
Long COVID in Children and Adolescents

 , , and
, , and 
Abstract
:1. Introduction
2. Epidemiology of Long COVID in Children
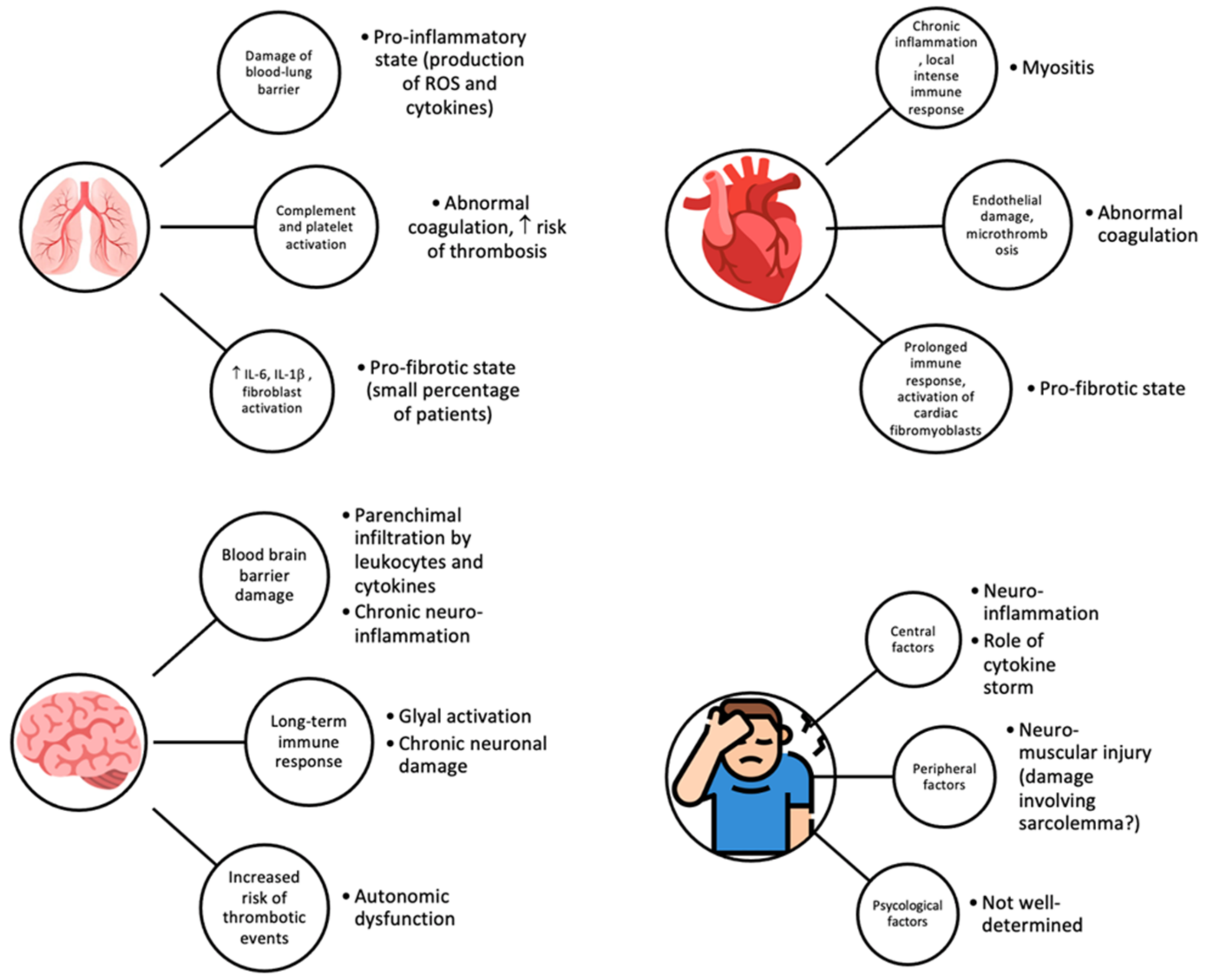
3. Pathophysiology and Immunological Aspects
4. Clinical Manifestations
5. Risk Factors for Long COVID
6. Long Term Consequences of Long COVID in Pediatric Age
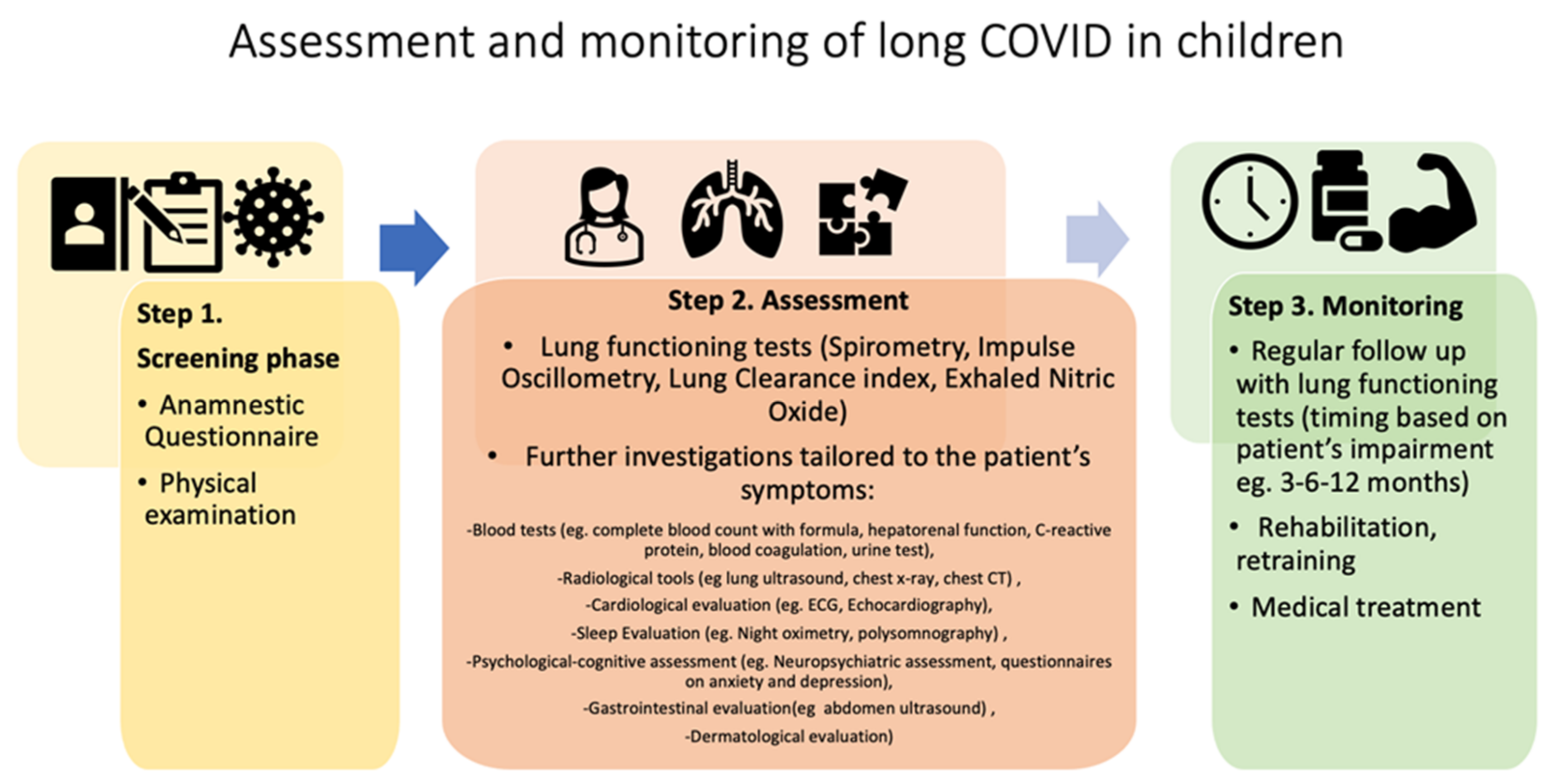
7. Monitoring and Follow-Up
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Academy of Pediatrics. Children and COVID-19: State-Level Data Report. Available online: www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/ (accessed on 22 November 2021).
- Li, B.; Zhang, S.; Zhang, R.; Chen, X.; Wang, Y.; Zhu, C. Epidemiological and clinical characteristics of COVID-19 in children: A systematic review and meta-analysis. Front Pediatr. 2020, 8, 591132. [Google Scholar] [CrossRef]
- Radia, T.; Williams, N.; Agrawal, P.; Harman, K.; Weale, J.; Cook, J.; Gupta, A. Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation. Paediatr. Respir. Rev. 2021, 38, 51–57. [Google Scholar] [CrossRef]
- Vella, L.A.; Rowley, A.H. Current insights into the pathophysiology of multisystem inflammatory syndrome in children. Curr. Pediatr. Rep. 2021, 9, 1–10. [Google Scholar] [CrossRef]
- NICE. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute for Health and Care Excellence (NICE): London, UK, 2020. [Google Scholar]
- Munblit, D.; Bobkova, P.; Spiridonova, E.; Shikhaleva, A.; Gamirova, A.; Blyuss, O.; Nekliudov, N.; Bugaeva, P.; Andreeva, M.; DunnGalvin, A.; et al. StopCOVID research team. Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19. Clin. Exp. Allergy 2021, 51, 1107–1120. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-covid syndrome in individuals admitted to hospital with Covid-19: Retrospective cohort study. BMJ 2021, 372, n693. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta Paediatr. 2021, 110, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Say, D.; Crawford, N.; McNab, S.; Wurzel, D.; Steer, A.; Tosif, S. Post-acute COVID-19 outcomes in children with mild and asymptomatic disease. Lancet Child Adolesc. Health 2021, 5, e22–e23. [Google Scholar] [CrossRef]
- Buonsenso, D.; Munblit, D.; De Rose, C.; Sinatti, D.; Ricchiuto, A.; Carfi, A.; Valentini, P. Preliminary evidence on long COVID in children. Acta Paediatr. 2021, 110, 2208–2211. [Google Scholar] [CrossRef]
- Osmanov, I.M.; Spiridonova, E.; Bobkova, P.; Gamirova, A.; Shikhaleva, A.; Andreeva, M.; Blyuss, O.; El-Taravi, Y.; DunnGalvin, A.; Comberiati, P.; et al. Risk factors for long covid in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur. Respir. J. 2021, 1, 2101341. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Shmueli, E.; Ehrlich, S.; Ziv, A.; Bar-On, O.; Birk, E.; Lowenthal, A.; Prais, D. Long COVID in Children: Observations from a Designated Pediatric Clinic. Pediatr. Infect. Dis. J. 2021, 40, e509–e511. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.; Nguyen, V.; Navaratnam, A.M.; Shrotri, M.; Kovar, J.; Hayward, A.C.; Fragaszy, E.; Aldridge, R.W.; Hardelid, P. Prevalence of persistent symptoms in children during the COVID-19 pandemic: Evidence from a household cohort study in England and Wales. medRxiv 2021. [Google Scholar] [CrossRef]
- Buonsenso, D.; Espuny Pujol, F.; Munblit, D.; Mcfarland, S.; Simpson, F. Clinical Characteristics, Activity Levels and Mental Health Problems in Children with Long COVID: A Survey of 510 Children. Preprints 2021. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Antonelli, M.; Murray, B.; Kläser, K.; Kerfoot, E.; Chen, L.; et al. Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2. Lancet Child Adolesc. Health 2021, 5, 708–718. [Google Scholar] [CrossRef]
- Office for National Statistics. Technical Article: Updated Estimates of the Prevalence of Post-Acute Symptoms among People with Coronavirus (COVID-19) in the UK: 26 April 2020 to 1 August 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/technicalarticleupdatedestimatesoftheprevalenceofpostacutesymptomsamongpeoplewithcoronaviruscovid19intheuk/26april2020to1august2021 (accessed on 1 December 2021).
- Roge, I.; Smane, L.; Kivite-Urtane, A.; Pucuka, Z.; Racko, I.; Klavina, L.; Pavare, J. Comparison of Persistent symptoms after COVID-19 and other non-SARS-CoV-2 infections in children. Front. Pediatr. 2021, 9, 752385. [Google Scholar] [CrossRef]
- Blankenburg, J.; Wekenborg, M.K.; Reichert, J.; Kirsten, C.; Kahre, E.; Haag, L.; Schumm, L.; Czyborra, P.; Berner, R.; Armann, J.P. Mental Health of Adolescents in the Pandemic: Long-COVID-19 or Long-Pandemic Syndrome? medRxiv 2021. [Google Scholar] [CrossRef]
- Brackel, C.L.H.; Lap, C.R.; Buddingh, E.P.; Houten, M.A.; van der Sande, L.J.T.M.; Langereis, E.J.; Bannier, M.A.G.E.; Pijnenburg, M.W.H.; Hashimoto, S.; Terheggen-Lagro, S.W.J. Pediatric long-COVID: An overlooked phenomenon? Pediatr. Pulmonol. 2021, 56, 2495–2502. [Google Scholar] [CrossRef]
- Radtke, T.; Ulyte, A.; Puhan, M.A.; Kriemler, S. Long-term Symptoms After SARS-CoV-2 Infection in Children and Adolescents. JAMA 2021, 326, 869–871. [Google Scholar] [CrossRef]
- Smane, L.; Stars, I.; Pucuka, Z.; Roge, I.; Pavare, J. Persistent clinical features in paediatric patients after SARS-CoV-2 virological recovery: A retrospective population-based cohort study from a single centre in Latvia. BMJ Paediatr. Open 2020, 4, e000905. [Google Scholar] [CrossRef]
- Stephenson, T.; Pinto Pereira, S.; Shafran, R.; De Stavola, B.; Rojas, N.; McOwat, K.; Simmons, R.; Zavala, M.; O’Mahoney, L.; Chalder, T.; et al. Long COVID—The physical and mental health of children and non-hospitalised young people 3 months after SARS-CoV-2 infection; a national matched cohort study (The CLoCk) study. In Nature Portfolio; Research Square: Durham, NC, USA, 2021. [Google Scholar]
- Sterky, E.; Olsson-Åkefeldt, S.; Hertting, O.; Herlenius, E.; Alfven, T.; Rinder, M.R.; Rhedin, S.; Hildenwall, H. Persistent symptoms in Swedish children after hospitalisation due to COVID-19. Acta Paediatrica 2021, 110, 2578–2580. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid-mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef] [PubMed]
- Di Sante, G.; Buonsenso, D.; De Rose, C.; Valentini, P.; Ria, F.; Sanguinetti, M.; Sali, M. Immune profile of children with post-acute sequelae of SARS-CoV-2 infection (Long COVID). medRxiv 2021. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Buonsenso, D.; Di Giuda, D.; Sigfrid, L.; Pizzuto, D.A.; Di Sante, G.; De Rose, C.; Lazzareschi, I.; Sali, M.; Baldi, F.; Chieffo, D.P.R.; et al. Evidence of lung perfusion defects and ongoing inflammation in an adolescent with post-acute sequelae of SARS-CoV-2 infection. Lancet Child Adolesc. Health 2021, 5, 677–680. [Google Scholar] [CrossRef]
- Dhawan, R.T.; Gopalan, D.; Howard, L.; Vicente, A.; Park, M.; Manalan, K.; Wallner, I.; Marsden, P.; Dave, S.; Branley, H.; et al. Beyond the clot: Perfusion imaging of the pulmonary vasculature after COVID-19. Lancet Respir. Med. 2021, 9, 107–116. [Google Scholar] [CrossRef]
- Daher, A.; Balfanz, P.; Cornelissen, C.; Müller, A.; Bergs, I.; Marx, N.; Müller-Wieland, D.; Hartmann, B.; Dreher, M.; Müller, T. Follow up of patients with severe coronavirus disease 2019 (COVID-19): Pulmonary and extrapulmonary disease sequelae. Respir. Med. 2020, 174, 106197. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month follow-up chest CT findings after severe COVID-19 pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Ambardar, S.R.; Hightower, S.L.; Huprikar, N.A.; Chung, K.K.; Singhal, A.; Collen, J.F. Post-COVID-19 pulmonary fibrosis: Novel sequelae of the current pandemic. J. Clin. Med. 2021, 10, 2452. [Google Scholar] [CrossRef] [PubMed]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2020, 21, e63–e67. [Google Scholar] [CrossRef] [PubMed]
- Yachou, Y.; El Idrissi, A.; Belapasov, V.; Benali, S.A. Neuroinvasion, neurotropic, and neuroinflammatory events of SARS-CoV-2: Understanding the neurological manifestations in COVID-19 patients. Neurol. Sci. 2020, 41, 2657–2669. [Google Scholar] [CrossRef] [PubMed]
- Zhong, P.; Xu, J.; Yang, D.; Shen, Y.; Wang, L.; Feng, Y.; Du, C.; Song, Y.; Wu, C.; Hu, X.; et al. COVID-19-associated gastrointestinal and liver injury: Clinical features and potential mechanisms. Signal Transduct. Target. Ther. 2020, 5, 256. [Google Scholar] [CrossRef]
- Yan, Z.; Yang, M.; Lai, C.-L. Long COVID-19 syndrome: A comprehensive review of its effect on various organ systems and recommendation on rehabilitation plans. Biomedicines 2021, 9, 966. [Google Scholar] [CrossRef]
- Islam, M.F.; Cotler, J.; Jason, L.A. Post-viral fatigue and COVID-19: Lessons from past epidemics. Fatigue Biomed. Health Behavior. 2020, 8, 61–69. [Google Scholar] [CrossRef]
- Dhochak, N.; Singhal, T.; Kabra, S.K.; Lodha, R. Pathophysiology of COVID-19: Why children fare better than adults? Indian J. Pediatr. 2020, 87, 537–546. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Nemati, H.; Shahisavandi, M.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; et al. Long COVID in children and adolescents. World J. Pediatr. 2021, 17, 495–499. [Google Scholar] [CrossRef]
- Zimmermann, P.; Pittet, L.F.; Curtis, N. How common is long COVID in children and adolescents? Pediatr. Infect. Dis. J. 2021, 40, e482–e487. [Google Scholar] [CrossRef]
- Sigfrid, L.; Drake, T.M.; Pauley, E.; Jesudason, E.C.; Olliaro, P.; Lim, W.S.; Gillesen, A.; Berry, C.; Lowe, D.J.; McPeake, J.; et al. Long covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg. Health 2021, 8, 100186. [Google Scholar] [CrossRef] [PubMed]
- Denina, M.; Pruccoli, G.; Scolfaro, C.; Mignone, F.; Zoppo, M.; Giraudo, I.; Silvestro, E.; Bertolotti, L.; Rosati, S.; Ramenghi, U.; et al. Sequelae of COVID-19 in hospitalized children: A 4-months follow-up. Pediatr. Infect. Dis. J. 2020, 39, e458–e459. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, E.S.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, E.T.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2021, 76, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Funke-Chambour, M.; Bridevaux, P.-O.; Clarenbach, C.F.; Soccal, P.M.; Nicod, L.P.; von Garnier, C. Swiss Recommendations for the follow-up and treatment of pulmonary long COVID. Respiration 2021, 100, 826–841. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.M.M.; Ghonimy, M.B.I. Post-COVID-19 pneumonia lung fibrosis: A worrisome sequelae in surviving patients. Egypt. J. Radiol. Nucl. Med. 2021, 52, 101. [Google Scholar] [CrossRef]
- British Thoracic Society. Guidance on Respiratory Follow up of Patients with a Clinico-Radiological Diagnosis of COVID-19 Pneumonia. Available online: https://www.brit-thoracic.org.uk (accessed on 1 December 2021).



{kind=link}
{kind=link}
| Study Reference | Study Design | Country | Number of Subjects | Controls | COVID-19 Laboratory Confirmed | Subjects with Associated Comorbidities (%) | Symptomatic at Time of Infection (%) | Need of Hospitalisation during Acute Phase (%) | Subjects with Long COVID (%) | Age (years), Median or Mean | Median Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ashkenazi-Hoffnung et al., 2021 [13] | Prospective cohort study | Israel | 90 | No | Yes | 31.1 | 96.7 | 12.2 | 100 | 12.5 | 112 d |
| Blankenburg et al., 2021 [19] | Cross-sectional | Germany | 1560 (188 seropositive) | Yes | Yes | - | - | - | - | 15 (14–16) | - |
| Brackel et al., 2021 [20] | Cross-sectional | Netherlands | 89 | No | No | - | - | - | 100 | 13 (9–15) | - |
| Buonsenso et al., 2021 [11] | Cross-sectional | Italy | 129 | No | No | - | 74.4 | 4.7 | 58.2 | 11 ± 4.4 | 162.5 ± 113.7 d |
| Buonsenso et al., 2021 [15] | Cross-sectional | UK, USA | 510 | No | Yes | 56.3 | 87.8 | 4.3 | 93.7 | 10.3 ± 3.8 | - |
| Miller et al., 2021 [14] | Prospective cohort study | UK | 4504 (175 positive) | Yes | Yes | - | - | - | 4.6 | 0–17 | - |
| Molteni et al., 2021 [16] | Prospective cohort study | UK | 3113 (1734 positive) | Yes | Yes | 13.1 | - | - | 4.4 | 5–17 | 4 w |
| Osmanov et al., 2021 [12] | Prospective cohort study | Russia | 518 | No | Yes | 44.7 | - | - | 24.7 | 10.4 (3–15) | 268 d |
| Radtke et al., 2021 [21] | Prospective cohort study | Switzerland | 1355 (109 positive) | Yes | Yes | - | - | - | 4 | 11 | 12 w |
| Roge et al., 2021 [18] | Cohort-study | Latvia | 236 | No | Yes | 22 | 93 | - | 64.4 | 10 | 73.5 d |
| Say et al., 2021 [10] | Prospective cohort study | Australia | 171 | No | Yes | 14 | 64 | 8 | 8 | 3.7 ± 3.5 | 3–6 m |
| Smane et al., 2020 [22] | Retrospective cohort study | Latvia | 30 | No | Yes | 23 | 83 | 16.6 | 30 | 9.2 ± 5.2 | 101 d |
| Stephenson et al., 2021 [23] | Prospective cohort study | UK | 6804 (3065 positive) | Yes | Yes | - | - | - | 66.5 | 11–17 | 15 w |
| Sterky et al., 2021 [24] | Prospective cohort study | Sweden | 55 | No | Yes | 35 | - | - | 22 | 0–18 | 219 d |
| Cardiovascular | Neurological/Neuropsychiatric |
|---|---|
| Chest tightness or pain (1–31%) | Brain fog |
| Palpitations (4–18%) | Concentration difficulties (2–81%) |
| Dermatological | Sleep disturbance (2–63%) |
| Skin rashes (2–52%) | Dizziness (3–20%) |
| Gastrointestinal | Irritability and mood changes (5–24%) |
| Stomachache (5–70%) | Headache (3–80%) |
| Abdominal pain (1–76%) | Memory loss |
| Diarrhea (2–24%) | Smell disorder (12–70%) |
| Vomiting (2–24%) | Taste disorder (20–70%) |
| General | Nocturnal sweating |
| Fatigue (3–87%) | Respiratory |
| Persistent fever (2–40%) | Cough (1–30%) |
| Loss of appetite or weight (2–50%) | Dyspnea (40–50%) |
| Muscular | Upper Airway |
| Myalgia or arthralgia (1–61%) | Nasal congestion or rhinorrhea (1–12%) |
| Sore throat (4–70%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fainardi, V.; Meoli, A.; Chiopris, G.; Motta, M.; Skenderaj, K.; Grandinetti, R.; Bergomi, A.; Antodaro, F.; Zona, S.; Esposito, S. Long COVID in Children and Adolescents. Life 2022, 12, 285. https://doi.org/10.3390/life12020285
Fainardi V, Meoli A, Chiopris G, Motta M, Skenderaj K, Grandinetti R, Bergomi A, Antodaro F, Zona S, Esposito S. Long COVID in Children and Adolescents. Life. 2022; 12(2):285. https://doi.org/10.3390/life12020285
Chicago/Turabian StyleFainardi, Valentina, Aniello Meoli, Giulia Chiopris, Matteo Motta, Kaltra Skenderaj, Roberto Grandinetti, Andrea Bergomi, Francesco Antodaro, Stefano Zona, and Susanna Esposito. 2022. "Long COVID in Children and Adolescents" Life 12, no. 2: 285. https://doi.org/10.3390/life12020285