
Treatment of Severe Atopic Dermatitis with Dupilumab in Three Patients with Renal Diseases

 and
and
Abstract
:1. Introduction
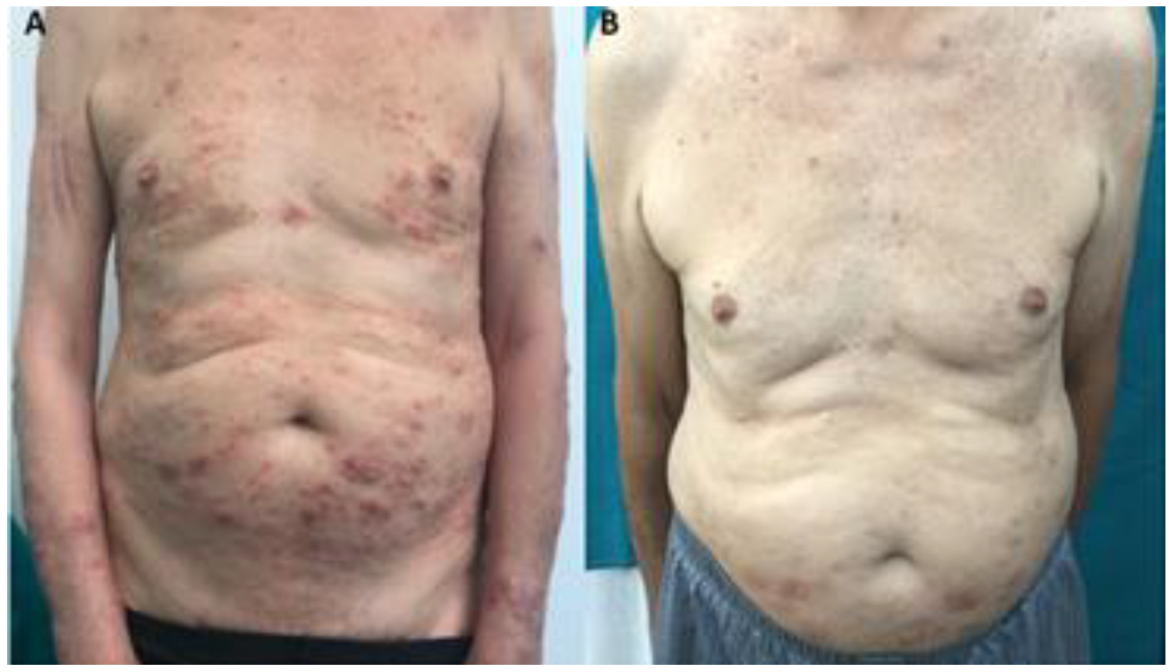
2. Report of Cases
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gooderham, M.J.; Hong, H.C.; Eshtiaghi, P.; Papp, K.A. Dupilumab: A review of its use in the treatment of atopic dermatitis. J. Am. Acad. Dermatol. 2018, 78 (Suppl. 1), S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Drucker, A.M.; Lam, M.; Flohr, C.; Thyssen, J.; Kabashima, K.; Bissonnette, R.; Dlova, N.C.; Aoki, V.; Chen, M.; Yu, J.; et al. Systemic Therapy for Atopic Dermatitis in older adults and adults with comorbidities: A scoping review and international eczema council survey. Dermatitis 2022, 33, 200–220. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Pulleiro, R.; García-Murias, M.; Fidalgo-Díaz, M.; García-González, M.Á. Molecular basis, diagnostic challenges and therapeutic approaches of alport syndrome: A primer for clinicians. Int. J. Mol. Sci. 2021, 22, 11063. [Google Scholar] [CrossRef] [PubMed]
- Patruno, C.; Napolitano, M.; Argenziano, G.; Peris, K.; Ortoncelli, M.; Girolomoni, G.; Offidani, A.; Ferrucci, S.M.; Amoruso, G.F.; Rossi, M.; et al. DADE-dupilumab for atopic dermatitis of the elderly study group. dupilumab therapy of atopic dermatitis of the elderly: A multicentre, real-life study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Makar, M.; Smyth, B.; Brennan, F. chronic kidney disease-associated pruritus: A review. Kidney Blood Press Res. 2021, 46, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.L.; Savage, K.T.; Qiu, C.C.; Jin, A.; Valdes-Rodriguez, R.; Mollanazar, N.K. Chronic pruritus responding to dupilumab-a case series. Medicines 2019, 6, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kha, C.; Raji, K.; Chisolm, S. treatment of atopic dermatitis with dupilumab in a renal transplant patient. Dermatitis 2020, 31, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Elamin, S.; Murphy, B. Dupilumab in the management of atopic dermatitis in an immunosuppressed renal transplant patient. Clin. Exp. Dermatol. 2022, 47, 1191–1193. [Google Scholar] [CrossRef] [PubMed]
- Varma, A.; Tassavor, M.; Levitt, J. The utility of dupilumab for use in the pediatric population. JAAD Case Rep. 2019, 5, 943–944. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.Q.; Chen, H.; Qiu, L.R.; Zhu, R.F. Case report: The application of dupilumab in atopic dermatitis children complicated with nephrotic syndrome. Front. Med. 2022, 9, 813313. [Google Scholar] [CrossRef] [PubMed]
- Ruszkowski, J.; Lisowska, K.A.; Pindel, M.; Heleniak, Z.; Dębska-Ślizień, A.; Witkowski, J.M. T cells in IgA nephropathy: Role in pathogenesis, clinical significance and potential therapeutic target. Clin. Exp. Nephrol. 2019, 23, 291–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Lee, S.Y.; Kim, J.S.; Kim, D.R.; Jung, S.W.; Jeong, K.H.; Lee, T.W.; Lee, Y.H.; Kim, Y.G.; Moon, J.Y.; et al. Elevated serum immunoglobulin E level as a marker for progression of immunoglobulin A nephropathy. Kidney Res. Clin. Pract. 2016, 35, 147–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanczosova, M.; Arenberger, P.; Rychlik, I.; Arenbergerova, M.; Gkalpakiotis, S. Improvement of atopic dermatitis and IgA nephropathy in a patient treated by dupilumab. Dermatol. Ther. 2021, 34, 14708. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Kawase, Y.; Nakajima, E.; Matsuura, Y.; Akita, W.; Aoki, R.; Suzuki, Y.; Mitsui, H. Exacerbation of IgA nephropathy in a patient receiving dupilumab. JAAD Case Rep. 2022, 21, 150–153. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient 1 | Patient 2 | Patient 3 | ||||
|---|---|---|---|---|---|---|
| Age at Baseline (yrs) | 36 | 44 | 77 | |||
| Renal disease | Alport syndrome | IgA nephropathy | Hypertensive nephrosclerosis | |||
| Concomitant treatment | Ramipril | Ramipril | Nifedipine | |||
| Previous treatmentsfor AD ^ | Emollients, topical corticosteroids, phototherapy | Emollients, topical corticosteroids | Emollients, topical corticosteroids | |||
| T0 | T1 | T0 | T1 | T0 | T1 | |
| EASI score | 31 | 1 | 27 | 0 | 37.5 | 6 |
| P-NRS | 7 | 2 | 7 | 0 | 10 | 4 |
| IGA score | 4 | 1 | 4 | 0 | 4 | 1 |
| DLQI score | 20 | 1 | 15 | 0 | 25 | 2 |
| Serum IgE (IU/mL) | 50.1 | 40 | 145 | 58.7 | 103 | 55 |
| Eosinophils (%) | 5.1 | 4.5 | 2.1 | 2 | 13.3 | 10.7 |
| Serum creatinine (mg/dL) | 2.15 | 1.87 | 0.90 | 1.05 | 4.85 | 4.94 |
| eGFR (mL/min/1.73 m2) | 38 | 43 | 97 | 86 | 12 | 12 |
| Proteinuria (g/24 h) | 2.40 | 2.50 | 1.61 | 1.39 | 1.2 | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foti, C.; Romita, P.; Ambrogio, F.; Manno, C.; Filotico, R.; Cassano, N.; Vena, G.A.; De Marco, A.; Cazzato, G.; Mennuni, B.G. Treatment of Severe Atopic Dermatitis with Dupilumab in Three Patients with Renal Diseases. Life 2022, 12, 2002. https://doi.org/10.3390/life12122002
Foti C, Romita P, Ambrogio F, Manno C, Filotico R, Cassano N, Vena GA, De Marco A, Cazzato G, Mennuni BG. Treatment of Severe Atopic Dermatitis with Dupilumab in Three Patients with Renal Diseases. Life. 2022; 12(12):2002. https://doi.org/10.3390/life12122002
Chicago/Turabian StyleFoti, Caterina, Paolo Romita, Francesca Ambrogio, Carlo Manno, Raffaele Filotico, Nicoletta Cassano, Gino Antonio Vena, Aurora De Marco, Gerardo Cazzato, and Biagina Gisella Mennuni. 2022. "Treatment of Severe Atopic Dermatitis with Dupilumab in Three Patients with Renal Diseases" Life 12, no. 12: 2002. https://doi.org/10.3390/life12122002