
Artificial Intelligence in Cancer Research: Trends, Challenges and Future Directions

Abstract
:1. Introduction
2. Cancer Statistics
3. Conventional Practices for Cancer Diagnosis and Treatment
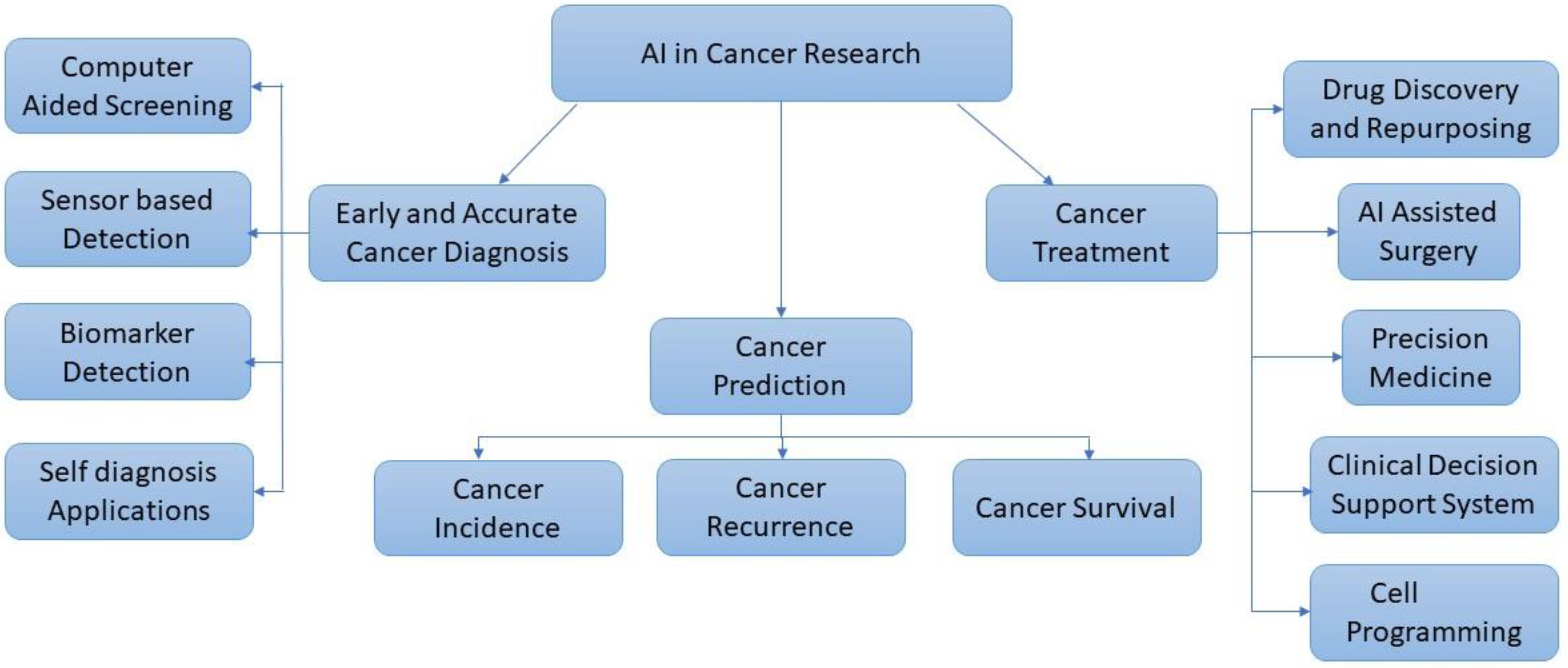
4. AI for Cancer Research
4.1. Cancer Data Repositories
- Ancora.ai.
- Be the Match: Jason Carter Clinical Trial Search and Support Program
- Bladder Cancer Advocacy Network
- BreastCancerTrials.org
- Center for Information and Study on Clinical Research Participation (CISCRP)
- CenterWatch
- ClinicalTrials.gov.
- EmergingMed Clinical Trial Navigator Service
- Lazarex Cancer Foundation
- Melanoma Research Alliance
- Metastatic Breast Cancer Project
- Metastatic Prostate Cancer Project
- National Brain Tumor Society Clinical Trial Finder
- National Cancer Institute (NCI) Clinical Trials
- Pancreatic Cancer Action Network Clinical Trial Finder
- SPOHNC Clinical Trial Navigation Service
- Targeted Agent and Profiling Utilization Registry (TAPUR) Study
- The Leukemia & Lymphoma Society Clinical Trial Support Center
- Us TOO Prostate Cancer Clinical Trial Finder
- World Health Organization (WHO) International Clinical Trials Registry Platform.
4.1.1. Types of Cancer Data Repositories
4.1.2. Radiographic Images
- Cancer Imaging Program (CIP) [22]: The National Cancer Institute’s (NCI) CIP supports and promotes basic, translational, and clinical imaging research related to cancer, as well as the integration and application of these imaging advancements to the study of cancer biology and the treatment of cancer and cancer risk.
- Cancercentre.ai [23]: It contains data like screenshots from the radiology platform that depict MRI of the prostate (T2-weighted images in axial plane). It provides trained radiologists with pre-screened images and identified features.
- The Cancer Imaging Archive (TCIA) [24]: TCIA has a sizable collection of medical photographs of cancer that are available for download by the general public. The image modality, or image type supplied are MRI, CT, digital histopathology, etc.
4.1.3. Genomic and Molecular Data
- The Cancer Genome Atlas (TCGA): Over 20,000 cancer samples from 33 different cancer types are characterised as TCGA, a popularly utilised public database for cancer research that produces numerous types of data and tools [20].
- International Cancer Genome Consortium (ICGC) [35]: In 50 of the most significant cancer forms, it maps the genetic flaws. Worldwide cancer researchers are given free access to all the data from the 25,000 cancer samples that were examined.
- cBioPortalData [36]: It allows visualization, analysis, and import of cBioPortal datasets as MultiAssayExperiment objects in Bioconductor.
- Genomics of Drug Sensitivity in Cancer [37]: It characterizes over a thousand human cancer cell lines, and hundreds of chemicals are tested on them. It also offers information on drug response as well as genomic-sensitivity markers.
- Cancer Cell Line Encyclopedia (CCLE) [38]: This is useful for investigating cancer biology, identifying cancer targets, and determining treatment efficacy.
- LinkedOmics [39]: It offers a platform for accessing, analysing, and comparing cancer multi-omics data inside and across tumour types.
4.1.4. Pathological Images
- Whole Slide Imaging Repository [47]: Pathology departments use scanned photos of traditional glass slides to create digital slides as their imaging method.
- Cancer Digital Slide Archive [48]: It hosts pathological images maintained by TCGA.
4.1.5. Clinical Data and Blood Profiling
- Data-CAN [50]: It is a cancer-data-knowledge network that was co-created in order to produce better results and greater social benefits for cancer research.
- Optum Oncology EHR data [51]: Optum data include vital signs, symptoms, problem descriptions, clinical evaluations, lab results, techniques, diagnoses, surgeries, and therapies. Additionally, it contains information about the cancer’s stage, grade, histology, genetic mutations, other blood biomarkers, lines of therapy, and assessments of the disease’s development and drug response to further increase its usefulness to oncology.
4.2. Using Cloud AI Platforms
4.3. AI for Cancer Prediction
4.4. AI for Cancer Diagnosis
4.5. AI for Cancer Treatment
5. Challenges
5.1. Technical Challenges
5.2. Ethical Challenges
6. Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Adeoye, J.; Akinshipo, A.; Thomson, P.; Su, Y.-X. Artificial intelligence-based prediction for cancer-related outcomes in Africa: Status and potential refinements. J. Glob. Health 2022, 12, 03017. [Google Scholar] [CrossRef]
- Pavlopoulou, A.; Spandidos, D.; Michalopoulos, I. Human cancer databases (Review). Oncol. Rep. 2014, 33, 3–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, Y.; Gupta, S.; Singla, R.; Hu, Y. A Systematic Review of Artificial Intelligence Techniques in Cancer Prediction and Diagnosis. Arch. Comput. Methods Eng. 2021, 29, 2043–2070. [Google Scholar] [CrossRef]
- Iqbal, M.; Javed, Z.; Sadia, H.; Qureshi, I.; Irshad, A.; Ahmed, R.; Malik, K.; Raza, S.; Abbas, A.; Pezzani, R.; et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: Looking into the future. Cancer Cell Int. 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dias, R.; Torkamani, A. Artificial Intelligence in clinical and Genomic Diagnostics. Genome Med. 2019, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Cancer. Who. Int. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 13 October 2022).
- Available online: https://www.mckinsey.com/industries/life-sciences/our-insights/playing-to-win-in-oncology-key-capabilities-for-success (accessed on 14 October 2022).
- Available online: https://www.mckinsey.com/industries/life-sciences/our-insights/delivering-innovation-2020-oncology-market-outlook (accessed on 14 October 2022).
- GLOBOCAN 2020: New Global Cancer Data|UICC. Uicc.Org. 2022. Available online: https://www.uicc.org/news/globocan-2020-new-global-cancer-data (accessed on 13 October 2022).
- Lee, D.; Yoon, S. Application of Artificial Intelligence-Based Technologies in the Healthcare Industry: Opportunities and Challenges. Int. J. Environ. Res. Public Health 2021, 18, 271. [Google Scholar] [CrossRef]
- Lee, H.; Chen, Y. Image Based Computer Aided Diagnosis System for Cancer Detection. Expert Syst. Appl. 2015, 42, 5356–5365. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0957417415000986?via%3Dihub (accessed on 13 October 2022).
- Mirbabaie, M.; Stieglitz, S.; Frick, N. Artificial intelligence in disease diagnostics: A critical review and classification on the current state of research guiding future direction. Health Technol. 2021, 11, 693–731. [Google Scholar] [CrossRef]
- National Cancer Institute. Can Artificial Intelligence Help See Cancer in New Ways? National Cancer Institute: Bethesda, MD, USA, 2022. Available online: https://www.cancer.gov/news-events/cancer-currents-blog/2022/artificial-intelligence-cancer-imaging (accessed on 13 October 2022).
- Ginghina, O.; Hudita, A.; Zamfir, M.; Spanu, A.; Mardare, M.; Bondoc, I.; Buburuzan, L.; Georgescu, S.E.; Costache, M.; Negrei, C.; et al. Liquid Biopsy and Artificial Intelligence as Tools to Detect Signatures of Colorectal Malignancies: A Modern Approach in Patient’s Stratification. Front. Oncol. 2022, 12, 856575. [Google Scholar] [CrossRef]
- Mascalchi, M.; Sali, L. Lung cancer screening with low dose CT and radiation harm from prediction models to cancer incidence data. Ann. Transl. Med. 2017, 5, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.; Albizri, A.; Harfouche, A.; Fosso-Wamba, S. Integrating human knowledge into artificial intelligence for complex and ill-structured problems: Informed artificial intelligence. Int. J. Inf. Manag. 2022, 64, 102479. [Google Scholar] [CrossRef]
- Zhou, J.; Cao, W.; Wang, L.; Pan, Z.; Fu, Y. Application of artificial intelligence in the diagnosis and prognostic prediction of ovarian cancer. Comput. Biol. Med. 2022, 146, 105608. [Google Scholar] [CrossRef] [PubMed]
- Shreve, J.; Khanani, S.; Haddad, T. Artificial Intelligence in Oncology: Current Capabilities, Future Opportunities, and Ethical Considerations. Am. Soc. Clin. Oncol. Educ. Book 2022, 42, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Deo, S. Computerized clinical database development in oncology. Indian J. Palliat. Care 2011, 17, 2. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Program. National Cancer Institute. 2022. Available online: https://www.cancer.gov/about-nci/organization/ccg/research/structural-genomics/tcga (accessed on 13 October 2022).
- Finding a Clinical Trial. Cancer.Net. 2022. Available online: https://www.cancer.net/research-and-advocacy/clinical-trials/finding-clinical-trial (accessed on 13 October 2022).
- Cancer Imaging Program. Cancer Imaging Program (CIP). (n.d.). Available online: https://imaging.cancer.gov/ (accessed on 18 November 2022).
- Cancer Center. AI-AI in Oncology. Cancer Center.AI-AI in Oncology and Pathology. 25 October 2022. Available online: https://cancercenter.ai/ (accessed on 18 November 2022).
- Welcome to the Cancer Imaging Archive. The Cancer Imaging Archive (TCIA). 16 July 2020. Available online: https://www.cancerimagingarchive.net/ (accessed on 18 November 2022).
- Innovation Insight for AI-Enabled Diagnostic Imaging Interpretation for Healthcare Provider CIOs. Gartner. 2022. Available online: https://www.gartner.com/en/documents/4000308 (accessed on 13 October 2022).
- Prior, F.; Smith, K.; Sharma, A.; Kirby, J.; Tarbox, L.; Clark, K.; Bennett, W.; Nolan, T.; Freymann, J. The public cancer radiology imaging collections of The Cancer Imaging Archive. Sci. Data 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial Intelligence in cancer imaging: Clinical challenges and applications. CA A Cancer J. Clinicians 2019, 69, 127–157. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, S.; Wang, H.; Liu, Y.; Garcia, A.; Stringfield, O.; Krewer, H.; Li, Q.; Cherezov, D.; Gatenby, R.A.; Balagurunathan, Y.; et al. Predicting malignant nodules from screening CT scans. J. Thorac. Oncol. 2016, 11, 2120–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Balagurunathan, Y.; Atwater, T.; Antic, S.; Li, Q.; Walker, R.C.; Smith, G.T.; Massion, P.P.; Schabath, M.B.; Gillies, R.J. Radiological image traits predictive of cancer status in pulmonary nodules. Clin. Cancer Res. 2017, 23, 1442–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Song, G.; Zang, Y.; Jia, J.; Wang, C.; Li, C.; Tian, J.; Dong, D.; Zhang, Y. Noninvasive radiomics approach potentially predicts non-functioning pituitary adenomas subtypes before surgery. Eur. Radiol. 2018, 28, 3692–3701. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-targeted or standard biopsy for prostate-cancer diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Balachandar, N.; Lam, C.K.; Yi, D.; Brown, J.; Beers, A.; Rosen, B.R.; Rubin, D.L.; Kalpathy-Cramer, J. Distributed deep learning networks among institutions for medical imaging. J. Am. Med. Inform. Assoc. 2018, 25, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Limkin, E.J.; Vakalopoulou, M.; Dercle, L.; Champiat, S.; Han, S.R.; Verlingue, L.; Brandao, D.; Lancia, A.; Ammari, S.; et al. A radiomics approach to assess tumor-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy. An imaging biomarker, retrospective multicohort study. Lancet Oncol. 2018, 19, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Yun, T.J.; Park, C.K.; Kim, J.-H.; Sohn, C.-H.; Won, J.K.; Park, S.-H.; Kim, I.H.; Choi, S.H. Combined use of susceptibility weighted magnetic resonance imaging sequences and dynamic susceptibility contrast perfusion weighted imaging to improve the accuracy of the differential diagnosis of recurrence and radionecrosis in high-grade glioma patients. Oncotarget 2017, 8, 20340–20353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ICGC Data Portal. Dcc.Icgc.Org. (n.d.). Available online: https://dcc.icgc.org/ (accessed on 18 November 2022).
- CBioPortal for Cancer Genomics. cBioPortal for Cancer Genomics. (n.d.). Available online: https://www.cbioportal.org/ (accessed on 18 November 2022).
- Genomics of Drug Sensitivity in Cancer. CancerRxGenes. (n.d.). Available online: https://www.cancerrxgene.org/ (accessed on 18 November 2022).
- Cancer Cell Line Encyclopedia (CCLE). OpenScholar. (n.d.). Available online: https://sites.broadinstitute.org/ccle/ (accessed on 18 November 2022).
- LinkedOmics Data Source. LinkedOmics. (n.d.). Available online: http://www.linkedomics.org/login.php#dataSource (accessed on 18 November 2022).
- Creighton, C. Making Use of Cancer Genomic Databases. Curr. Protoc. Mol. Biol. 2018, 121, 19.14.1–19.14.13. [Google Scholar] [CrossRef] [PubMed]
- Shao, D.; Dai, Y.; Li, N.; Cao, X.; Zhao, W.; Cheng, L.; Rong, Z.; Huang, L.; Wang, Y.; Zhao, J. Artificial intelligence in clinical research of cancers. Brief. Bioinform. 2022, 23, bbab523. [Google Scholar] [CrossRef]
- Chen, Z.H.; Lin, L.; Wu, C.F.; Li, C.F.; Xu, R.H.; Sun, Y. Artificial Intelligence for assisting cancer diagnosis and treatment in the era of Precision Medicine. Cancer Commun. 2021, 41, 1100–1115. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.M.; Michelini, V.V.; Snell, J.M.; Balu, S.; Hoyle, A.P.; Parker, J.S.; Hayward, M.C.; Eberhard, D.A.; Salazar, A.H.; McNeillie, P.; et al. Next-Generation Sequencing-Guided Cancer Care Through Cognitive Computing. Oncologist 2018, 23, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Jaganathan, K.; Panagiotopoulou, S.K.; McRae, J.F.; Darbandi, S.F.; Knowles, D.; Li, Y.I.; Kosmicki, J.A.; Arbelaez, J.; Cui, W.; Schwartz, G.B.; et al. Predicting splicing from primary sequence with deep learning. Cell 2019, 176, 535–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Cao, H.; Zhang, J.Z.H.; Qi, Y. Computational protein design with deep learning neural networks. Sci. Rep. 2018, 8, 6349. [Google Scholar] [CrossRef]
- Zhang, H.; Qureshi, M.A.; Wahid, M.; Charifa, A.; Ehsan, A.; Andrew, I.; De Dios, I.; Ma, W.; Sharma, I.; McCloskey, J.; et al. Differential diagnosis of hematologic and solid tumors using targeted transcriptome and artificial intelligence. Am. J. Pathol. 2022. [Google Scholar] [CrossRef]
- Whole Slide Imaging Repository. DPA. (n.d.). Available online: https://digitalpathologyassociation.org/whole-slide-imaging-repository (accessed on 18 November 2022).
- Digital Slide Archive (DSA). (n.d.). Available online: https://cancer.digitalslidearchive.org/ (accessed on 18 November 2022).
- Clinical Validation, DKK1 Chromogenic In-Situ Hybridization, (CISH) Assay, Image Analysis, Pathologist, Wnt Signaling, CD8 Inflammation, Heterogeneity, Dako PD-L1, io, Cytotoxic CD8 T Cell, Non-Small Cell Lung Cancer, NSCLC, Companion Diagnostic, Protein Tyrosine Kinase 7, PTK7 Biomarker Analysis Posters & Publications Archive. Flagship Biosciences. 5 May 2022. Available online: https://www.flagshipbio.com/posters-publications/ (accessed on 17 November 2022).
- Clinical Datasets. DATA. 24 February 2022. Available online: https://www.data-can.org.uk/health-data/datasets/ (accessed on 18 November 2022).
- Electronic Health Records (EHR) Data. Optum. (n.d.). Available online: https://www.optum.com/business/life-sciences/real-world-data/ehr-data.html (accessed on 18 November 2022).
- Wang, L.; Fu, S.; Wen, A.; Ruan, X.; He, H.; Liu, S.; Moon, S.; Mai, M.; Riaz, I.B.; Wang, N.; et al. Assessment of electronic health record for cancer research and patient care through a scoping review of Cancer Natural Language Processing. JCO Clin. Cancer Inform. 2022, 6, e2200006. [Google Scholar] [CrossRef] [PubMed]
- AI in Cancer Detection and Treatment: Applications, Benefits, and Challenges-ITRex. ITRex. 2022. Available online: https://itrexgroup.com/blog/ai-in-cancer-detection-treatment-applications-benefits-challenges/# (accessed on 14 October 2022).
- Jin, A.; Gomez, S.; Luft, H.; Lichtensztajn, D.; Thompson, C. External validity of electronic health record studies of cancer patients. J. Patient-Cent. Res. Rev. 2017, 4, 150. [Google Scholar] [CrossRef]
- Hunter, B.; Hindocha, S.; Lee, R. The Role of Artificial Intelligence in Early Cancer Diagnosis. Cancers 2022, 14, 1524. [Google Scholar] [CrossRef] [PubMed]
- News.Microsoft.Com. 2022. Available online: https://news.microsoft.com/stories/computingcancer/ (accessed on 13 October 2022).
- Google Cloud Enables the National Cancer Institute’s Institute for Systems Biology-Cancer Gateway in the Cloud to Support Breast Cancer Research with Fast and Secure Data Sharing|Google Cloud Blog. Google Cloud Blog. 2022. Available online: https://cloud.google.com/blog/topics/public-sector/google-cloud-enables-national-cancer-institutes-institute-systems-biology-cancer-gateway-cloud-support-breast-cancer-research-fast-and-secure-data-sharing (accessed on 13 October 2022).
- Kowalewski, K.; Egen, L.; Fischetti, C.; Puliatti, S.; Juan, G.; Taratkin, M.; Ines, R.B.; Abate, M.A.S.; Mühlbauer, J.; Wessels, F.; et al. Artificial intelligence for renal cancer: From imaging to histology and beyond. Asian J. Urol. 2022, 9, 243–252. [Google Scholar] [CrossRef]
- Venkatesan, D.; Elangovan, A.; Winster, H.; Pasha, M.; Abraham, K.; Satheeshkumar, J.; Sivaprakash, P.; Niraikulam, A.; Gopalakrishnan, A.V.; Narayanasamy, A.; et al. Diagnostic and therapeutic approach of artificial intelligence in neuro-oncological diseases. Biosens. Bioelectron. 2022, 11, 100188. [Google Scholar] [CrossRef]
- Yirmibesoglu Erkal, E.; Akpınar, A.; Erkal, H. Ethical evaluation of artificial intelligence applications in radiotherapy using the Four Topics Approach. Artif. Intell. Med. 2021, 115, 102055. [Google Scholar] [CrossRef]
- Luk, S.; Ford, E.; Phillips, M.; Kalet, A. Improving the Quality of Care in Radiation Oncology using Artificial Intelligence. Clin. Oncol. 2022, 34, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Bohr, A.; Memarzadeh, K. The rise of artificial intelligence in healthcare applications. Artif. Intell. Healthc. 2020, 25–60. [Google Scholar] [CrossRef]
- Cool Vendors in AI Governance and Responsible AI. Gartner. 2022. Available online: https://www.gartner.com/en/documents/4002446 (accessed on 14 October 2022).
- Available online: https://www.cnbc.com/2017/05/11/from-coding-to-cancer-how-ai-is-changing-medicine.html (accessed on 13 October 2022).
- Rani, P.; Dutta, K.; Kumar, V. Artificial intelligence techniques for prediction of drug synergy in malignant diseases: Past, present, and future. Comput. Biol. Med. 2022, 144, 105334. [Google Scholar] [CrossRef]
- Available online: https://www.mckinsey.com/~/media/McKinsey/Industries/Healthcare%20Systems%20and%20Services/Our%20Insights/The%20next%20wave%20of%20innovation%20in%20oncology/The-next-wave-of-innovation-in-oncology.ashx (accessed on 14 October 2022).
- Cancer Moonshot℠. National Cancer Institute. 2022. Available online: https://www.cancer.gov/research/key-initiatives/moonshot-cancer-initiative (accessed on 14 October 2022).
- Allen, F.; Crepaldi, L.; Alsinet, C.; Strong, A.; Kleshchevnikov, V.; De Angeli, P.; Páleníková, P.; Khodak, A.; Kiselev, V.; Kosicki, M.; et al. Predicting the mutations generated by repair of Cas9-induced double-strand breaks. Nat. Biotechnol. 2018, 37, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.; Somasundaram, L.; Raj, I.; Ic-Mex, D.; Phal, A.; Schmidt, S.; Ng, W.I.; Mar, D.; Decarreau, J.; Moss, N.; et al. dCas9 fusion to computer-designed PRC2 inhibitor reveals functional TATA box in distal promoter region. Cell Rep. 2022, 38, 110457. [Google Scholar] [CrossRef]
- Park, Y.; Casey, D.; Joshi, I.; Zhu, J.; Cheng, F. Emergence of New Disease: How Can Artificial Intelligence Help? Trends Mol. Med. 2020, 26, 627–629. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. The Tech Revolutionizing Cancer Research and Care; National Cancer Institute: Bethesda, MD, USA, 2022. Available online: https://www.cancer.gov/news-events/nca50/stories/technologies-and-innovations (accessed on 13 October 2022).


{kind=link}
| Cancer Type | Deaths |
|---|---|
| Lung | 10,000,000 |
| Colon and Rectum | 916,000 |
| Liver | 830,000 |
| Stomach | 769,000 |
| Breast | 685,000 |
| Cancer Type | New Cases |
|---|---|
| Breast | 2,260,000 |
| Lung | 2,210,000 |
| Colon and Rectum | 1,930,000 |
| Prostrate | 1,410,000 |
| skin (non-melanoma) | 1,210,000 |
| Stomach | 1,090,000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sebastian, A.M.; Peter, D. Artificial Intelligence in Cancer Research: Trends, Challenges and Future Directions. Life 2022, 12, 1991. https://doi.org/10.3390/life12121991
Sebastian AM, Peter D. Artificial Intelligence in Cancer Research: Trends, Challenges and Future Directions. Life. 2022; 12(12):1991. https://doi.org/10.3390/life12121991
Chicago/Turabian StyleSebastian, Anu Maria, and David Peter. 2022. "Artificial Intelligence in Cancer Research: Trends, Challenges and Future Directions" Life 12, no. 12: 1991. https://doi.org/10.3390/life12121991