
Data Mining Identifies CCN2 and THBS1 as Biomarker Candidates for Cardiac Hypertrophy
by
 ,
,
Markus Johansson
1,2,*,† ,
,
Benyapa Tangruksa
1,*,†, 
Sepideh Heydarkhan-Hagvall
1,3, 
Anders Jeppsson
2,4,
Peter Sartipy
1 and
Jane Synnergren
1 1
Systems Biology Research Center, School of Bioscience, University of Skövde, SE-541 28 Skövde, Sweden
2
Department of Molecular and Clinical Medicine, Institute of Medicine, The Sahlgrenska Academy at University of Gothenburg, SE-413 45 Gothenburg, Sweden
3
Bioscience, Research and Early Development, Cardiovascular, Renal and Metabolism (CVRM), BioPharmaceuticals R&D, AstraZeneca, SE-413 83 Gothenburg, Sweden
4
Department of Cardiothoracic Surgery, Sahlgrenska University Hospital, SE-413 45 Gothenburg, Sweden
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Life 2022, 12(5), 726; https://doi.org/10.3390/life12050726
Submission received: 20 April 2022
/
Revised: 6 May 2022
/
Accepted: 11 May 2022
/
Published: 12 May 2022
(This article belongs to the Special Issue The Molecular Mechanism of Cardiovascular Disease)
Abstract
:Cardiac hypertrophy is a condition that may contribute to the development of heart failure. In this study, we compare the gene-expression patterns of our in vitro stem-cell-based cardiac hypertrophy model with the gene expression of biopsies collected from hypertrophic human hearts. Twenty-five differentially expressed genes (DEGs) from both groups were identified and the expression of selected corresponding secreted proteins were validated using ELISA and Western blot. Several biomarkers, including CCN2, THBS1, NPPA, and NPPB, were identified, which showed significant overexpressions in the hypertrophic samples in both the cardiac biopsies and in the endothelin-1-treated cells, both at gene and protein levels. The protein-interaction network analysis revealed CCN2 as a central node among the 25 overlapping DEGs, suggesting that this gene might play an important role in the development of cardiac hypertrophy. GO-enrichment analysis of the 25 DEGs revealed many biological processes associated with cardiac function and the development of cardiac hypertrophy. In conclusion, we identified important similarities between ET-1-stimulated human-stem-cell-derived cardiomyocytes and human hypertrophic cardiac tissue. Novel putative cardiac hypertrophy biomarkers were identified and validated on the protein level, lending support for further investigations to assess their potential for future clinical applications.
1. Introduction
Cardiac hypertrophy is a condition in which the heart muscle thickens as an adaptive response to several stimuli. When stimulated, cardiomyocytes (CMs) increase in size and cause an enlargement of the heart [1], which can be further categorized into physiological or pathological cardiac hypertrophy. Physiological hypertrophy occurs naturally by exercise, pregnancy, or puberty [2,3,4]. This type of hypertrophy is generally harmless and reversible. On the other hand, prolonged pathological cardiac hypertrophy can lead to heart failure and severe cardiovascular disease. The development of pathological cardiac hypertrophy is associated with aortic stenosis, gene mutations, chronic hypertension, neurohormonal stimulation, and physical stretching [5,6]. The heart increases in size and is unable to pump blood effectively due to the remodeling of several pathways that affect the morphology and function of the heart. The characteristics of pathological cardiac hypertrophy include an increase in glucose consumption by the CMs, an increase in natriuretic peptide protein production, and an aberrant gene-expression profile [7,8,9].
To study cardiac hypertrophy in vitro, model systems of high quality and high human relevance are needed. We and others have reported on the development of hypertrophic disease models based on human-induced pluripotent stem-cell-derived CMs (hiPSC-CMs), which provides advantages in terms of high throughput and high translatability of the results [10,11,12].
To induce hypertrophy in hiPSC-CMs, endothelin 1 (ET-1) stimulation or stretch stimulation was applied [10,13,14,15,16]. ET-1 is a neurohormone that contributes to the thickening of heart muscles by stimulating receptors that couple to the heterotrimeric G-protein. The stimulation results in the activation of downstream signaling pathways that lead to an increase in catalytic activities and trigger hypertrophic conditions [15]. ET-1 stimulation in cell cultures increases the size of the CMs and increases the lactate levels due to higher glucose consumption. It also results in elevated levels of A- and B-type natriuretic peptides (ANP and BNP) [10,11,16,17], which are characteristics of pathological cardiac hypertrophy.
The similarities between in vitro cardiac hypertrophy models and the in vivo conditions in human hypertrophic hearts are of high importance for the translational relevance of the models. Aggarwal et al. (2014) previously reported on a comparative study of differentially expressed genes (DEGs) in human myocardial biopsies from patients with aortic stenosis-induced left ventricular hypertrophy with DEGs of an ET-1 stimulated hiPSC-CMs hypertrophic model using a principal component analysis approach. Their heart biopsies were obtained from patients with cardiac hypertrophy with different levels of ejection fractions (EFs). Interestingly, a large number of genes with similarities in expression changes in all hypertrophic samples were identified [12]. However, further analysis of the correlations between mRNA profiles of in vitro cardiac hypertrophy models and corresponding in vivo cardiac tissue is needed.
In the present study, we compare the overlap of DEGs identified in data from our in vitro hiPSC-CM hypertrophy model [14] and compare this to the transcriptional data from patient cardiac biopsies to identify biomarkers for the diagnosis and monitoring of cardiac hypertrophy. Several candidates were identified and some of these were selected for further validation of protein levels.
2. Materials and Methods
2.1. Transcriptomics Datasets from In Vitro and In Vivo Experiments
Gene-expression data from hypertrophic hiPSC-CMs [10] were used in this study. Briefly, the hypertrophic response was induced in the hiPSC-CMs by ET-1 stimulation (10 nM). Every 24 h, fresh medium containing ET-1 was added to the hiPSC-CMs. RNA-seq was carried out in triplicates on the ET-1-stimulated and -untreated cells after 8, 24, 48, 72, and 96 h, respectively. Johansson et al. reported that 93% of CMs were positive for the cardiac specific marker cardiac troponin T [10]. In the study, DEGs were identified by the quasi-likelihood F-test using the edgeR package. DEGs with a false discovery rate (FDR) ≤ 0.05 and an absolute fold change (FC) value of ≤2 were considered as differentially expressed. We combined the identified DEGs from all time points in our downstream analysis. The raw and processed RNA-seq datasets are accessible at ArrayExpress (https://www.ebi.ac.uk/arrayexpress/, accessed on 4 April 2022); accession number: E-MTAB-8548.
To investigate the correlations between the in vitro hypertrophy model and corresponding human hypertrophic cardiac tissue, data from myocardial left ventricular biopsy samples from a publicly available microarray dataset [12] were analyzed. This dataset contained two experimental groups and one control group. The experimental groups were left ventricular samples from male patients with aortic stenosis and noticeable left ventricular hypertrophy, in which EF was classified as normal (EF > 50%, n = 3) or low (EF < 30%, n = 3). The control biopsies were collected from male patients with coronary disease, but without a hypertrophic phenotype and with normal EF (>60%, n = 3). The RNA isolated from biopsies was analyzed using Affymetrix HG-U133A and U133B microarrays. This microarray data is accessible at ArrayExpress (https://www.ebi.ac.uk/arrayexpress/, accessed on 4 April 2022); accession number: E-MEXP-2296.
2.2. Differentially Expressed Genes in Biopsies from Cardiac Hypertrophic Biopsies
The gene-expression data from the cardiac biopsies [12] was analyzed to identify DEGs using the Miodin R package [18]. The background filtering threshold was set to six to remove low-expressed transcripts. The background filtering threshold was selected based on the average expression value of pluripotency marker genes (LIN28A, NANOG, PF4, and POU5F1), which are not expected to be expressed in differentiated cells [19,20]. The normalized data from U133A GeneChip contained 22,283 features. After the background filtering, 16,017 and 16,047 features remained for low and normal EF samples, respectively. For the U133B GeneChip, the normalized data contained 22,645 features. After the background expression filtering, 12,339 and 12,293 features remained for low and normal EF samples, respectively. The genes with an absolute log2FC of >1 and FDR ≤ 0.05 were considered as statistically significant. The DEGs identified from low and normal EF samples were combined for downstream analysis.
2.3. Functional Annotation Analysis of Differentially Expressed Genes Using IPA
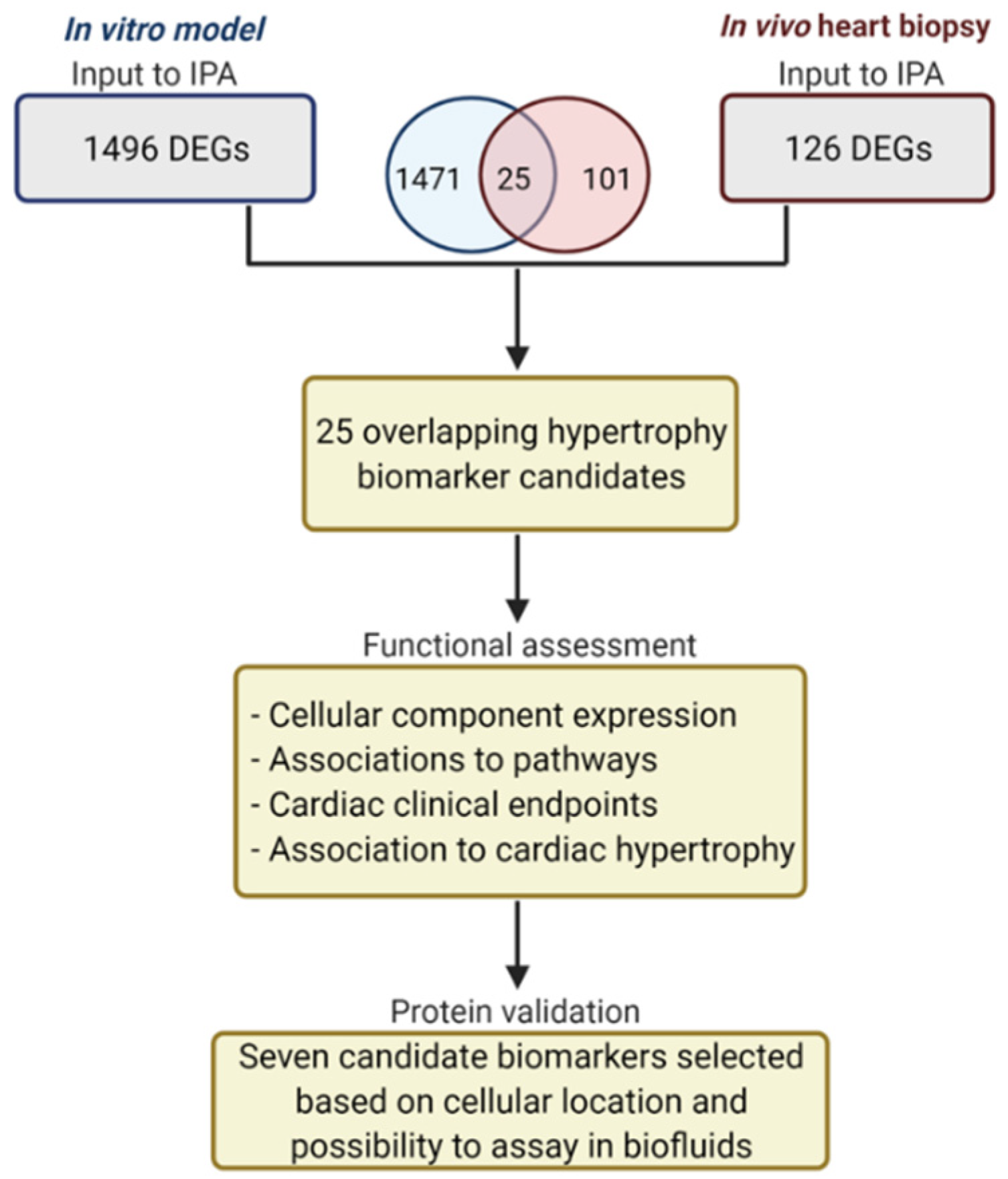
The DEGs from all samples were uploaded to IPA for functional annotation. Duplicates and ambiguous transcripts that represented multiple loci or genes were removed. In total, 1496 unique DEGs from the in vitro data and 126 unique DEGs from the in vivo cardiac biopsies data were analyzed with the use of Ingenuity Pathway Analysis (IPA) software (QIAGEN Inc., Redwood City, CA, USA, https://digitalinsights.qiagen.com/IPA). In total, 25 overlapping DEGs between the heart biopsies and the cardiac stem-cell-based model were identified. The Core Analysis and Tox functions in IPA were applied for a functional assessment of the biomarkers and their subcellular locations, cardiac clinical endpoints, associated pathways, and significant cardiac hypertrophy associations (p ≤ 0.05) were identified. The pathways associated with more than two DEGs were reported in this analysis. Based on the subcellular locations and detectability, seven upregulated genes, for which corresponding proteins are secreted into the extracellular space and are detectable in biofluids, were selected for further protein validation. Figure 1 shows the workflow for candidate biomarker identification, functional assessment, and the protein-validation process.
2.4. Protein Validation of Selected Cardiac Hypertrophy Candidates
For the analysis of the secreted proteins, conditioned media were collected in triplicates and centrifuged (300× g, 3 min) to remove potential cell debris, and stored at −80 °C. ELISA was used to measure the concentration of ANP (cat EIAANP, ThermoFisher Scientific, Waltham, MA, USA), proBNP (cat EHPRONPPB, ThermoFisher Scientific), and CCN2 (CTGF) (cat ab261851, Abcam, Cambridge, United Kingdom), according to the manufacturer’s instructions. Due to difficulties of analyzing THBS1 and NES using ELISA, quantitative Western blot was employed for those specific proteins.
A more detailed description is included in the Supplementary Materials (Supplementary file S1). In short, the prepared samples were loaded onto a NuPAGE™ 4–12% Bis-Tris Gels (Invitrogen, Waltham, MA, USA). Wells were loaded with either 15 µL of sample-mix per well or 2 µL of the Precision Plus Protein Dual Color Standards (Bio-Rad laboratories, Inc., Hercules, CA, USA). The SDS PAGE ran at 200 V for 45 min. The proteins were transferred to an Immobilon-FL PVDF membrane (Merck Millipore, Ltd., Burlington, MA, USA) and blotted. The membranes were then incubated with the specific primary antibodies overnight. Next, membranes were transferred to a blocking buffer containing the secondary antibody, and incubated for 1 h at room temperature. The membranes were imaged with an Oddyssey CLx (Li-Cor, Inc., Lincoln, NE, USA) and the band strength was assessed using Image Studio Lite (Li-Cor, Inc.).
2.5. Protein-Network Analysis
The protein–protein interaction network analysis was performed using Cytoscape (v3.9.1) [21] with the STRING plugin (v1.7.0). The list of 25 overlapping DEGs was used as input and imported into Cytoscape. The minimum interaction score for the analysis was set to medium (0.4). Proteins with more than five interactions with other proteins were identified as hub proteins.
2.6. Gene Ontology Enrichment Analysis
The 25 DEGs were analyzed for enriched terms using STRING enrichment functions in the Cytoscape software and visualized using EnrichmentMAP (v3.3.3). The results were filtered to only include significantly enriched Gene Ontology (GO) biological processes (BPs). The significant threshold was set to p < 0.05.
3. Results
3.1. Transcriptomic Analysis of In Vitro and In Vivo Data
Using a combined criteria of FDR < 0.05 and absolute log2 fold change (abs(log2FC)) > 1, we identified a total of 1998 DEGs combining all the timepoints from the in vitro data, and 212 DEGs combining low and normal EF from the in vivo data. Out of these, 1496 and 126 were unique DEGs within the in vitro and in vivo data, respectively. As shown in the Venn diagram in Figure 1, 25 DEGs overlapped between the in vitro and in vivo data (Table 1). A detailed list of the 25 genes (FDR ≤ 0.05, abs(log2FC) > 1) is shown in Table A1 and Table A2.
3.2. Functional Assessment of the 25 DEGs
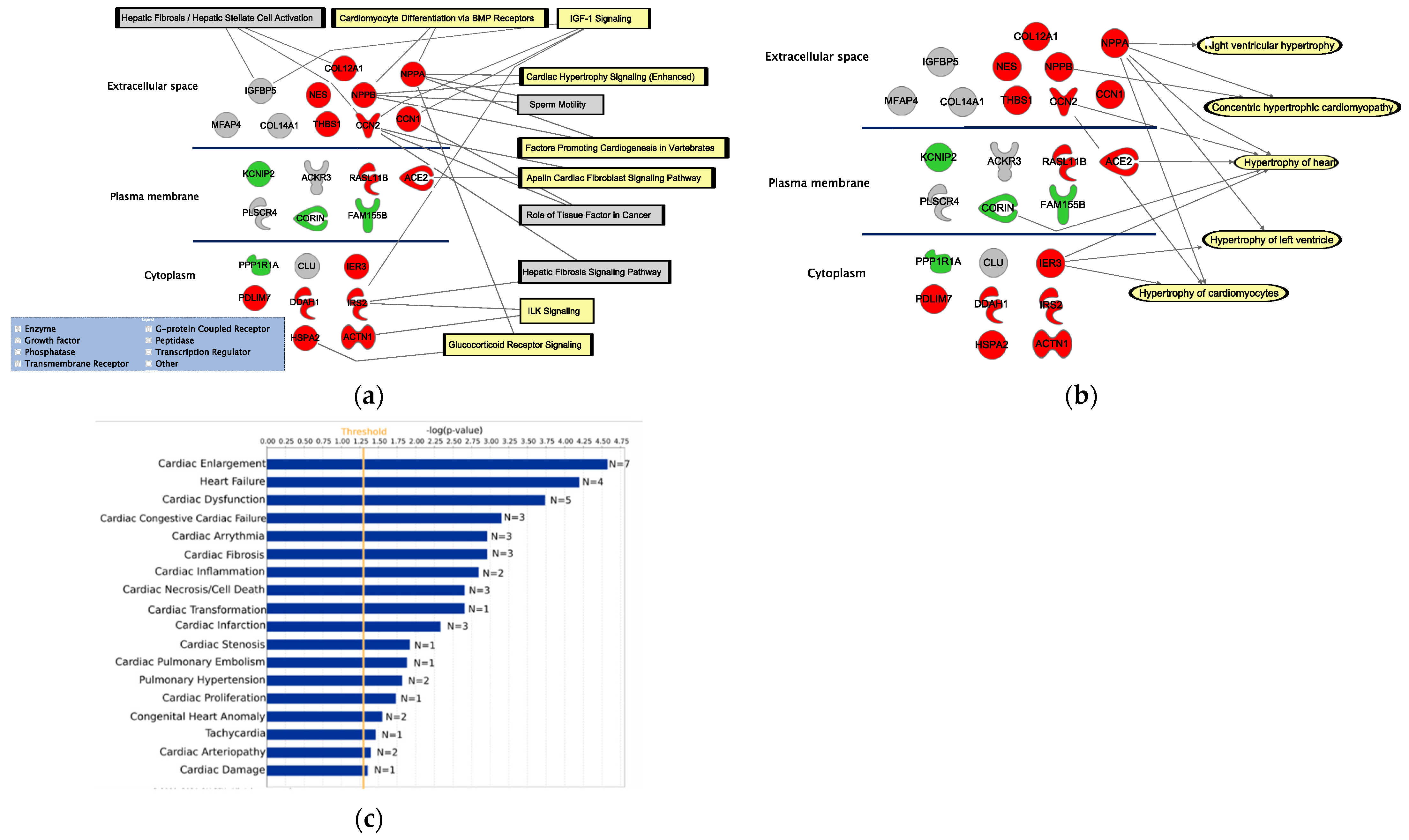
The corresponding proteins from the 25 DEGs were expressed in different cellular locations, including the extracellular space, the plasma membrane, and cytoplasm (Figure 2a,b). Relevant pathways associated with more than one of these genes are, for example, ‘Cardiomyocyte differentiation via bmp receptors’, ‘IGF-1 signaling’, ‘Cardiac hypertrophy signaling (enhanced)’, ‘Factor promoting cardiogenesis in vertebrates’, ‘Apelin cardiac fibroblast signaling pathway’, ‘ILK signaling’, and ‘Glucoticoid receptor signaling’. Five significant hypertrophy pathways were identified to be associated with the DEGs, including ‘Right ventricular hypertrophy’ (p = 4.31 × 10−2), ‘Concentric hypertrophic cardiomyopathy’ (p = 4.15 × 10−7), ‘Hypertrophy of the heart’ (p = 1.06 × 10−4), ‘Hypertrophy of the left ventricle’ (p = 4.95 × 10−3), and ‘Hypertrophy of cardiomyocytes’ (p = 6.07 × 10−4).
In this paper, we report on several novel DEGs, including IGFB5, MFAP4, COL14A1, COL12A1, NES, THBS1, CCN1, KCNIP2, ACKR3, RASL1B, PLSCR4, FAM155B, PPP1RA, CLU, PDLIM7, DDAH1, IRS2, HSPA2, and ACTN1. The association of these genes to any of the five hypertrophy pathways has not been shown before.
Using the IPA’s Tox function tool, we were able to significantly link 18 cardiac clinical pathology endpoints to the 25 overlapping DEGs (Figure 2c). Interestingly, the cardiac endpoint with the highest number of genes from our list of candidate hypertrophy biomarkers is the ‘Cardiac enlargement’ (p = 2.65 × 10−5, n = 7).
3.3. Protein Validation of the Selected DEGs
Seven of the DEGs were selected for protein validation, including CCN1, CCN2, COL12A1, NES, NPPA, NPPB, and THBS1. The selected candidates show upregulated gene expression levels in both in vivo and in vitro data. They were detected in biofluids, and are known to be secreted into the extracellular space.
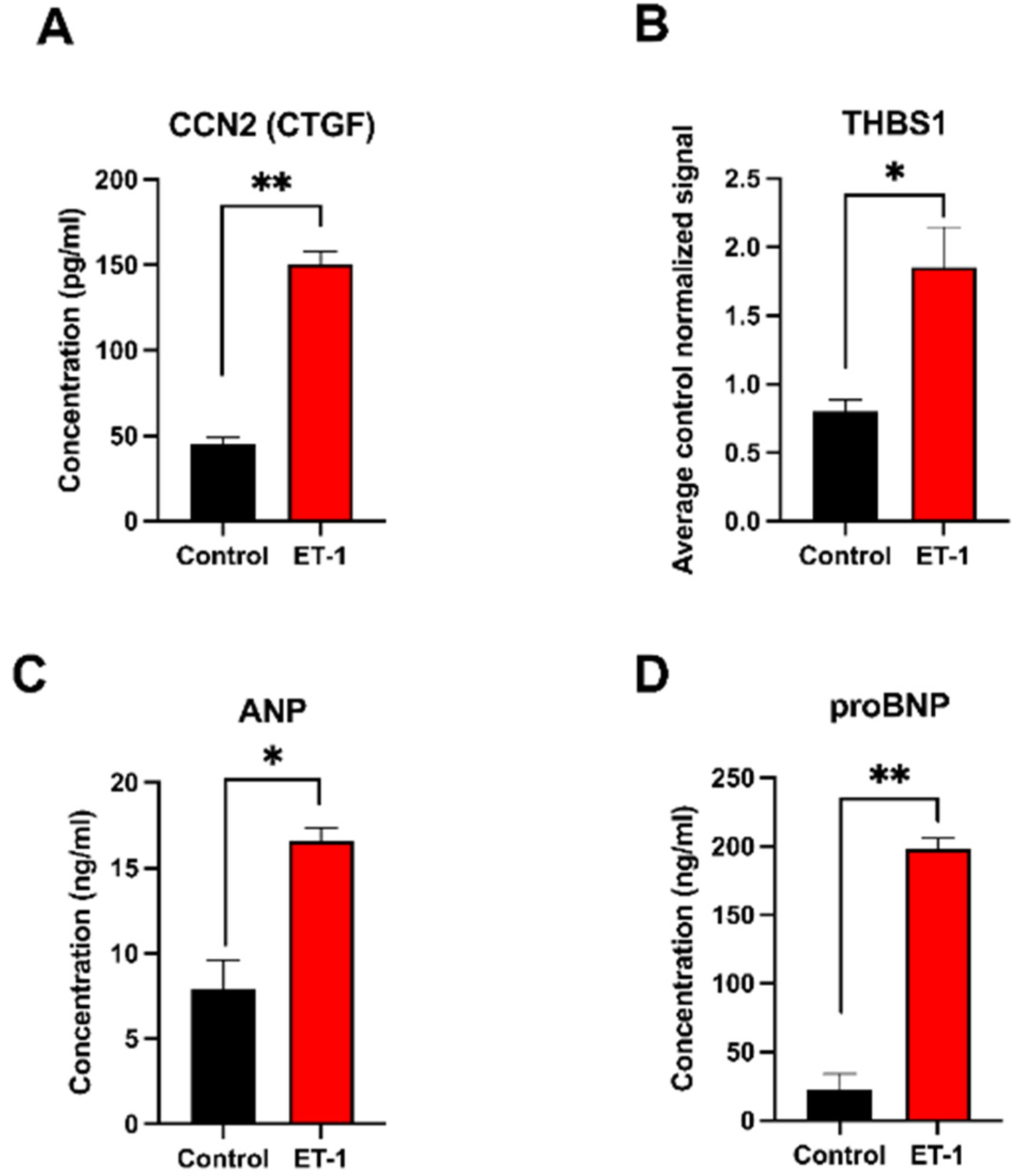
The protein ‘Cellular Communication Network Factor 2’ (CCN2/CTGF) is known to be induced in heart failure and showed upregulation in the hypertrophic samples in both the in vitro and in vivo data. The protein analysis of the conditioned media from the in vitro samples showed a more than 3-fold increase in CCN2/CTGF (FC = 3.3, p = 0.0032) in the cultures stimulated with ET-1 for 24 h (150.5 ng/mL vs. 45.1 ng/mL) (Figure 3A). The gene expression data showed comparable results with a 3-fold upregulation at 24 h (Table A1).
Thrombospondin 1, which is a glycoprotein that is involved in cell–cell and cell–matrix interactions, was first analyzed with the ELISA method, but due to difficulties in detecting a signal, a quantitative Western blot analysis was performed instead. The results showed a significant 2.3-fold increase at 24 h (p = 0.02) (Figure 3B and Figure S1). From the gene expression data, a significant upregulation was also observed at 24 h (FC = 2.2) (Table A1).
The natriuretic proteins ANP and proBNP, known markers for cardiac hypertrophy, were both upregulated significantly in the ET-1 stimulated cultures. The ANP level in ET-1 induced sample was more than 2-fold (p = 0.006) higher compared to the control at 24 h (Figure 3C). A much higher concentration of proBNP (>9-fold (p = 0.002)) was detected in ET-1-stimulated samples compared to the controls at 24 h (Figure 3D).
No proteins of CCN1, COL12A1, and NES were detected using ELISA or Western blot (data not shown).
3.4. Protein Interaction Network Analysis
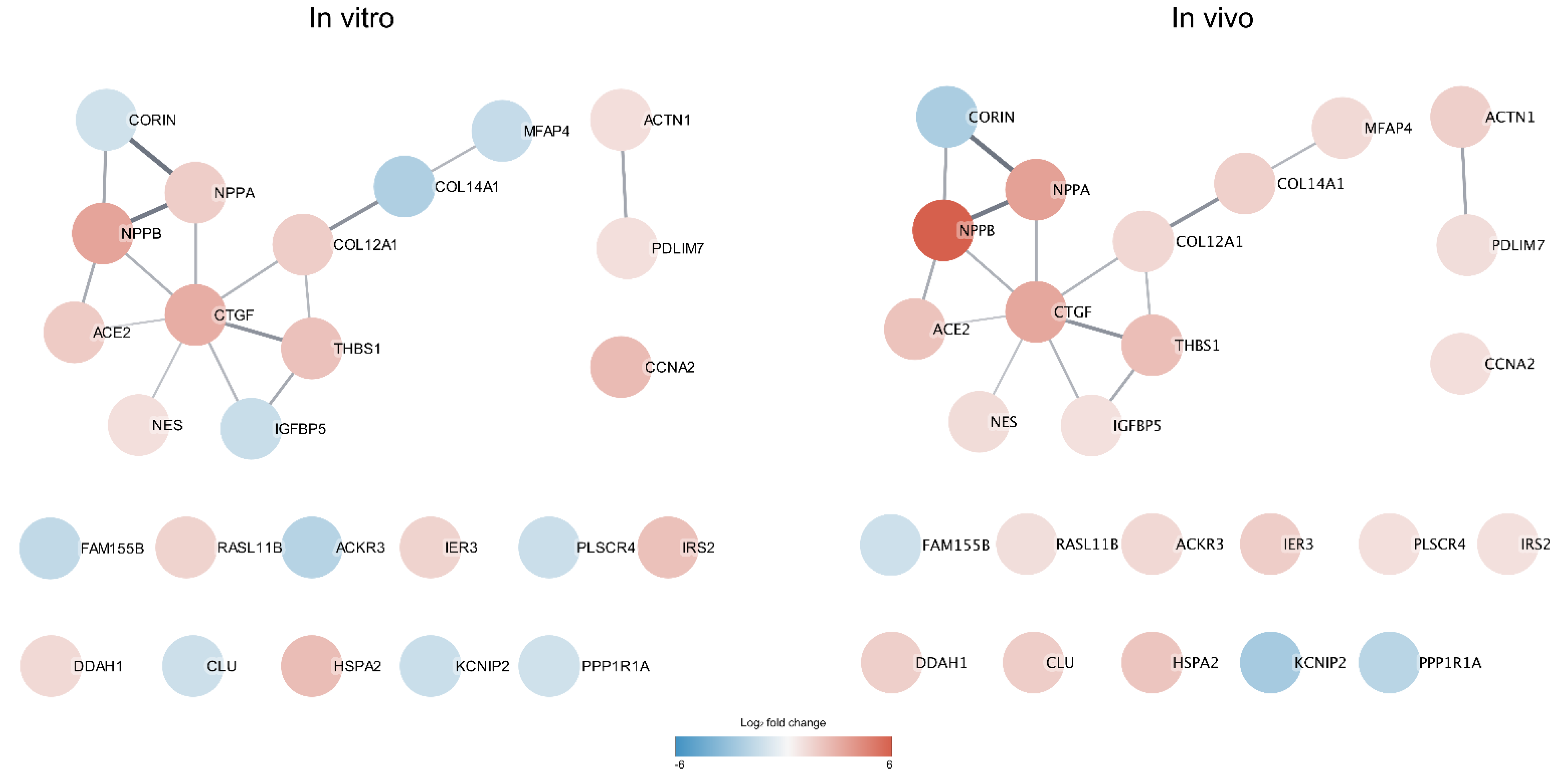
A STRING protein–protein interaction (PPI) network analysis was performed to investigate any known protein interactions among the 25 DEGs identified from intersecting the in vitro and in vivo data. The PPI enrichment shows that the derived network has significantly more interactions than what is expected by random analysis (p-value 6.34 × 10−7). Interestingly, CCN2/CTGF protein was detected as the central hub node in the network with seven interactions to other differentially expressed gene products. The color of the nodes indicates the magnitude of the log2FC differences in gene expression. High similarities in FC magnitude between the control and hypertrophic samples in both the in vitro and in vivo data were observed. This suggests that the hypertrophic response in the in vitro model mimics to a high degree the hypertrophic response of CMs in vivo. However, some genes, e.g., IGFBP5, COL14A1, MFAP4, ACKR3, PLSCR4, and CLU, show a conflicting differential expression direction in the in vitro and in vivo data (Figure 4).
3.5. Gene Ontology (GO) Enrichment Analysis
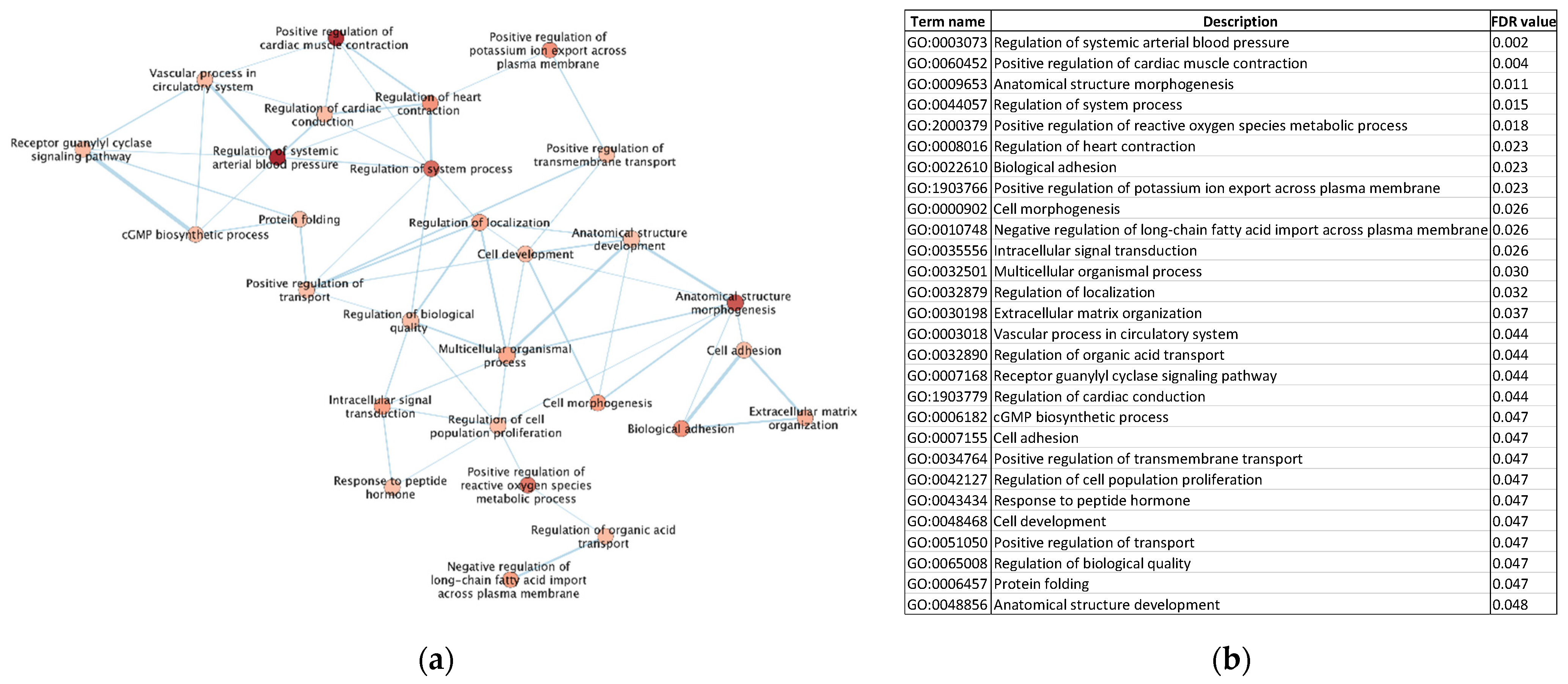
The GO enrichment analysis was performed to explore enriched biological process (BP) terms identified for the 25 DEGs. In total, 28 GO-BP terms were significantly enriched. The five most enriched terms were ‘Regulation of systemic arterial blood pressure’, ‘Positive regulation of cardiac muscle contraction’, ‘Anatomical structure morphogenesis’, ‘Regulation of system process’, and ‘Positive regulation of reactive oxygen species metabolic process’. All the enriched terms are visualized in Figure 5.
4. Discussion
In this study, we identified candidate cardiac hypertrophy biomarkers that show significant differential expression both in an hiPSC-CM hypertrophy in vitro model and in human hypertrophic heart biopsies. We utilized published transcriptomic data from Aggarwal et al. (2014) and Johansson et al. (2020). Johansson et al. performed transcriptional characterization of an in vitro hypertrophy model in their study, and Aggarwal et al. compared mRNA expressions using PCA on overlapping DEGs to highlight differences between in vitro and in vivo data. In the present study, we further analyzed these datasets, but now focused on identifying similarities instead of differences between the in vitro model and in vivo data. The overlapping DEGs were further validated on a protein level. These results provide novel data, showing how the stem-cell-based hypertrophy model mimics the hypertrophy of the heart.
Supporting our findings, previously known biomarkers of hypertrophy, such as NPPA and NPPB, also showed a significant differential expression in our datasets. In this paper, we identified and validated two potential cardiac hypertrophy markers, CCN2/CTGF and THBS1.
The PPI analysis identified CCN2/CTGF, which encodes for the protein ‘connective tissue growth factor’, as a central hub node, indicating an important role in the progression of cardiac hypertrophy. The gene expression of CCN2/CTGF was also found to be highly upregulated in both the in vitro and in vivo data. Moreover, the corresponding protein was also significantly upregulated in the conditioned media from the ET-1-treated hiPSC-CMs. Increased levels of CCN2/CTGF have also been observed in conditions such as myocardial infarction, hypertension, and diabetes [22,23,24]. Combining that information with its known profibrotic properties makes it a plausible contributor to the development and progression of cardiac hypertrophy. ET-1 stimulation of rat CMs has previously been shown to upregulate CCN2/CTGF. Additionally, it has been shown that direct treatment by CCN2/CTGF protein stimulates the hypertrophic growth of the cells in rat CMs. However, the expression of known hypertrophic markers, such as BNP and ACTA1, were not elevated under these conditions due to the modulation of different signaling pathways compared to the ET-1 stimulation of CMs, suggesting that CCN2/CTGF protein alone is not sufficient to induce the pathological form of cardiac hypertrophy [25].
There are several studies indicating the role of CCN2/CTGF protein as a biomarker for cardiovascular diseases and report that plasma levels of CCN2/CTGF protein correlate with the plasma levels of the known hypertrophy marker BNP in patients with heart failure. It has also been suggested that CCN2/CTGF protein could be a biomarker for comparing the severeness of heart failure [26,27,28]. Moreover, a recent study comparing patients that underwent septal myectomy due to cardiac hypertrophy to structurally normal hearts that were harvested following non-cardiac-related deaths showed that CCN2/CTGF was significantly upregulated and appeared to be a key mediator of myocardial fibrosis [29]. This study supports the potential role of CCN2/CTGF as a biomarker of cardiac hypertrophy.
The THBS1 gene encodes for a binding glycoprotein thrombospondin 1 (TSP-1). It is associated with angiogenesis, cell migration, and cardiac remodeling, which are hallmarks of cardiac hypertrophy. The TSP-1 protein has been shown to be both pro- and anti-angiogenic [30,31,32]. It has also been shown that THBS1 promotes follicular angiogenesis and hypertrophic scar fibroblasts [33,34]. The overexpression of TSP-1 induces lethal cardiac atrophy (a reduction in heart muscle mass) in mice, and the TSP-1 knocked-out mice develop a severe cardiac hypertrophy during the stimulation [35]. In contrast, we found that THBS1 is overexpressed in both the cell-based hypertrophy model and in the cardiac biopsies from patients with cardiac hypertrophy. These results highlight the differences in the cardiovascular system in animals and in humans and suggest that the development of a relevant in vitro model that represents the mechanism of cardiac hypertrophy in humans is of great importance. The TSP family has several functional domains that interact with different proteins and receptors. TSP-1 is pro-angiogenic when interacting with α9β1 integrin [30], but notably, the opposite effect occurs when it interacts with CD36 and CD47 [31,32]. The expression of TSPs increases under cardiac stress [36] and results from a study on canine and murine models showed that the elevation of TSP-1 during myocardial injury helps to protect the heart and prevent the expansion of infarctions [37]. Another study suggests that the increase in TSP-2 (an important paralog of TSP-1) is a sign of cardiac hypertrophy that is prone to develop into heart failure [38].
In an animal disease model of hypertrophic cardiomyopathy with a significant enlargement of the left ventricle and severe heart failure, it was shown that both THBS1 and CCN2/CTGF were significantly upregulated in the diseased condition [39]. The analysis of THBS1 and CCN2/CTGF in both CMs and non-CM isolated from the mice showed that there was an upregulation of CCN2/CTGF in both CMs and non-CMs. However, for THBS1, the upregulation was only observed in the CMs but not in the non-CMs population. This result is in line with another study, for which the results suggest that CMs accounts for the upregulation of the THBS1-CD47 axis in left ventricular heart failure [40]. CCN2/CTGF was also analyzed on a protein level, and the results showed a plasma level more than double when compared to the control mice. Interestingly, it was shown that treating neonatal ventricular cardiomyocytes (NVCM) with recombinant CCN2/CTGF protein resulted in a rapid upregulation of THBS1 [39].
We identified THBS1 as a biomarker candidate for cardiac hypertrophy, since it is overexpressed in both the hiPSC-based hypertrophy model and in biopsies from patients with cardiac hypertrophy. Little is known about the potential role of THBS1 in cardiac hypertrophy and more research on the interactions between THBS1 and the different receptors and the mechanism underpinning the TSP protein expression is required to provide a better understanding of the role of TSP-1 in cardiac hypertrophy and cardiovascular diseases.
The NPPA and NPPB genes are established cardiac hypertrophy biomarkers. These paralog genes encode natriuretic peptide cardiac hormones, the ANP and BNP proteins. They mediate cardiovascular homeostasis through the regulation of natriuresis, diuresis, vasorelaxation, and renin inhibition [41,42,43,44]. ANP and BNP are highly expressed during the development of the ventricles, but strongly downregulated after birth [45,46,47]. Studies show a reactivation of the two hormones in ventricular CMs during heart failure and cardiac hypertrophy [45,48,49,50]. These two genes were upregulated in both the in vitro ET-1-induced cardiac hypertrophy model and in the hypertrophic heart biopsies. In our in vitro model, NPPA was upregulated at all time points during ET-1 stimulation, while the NPPB was upregulated at 8 h, 24 h, and 72 h (but not at 48 h and 96 h). In the in vivo heart biopsy data, the NPPA and NPPB genes were upregulated only in the hypertrophic hearts with a low EF. This suggests that NPPA and NPPB become more relevant at the later stage of cardiac hypertrophy. Further investigations on the characteristics of cardiac hypertrophy and the progression of this severe condition are still needed to further refine the disease models.
The network analysis of the overlapping 25 DEGs that were significantly upregulated in hypertrophic samples showed interesting interaction patterns, and of specific note is that CCN2/CTGF was identified as a hub protein in the network with interactions for seven of the other 25 DEGs. This supports the fact that CCN2/CTGF is an important protein in cardiac hypertrophy development and likely of high relevance for benchmarking hypertrophy progression.
The GO analysis also revealed that most of the enriched terms are of high relevance to cardiac hypertrophy development and indicates that data from the in vitro model reflect the in vivo model in important aspects. It was also confirmed in the cardiac clinical endpoint analysis, which found cardiac enlargement as the most significant endpoint. The expression profiles of several hypertrophy genes, such as NPPA and NPPB, are highly similar for both in vitro and in vivo data. The in vivo data used in this study were generated using the Affymetrix microarray platform with predefined probes, which, to some extent, limited the possibilities to identify novel transcripts. For future studies, it would be of interest to analyze data from patient biopsies using the RNA-seq technology, which can identify novel transcripts and allow for a better comparison with the in vitro model. Additionally, blood samples from patients with cardiac hypertrophy would be important to include in future studies to verify if the suggested candidate biomarkers are detectable in blood samples of patients with cardiac hypertrophy. Despite the current limitations, the results from this study demonstrate that in vitro models of cardiac hypertrophy have a great potential to be effective tools for novel drug-screening approaches and for the development of novel therapies for the treatment of cardiovascular diseases.
5. Conclusions
The differential expression comparison between the hiPSC-CM-based in vitro model and hypertrophic cardiac biopsies allows potential cardiac hypertrophy biomarkers to be identified and validated. The functional enrichment analysis and the PPI analysis revealed that the overlapping 25 DEGs were associated with cardiac functions and cardiac hypertrophy. Most of the overlapping genes were differentially expressed in the same direction in the in vivo and in vitro samples, except for six genes (ACKR3, CLU, COL14A1, IGFBP5, MFAP4, and PLSCR4), which were downregulated in the in vitro model but upregulated in the hypertrophic cardiac biopsies. In the study, CCN2/CTGF and THBS1 were identified as interesting candidate cardiac hypertrophy biomarkers that are expressed in both the ET-1-induced cardiac hypertrophy in vitro model and the hypertrophic cardiac biopsies at both gene and protein levels. Additional research is needed to be able to reveal the specific roles of the identified biomarkers in cardiac hypertrophy and to validate their potential applications in a clinical setting.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/life12050726/s1, Material and methods, Western blot analysis.
Author Contributions
Conceptualization, P.S., S.H.-H., A.J. and J.S.; methodology, B.T., M.J., S.H.-H., P.S. and J.S.; formal analysis, B.T. and M.J.; investigation, P.S., S.H.-H., A.J. and J.S.; resources, J.S.; data curation, M.J. and B.T.; writing—original draft preparation, B.T., M.J. and J.S.; writing—review and editing, B.T., M.J., S.H.-H., P.S., J.S. and A.J.; visualization, M.J., B.T. and J.S.; supervision, A.J., P.S. and J.S.; funding acquisition, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Systems Biology Research Centre at the University of Skövde under grants from the Knowledge Foundation (20160294, 20160330, 20200014), Takara Bio Europe, Gothenburg, Sweden, and AstraZeneca R&D, Gothenburg.
Institutional Review Board Statement
The commercially available cell line used in this study was obtained in accordance with the Declaration of Helsinki, and was approved by the Ethics Committee, Comité de Protection des Personnes IIe de France XI, number 11 015, on 3 March 2011.
Informed Consent Statement
Not applicable.
Data Availability Statement
This study is based on two trancriptomics datasets, which are available for download at ArrayExpress (https://www.ebi.ac.uk/arrayexpress/, accessed on 4 April 2022) accession numbers: E-MTAB-11030 and E-MEXP-2296.
Acknowledgments
The graphical abstract was created with BioRender software. The networks and functional analyses were generated through the use of IPA (Qiagen Inc., https://www.qiagenbioinformatics.com/products/ingenuity-pathway-analysis, accessed on 1 March 2022).
Conflicts of Interest
P.S. and S.H. are employees at AstraZeneca. The other authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
log2 FC from the in vitro data of the 25 significant overlapping DEGs.
| Gene Symbol | 8 h | 24 h | 48 h | 72 h | 96 h |
|---|---|---|---|---|---|
| ACE2 | 1.831 | 1.358 | 1.432 | ||
| ACKR3 | −1.116 | −1.738 | −1.119 | ||
| ACTN1 | 1.066 | ||||
| CCN1 | 2.431 | 1.053 | |||
| CCN2 | 2.999 | 1.568 | |||
| CLU | −1.066 | −1.125 | |||
| COL12A1 | 1.335 | 1.745 | 1.299 | 1.255 | 1.259 |
| COL14A1 | −1.938 | −1.661 | −1.557 | ||
| CORIN | −1.033 | ||||
| DDAH1 | 1.283 | ||||
| FAM155B | −1.419 | ||||
| HSPA2 | 1.997 | 2.369 | 1.101 | ||
| IER3 | 1.517 | 1.182 | |||
| IGFBP5 | −1.235 | ||||
| IRS2 | 2.218 | ||||
| KCNIP2 | −1.186 | ||||
| MFAP4 | −1.098 | −1.228 | −1.305 | −1.166 | |
| NES | 1.053 | ||||
| NPPA | 1.048 | 1.754 | 1.517 | 1.025 | 1.208 |
| NPPB | 3.334 | 2.903 | 1.082 | ||
| PDLIM7 | 1.031 | ||||
| PLSCR4 | −1.162 | ||||
| PPP1R1A | −1.039 | ||||
| RASL11B | 1.524 | 1.174 | |||
| THBS1 | 2.204 | 1.118 |
Appendix B
Table A2.
log2 FC from the in vitro data of the 25 significant overlapping DEGs.
| Gene Symbol | Normal EF | Low EF |
|---|---|---|
| ACE2 | 2.145 | |
| ACKR3 | 1.407 | 1.203 |
| ACTN1 | 1.662 | |
| CCN1 | 1.09 | |
| CCN2 | 3.25 | 3.225 |
| CLU | 1.74 | |
| COL12A1 | 1.36 | |
| COL14A1 | 1.86 | 1.381 |
| CORIN | −2.035 | |
| DDAH1 | 1.511 | 1.843 |
| FAM155B | −1.073 | |
| HSPA2 | 1.754 | 2.355 |
| IER3 | 1.747 | |
| IGFBP5 | 1.002 | |
| IRS2 | 1.001 | |
| KCNIP2 | −2.177 | |
| MFAP4 | 1.284 | |
| NES | 1.173 | |
| NPPA | 3.459 | |
| NPPB | 5.987 | |
| PDLIM7 | 1.108 | |
| PLSCR4 | 1.059 | |
| PPP1R1A | −1.637 | −1.659 |
| RASL11B | 1.094 | |
| THBS1 | 2.329 |
References
- Frey, N.; Katus, H.A.; Olson, E.N.; Hill, J.A. Hypertrophy of the heart: A new therapeutic target? Circulation 2004, 109, 1580–1589. [Google Scholar] [CrossRef] [Green Version]
- Pluim, B.M.; Zwinderman, A.H.; van der Laarse, A.; van der Wall, E.E. The athlete's heart. A meta-analysis of cardiac structure and function. Circulation 2000, 101, 336–344. [Google Scholar] [CrossRef] [Green Version]
- Eghbali, M.; Deva, R.; Alioua, A.; Minosyan, T.Y.; Ruan, H.; Wang, Y.; Toro, L.; Stefani, E. Molecular and functional signature of heart hypertrophy during pregnancy. Circ. Res. 2005, 96, 1208–1216. [Google Scholar] [CrossRef] [Green Version]
- Janz, K.F.; Dawson, J.D.; Mahoney, L.T. Predicting heart growth during puberty: The Muscatine Study. Pediatrics 2000, 105, E63. [Google Scholar] [CrossRef] [Green Version]
- Badiani, S.; van Zalen, J.; Treibel, T.A.; Bhattacharyya, S.; Moon, J.C.; Lloyd, G. Aortic Stenosis, a Left Ventricular Disease: Insights from Advanced Imaging. Curr. Cardiol. Rep. 2016, 18, 80. [Google Scholar] [CrossRef] [Green Version]
- Marian, A.J. Genetic determinants of cardiac hypertrophy. Curr. Opin. Cardiol. 2008, 23, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Frey, N.; Olson, E.N. Cardiac hypertrophy: The good, the bad, and the ugly. Annu. Rev. Physiol. 2003, 65, 45–79. [Google Scholar] [CrossRef]
- Almeida, P.; Azevedo, A.; Rodrigues, R.; Dias, P.; Frioes, F.; Vazquez, B.; Abreu-Lima, C.; Bettencourt, P.; Barros, H. B-type natriuretic peptide and left ventricular hypertrophy in hypertensive patients. Rev. Port. Cardiol. 2003, 22, 327–336. [Google Scholar]
- Kolwicz, S.C., Jr.; Tian, R. Glucose metabolism and cardiac hypertrophy. Cardiovasc. Res. 2011, 90, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Johansson, M.; Ulfenborg, B.; Andersson, C.X.; Heydarkhan-Hagvall, S.; Jeppsson, A.; Sartipy, P.; Synnergren, J. Cardiac hypertrophy in a dish: A human stem cell based model. Biol. Open 2020, 9, bio052381. [Google Scholar] [CrossRef]
- Carlson, C.; Koonce, C.; Aoyama, N.; Einhorn, S.; Fiene, S.; Thompson, A.; Swanson, B.; Anson, B.; Kattman, S. Phenotypic screening with human iPS cell-derived cardiomyocytes: HTS-compatible assays for interrogating cardiac hypertrophy. J. Biomol. Screen 2013, 18, 1203–1211. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, P.; Turner, A.; Matter, A.; Kattman, S.J.; Stoddard, A.; Lorier, R.; Swanson, B.J.; Arnett, D.K.; Broeckel, U. RNA expression profiling of human iPSC-derived cardiomyocytes in a cardiac hypertrophy model. PLoS ONE 2014, 9, e108051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LaBarge, W.; Mattappally, S.; Kannappan, R.; Fast, V.G.; Pretorius, D.; Berry, J.L.; Zhang, J. Maturation of three-dimensional, hiPSC-derived cardiomyocyte spheroids utilizing cyclic, uniaxial stretch and electrical stimulation. PLoS ONE 2019, 14, e0219442. [Google Scholar] [CrossRef]
- Johansson, M.; Ulfenborg, B.; Andersson, C.X.; Heydarkhan-Hagvall, S.; Jeppsson, A.; Sartipy, P.; Synnergren, J. Multi-Omics Characterization of a Human Stem Cell-Based Model of Cardiac Hypertrophy. Life 2022, 12, 293. [Google Scholar] [CrossRef]
- Bupha-Intr, T.; Haizlip, K.M.; Janssen, P.M. Role of endothelin in the induction of cardiac hypertrophy in vitro. PLoS ONE 2012, 7, e43179. [Google Scholar] [CrossRef] [Green Version]
- Jen, H.L.; Yin, W.H.; Chen, J.W.; Lin, S.J. Endothelin-1-Induced Cell Hypertrophy in Cardiomyocytes is Improved by Fenofibrate: Possible Roles of Adiponectin. J. Atheroscler. Thromb. 2017, 24, 508–517. [Google Scholar] [CrossRef] [Green Version]
- Dai, C.; Li, Q.; May, H.I.; Li, C.; Zhang, G.; Sharma, G.; Sherry, A.D.; Malloy, C.R.; Khemtong, C.; Zhang, Y.; et al. Lactate Dehydrogenase A Governs Cardiac Hypertrophic Growth in Response to Hemodynamic Stress. Cell Rep. 2020, 32, 108087. [Google Scholar] [CrossRef]
- Ulfenborg, B. Vertical and horizontal integration of multi-omics data with miodin. BMC Bioinform. 2019, 20, 649. [Google Scholar] [CrossRef] [Green Version]
- Ohashi, F.; Miyagawa, S.; Yasuda, S.; Miura, T.; Kuroda, T.; Itoh, M.; Kawaji, H.; Ito, E.; Yoshida, S.; Saito, A.; et al. CXCL4/PF4 is a predictive biomarker of cardiac differentiation potential of human induced pluripotent stem cells. Sci. Rep. 2019, 9, 4638. [Google Scholar] [CrossRef]
- Bharathan, S.P.; Manian, K.V.; Aalam, S.M.; Palani, D.; Deshpande, P.A.; Pratheesh, M.D.; Srivastava, A.; Velayudhan, S.R. Systematic evaluation of markers used for the identification of human induced pluripotent stem cells. Biol. Open 2017, 6, 100–108. [Google Scholar] [CrossRef] [Green Version]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.S.; Øie, E.; Vinge, L.E.; Yndestad, A.; Øystein Andersen, G.; Andersson, Y.; Attramadal, T.; Attramadal, H. Connective tissue growth factor--a novel mediator of angiotensin II-stimulated cardiac fibroblast activation in heart failure in rats. J. Mol. Cell. Cardiol. 2004, 36, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.M.; Lam, A.; Abraham, J.A.; Schreiner, G.F.; Joly, A.H. CTGF expression is induced by TGF- beta in cardiac fibroblasts and cardiac myocytes: A potential role in heart fibrosis. J. Mol. Cell. Cardiol. 2000, 32, 1805–1819. [Google Scholar] [CrossRef]
- Way, K.J.; Isshiki, K.; Suzuma, K.; Yokota, T.; Zvagelsky, D.; Schoen, F.J.; Sandusky, G.E.; Pechous, P.A.; Vlahos, C.J.; Wakasaki, H.; et al. Expression of connective tissue growth factor is increased in injured myocardium associated with protein kinase C beta2 activation and diabetes. Diabetes 2002, 51, 2709–2718. [Google Scholar] [CrossRef] [Green Version]
- Hayata, N.; Fujio, Y.; Yamamoto, Y.; Iwakura, T.; Obana, M.; Takai, M.; Mohri, T.; Nonen, S.; Maeda, M.; Azuma, J. Connective tissue growth factor induces cardiac hypertrophy through Akt signaling. Biochem. Biophys. Res. Commun. 2008, 370, 274–278. [Google Scholar] [CrossRef]
- Koitabashi, N.; Arai, M.; Niwano, K.; Watanabe, A.; Endoh, M.; Suguta, M.; Yokoyama, T.; Tada, H.; Toyama, T.; Adachi, H.; et al. Plasma connective tissue growth factor is a novel potential biomarker of cardiac dysfunction in patients with chronic heart failure. Eur. J. Heart Fail. 2008, 10, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Koitabashi, N.; Arai, M.; Kogure, S.; Niwano, K.; Watanabe, A.; Aoki, Y.; Maeno, T.; Nishida, T.; Kubota, S.; Takigawa, M.; et al. Increased Connective Tissue Growth Factor Relative to Brain Natriuretic Peptide as a Determinant of Myocardial Fibrosis. Hypertension 2007, 49, 1120–1127. [Google Scholar] [CrossRef] [Green Version]
- Gerritsen, K.G.; Falke, L.L.; van Vuuren, S.H.; Leeuwis, J.W.; Broekhuizen, R.; Nguyen, T.Q.; de Borst, G.J.; Nathoe, H.M.; Verhaar, M.C.; Kok, R.J.; et al. Plasma CTGF is independently related to an increased risk of cardiovascular events and mortality in patients with atherosclerotic disease: The SMART study. Growth Factors 2016, 34, 149–158. [Google Scholar] [CrossRef]
- Patel, V.; Syrris, P.; Coats, C.; Lucena, J.; Lara-Pezzi, E.; Garcia-Pavia, P.; Elliott, P.M. Genetic regulation of myocardial fibrosis in hypertrophic cardiomyopathy. Eur. Heart J. 2021, 42, ehab724.1778. [Google Scholar] [CrossRef]
- Staniszewska, I.; Zaveri, S.; Del Valle, L.; Oliva, I.; Rothman, V.L.; Croul, S.E.; Roberts, D.D.; Mosher, D.F.; Tuszynski, G.P.; Marcinkiewicz, C. Interaction of alpha9beta1 integrin with thrombospondin-1 promotes angiogenesis. Circ. Res. 2007, 100, 1308–1316. [Google Scholar] [CrossRef] [Green Version]
- Dawson, D.W.; Pearce, S.F.; Zhong, R.; Silverstein, R.L.; Frazier, W.A.; Bouck, N.P. CD36 mediates the In vitro inhibitory effects of thrombospondin-1 on endothelial cells. J. Cell Biol. 1997, 138, 707–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, S.; Martin-Manso, G.; Pendrak, M.L.; Garfield, S.H.; Isenberg, J.S.; Roberts, D.D. Thrombospondin-1 inhibits VEGF receptor-2 signaling by disrupting its association with CD47. J. Biol. Chem. 2010, 285, 38923–38932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bender, H.R.; Campbell, G.E.; Aytoda, P.; Mathiesen, A.H.; Duffy, D.M. Thrombospondin 1 (THBS1) Promotes Follicular Angiogenesis, Luteinization, and Ovulation in Primates. Front. Endocrinol. 2019, 10, 727. [Google Scholar] [CrossRef] [Green Version]
- Jiang, D.; Guo, B.; Lin, F.; Hui, Q.; Tao, K. Effect of THBS1 on the Biological Function of Hypertrophic Scar Fibroblasts. Biomed Res. Int. 2020, 2020, 8605407. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, D.; Schips, T.G.; Vo, A.; Grimes, K.M.; Baldwin, T.A.; Brody, M.J.; Accornero, F.; Sargent, M.A.; Molkentin, J.D. Thbs1 induces lethal cardiac atrophy through PERK-ATF4 regulated autophagy. Nat. Commun. 2021, 12, 3928. [Google Scholar] [CrossRef]
- Schellings, M.W.; van Almen, G.C.; Sage, E.H.; Heymans, S. Thrombospondins in the heart: Potential functions in cardiac remodeling. J. Cell Commun. Signal 2009, 3, 201–213. [Google Scholar] [CrossRef] [Green Version]
- Frangogiannis, N.G.; Ren, G.; Dewald, O.; Zymek, P.; Haudek, S.; Koerting, A.; Winkelmann, K.; Michael, L.H.; Lawler, J.; Entman, M.L. Critical role of endogenous thrombospondin-1 in preventing expansion of healing myocardial infarcts. Circulation 2005, 111, 2935–2942. [Google Scholar] [CrossRef] [Green Version]
- Schroen, B.; Heymans, S.; Sharma, U.; Blankesteijn, W.M.; Pokharel, S.; Cleutjens, J.P.; Porter, J.G.; Evelo, C.T.; Duisters, R.; van Leeuwen, R.E.; et al. Thrombospondin-2 is essential for myocardial matrix integrity: Increased expression identifies failure-prone cardiac hypertrophy. Circ. Res. 2004, 95, 515–522. [Google Scholar] [CrossRef] [Green Version]
- Tsoutsman, T.; Wang, X.; Garchow, K.; Riser, B.; Twigg, S.; Semsarian, C. CCN2 plays a key role in extracellular matrix gene expression in severe hypertrophic cardiomyopathy and heart failure. J. Mol. Cell. Cardiol. 2013, 62, 164–178. [Google Scholar] [CrossRef]
- Sharifi-Sanjani, M.; Shoushtari, A.H.; Quiroz, M.; Baust, J.; Sestito, S.F.; Mosher, M.; Ross, M.; McTiernan, C.F.; St. Croix, C.M.; Bilonick, R.A.; et al. Cardiac CD47 Drives Left Ventricular Heart Failure Through Ca2+-CaMKII-Regulated Induction of HDAC3. J. Am. Heart Assoc. 2014, 3, e000670. [Google Scholar] [CrossRef] [Green Version]
- Pandey, K.N. Biology of natriuretic peptides and their receptors. Peptides 2005, 26, 901–932. [Google Scholar] [CrossRef] [PubMed]
- Rubattu, S.; Bigatti, G.; Evangelista, A.; Lanzani, C.; Stanzione, R.; Zagato, L.; Manunta, P.; Marchitti, S.; Venturelli, V.; Bianchi, G.; et al. Association of atrial natriuretic peptide and type a natriuretic peptide receptor gene polymorphisms with left ventricular mass in human essential hypertension. J. Am. Coll. Cardiol. 2006, 48, 499–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishimoto, I.; Tokudome, T.; Nakao, K.; Kangawa, K. Natriuretic peptide system: An overview of studies using genetically engineered animal models. FEBS J. 2011, 278, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- von Lueder, T.G.; Sangaralingham, S.J.; Wang, B.H.; Kompa, A.R.; Atar, D.; Burnett, J.C., Jr.; Krum, H. Renin-angiotensin blockade combined with natriuretic peptide system augmentation: Novel therapeutic concepts to combat heart failure. Circ. Heart Fail. 2013, 6, 594–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, K.R.; Knowlton, K.U.; Zhu, H.; Chien, S. Regulation of cardiac gene expression during myocardial growth and hypertrophy: Molecular studies of an adaptive physiologic response. FASEB J. 1991, 5, 3037–3046. [Google Scholar] [CrossRef] [PubMed]
- Cameron, V.A.; Aitken, G.D.; Ellmers, L.J.; Kennedy, M.A.; Espiner, E.A. The sites of gene expression of atrial, brain, and C-type natriuretic peptides in mouse fetal development: Temporal changes in embryos and placenta. Endocrinology 1996, 137, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Houweling, A.C.; Somi, S.; Massink, M.P.; Groenen, M.A.; Moorman, A.F.; Christoffels, V.M. Comparative analysis of the natriuretic peptide precursor gene cluster in vertebrates reveals loss of ANF and retention of CNP-3 in chicken. Dev. Dyn. 2005, 233, 1076–1082. [Google Scholar] [CrossRef]
- Goetze, J.P.; Bruneau, B.G.; Ramos, H.R.; Ogawa, T.; de Bold, M.K.; de Bold, A.J. Cardiac natriuretic peptides. Nat. Rev. Cardiol. 2020, 17, 698–717. [Google Scholar] [CrossRef]
- Sergeeva, I.A.; Hooijkaas, I.B.; Ruijter, J.M.; van der Made, I.; de Groot, N.E.; van de Werken, H.J.; Creemers, E.E.; Christoffels, V.M. Identification of a regulatory domain controlling the Nppa-Nppb gene cluster during heart development and stress. Development 2016, 143, 2135–2146. [Google Scholar] [CrossRef] [Green Version]
- Man, J.C.K.; van Duijvenboden, K.; Krijger, P.H.L.; Hooijkaas, I.B.; van der Made, I.; de Gier-de Vries, C.; Wakker, V.; Creemers, E.E.; de Laat, W.; Boukens, B.J.; et al. Genetic Dissection of a Super Enhancer Controlling the Nppa-Nppb Cluster in the Heart. Circ. Res. 2021, 128, 115–129. [Google Scholar] [CrossRef]
Figure 1.
Overview of the candidate hypertrophy biomarker identification and validation process.

Figure 2.
Functional assessment of the 25 DEGs. (a) Pathways associated with two or more of the DEGs (pathways associated with the hypertrophy condition are in yellow). Red represents DEGs that are upregulated in both in vitro and in vivo data and green represents downregulated. Grey indicates that the DEGs are regulated in the opposite direction in the in vivo and in vitro data. (b) Association of the DEGs to cardiac hypertrophy. (c) Association of the DEGs to cardiac clinical endpoints.
Figure 2.
Functional assessment of the 25 DEGs. (a) Pathways associated with two or more of the DEGs (pathways associated with the hypertrophy condition are in yellow). Red represents DEGs that are upregulated in both in vitro and in vivo data and green represents downregulated. Grey indicates that the DEGs are regulated in the opposite direction in the in vivo and in vitro data. (b) Association of the DEGs to cardiac hypertrophy. (c) Association of the DEGs to cardiac clinical endpoints.

Figure 3.
Differentially expressed proteins in the conditioned media analyzed with ELISA and Western blot after 24 h of ET-1 stimulation. (A) Concentration of the CCN2 (CTGF) protein. Y-axis shows the concentration in pg/mL. (B) Expression levels of the THBS1 protein at 24 h measured with quantitative Western blot. The Y-axis shows the average control normalized signal (representing expression level). (C,D) Concentration of the ANP and proBNP proteins, respectively. Y-axis shows the concentration in ng/mL. Standard deviation (SD) is shown as error bars (n = 3); * = p < 0.05; ** = p < 0.01.
Figure 3.
Differentially expressed proteins in the conditioned media analyzed with ELISA and Western blot after 24 h of ET-1 stimulation. (A) Concentration of the CCN2 (CTGF) protein. Y-axis shows the concentration in pg/mL. (B) Expression levels of the THBS1 protein at 24 h measured with quantitative Western blot. The Y-axis shows the average control normalized signal (representing expression level). (C,D) Concentration of the ANP and proBNP proteins, respectively. Y-axis shows the concentration in ng/mL. Standard deviation (SD) is shown as error bars (n = 3); * = p < 0.05; ** = p < 0.01.

Figure 4.
STRING protein–protein interaction network (PPI) was generated by importing the 25 overlapping DEGs between the in vitro and in vivo data into Cytoscape and the STRING plugin. The lines between the proteins indicate an interaction. The thicker the line is, the more confident is the evidence for this interaction between the proteins. The color of the proteins indicates the FC levels observed in the in vitro (left PPI network) and in vivo data (right PPI network). Red colors represent upregulation and blue colors represent downregulation.
Figure 4.
STRING protein–protein interaction network (PPI) was generated by importing the 25 overlapping DEGs between the in vitro and in vivo data into Cytoscape and the STRING plugin. The lines between the proteins indicate an interaction. The thicker the line is, the more confident is the evidence for this interaction between the proteins. The color of the proteins indicates the FC levels observed in the in vitro (left PPI network) and in vivo data (right PPI network). Red colors represent upregulation and blue colors represent downregulation.

Figure 5.
Gene Ontology (GO) enrichment map. (a) The 25 overlapping DEGs were analyzed for enriched GO terms (Biological Process (BP)). The color of the circles, representing a GO-BP term, corresponds to the p-value (FDR). The thickness of the lines between terms indicates how closely related the terms are to each other. The thicker the line, the more closely related. (b) A table with the FDR-values of the terms in the GO enrichment map in (a).
Figure 5.
Gene Ontology (GO) enrichment map. (a) The 25 overlapping DEGs were analyzed for enriched GO terms (Biological Process (BP)). The color of the circles, representing a GO-BP term, corresponds to the p-value (FDR). The thickness of the lines between terms indicates how closely related the terms are to each other. The thicker the line, the more closely related. (b) A table with the FDR-values of the terms in the GO enrichment map in (a).

Table 1.
The 25 overlapping DEGs were significantly differentially expressed (FDR ≤ 0.05, abs(log2FC) > 1) in both the in vitro and in vivo hypertrophy datasets. This table shows their detectability in biofluids and their expression levels in the in vitro models and in the hypertrophic cardiac biopsies. Each square represents an upregulated ( ![Life 12 00726 i001]() ), downregulated (
), downregulated ( ![Life 12 00726 i002]() ), or non-differentially expressed gene (
), or non-differentially expressed gene ( ![Life 12 00726 i003]() ) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).
) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).
 ), downregulated (
), downregulated (  ), or non-differentially expressed gene (
), or non-differentially expressed gene (  ) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).
) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).
Table 1.
The 25 overlapping DEGs were significantly differentially expressed (FDR ≤ 0.05, abs(log2FC) > 1) in both the in vitro and in vivo hypertrophy datasets. This table shows their detectability in biofluids and their expression levels in the in vitro models and in the hypertrophic cardiac biopsies. Each square represents an upregulated ( ![Life 12 00726 i001]() ), downregulated (
), downregulated ( ![Life 12 00726 i002]() ), or non-differentially expressed gene (
), or non-differentially expressed gene ( ![Life 12 00726 i003]() ) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).
) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).
), downregulated ( ), or non-differentially expressed gene ( ) at the different time points (8, 24, 48, 72, and 96 h; n = 3 each) in the in vitro samples and in the cardiac samples with a normal EF (n = 3) or low EF (n = 3).| Gene Symbol | Blood | Plasma/Serum | Urine | Not Detected in Biofluids | In Vitro Expression (8–96 h) | In Vivo Expression (Normal and Low EF) |
|---|---|---|---|---|---|---|
| ACE2 | x | | | |||
| ACKR3 | x | x | | | ||
| ACTN1 | x | x | x | | | |
| CCN1 | x | x | | | ||
| CCN2 | x | x | | | ||
| CLU | x | x | x | | | |
| COL12A1 | x | | | |||
| COL14A1 | x | | | |||
| CORIN | x | | | |||
| DDAH1 | x | | | |||
| FAM155B | x | x | | | ||
| HSPA2 | x | | | |||
| IER3 | x | | | |||
| IGFBP5 | x | x | x | | | |
| IRS2 | x | x | | | ||
| KCNIP2 | x | | | |||
| MFAP4 | x | | | |||
| NES | x | x | | | ||
| NPPA | x | x | | | ||
| NPPB | x | x | | | ||
| PDLIM7 | x | | | |||
| PLSCR4 | x | | | |||
| PPP1R1A | x | | | |||
| RASL11B | x | | | |||
| THBS1 | x | x | x | | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Johansson, M.; Tangruksa, B.; Heydarkhan-Hagvall, S.; Jeppsson, A.; Sartipy, P.; Synnergren, J. Data Mining Identifies CCN2 and THBS1 as Biomarker Candidates for Cardiac Hypertrophy. Life 2022, 12, 726. https://doi.org/10.3390/life12050726
AMA Style
Johansson M, Tangruksa B, Heydarkhan-Hagvall S, Jeppsson A, Sartipy P, Synnergren J. Data Mining Identifies CCN2 and THBS1 as Biomarker Candidates for Cardiac Hypertrophy. Life. 2022; 12(5):726. https://doi.org/10.3390/life12050726
Chicago/Turabian StyleJohansson, Markus, Benyapa Tangruksa, Sepideh Heydarkhan-Hagvall, Anders Jeppsson, Peter Sartipy, and Jane Synnergren. 2022. "Data Mining Identifies CCN2 and THBS1 as Biomarker Candidates for Cardiac Hypertrophy" Life 12, no. 5: 726. https://doi.org/10.3390/life12050726
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.