
Aging and Wound Healing of the Skin: A Review of Clinical and Pathophysiological Hallmarks
 ,
,
Abstract
:1. Introduction
2. Prevalence of the Aging Population
3. Mechanism of Skin Aging
3.1. Intrinsic Aging
3.2. Extrinsic Aging
4. Observation on Skin Aging
4.1. Epidermis
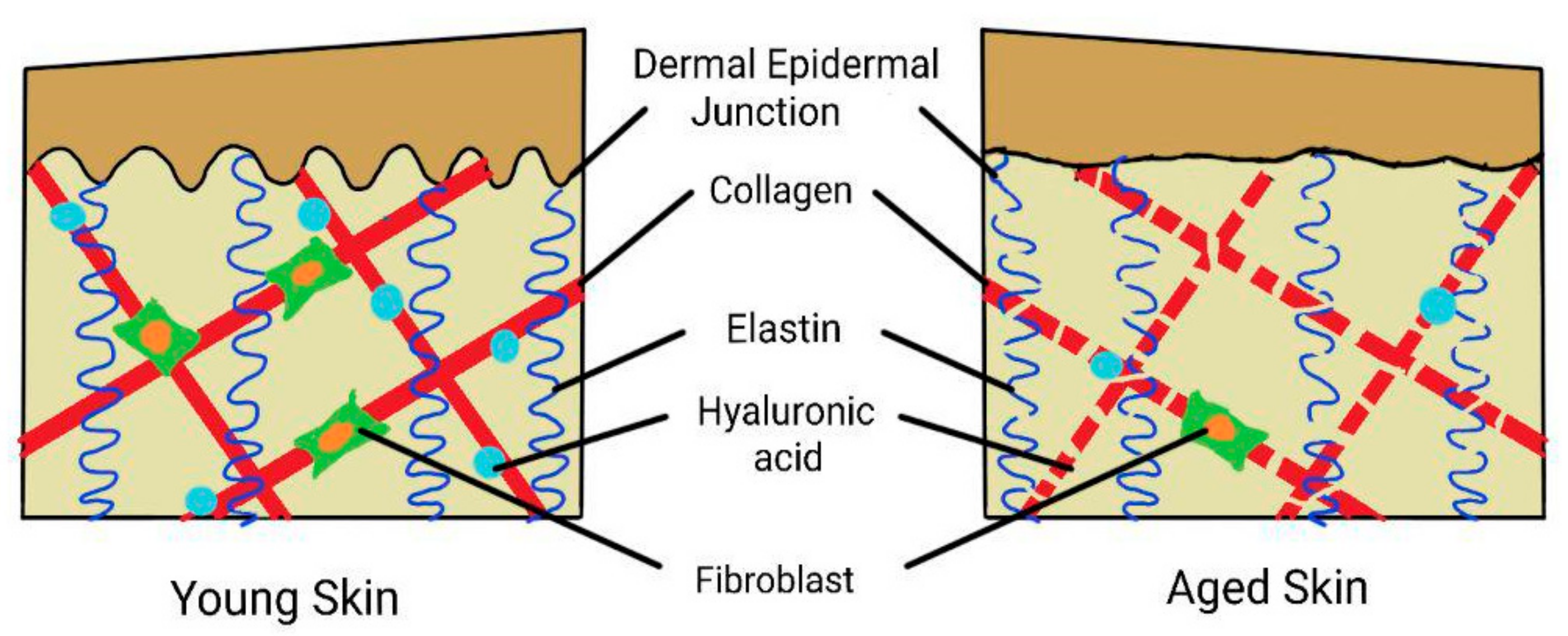
4.2. Dermal-Epidermal Junction (DEJ)
4.3. Dermis
5. The Effects of Skin Aging on Wound Healing
5.1. Normal Wound Healing Physiology
5.1.1. Inflammatory Phase
5.1.2. Reepithelialization Phase
5.1.3. Tissue Remodeling Phase
5.2. Alteration of Wound Healing Process Due to Aging
5.2.1. Prolong Inflammatory Phase
5.2.2. Oxidative Stress
5.2.3. Inefficient Microcirculation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, S.; Bajorek, B. Defining ‘Elderly’ in Clinical Practice Guidelines for Pharmacotherapy. Pharm. Pract. 2014, 12, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathor, M.Y.; Khattak, M.M.A.K.; Yusof, N.M. End-Of-Life: Old Age in Contemporary Society, Self-Perception of Aging And ‘An’ Islamic Perspective. Int. J. Hum. Health Sci. 2019, 3, 64–73. [Google Scholar] [CrossRef] [Green Version]
- Jaul, E.; Barron, J. Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Front. Public Health 2017, 5, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschi, C.; Garagnani, P.; Morsiani, C.; Conte, M.; Santoro, A.; Grignolio, A.; Monti, D.; Capri, M.; Salvioli, S. The Continuum of Aging and Age-Related Diseases: Common Mechanisms but Different Rates. Front. Med. 2018, 5, 61. [Google Scholar] [CrossRef] [Green Version]
- Gould, L.; Abadir, P.; Brem, H.; Carter, M.; Conner-Kerr, T.; Davidson, J.; DiPietro, L.; Falanga, V.; Fife, C.; Gardner, S.; et al. Chronic Wound Repair and Healing in Older Adults: Current Status and Future Research. J. Am. Geriatr. Soc. 2015, 63, 427–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). World Report on Aging and Health; Publications of the World Health Organization: Geneva, Switzerland, 2015; pp. 1–246. ISBN 9789240694811.
- World Health Organization (WHO). GHE: Life Expectancy and Healthy Life Expectancy. 2020. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-life-expectancy-and-healthy-life-expectancy (accessed on 15 February 2021).
- Tobi, S.U.M.; Fathi, M.S.; Amaratunga, D. Ageing in Place, an Overview for the Elderly in Malaysia. AIP Conf. Proc. 2017, 1891, 020101–020106. [Google Scholar] [CrossRef] [Green Version]
- Oliver, M. Population Ageing and Economic Growth in Japan. Int. J. Sociol. Soc. Policy 2015, 35, 841–863. [Google Scholar] [CrossRef]
- Al-Nuaimi, Y.; Sherratt, M.J.; Griffiths, C.E.M. Skin Health in Older Age. Maturitas 2014, 79, 256–264. [Google Scholar] [CrossRef]
- Gilaberte, Y.; Prieto-Torres, L.; Pastushenko, I.; Juarranz, Á. Anatomy and Function of the Skin. In Nanoscience in Dermatology; Hamblin, M.R., Avci, P., Prow, T.W., Eds.; Academic Press: Saint Louis, MO, USA, 2016; pp. 1–14. ISBN 9780128029459. [Google Scholar]
- Lavers, I. Exploring Skin Anatomy, Function and Site-Specific Treatment Options. J. Aesthetic Nurs. 2017, 6, 172–180. [Google Scholar] [CrossRef]
- Limbert, G.; Masen, M.A.; Pond, D.; Graham, H.K.; Sherratt, M.J.; Jobanputra, R.; McBride, A. Biotribology of the Ageing Skin—Why We Should Care. Biotribology 2019, 17, 75–90. [Google Scholar] [CrossRef]
- Swaney, M.H.; Kalan, L.R. Living in Your Skin: Microbes, Molecules, and Mechanisms. Infect. Immun. 2021, 89, e00695-20. [Google Scholar] [CrossRef]
- Tobin, D.J. Introduction to Skin Aging. J. Tissue Viability 2017, 26, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.C.; Park, T.J.; Kang, H.Y. Skin-Aging Pigmentation: Who Is the Real Enemy? Cells 2022, 11, 2541. [Google Scholar] [CrossRef] [PubMed]
- Lavretsky, H.; Newhouse, P.A. Stress, Inflammation and Aging. Am. J. Geriatr. Psychiatry 2013, 20, 729–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Lyga, J. Brain-Skin Connection: Stress, Inflammation and Skin Aging. Inflamm. Allergy Drug Targets 2014, 13, 177–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aunan, J.R.; Watson, M.M.; Hagland, H.R.; Søreide, K. Molecular and Biological Hallmarks of Ageing. Br. J. Surg. 2016, 103, 29–46. [Google Scholar] [CrossRef] [Green Version]
- Maynard, S.; Fang, E.F.; Scheibye-Knudsen, M.; Croteau, D.L.; Bohr, V.A. DNA Damage, DNA Repair, Aging, and Neurodegeneration. Cold Spring Harb. Perspect. Med. 2015, 5, a025130. [Google Scholar] [CrossRef] [Green Version]
- Chilton, W.; O’Brien, B.; Charchar, F. Telomeres, Aging and Exercise: Guilty by Association? Int. J. Mol. Sci. 2017, 18, 2573. [Google Scholar] [CrossRef] [Green Version]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The Hallmarks of Aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef] [Green Version]
- Zouboulis, C.C.; Makrantonaki, E.; Nikolakis, G. When the Skin Is in the Center of Interest: An Aging Issue. Clin. Dermatol. 2019, 37, 296–305. [Google Scholar] [CrossRef]
- Strnadova, K.; Sandera, V.; Dvorankova, B.; Kodet, O.; Duskova, M.; Smetana, K.; Lacina, L. Skin Aging: The Dermal Perspective. Clin. Dermatol. 2019, 37, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Duan, E. Fighting against Skin Aging: The Way from Bench to Bedside. Cell Transplant. 2018, 27, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Taghavikhalilbad, A.; Adabi, S.; Clayton, A.; Soltanizadeh, H.; Mehregan, D.; Avanaki, M.R.N. Semi-Automated Localization of Dermal Epidermal Junction in Optical Coherence Tomography Images of Skin. Appl. Opt. 2017, 56, 3116–3121. [Google Scholar] [CrossRef] [PubMed]
- Bonté, F.; Girard, D.; Archambault, J.C.; Desmoulière, A. Skin Changes during Ageing. In Biochemistry and Cell Biology of Ageing: Part II Clinical Science; Harris, J.R., Korolchuk, V.I., Eds.; Springer: Singapore, 2019; Volume 91, pp. 249–280. ISBN 9789811336812. [Google Scholar]
- Bonifant, H.; Holloway, S. A Review of the Effects of Ageing on Skin Integrity and Wound Healing. Br. J. Community Nurs. 2019, 24, S28–S33. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.C.; Aveleira, C.; Cavadas, C. Skin Senescence: Mechanisms and Impact on Whole-Body Aging. Trends Mol. Med. 2022, 28, 97–109. [Google Scholar] [CrossRef]
- Wong, R.; Geyer, S.; Weninger, W.; Guimberteau, J.C.; Wong, J.K. The Dynamic Anatomy and Patterning of Skin. Exp. Dermatol. 2016, 25, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Cole, M.A.; Quan, T.; Voorhees, J.J.; Fisher, G.J. Extracellular Matrix Regulation of Fibroblast Function: Redefining Our Perspective on Skin Aging. J. Cell Commun. Signal. 2018, 12, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Mathew-Steiner, S.S.; Roy, S.; Sen, C.K. Collagen in Wound Healing. Bioengineering 2021, 8, 63. [Google Scholar] [CrossRef]
- Blair, M.J.; Jones, J.D.; Woessner, A.E.; Quinn, K.P. Skin Structure-Function Relationships and the Wound Healing Response to Intrinsic Aging. Adv. Wound Care 2020, 9, 127–143. [Google Scholar] [CrossRef]
- Qin, Z.; Balimunkwe, R.M.; Quan, T. Age-Related Reduction of Dermal Fibroblast Size Upregulates Multiple Matrix Metalloproteinases as Observed in Aged Human Skin in Vivo. Br. J. Dermatol. 2017, 177, 1337–1348. [Google Scholar] [CrossRef]
- Li, Y.; Lei, D.; Swindell, W.R.; Xia, W.; Weng, S.; Fu, J.; Worthen, C.A.; Okubo, T.; Johnston, A.; Gudjonsson, J.E.; et al. Age-Associated Increase in Skin Fibroblast-Derived Prostaglandin E2 Contributes to Reduced Collagen Levels in Elderly Human Skin. J. Investig. Dermatol. 2015, 135, 2181–2188. [Google Scholar] [CrossRef] [Green Version]
- Nicol, N.H. “Dermatologic Nursing Essentials Spotlight” New Column Features Highlights of Dermatology Nursing Textbook in the Journal of the Dermatology Nurses’ Association. J. Dermatol. Nurses. Assoc. 2017, 9, 121–122. [Google Scholar] [CrossRef]
- Xiong, Z.-M.; O’Donovan, M.; Sun, L.; Choi, J.Y.; Ren, M.; Cao, K. Anti-Aging Potentials of Methylene Blue for Human Skin Longevity. Sci. Rep. 2017, 7, 2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Re Domínguez, M.L.; Di Martino Ortiz, B.; Rodríguez Masi, M.; Knopfelmacher Domínguez, O.; Bolla Argüello de Lezcano, L. Dermatoporosis, an Emerging Disease: Case Report. Our Dermatol. Online 2016, 7, 191–194. [Google Scholar] [CrossRef]
- Dyer, J.M.; Miller, R.A. Chronic Skin Fragility of Aging: Current Concepts in the Pathogenesis, Recognition, and Management of Dermatoporosis. J. Clin. Aesthet. Dermatol. 2018, 11, 13–18. [Google Scholar] [PubMed]
- Bukhari, S.N.A.; Roswandi, N.L.; Waqas, M.; Habib, H.; Hussain, F.; Khan, S.; Sohail, M.; Ramli, N.A.; Thu, H.E.; Hussain, Z. Hyaluronic Acid, a Promising Skin Rejuvenating Biomedicine: A Review of Recent Updates and Pre-Clinical and Clinical Investigations on Cosmetic and Nutricosmetic Effects. Int. J. Biol. Macromol. 2018, 120, 1682–1695. [Google Scholar] [CrossRef]
- Lee, D.H.; Oh, J.; Chung, J.H. Glycosaminoglycan and Proteoglycan in Skin Aging. J. Dermatol. Sci. 2016, 83, 174–181. [Google Scholar] [CrossRef]
- Papakonstantinou, E.; Roth, M.; Karakiulakis, G. Hyaluronic Acid: A Key Molecule in Skin Aging. Dermato-Endocrinology 2012, 4, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Maquart, F.-X.; Brézillon, S.; Wegrowski, Y. Proteoglycans in Skin Aging. In Textbook of Aging Skin; Farage, M.A., Miller, K.W., Maibach, H.I., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 131–147. ISBN 978-3-662-47398-6. [Google Scholar]
- Chajra, H.; Auriol, D.; Joly, F.; Pagnon, A.; Rodrigues, M.; Allart, S.; Redziniak, G.; Lefevre, F. Reactivating the Extracellular Matrix Synthesis of Sulfated Glycosaminoglycans and Proteoglycans to Improve the Human Skin Aspect and Its Mechanical Properties. Clin. Cosmet. Investig. Dermatol. 2016, 9, 461–472. [Google Scholar] [CrossRef] [Green Version]
- Nikitovic, D.; Aggelidakis, J.; Young, M.F.; Iozzo, R.V.; Karamanos, N.K.; Tzanakakis, G.N. The Biology of Small Leucine-Rich Proteoglycans in Bone Pathophysiology. J. Biol. Chem. 2012, 287, 33926–33933. [Google Scholar] [CrossRef]
- Sgonc, R.; Gruber, J. Age-Related Aspects of Cutaneous Wound Healing: A Mini-Review. Gerontology 2013, 59, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Bejar, M.T.; Jimenez-Gomez, P.; Moutsopoulos, I.; Colom, B.; Han, S.; Calero-Nieto, F.J.; Göttgens, B.; Mohorianu, I.; Simons, B.D.; Alcolea, M.P. Defining the Transcriptional Signature of Esophageal-to-Skin Lineage Conversion. bioRxiv 2021. [Google Scholar] [CrossRef]
- Hsu, Y.C.; Fuchs, E. Building and Maintaining the Skin. Cold Spring Harb. Perspect. Biol. 2022, 14, a040840. [Google Scholar] [CrossRef] [PubMed]
- Cañedo-Dorantes, L.; Cañedo-Ayala, M. Skin Acute Wound Healing: A Comprehensive Review. Int. J. Inflam. 2019, 2019, 3706315. [Google Scholar] [CrossRef] [PubMed]
- Almadani, Y.H.; Vorstenbosch, J.; Davison, P.G.; Murphy, A.M. Wound Healing: A Comprehensive Review. Semin. Plast. Surg. 2021, 35, 141–144. [Google Scholar] [CrossRef]
- Gonzalez, A.C.D.O.; Andrade, Z.D.A.; Costa, T.F.; Medrado, A.R.A.P. Wound Healing—A Literature Review. An. Bras. Dermatol. 2016, 91, 614–620. [Google Scholar] [CrossRef] [Green Version]
- Gushiken, L.F.S.; Beserra, F.P.; Bastos, J.K.; Jackson, C.J.; Pellizzon, C.H. Cutaneous Wound Healing: An Update from Physiopathology to Current Therapies. Life 2021, 11, 665. [Google Scholar] [CrossRef]
- Sorg, H.; Tilkorn, D.J.; Hager, S.; Hauser, J.; Mirastschijski, U. Skin Wound Healing: An Update on the Current Knowledge and Concepts. Eur. Surg. Res. 2017, 58, 81–94. [Google Scholar] [CrossRef]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound Repair and Regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Tracy, L.E.; Minasian, R.A.; Caterson, E.J. Extracellular Matrix and Dermal Fibroblast Function in the Healing Wound. Adv. Wound Care 2016, 5, 119–136. [Google Scholar] [CrossRef]
- Wang, P.; Huang, B.; Horng, H.; Yeh, C. Wound Healing. J. Chin. Med. Assoc. 2018, 81, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Cherng, J.-H. The Strategies of Natural Polysaccharide in Wound Healing. In Wound Healing—Current Perspectives; Dogan, K.H., Ed.; IntechOpen: London, UK, 2018; ISBN 9781789855371. [Google Scholar]
- Zhong, L.; Simard, M.J.; Huot, J. Endothelial MicroRNAs Regulating the NF-KB Pathway and Cell Adhesion Molecules during Inflammation. FASEB J. 2018, 32, 4070–4084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khaidakov, M.; Wang, X.; Mehta, J.L. Potential Involvement of LOX-1 in Functional Consequences of Endothelial Senescence. PLoS ONE 2011, 6, e20964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu, R.; Jin, S.; Sun, P.; Haensel, D.; Nguyen, Q.H.; Dragan, M.; Kessenbrock, K.; Nie, Q.; Dai, X. Wound Healing in Aged Skin Exhibits Systems-Level Alterations in Cellular Composition and Cell-Cell Communication. Cell Rep. 2022, 40, 111155. [Google Scholar] [CrossRef]
- Sanchez, M.C.; Lancel, S.; Boulanger, E.; Neviere, R. Targeting Oxidative Stress and Mitochondrial Dysfunction in the Treatment of Impaired Wound Healing: A Systematic Review. Antioxidants 2018, 7, 98. [Google Scholar] [CrossRef] [Green Version]
- Ding, X.; Kakanj, P.; Leptin, M.; Eming, S.A. Regulation of the Wound Healing Response during Aging. J. Investig. Dermatol. 2021, 141, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- André-Lévigne, D.; Modarressi, A.; Pepper, M.S.; Pittet-Cuénod, B. Reactive Oxygen Species and NOX Enzymes Are Emerging as Key Players in Cutaneous Wound Repair. Int. J. Mol. Sci. 2017, 18, 2149. [Google Scholar] [CrossRef] [Green Version]
- Makrantonaki, E.; Wlaschek, M.; Scharffetter-Kochanek, K. Pathogenese von Wundheilungsstörungen Bei Älteren Patienten. JDDG J. Ger. Soc. Dermatol. 2017, 15, 255–275. [Google Scholar] [CrossRef] [Green Version]
- Jeya, R.; Samdavid, R.; Shvedova, M.; Shin, G.H.; Roh, D.S. An Insight into Aging, Senescence, and Their Impacts on Wound Healing. Adv. Geriatr. Med. Res. 2021, 3, e210017. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Effect of Aging on Wound Healing | Cell/Tissue/Organ Involved | Action | References |
|---|---|---|---|
| Prolong inflammatory phase | ↑Platelets | ↑Pro-inflammatory cytokines (e.g., PDGF, TGF-β & TGF-α) | [57] |
| ↓Adhesion molecules | Impairs the monocyte infiltration | [46] | |
| ↓Macrophage | ↓Granulation tissue formation, angiogenesis, collagen and growth factor synthesis ↓M2, hence prolong inflammation and halt tissue repair | [46,56] | |
| ↑Pro-inflammatory cytokines | Activates the COX pathway ↑PGE2 production | [35,56] | |
| ↑PGE2 | ↓Fibroblast and collagen synthesis, hence impairs the proliferative phase | [35] | |
| Oxidative stress | ↑Reactive oxygen species (ROS) | ↑Tissue damage, lipid peroxidation, promote protein breakdown and DNA damage, hence↑cell apoptosis and senescence | [23,64] |
| Inefficient microcirculation | Impaired blood vessels | ↓Inflammatory cells and chemical mediators at injury site Relative hypoperfusion at injury site Hypoxia that causes cell death due to apoptosis and necrosis | [5,64] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khalid, K.A.; Nawi, A.F.M.; Zulkifli, N.; Barkat, M.A.; Hadi, H. Aging and Wound Healing of the Skin: A Review of Clinical and Pathophysiological Hallmarks. Life 2022, 12, 2142. https://doi.org/10.3390/life12122142
Khalid KA, Nawi AFM, Zulkifli N, Barkat MA, Hadi H. Aging and Wound Healing of the Skin: A Review of Clinical and Pathophysiological Hallmarks. Life. 2022; 12(12):2142. https://doi.org/10.3390/life12122142
Chicago/Turabian StyleKhalid, Kamarul Ariffin, Ahmad Faris Mohd Nawi, Nuraqilah Zulkifli, Md. Abul Barkat, and Hazrina Hadi. 2022. "Aging and Wound Healing of the Skin: A Review of Clinical and Pathophysiological Hallmarks" Life 12, no. 12: 2142. https://doi.org/10.3390/life12122142