, 2377–2385. [Google Scholar] [CrossRef]
- Hakakzadeh, A.; Shariat, A.; Honarpishe, R.; Moradi, V.; Ghannadi, S.; Sangelaji, B.; Nakhostin Ansari, N.; Hasson, S.; Ingle, L. Concurrent impact of bilateral multiple joint functional electrical stimulation and treadmill walking on gait and spasticity in post-stroke survivors: A pilot study. Physiother. Theory Pract. 2019, 37, 1368–1376. [Google Scholar] [CrossRef]
- Shariat, A.; Nakhostin Ansari, N.; Honarpishe, R.; Moradi, V.; Hakakzadeh, A.; Cleland, J.A.; Kordi, R. Effect of cycling and functional electrical stimulation with linear and interval patterns of timing on gait parameters in patients after stroke: A randomized clinical trial. Disabil. Rehabil. 2021, 43, 1890–1896. [Google Scholar] [CrossRef]
- Guiu Tula, F.X.; Cabanas Valdes, R.; Sitja Rabert, M.; Urrutia, G.; Gomara Toldra, N. The Efficacy of the proprioceptive neuromuscular facilitation (PNF) approach in stroke rehabilitation to improve basic activities of daily living and quality of life: A systematic review and meta-analysis protocol. BMJ Open 2017, 7, e016739. [Google Scholar] [CrossRef] [Green Version]
- Gunning, E.; Uszynski, M.K. Effectiveness of the Proprioceptive Neuromuscular Facilitation method on gait parameters in patients with stroke: A systematic review. Arch. Phys. Med. Rehabil. 2019, 100, 980–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cayco, C.S.; Gorgon, E.J.R.; Lazaro, R.T. Effects of proprioceptive neuromuscular facilitation on balance, strength, and mobility of an older adult with chronic stroke: A case report. J. Bodyw. Mov. Ther. 2017, 21, 767–774. [Google Scholar] [CrossRef]
- Gabriel, D.A.; Kamen, G.; Frost, G. Neural adaptations to resistive exercise: Mechanisms and recommendations for training practices. Sports Med. 2006, 36, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Shimura, K.; Kasai, T. Effects of proprioceptive neuromuscular facilitation on the initiation of voluntary movement and motor evoked potentials in upper limb muscles. Hum. Mov. Sci. 2002, 21, 101–113. [Google Scholar] [CrossRef]
- Cayco, C.S.; Gorgon, E.J.R.; Lazaro, R.T. Proprioceptive neuromuscular facilitation to improve motor outcomes in older adults with chronic stroke. Neurosciences 2019, 24, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, T.S.; de Sousa e Silva, E.M.; Sousa Silva, W.H.; de Alencar Caldas, V.V.; Silva, D.L.; Costa Cavalcanti, F.A.; Lindquist, A.R. Effects of a training program based on the proprioceptive neuromuscular facilitation method on post-stroke motor recovery: A preliminary study. J. Bodyw. Mov. Ther. 2014, 18, 526–532. [Google Scholar] [CrossRef]
- Jeun, Y.J. Meta-analysis of the Effect of Proprioceptive Neuromuscular Facilitation Training on Gait Ability in Patients with Storke. J. Korea Soc. Comput. Inf. 2021, 26, 165–172. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Foley, N.C.; Teasell, R.W.; Bhogal, S.K.; Speechley, M.R. Stroke Rehabilitation Evidence-Based Review: Methodology. Top. Stroke Rehabil. 2003, 10, 1–7. [Google Scholar] [CrossRef]
- Foley, N.C.; Bhogal, S.K.; Teasell, R.W.; Bureau, Y.; Speechley, M.R. Estimates of quality and reliability with the physiotherapy evidence-based database scale to assess the methodology of randomized controlled trials of pharmacological and nonpharmacological interventions. Phys. Ther. 2006, 86, 817–824. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Bang, D.H.; Song, M.S. The effect of neck pattern of PNF on balance and walking ability in patients with chronic stroke. PNF Mov. 2019, 17, 47–56. [Google Scholar]
- Cheng, K.; Yin, L.C.; Tsai, F.; Hao, S.B. Effect of improved PNF technique on lower limb function of patients with cerebral apoplexy hemiplegia. China Modern Doctor. 2010, 48, 162–163. (In Chinese) [Google Scholar]
- Hwangbo, P.N.; Kyoung, D.K. Effects of proprioceptive neuromuscular facilitation neck pattern exercise on the ability to control the trunk and maintain balance in chronic stroke patients. J. Phys. Ther. Sci. 2016, 28, 850–853. [Google Scholar] [CrossRef] [Green Version]
- Jeong, W.S.; Park, S.K.; Park, J.H.; Lee, H.G.; Kim, K.Y. Effect of PNF combination patterns on muscle activity of the lower extremities and gait ability in stroke patients. J. Korea Cont. Assoc. 2012, 12, 318–328. (In Korean) [Google Scholar] [CrossRef] [Green Version]
- Kim, B.R.; Kang, T.W. The effects of proprioceptive neuromuscular facilitation lower-leg taping and treadmill training on mobility in patients with stroke. Int. J. Rehabil. Res. Int. Z. Fur Rehabil. Rev. Int. De Rech. De Readapt. 2018, 41, 343–348. [Google Scholar] [CrossRef]
- Kim, C.H.; Kim, Y.N. Effects of proprioceptive neuromuscular facilitation and treadmill training on the balance and walking ability of stroke patients. J. Korea Phys. Ther. 2018, 30, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Kim, K.H.; Lee, S.M. Effects of eye movement with PNF neck movement on trunk stability and standing position balance ability of chronic stroke patients. Phys. Med. 2020, 30, 206–213. [Google Scholar] [CrossRef]
- Kim, K.; Lee, D.K.; Jung, S.I. Effect of coordination movement using the PNF pattern underwater on the balance and gait of stroke patients. J. Phys. Ther. Sci. 2015, 27, 3699–3701. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.M.; Kim, Y.M. Effect of both lower extremities proprioceptive neuromuscular facilitation training with functional electrical stimulation on the balance and gait of stroke patient: A randomized controlled trial. Korean Soc. Phys. Med. 2020, 15, 123–132. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, E.J.; Gong, W.T. The effects of trunk stability exercise using PNF on the functional reach test and muscle activities of stroke patients. J. Phys. Ther. Sci. 2011, 23, 699–702. [Google Scholar] [CrossRef] [Green Version]
- Krukowska, J.; Bugajski, M.; Sienkiewicz, M.; Czernicki, J. The influence of NDT-Bobath and PNF methods on the field support and total path length measure foot pressure (COP) in patients after stroke. Neurol. Neurochir. Pol. 2016, 50, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Nam, K.W.; Kim, K.Y.; Yoon, J.W.; Park, J.H. Effect of weight bearing exercise on weight bearing and balance for patients with chronic stroke. J. Korean Soc. Phys. Ther. 2012, 24, 253–261. (In Korean) [Google Scholar]
- Lim, C.G. The effects of proprioceptive neuromuscular facilitation (PNF) pattern exercise using the sprinter and the skater on balance and gait function in the stroke patients. J. Korean Soc. Phys. Ther. 2014, 26, 249–256. (In Korean) [Google Scholar]
- Moon, S.H.; Hong, W.S.; Kim, S.S.; An, H.J.; Song, Y.H.; Kim, Y.K.; Choi, J.H.; Kim, B.K.; Kim, S.H.; Choi, W.S. The impact of functional electrical stimulus and proprioceptive neuromuscular facilitation to scapula adductor on upper limb functions and gait of the patients with stroke. J. Int. Acad. Phys. Ther. Res. 2010, 1, 143–148. [Google Scholar]
- Park, S.E.; Min, K.O.; Lee, S.B.; Choi, W.S.; Kim, S.H. Effect of eye movements and proprioceptive neuromuscular facilitation on balance and head alignment in stroke patients with neglect syndrome. J. Phys. Ther. Sci. 2016, 28, 596–601. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J. The immediate effects of proprioceptive neuromuscular facilitation with taping on gait parameters in patients with chronic stroke. J. Phys. Ther. Sci. 2017, 29, 2018–2021. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, T.; Britto, H.; Oliveira, D.; Silva, E.; Galvao, E.; Lindquist, A. Effects of treadmill training with partial body weight support and the proprioceptive neuromuscular facilitation method on hemiparetic gait: A randomized controlled study. Eur. J. Phys. Rehabil. Med. 2013, 49, 451–461. [Google Scholar]
- Seo, K.C.; Lee, J.H.; Lee, S.Y. Impact of PNF-based walking exercise on a ramp on gait performance of stroke patients. J. Phys. Ther. Sci. 2012, 24, 1243–1246. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, J.; Maitland, M.; Beckstead, J.; Anemaet, W.K. Locomotor training on a treadmill compared with pnf training in adults with chronic stroke. Technol. Innov. 2014, 15, 325–332. [Google Scholar] [CrossRef]
- Downs, S.; Marquez, J.; Chiarelli, P. The Berg Balance Scale has high intra- and inter-rater reliability but absolute reliability varies across the scale: A systematic review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Portnoy, S.; Reif, S.; Mendelboim, T.; Rand, D. Postural control of individuals with chronic stroke compared to healthy participants: Timed-Up-and-Go, Functional Reach Test and center of pressure movement. Eur. J. Phys. Rehabil. Med. 2017, 53, 685–693. [Google Scholar] [CrossRef] [PubMed]
- In, T.S.; Jung, J.H.; Jung, K.S.; Cho, H.Y. Effect of Sit-to-Stand Training Combined with Taping on Spasticity, Strength, Gait Speed and Quality of Life in Patients with Stroke: A Randomized Controlled Trial. Life 2021, 11, 511. [Google Scholar] [CrossRef] [PubMed]
- Shinde, K.; Ganvir, S. Effectiveness of trunk proprioceptive neuromuscular facilitation techniques after stroke: A meta-analysis. Natl. J. Med. Allied. Sci. 2014, 3, 29–34. [Google Scholar]
- Wang, T.J.; Belza, B.; Elaine Thompson, F.; Whitney, J.D.; Bennett, K. Effects of aquatic exercise on flexibility, strength and aerobic fitness in adults with osteoarthritis of the hip or knee. J. Adv. Nurs. 2007, 57, 141–152. [Google Scholar] [CrossRef]
- Rode, G.; Tiliket, C.; Boisson, D. Predominance of postural imbalance in left hemiparetic patients. Scand J. Rehabil. Med. 1997, 29, 11–16. [Google Scholar]
- Espi-Lopez, G.V.; Lopez-Martinez, S.; Ingles, M.; Serra-Ano, P.; Aguilar-Rodriguez, M. Effect of manual therapy versus proprioceptive neuromuscular facilitation in dynamic balance, mobility and flexibility in field hockey players. A randomized controlled trial. Phys. Ther. Sport. 2018, 32, 173–179. [Google Scholar] [CrossRef]
- van Nes, I.J.; Nienhuis, B.; Latour, H.; Geurts, A.C. Posturographic assessment of sitting balance recovery in the subacute phase of stroke. Gait Posture 2008, 28, 507–512. [Google Scholar]
- Manaf, H.; Justine, M.; Omar, M. Functional balance and motor impairment correlations with gait parameters during timed up and go test across three attentional loading conditions in stroke survivors. Stroke Res. Treat. 2014, 2014, 439304. [Google Scholar] [CrossRef]
- Kim, Y.N.; Lee, D.K. Comparison between Aquatic and Ground Environments of Rhythmic Initiation for Postural Control. J. Phys. Ther. Sci. 2012, 24, 1269–1271. [Google Scholar] [CrossRef] [Green Version]
- Dettmann, M.A.; Linder, M.T.; Sepic, S.B. Relationships among walking performance, postural stability, and functional assessments of the hemiplegic patient. Am. J. Phys. Med. 1987, 66, 77–90. [Google Scholar] [PubMed]
- Nardone, A.; Godi, M.; Grasso, M.; Guglielmetti, S.; Schieppati, M. Stabilometry is a predictor of gait performance in chronic hemiparetic stroke patients. Gait Posture 2009, 30, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.Y. Effect of proprioceptive neuromuscular facilitation on the gait of patients with hemiplegia of long and short duration. Phys. Ther. 1994, 74, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Haruyama, K.; Kawakami, M.; Otsuka, T. Effect of core stability training on trunk function, standing balance, and mobility in stroke patients. Neurorehabilit. Neural. Repair. 2017, 31, 240–249. [Google Scholar] [CrossRef] [Green Version]
- Geurts, A.C.; de Haart, M.; van Nes, I.J.; Duysens, J. A review of standing balance recovery from stroke. Gait Posture 2005, 22, 267–281. [Google Scholar] [CrossRef]
- Mayo, N.E.; Wood-Dauphinee, S.; Ahmed, S.; Gordon, C.; Higgins, J.; McEwen, S.; Salbach, N. Disablement following stroke. Disabil. Rehabil. 1999, 21, 258–268. [Google Scholar] [CrossRef]
- Smith, M.T.; Baer, G.D. Achievement of simple mobility milestones after stroke. Arch. Phys. Med. Rehabil. 1999, 80, 442–447. [Google Scholar] [CrossRef]
- Platz, T. Evidence-Based Guidelines and Clinical Pathways in Stroke Rehabilitation-An International Perspective. Front. Neurol. 2019, 10, 200. [Google Scholar] [CrossRef] [Green Version]
- Ghannadi, S.; Shariat, A.; Ansari, N.N.; Tavakol, Z.; Honarpishe, R.; Dommerholt, J.; Noormohammadpour, P.; Ingle, L. The Effect of Dry Needling on Lower Limb Dysfunction in Poststroke Survivors. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2020, 29, 104814. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Term | Keyword |
|---|---|
| #1 Population | “Stroke” OR “Cerebrovascular accident” OR “Cerebrovascular disease” OR “Cerebrovascular disorders” OR “CVA” OR “Hemiplegic” OR “Hemiplegia” |
| #2 Intervention | “Proprioceptive Neuromuscular Facilitation” OR “PNF” OR “Proprioceptive” OR “Neuromuscular Facilitation” |
| #3 Outcomes | “Gait” OR “Walking” OR “Ambulation” OR “Lower extremity” OR “Endurance” OR “Balance” OR “Mobility” OR “Posture” OR “Postural control” |
| #4 Final Search | #1 AND #2 AND #3 |
| Scale Item | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study/Author | Eligibility † | Randomization | Allocation Concealment | Comparison at the Baseline | Blinded Participants | Blinded Therapists | Blinded Evaluators | Adequate Follow-Up | Intention-to-Treat Analysis | Comparisons between Groups | Measures of Precision and Variability | Total Score |
| Bang and Song, 2019 [22] | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | ||||||
| Cheng et al., 2010 [23] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Hwangbo and Kim 2016 [24] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Joeng et al., 2012 [25] | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | ||||||
| Kim and Kim 2018 [26] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 6 | ||||
| Kim and Kang 2018 [27] | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | ||||||
| Kim and Kim, 2020 [28] | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | ||||||
| Kim et al., 2015 [29] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Kim et al., 2020 [30] | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | ||||||
| Kim et al., 2011 [31] | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | ||||||
| Krukowska et al., 2016 [32] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Lee et al., 2012 [33] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Lim 2014 [34] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 6 | ||||
| Moon et al., 2010 [35] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 6 | ||||
| Park et al., 2016 [36] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Park 2017 [37] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 5 | |||||
| Ribeiro et al., 2013 [38] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 7 | |||
| Seo et al., 2012 [39] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 6 | ||||
| Stephenson et al., 2014 [40] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 6 | ||||
| RCT Study Author, Year | Number of Participants (Mean Age in Years) | Grouping and Intervention (Time in Minutes) | Total Sessions (Times/Week) | Outcome Measures | Significant Improvement * |
|---|---|---|---|---|---|
| Bang and Song 2019 [22] | 14 EG: 7 (58.86 ± 6.49) CG: 7 (57.71 ± 6.70) | EG: PNF (20) CG: treadmill (20) # PNF neck pattern | 20 (5 for 4 weeks) | Balance: BBS Gait parameters | BBS and in terms of gait speed, cadence, step length, and double-limb |
| Cheng et al., 2010 [23] | 64 EG: 32 (52.3 ± 9.5) CG: 32 (51.7 ± 10.3) | EG: PNF + CIMT (45) CG: CIMT (30-60) # PNF trunk and limbs, gait patterns with resistance, stretch, rhythmic stability, dynamic reversal | 40 (5 for 8 weeks) | Upper limb function and fine motor evaluation: STEF Gait velocity: 10MWT ADL: MBI | STEF, 10MWT and MBI: EG. |
| Kim et al., 2011 [31] | 40 EG: 20 (51.4 ± 5.7) CG: 20 (53.5 ± 7.1) | EG: PNF (10) + general therapeutic exercise (20) CG: general therapeutic exercise (30) | 30 (5 for 6 weeks) | Trunk stability: FRT Muscle activity: EMG | FRT, activities of soleus and quadriceps: EG |
| #PNFstabilizing reversal and Rhythmic stabilization (sitting, standing) | |||||
| Hwangbo and Kim, 2016 [24] | 30 EG: 15 (59.4 ± 9.1) CG: 15 (55.9 ± 9.8) | EG: PNF (30) + traditional rehabilitation (30) CG: traditional rehabilitation (60) | 30 (5 for 6 weeks) | Trunk control: TIS Balance: BBS | BBS, dynamic sitting, coordination and TIS: EG |
| # PNF neck pattern (sitting) | |||||
| Kim and Kang 2018 [26] | 27 EG: 14 (51.4 ± 2.6) CG: 13 (51.5 ± 2.9) | EG: treadmill with PNF lower-leg taping (30) CG: treadmill with placebo lower-leg taping (30) # PNF flexion–adduction–external rotation pattern | 30 (5 for 6 weeks) | Balance: TUG Walking ability: 10MWT and 6MWT | TUG, 10MWT and 6MWT: EG |
| Kim and Kim 2018 [27] | 23 EG: 12 (60.8 ± 3.1) CG: 11 (60.6 ± 3.4) | EG: PNF (15) + treadmill (15) CG: treadmill training (30) # PNF scapular and pelvic patterns with hold-relax, contract-relax, and dynamic reversal (sidelying) | 30 (5 for 6 weeks) | Balance: TUG Walking ability: 10MWT and 6MWT | TUG, 10MWT and 6MWT: EG |
| Kim and Kim 2020 [28] | 10 EG: 5 (70.61 ± 13.08) CG: 5 (71.00 ± 6.02) | EG: PNF (30) + functional electrical stimulation (30) CG: general physical therapy (30) + functional electrical stimulation (30) #PNF bilateral lower extremity asymmetric flexion/extension patterns | 20 (5 for 4 weeks) | Balance: BBS, TUG Gait parameters | Balance: BBS, TUG Gait Velocity |
| Kim et al., 2015 [29] | 20 EG: 10 (65.9 ± 6.2) CG: 10 (64.1 ± 3.6) | EG: PNF underwater (8) + NDT (30) CG: NDT (30) | 30 (5 for 6 weeks) | Balance: BBS and FRT Gait velocity: 10MWT Gait function: TUG | BBS, FRT, 10MWT and TUG: EG |
| # PNF sprinter and skate patterns (standing, underwater) | |||||
| Kim et al., 2020 [30] | 30 EG: 15 (56.8 ± 3.44) CG: 15 (57.53±3.59) | EG: eye movement (15) + PNF (15) + conservative treatment (30) CG: conservative treatment (60) | 24 (3 for 8 weeks) | Trunk control: TIS Balance: COP, LOS, BBS, FRT | TIS, COP, LOS, BBS, FRT |
| #PNF neck pattern movement training | |||||
| Krukowska et al., 2016 [32] | 72 EG: 34 (52.7 ± 7.5) CG: 39 (52.7 ± 6.3) | EG: PNF † CG: Bobath-NDT † #PNF diagonal and spiral patterns | 36 (6 for 6 weeks) | Balance: force platform (COP of field support and total path length) | Movement of COP: CG |
| Lee et al., 2012 [33] | 27 EG1: 9 (49.1 ± 9.0) EG2: 10 (51.7 ± 17.4) CG1: 9 (44.8 ± 8.6) | EG1: PNF (30) EG2: functional weight bearing exercise (30) CG: general exercise (30) # PNF sprinter pattern (side lying, half standing, modified plantigrade posture) | 12 (3 for 4 weeks) | Weight bearing and static balance capability: FICSIT-4, force platform Dynamic balance: FSST and TUG | FICSIT-4, GBS: EG1, EG2 FSST, TUG: EG1, EG2 |
| Lim 2014 [34] | 22 EG: 11 (55.5 ± 5.4) CG: 11 (56.4 ± 5.7) | EG: PNF (15) + conventional physical therapy (35) CG: conventional physical therapy (50) # PNF pattern sprinter and skater (sitting and half standing) | 20 (5 for 4 weeks) | Balance: FRT and BBS Gait function: TUG | FRT, BBS and TUG: EG |
| Moon et al., 2010 [35] | 15 aPNFG: 5 (49.8 ± 2.9) cPNFG: 5 (53.4 ± 2.5) CG: 5 (52.4 ± 7.1) | aPNFG: PNF (30) cPNFG: PNF (15) + ES (15) CG: ES (30) #PNF scapula + upper limb- combining-isotonic- dynamic reversal (side lying, sitting) | 30 (5 for 6 weeks) | Upper limb functions: MFT Gait velocity: walking distance/minutes Weight bearing: force platform | Upper limb function: aPNFG |
| Park et al., 2016 [36] | 20 EG: 10 (61.1 ± 8.2) CG: 10 (60.2 ± 7.9) | EG: PNF (30 times) + EMP (20 times) † CG: EMP (20 times) † # PNF neck pattern with contract-relax (sitting) | 30 (5 for 6 weeks) | Balance: force platform (Static and dynamic balance: sway length and area with eye open/closed; Dynamic balance: limit of stability with forward/backward and left/right) Head alignment: GPS | Static balance with eye closed: EG Head alignment: EG |
| Park 2017 [37] | 20 aPNFG: 7 (57.3 ± 9.4) cPNFG: 7 (51.7 ± 6.5) CG: 6 (64.8 ± 15.2) | aPNFG: PNF (30) cPNFG: PNF (30) + kinesio taping CG: kinesio taping | 1 | Gait parameters | Cadence, speed, and stride length: cPNFG |
| # PNF sprinter and skater patterns (sitting, standing) | |||||
| Ribeiro et al., 2013 [38] | 20 EG: 9 (58.3 ± 8.9) CG: 11(56.5 ± 8.3) | EG: PNF (30) CG: treadmill with partial body weight support (30) | 12 (4 for 3 weeks) | Motor recovery and basic mobility: STREAM ADL: Motor FIM Gait parameters | Ankle dorsiflexion during swing phase: EG |
| # PNF scapular and pelvic patterns (sidelying, sitting and standing with stretching and maximum resistance) | |||||
| Seo et al., 2012 [39] | 40 EG: 20 (64.1 ± 3.2) CG: 20 (65.8 ± 6.0) | EG: PNF-based walking exercise (30) + general physical therapy (30) CG: general physical therapy (30) + walking exercise (30) | 20 (5 for 4 weeks) | Gait function: temporal, spatial parameters and FAP | All parameters of gait performance and FAP: EG |
| # PNF gait training | |||||
| Stephenson et al., 2014 [40] | 18 EG: 6 (63.3 ± 12.4) CG1: 6 (55.0 ± 9.4) CG2: 6 (63.8 ± 12.2) | EG: PNF gait training (30) CG1: treadmill with body weight support (20) CG2: no interventions # PNF pelvic and lower extremity patterns and gait training | 12 (3 for 4 weeks) | Gait velocity and cadence: 10MWT Gait disability: WGS | Gait velocity and cadence: EG > CG1 WGS total score: EG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, P.T.; Chou, L.-W.; Hsieh, Y.-L. Proprioceptive Neuromuscular Facilitation-Based Physical Therapy on the Improvement of Balance and Gait in Patients with Chronic Stroke: A Systematic Review and Meta-Analysis. Life 2022, 12, 882. https://doi.org/10.3390/life12060882
Nguyen PT, Chou L-W, Hsieh Y-L. Proprioceptive Neuromuscular Facilitation-Based Physical Therapy on the Improvement of Balance and Gait in Patients with Chronic Stroke: A Systematic Review and Meta-Analysis. Life. 2022; 12(6):882. https://doi.org/10.3390/life12060882
Chicago/Turabian StyleNguyen, Phan The, Li-Wei Chou, and Yueh-Ling Hsieh. 2022. "Proprioceptive Neuromuscular Facilitation-Based Physical Therapy on the Improvement of Balance and Gait in Patients with Chronic Stroke: A Systematic Review and Meta-Analysis" Life 12, no. 6: 882. https://doi.org/10.3390/life12060882