1. Introduction
Cardiovascular diseases (CVD) are estimated to be responsible for 31% of all deaths worldwide [
1]. Cardiac hypertrophy is, in its pathological form, irreversible and is initially a process where the heart is compensating for an increased workload, commonly due to extrinsic pathological stimuli, such as myocardial infarction, aortic stenosis, chronic hypertension, or other conditions, that alter the homeostasis of the heart [
2]. In order to increase the quality of life and outcomes for affected patients, new and improved treatment options are needed.
To investigate the changes that occur during the development of cardiac hypertrophy, in vitro models based on human pluripotent stem cells offer an attractive alternative. In the past decade, the availability of human-induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) with high similarity to bona fide CMs has increased rapidly [
3,
4,
5,
6]. Several strategies to induce hypertrophy in hiPSC-CMs have also been developed using neurohormonal stimulation- or stretch-induced methods [
7,
8,
9]. Endothelin-1 (ET-1) is frequently used in neurohormonal models and has been shown to induce hypertrophy within 24 h [
10,
11,
12]. ET-1 binds to G-protein coupled receptors, which downstream leads to the activation and production of inositol-1.4.5-triphosphate (IP
3), resulting in the release of intracellular calcium (Ca
2+). The release of intracellular Ca
2+ has been shown to mediate hypertrophic signaling via the calcineurin-NFAT pathway and potentially through other signaling pathways [
13,
14]. ET-1 stimulation is also an inducer of MAPK signaling, which is involved in CM cell growth [
15]. Although these in vitro models have provided important knowledge about mechanistic aspects of cardiac hypertrophy, additional characterization is needed to support their further use as relevant disease models [
16].
Two well-known protein markers altered in cardiac hypertrophy are ANP and BNP. These proteins are natriuretic peptides that are secreted from CMs in response to the stretching of the myocardium [
17]. They both lower vascular tone and cardiac output as well as regulate blood volume through inhibition of aldosterone synthesis and renin secretion [
18]. There are also specific signaling pathways that are involved in cell growth, cytoskeleton remodeling, fibrosis, and metabolism that are altered during the development of cardiac hypertrophy [
19,
20,
21,
22,
23]. With translatable in vitro models, we can expand our knowledge of the molecular regulation of cardiac hypertrophy and identify novel multimodal biomarkers that can aid in the early detection of the disease.
RNA sequencing (RNA-seq) analysis has become less expensive and more standardized over the past decade and is ideal for studying the whole transcriptome and for the investigation of individual genes as well as groups of genes. It provides a snapshot of all transcribed genes in a sample and can reveal underlying mechanisms associated with cellular phenotype or function.
Recent advances in proteomic technologies have facilitated the identification of biomarkers in the secretome using high-throughput affinity proteomics, which can be used for the detection of proteins in serum, plasma, and conditioned cell culture media [
24]. Using this method, it is possible to quantify the proteins that are secreted by the CMs and subsequently identify their possible associations with cardiac hypertrophy. Moreover, the identification of novel multimodal biomarkers that can detect early signs of cardiac hypertrophy would also be more approachable. A major advantage of this technique over mass spectrometry is that it requires very low sample volume, and it can be applied using fluids with a high content of albumin, such as cell culture media, which has been a limitation for other methods [
25].
In this study, we used hiPSC-CMs stimulated with ET-1 as a model system to explore changes in gene- and secreted protein expression. We used RNA-seq and high-throughput affinity proteomics together with ELISA to characterize the hypertrophic response of ET-1 stimulation in the cells. Moreover, Ingenuity Pathway Analysis (IPA) was applied to analyze altered canonical pathways, cardiac effects, and predicted upstream regulators based on the differentially expressed genes (DEGs).
4. Discussion
In this study, we have used a cell-based model of cardiac hypertrophy by stimulating hiPSC-derived CMs with ET-1 and characterized the response on transcriptome and secretome levels. The results were in line with previous studies and provided further insights into the molecular machinery underlying the initiation and development of cardiac hypertrophy [
10,
11,
30]. Our results illustrated that known cardiac hypertrophy genes were differentially expressed in our model and signaling pathways that are important in a hypertrophic response were enriched in the ET-1 stimulated cultures. Our analysis of secreted proteins also showed that there were several key proteins associated with cardiac hypertrophy that were differentially expressed in our model, and potential new candidate biomarkers or putative drug targets were identified.
hiPSC-derived CMs have been used for the development of several in vitro disease models [
31,
32,
33]. They have shown to be promising for studies of cardiac hypertrophy, with characteristics resembling the in vivo situation. For example, we and others have previously reported that the hiPSC-derived CMs increase in size, have altered metabolism, and a transcriptional pattern indicative of hypertrophy when exposed to substances such as ET-1 and phenylephrine [
10,
11,
12]. Although information is still lacking regarding the optimal maturation stage of the CMs for use in a hypertrophy model, our results demonstrated that cells cultured for at least 20 days produce a robust hypertrophic response [
10].
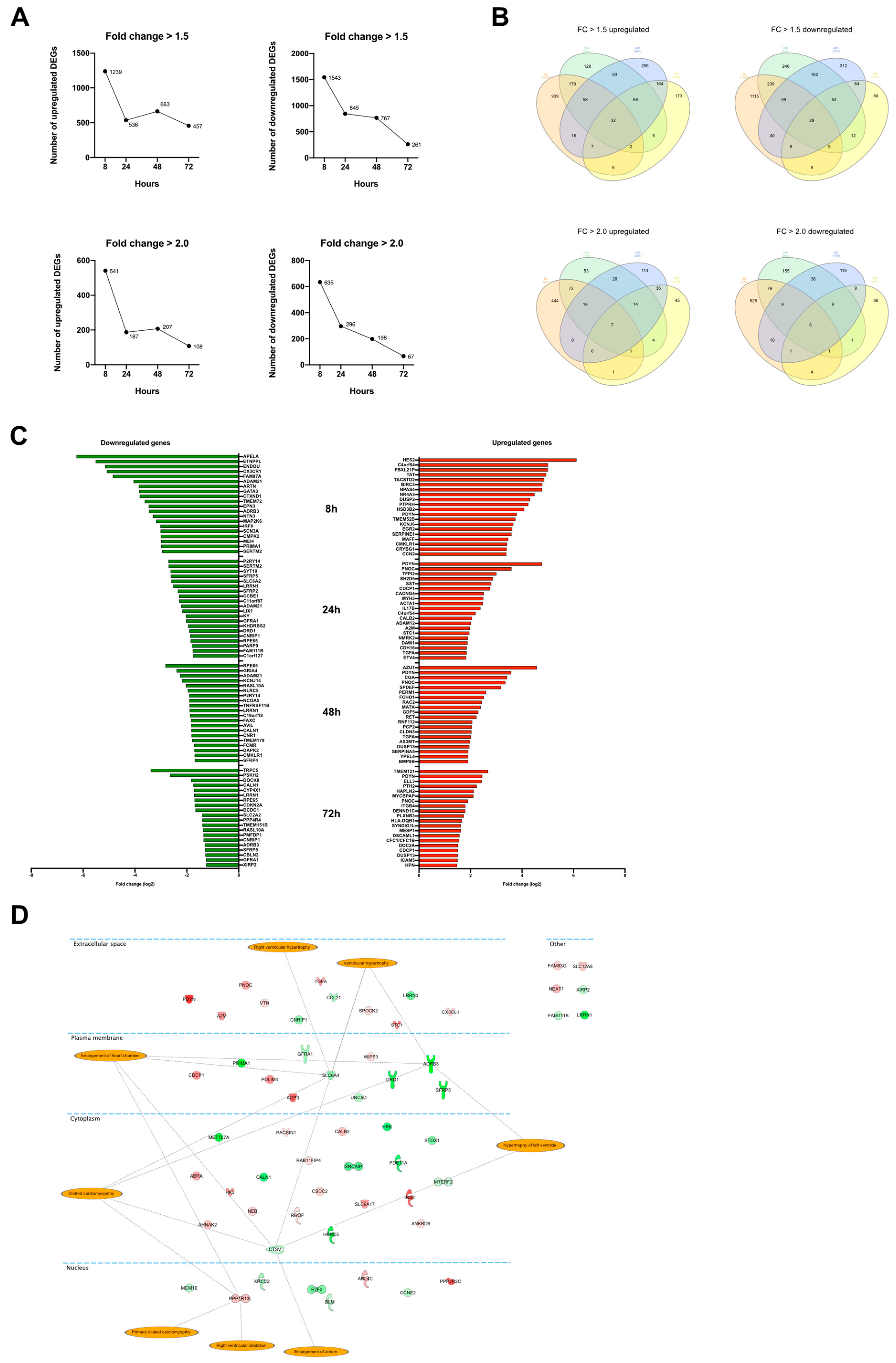
Our analysis identified an increased expression of many genes that are related to cardiac hypertrophy already at 8 h of ET-1 stimulation. In fact, the largest numbers of DEGs were observed at the earliest time point (8 h) and then decreased over the 24, 48, and 72 h time points. This change was observed when analyzing both DEGs with a FC of 2 and 1.5. The trend in the data with a lower number of DEGs over time was in contrast to the stretch model of cardiac hypertrophy, where an increase in DEGs is observed with extended treatment [
34]. Notably, our gene expression data at the 8 h time point were most similar to the latest time point (48 h) in the stretch model. It is possible that the neurohormonal approach that we used resulted in a more rapid hypertrophic response compared to the stretch model. It should be noted, however, that there is also a difference between the cellular source and species used in the studies (neonatal rat CM vs. human hiPSC-derived CMs), adding further complexity when interpreting data across the studies.
Some of the genes with the highest fold change that were picked up from the differential expression analysis were
PDYN,
PNOC, and
TGF. The
PDYN gene was upregulated at all time points and was also the most upregulated gene at 24 h and the second most upregulated at 48 h and 72 h. The
PDYN gene encodes the protein Proenkephalin-B, which is a preproprotein that is processed into several opioid peptides. They bind primarily to the K-opioid receptors that have been found to be widely expressed in the human heart [
35,
36]. Information about endogenous opioid peptides and their role in the cardiac hypertrophy development is sparse. However, there are data that support the hypothesis that the opioid system initially has a cardioprotective role. For example, in rat CMs, it has been shown that the use of a K-opioid receptor agonist protects against hypertrophy and fibrosis when stimulating the cells with the prohypertrophic agent isoprenaline [
37]. Taken together with the data from the present study,
PDYN appears to be a key candidate for further research in order to understand its potential involvement in the development of cardiac hypertrophy.
The gene
PNOC, which was also among the top DEGs at all time points, codes for the protein prepronociceptin. Studies using other in vitro models of cardiac hypertrophy have reported upregulation of
PNOC when neonatal rat CMs were stimulated with isoprenaline and phenylephrine. However, stimulation with ET-1 did not upregulate
PNOC [
38]. In contrast, in our model, using hiPSC-derived CMs, we saw a significant upregulation of this gene after ET-1 stimulation. The effect of the upregulation of
PNOC in humans is not well studied, and in pre-clinical models, the data are inconsistent. For example, in rodents,
PNOC has been shown to have inhibitory effects on cardiovascular parameters, while in sheep, it increases blood pressure [
39,
40]. More research is needed to elucidate if the distinct upregulation of
PNOC forms part of any cardioprotective mechanisms or if it may play a role in the long-term progression of cardiac hypertrophy.
The most downregulated gene at all time points was
APELA, encoding for an apelin receptor ligand. The apelin signaling in cardiac hypertrophy has been studied but whether apelin is beneficial or aggravating in this setting remains unclear [
41,
42,
43,
44]. In rats, administration of angiotensin II downregulates the expression of apelin within 24 h [
45]. In humans, there are data suggesting a strong negative correlation between serum apelin levels and left ventricular hypertrophy [
46].
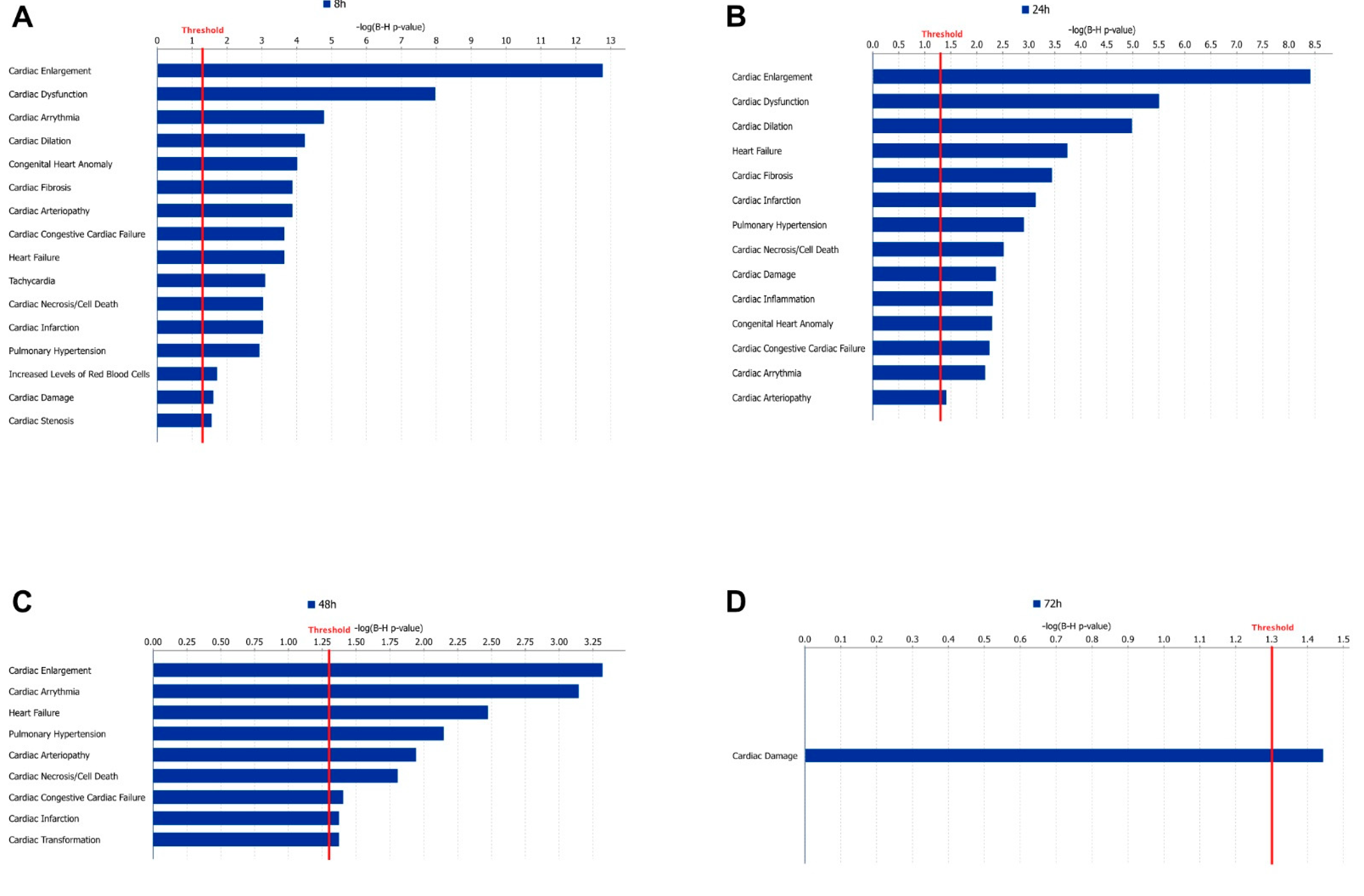
The pathway analysis using IPA identified the largest number of significantly enriched pathways at the 8 h time point; the number then decreased over time. This could be a consequence of the number of DEGs since fewer DEGs make the analysis less sensitive. These observations are in line with our previous study [
10]. ‘The Cardiac hypertrophy’ (enhanced) pathway was significantly enriched at 8 h, which was expected. However, already at 24 h, this pathway became inhibited, indicating that many of the genes in the pathway that were upregulated at 8 h were downregulated at 24 h. This switch in gene expression suggests a fast adaption or feedback response on a transcriptional level. Inhibition of hypertrophy pathways has been shown before when using in vitro models and hypertrophic stimulation for more than 24 h [
7]. While many pathways were only enriched at the first time point in our data, we know from our previous study that the hypertrophy phenotype is persistent over time [
10].
Our results showed similarities with previous studies. Signaling pathways that were enriched in our data have been previously reported by others, including actin cytoskeleton, angiopoietin,
IL-6,
IL-8,
HMGB1, and metabolic pathways [
7,
34]. Interestingly, adrenergic signaling in CMs was downregulated in both our neurohormonal model as well as the stretch model described by Ovchinnikova et al. [
7]. In heart failure, β-adrenergic signaling is downregulated, possibly as a compensatory mechanism. Today, inhibiting β-adrenergic signaling using β-antagonists is a cornerstone in the pharmacological treatment of heart failure [
47]. We also found that
IL-6, Oncostatin M, and JAK/STAT signaling were enriched at 8 h. An increase in the signaling of these pathways suggests that the STAT3 pathway is enriched, something that we also found in our analysis. Enrichment of the STAT3 pathway has been shown to promote cardiac hypertrophy by inducing the growth of CMs. Overexpression studies have also found that it increases the expression of hypertrophy genes, such as
NPPA,
MYH7, and
CTF1 [
48].
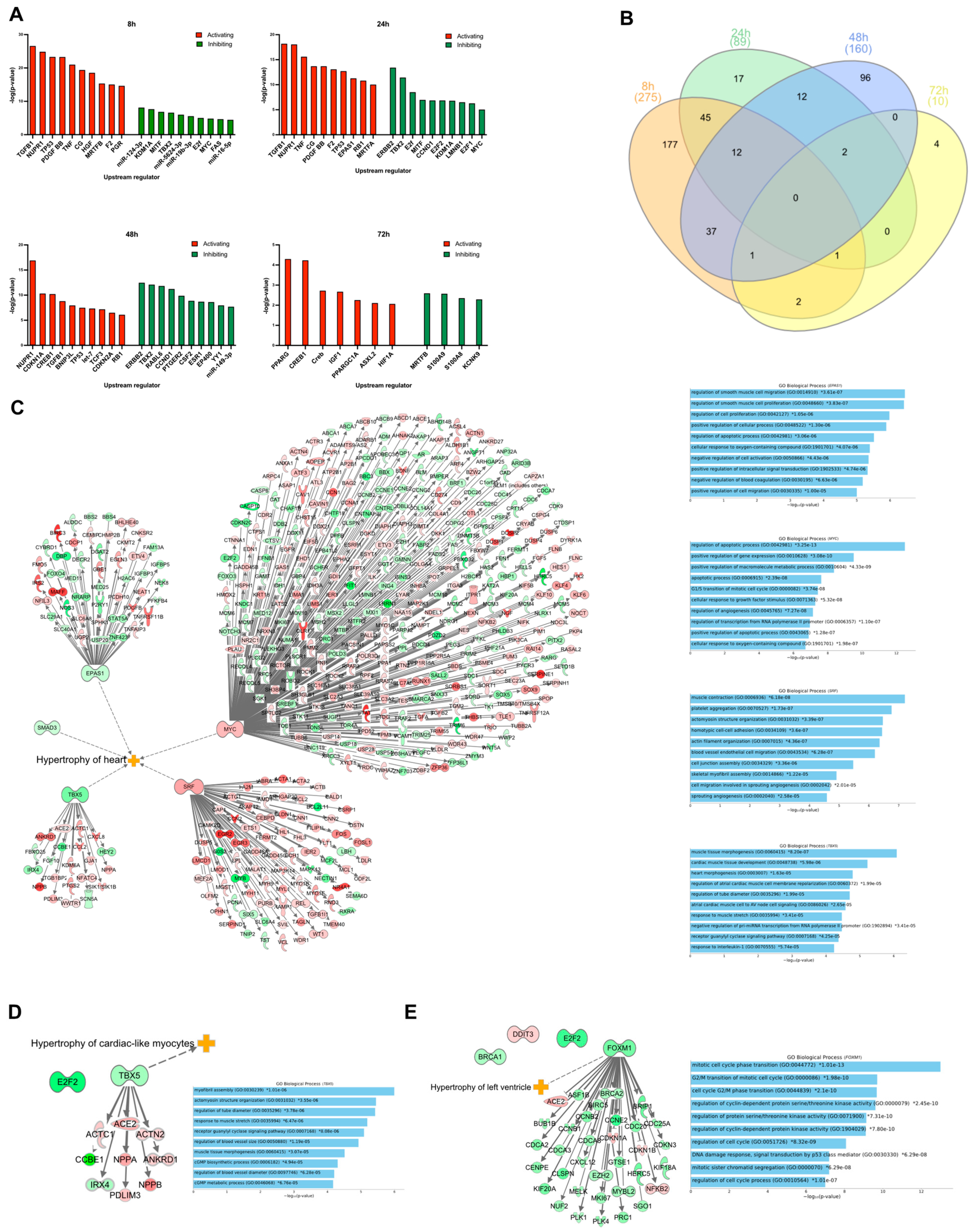
From the upstream regulator analysis using IPA, several TRs that play a role in cardiac hypertrophy were identified as differentially expressed in our data set. These regulators affect, in the majority of cases, many genes that were differentially expressed in our data and may therefore represent interesting targets in drug discovery.
MYC was one of the most active TRs that was differentially expressed in our study and is known to be important in early development, where it controls the proliferation of CMs [
49]. In addition, it is upregulated when CMs are exposed to hypertrophic stimuli, and it can also induce hypertrophy by itself [
50,
51,
52]. Neonatal rat CMs cultured in vitro and stimulated with ET-1 showed a significant hypertrophic response with the upregulation of
MYC, a response attenuated when
MYC was inhibited [
53]. Another TR associated with cardiac hypertrophy that was upregulated in our stimulated CMs is
SRF.
SRF is known to be required for the induction of the “fetal gene program”, which is a set of genes that is characteristic of cardiac hypertrophy [
54]. Overexpression studies in animals show that it regulates the fetal genes long before an increase in heart weight is observed [
55]. We observed differential expression of some, but not all, of the genes in the fetal gene program (e.g.,
NPPA,
NPPB, and
ACTA1). We also analyzed some upstream regulators that are transcription factors.
TBX5, which was differentially expressed at 8 and 24 h, regulates the expression of several genes that are specific to the heart [
56]. Although
TBX5 was downregulated at 8 and 24 h, it is possible that this gene was upregulated at an even earlier time point. Importantly, GO enrichment analysis of the DEGs that
TBX5 regulates in our data set identified many GO terms associated with the heart. This suggests that
TBX5 may be a target for drugs against cardiac hypertrophy since it will be more specific to the heart.
As described in the differential expression analysis, we identified many genes that are of importance in cardiac hypertrophy, showing that our model resembles the in vivo situation in many aspects. Therefore, we went on to use the model for the identification of differentially expressed proteins that are secreted from the CMs, and that can be measured in the conditioned media.
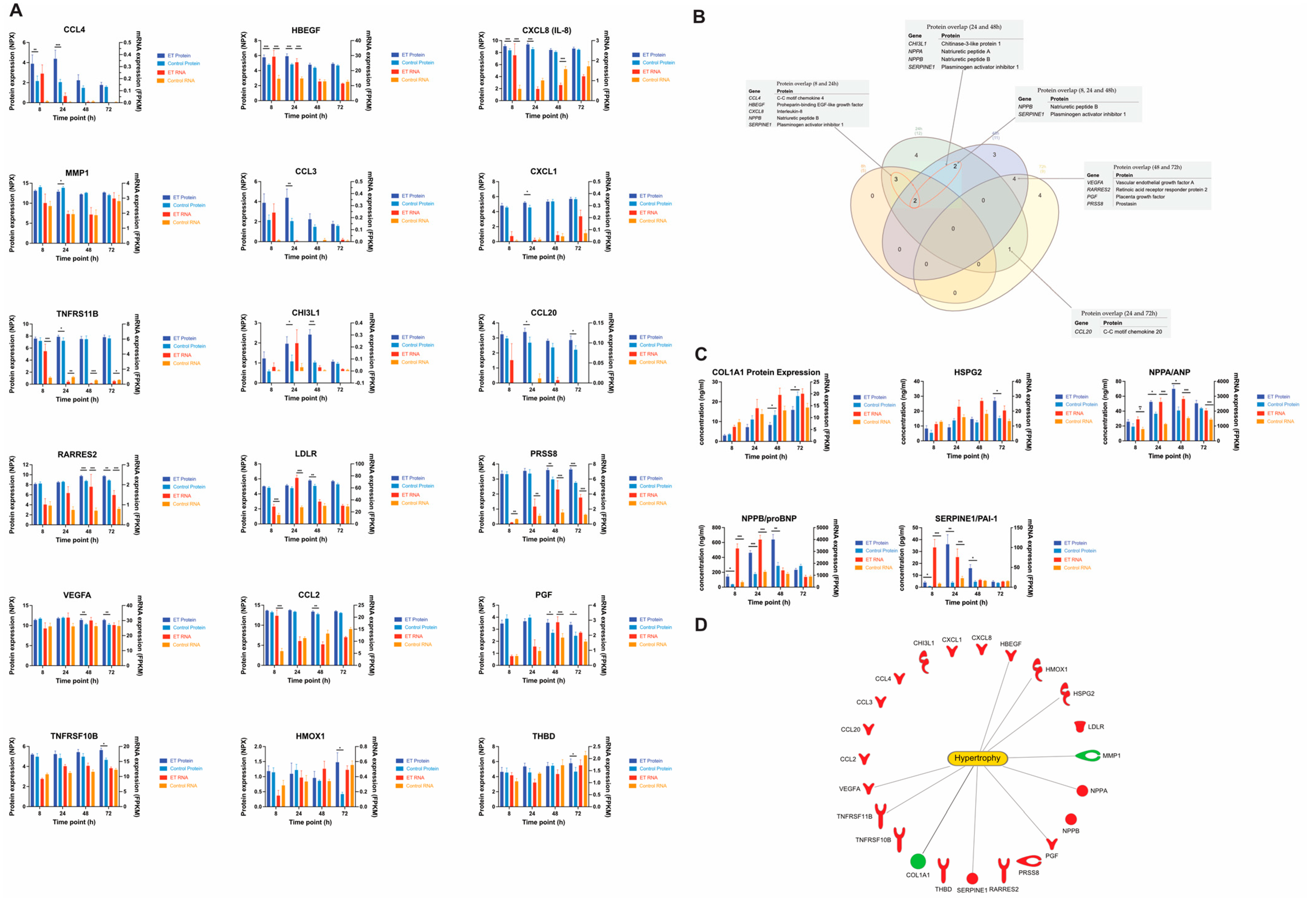
We performed a focused proteomics analysis using Olinks CVD II, III, and Inflammation panels to identify differentially expressed secreted proteins. To our knowledge, this is the first time where secretome analysis has been performed on conditioned media from a human stem cell-based model of cardiac hypertrophy. The secretome studies of CMs reported to date have been performed using animal models or during differentiation of stem cells to CMs [
57,
58,
59]. Twenty-three proteins were significantly differentially expressed at least at one of the time points in our study. Notably, 10 of them had the corresponding gene significantly differentially expressed also at some time point in the experiment. These genes/proteins were
CXCL8,
HBEGF,
LDLR,
NPPA,
NPPB RARRES2,
SERPINE1,
TNFRS11B,
PGF, and
PRSS8 (
Figure 5). However, the potential time difference from mRNA to secreted protein should not be neglected and when the correlation analysis was performed with one time point shifted for the proteins (e.g., mRNA at 8 h vs. protein at 24 h), the observed correlation was substantially higher. In fact, when using the time shift approach, the majority of gene–protein pairs had a correlation value > 0.8. The rate of mRNA to protein is in part affected by the translation rate, the binding of regulatory elements, such as micro-RNAs, protein half-life modulation through the ubiquitin–proteasome pathway, and protein synthesis delay [
60]. These are all factors that may explain the observed difference in the correlation between the different proteins in the study.
Seven secreted proteins were identified as differentially expressed at 72 h, and many of them showed a strong correlation between protein expression and gene expression. Chemerin, which is encoded by the gene
RARRES2, was significantly upregulated at both gene and protein levels at 48 and 72 h and had an overall correlation between gene and protein expression for the ET-1 stimulated cells of r = 0.72. Chemerin has a well-known role in metabolic syndrome and may contribute to hypertension by acting on chemokine-like receptor 1 [
61,
62].
Two growth factors that are in the same family, vascular endothelial growth factor A and placental growth factor, were also significantly upregulated at 72 h. Both these proteins are associated with angiogenesis and vasculogenesis and may indicate that the heart compensates for the increase in work and size by trying to increase its vascular network [
63,
64]. This mechanism is observed in physiological cardiac hypertrophy, where the blood flow to the heart grows in proportion to the size of the heart. Our relatively pure CM population made it difficult to assess if the increase in these growth factors could stimulate the formation of new blood vessels. However, an increase could very well be an indicator of stress of the heart and possibly an early sign of hypoxia in the CMs [
65].
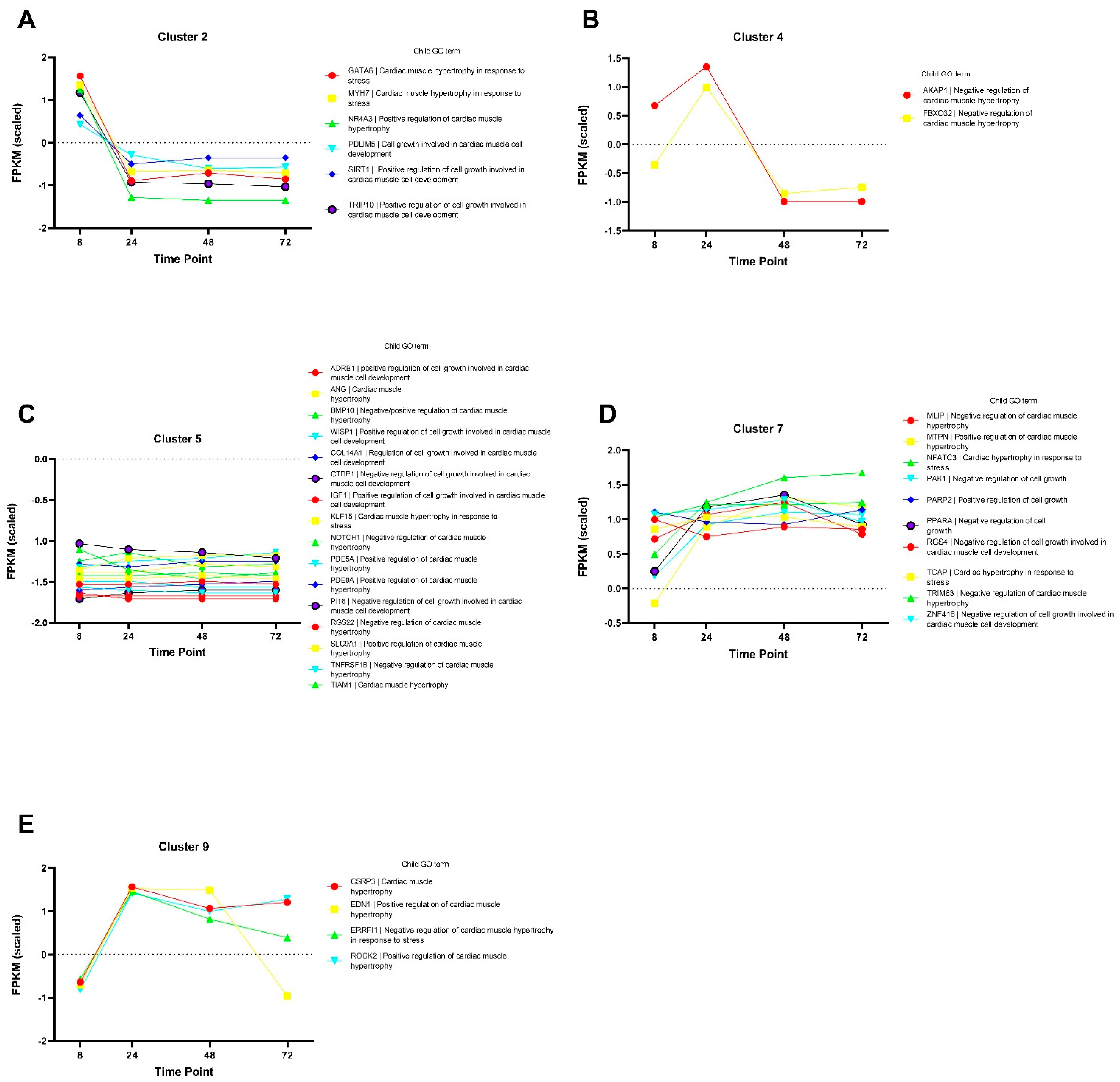
In summary, we have shown that our model of cardiac hypertrophy based on hiPSC-CM and neurohormonal stimulation recapitulates important characteristics of cardiac hypertrophy on a transcriptional level. Pathway and cluster analyses also shed novel insight into the underlying mechanisms potentially regulating cardiac hypertrophy on a cellular level. Additionally, several secreted proteins were differentially expressed, and further investigations are warranted to determine their exact role in the hypertrophy response and how they can be used clinically in the future.


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}