
Acute Respiratory Distress Syndrome and the Use of Inhaled Pulmonary Vasodilators in the COVID-19 Era: A Narrative Review
 ,
,
Abstract
:1. Introduction
2. Methods
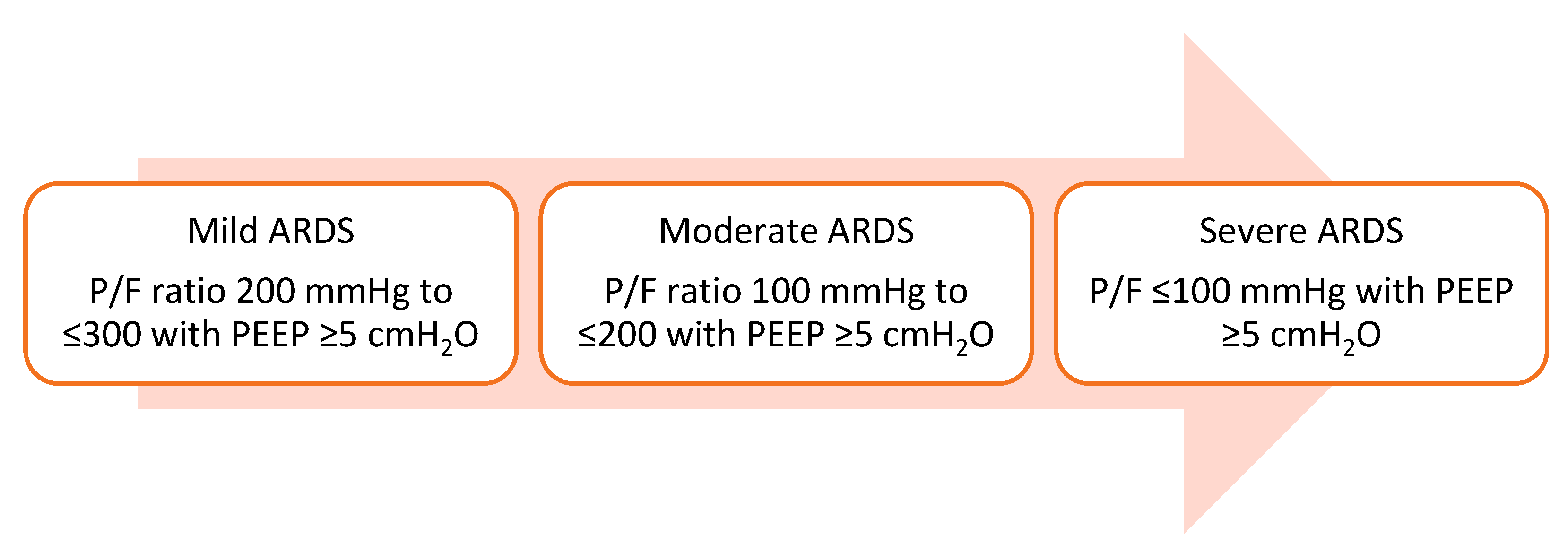
2.1. Definition of Acute Respiratory Distress Syndrome
2.2. Pathophysiology of ARDS and COVID-19-Related ARDS (CARDS)
2.2.1. An Overview of the Pathogenesis of ARDS
2.2.2. Tissue Injury and Exudative Phase
2.2.3. Proliferative Phase
2.3. Pathogenesis of COVID-19-Associated Acute Respiratory Distress Syndrome (CARDS)
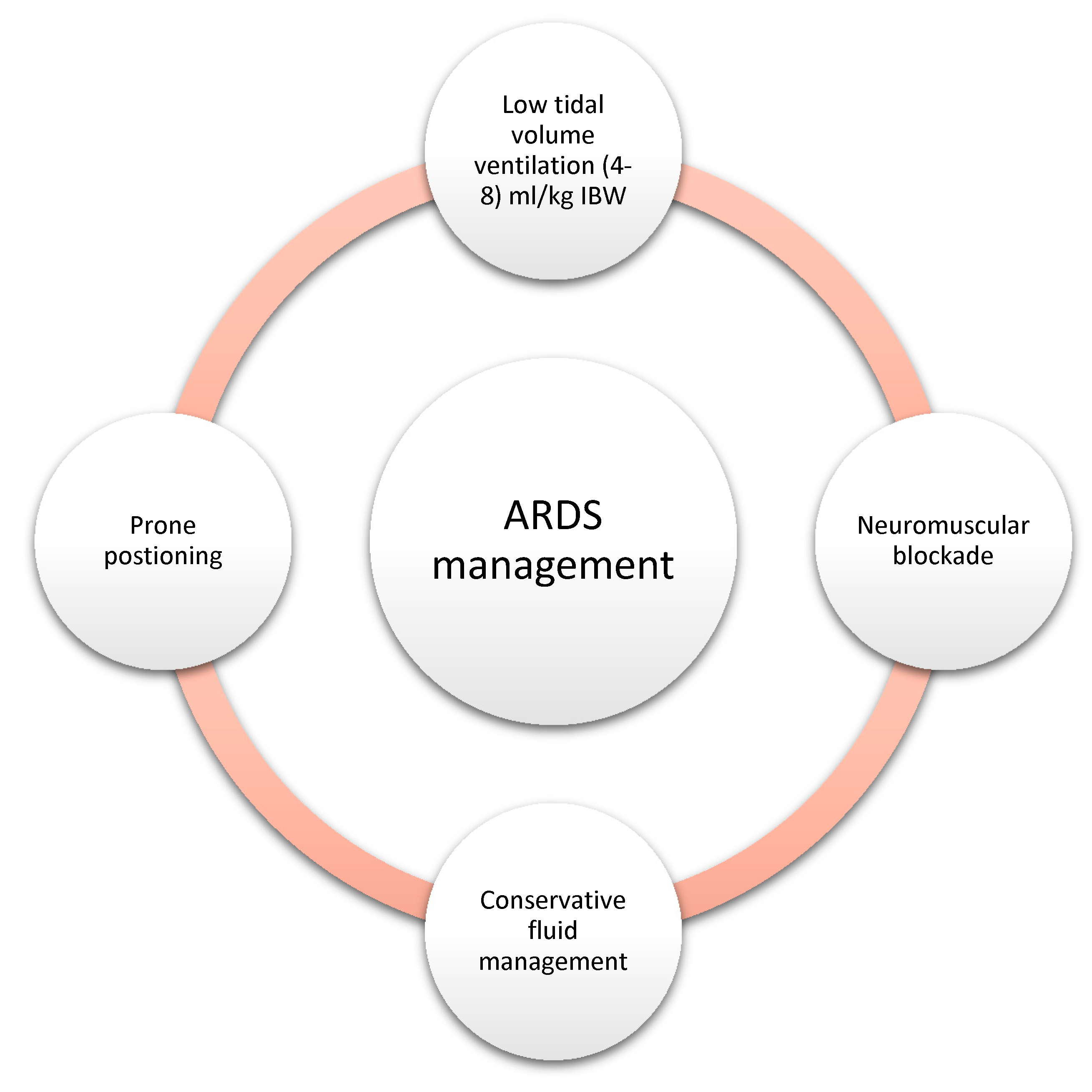
2.4. Standard Therapies for ARDS
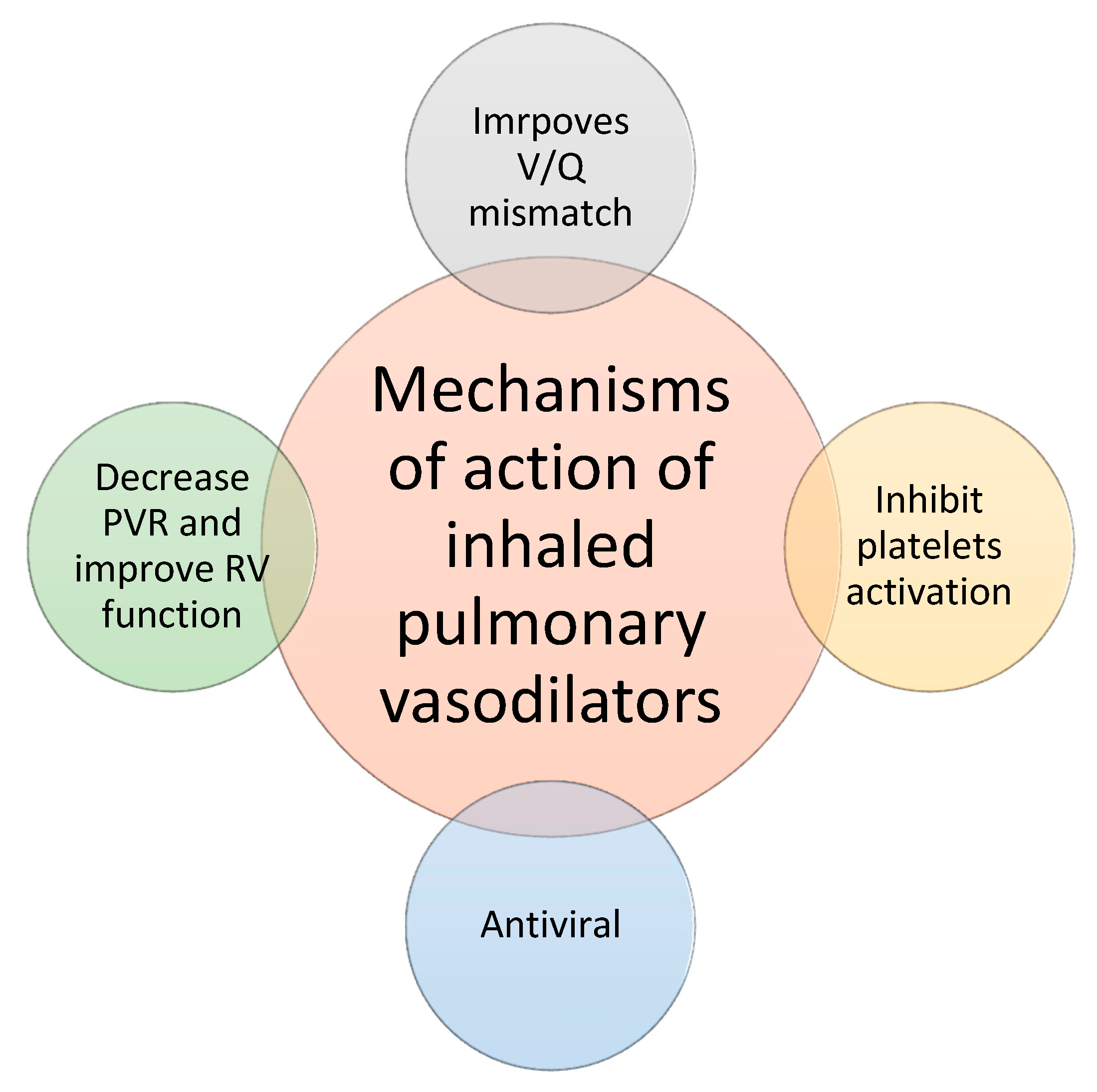
2.5. Principles of Inhaled Pulmonary Vasodilators
3. Inhaled Nitric Oxide
3.1. Introduction
3.2. Mechanism of Action
3.3. Metabolism of NO
3.4. Adverse Effects
3.4.1. Hypotension
3.4.2. Methemoglobinemia
3.4.3. Platelet Inhibition and Prolonged Bleeding Time
3.4.4. Pulmonary Edema in Heart Failure
3.4.5. Rebound Hypoxia and Pulmonary Hypertension on Withdrawal
3.4.6. Renal Failure
3.5. Weaning of Inhaled Nitric Oxide
3.6. How to Administer Inhaled Nitric Oxide
4. Inhaled NO Use in the COVID Era
4.1. Role of iNO in Moderate to Severe CARDS
4.2. Role of iNO in Mild COVID-19 Infection
4.3. Preventive Role of NO and Limitations of Its Use
5. Inhaled Prostaglandins
5.1. Introduction
5.2. Metabolism of Inhaled Prostaglandins
5.3. Adverse Events of Inhaled Prostaglandins
5.4. Weaning of Inhaled Prostaglandins
5.5. Equipment for Inhaled Prostaglandins Use
5.6. Inhaled Prostaglandins Use in the COVID Era
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Force, T.A.D.T. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Fujishima, S. Pathophysiology and biomarkers of acute respiratory distress syndrome. J. Intensive Care 2014, 2, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiener-Kronish, J.P.; Albertine, K.H.; Matthay, M.A. Differential responses of the endothelial and epithelial barriers of the lung in sheep to Escherichia coli endotoxin. J. Clin. Investig. 1991, 88, 864–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, L.B.; Matthay, M.A. Alveolar fluid clearance is impaired in the majority of patients with acute lung injury and the acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2001, 163, 1376–1383. [Google Scholar] [CrossRef]
- Swenson, K.E.; Swenson, E.R. Pathophysiology of Acute Respiratory Distress Syndrome and COVID-19 Lung Injury. Crit. Care Clin. 2021, 37, 749–776. [Google Scholar] [CrossRef]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Tian, S.; Hu, W.; Niu, L.; Liu, H.; Xu, H.; Xiao, S.-Y. Pulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung Cancer. J. Thorac. Oncol. 2020, 15, 700–704. [Google Scholar] [CrossRef]
- Gibson, L.E.; Fenza, R.D.; Lang, M.; Capriles, M.I.; Li, M.D.; Kalpathy-Cramer, J.; Little, B.P.; Arora, P.; Mueller, A.L.; Ichinose, F.; et al. Right Ventricular Strain Is Common in Intubated COVID-19 Patients and Does Not Reflect Severity of Respiratory Illness. J. Intensive Care Med. 2021, 36, 900–909. [Google Scholar] [CrossRef]
- THE ACUTE RESPIRATORY DISTRESS SYNDROME NETWORK. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Forel, J.-M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.-M.; Perez, D.; Seghboyan, J.-M.; et al. Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Comparison of Two Fluid-Management Strategies in Acute Lung Injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ferrando, C.; Martínez, D.; Ambrós, A.; Muñoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; González-Higueras, E.; Conesa, L.A.; et al. Dexamethasone treatment for the acute respiratory distress syndrome: A multicentre, randomised controlled trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- Tavazzi, G.; Pozzi, M.; Mongodi, S.; Dammassa, V.; Romito, G.; Mojoli, F. Inhaled nitric oxide in patients admitted to intensive care unit with COVID-19 pneumonia. Crit. Care 2020, 24, 508. [Google Scholar] [CrossRef]
- Cherian, S.V.; Kumar, A.; Akasapu, K.; Ashton, R.W.; Aparnath, M.; Malhotra, A. Salvage therapies for refractory hypoxemia in ARDS. Respir Med. 2018, 141, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Ñamendys-Silva, S.A. ECMO for ARDS due to COVID-19. Heart Lung 2020, 49, 348–349. [Google Scholar] [CrossRef] [Green Version]
- Jolin, A.; Bjertnaes, L. Hypoxic pulmonary vasoconstriction in the adult respiratory distress syndrome. Acta Anaesthesiol. Scand. Suppl. 1991, 95, 40–52; discussion 53–54. [Google Scholar] [CrossRef]
- Raffin, T.A. ARDS: Mechanisms and Management. Hosp. Pract. 1987, 22, 65–80. [Google Scholar] [CrossRef]
- Zaid, Y.; Guessous, F.; Puhm, F.; Elhamdani, W.; Chentoufi, L.; Morris, A.C.; Cheikh, A.; Jalali, F.; Boilard, E.; Flamand, L. Platelet reactivity to thrombin differs between patients with COVID-19 and those with ARDS unrelated to COVID-19. Blood Adv. 2021, 5, 635–639. [Google Scholar] [CrossRef]
- Fuller, B.M.; Mohr, N.M.; Skrupky, L.; Fowler, S.; Kollef, M.H.; Carpenter, C.R. The Use of Inhaled Prostaglandins in Patients With ARDS. Chest 2015, 147, 1510–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichinose, F.; Roberts, J.D.; Zapol, W.M. Inhaled Nitric Oxide. Circulation 2004, 109, 3106–3111. [Google Scholar] [CrossRef] [PubMed]
- Rossaint, R.; Falke, K.J.; Lopez, F.; Slama, K.; Pison, U.; Zapol, W.M. Inhaled Nitric Oxide for the Adult Respiratory Distress Syndrome. N. Engl. J. Med. 1993, 328, 399–405. [Google Scholar] [CrossRef]
- Lisi, F.; Zelikin, A.N.; Chandrawati, R. Nitric Oxide to Fight Viral Infections. Adv. Sci. 2021, 8, 2003895. [Google Scholar] [CrossRef] [PubMed]
- Frostell, C.; Fratacci, M.D.; Wain, J.C.; Jones, R.; Zapol, W.M. Inhaled nitric oxide. A selective pulmonary vasodilator reversing hypoxic pulmonary vasoconstriction. Circulation 1991, 83, 2038–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, B.; Ichinose, F.; Bloch, D.B.; Zapol, W.M. Inhaled nitric oxide. Br. J. Pharmacol. 2019, 176, 246–255. [Google Scholar] [CrossRef] [Green Version]
- Ignarro, L.J. Inhaled NO and COVID-19. Br. J. Pharmacol. 2020, 177, 3848–3849. [Google Scholar] [CrossRef]
- Weinberger, B.; Laskin, D.L.; Heck, D.E.; Laskin, J.D. The Toxicology of Inhaled Nitric Oxide. Toxicol. Sci. 2001, 59, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Hamza, A.; Nasrullah, A.; Singh, R.; DiSilvio, B. Phenazopyridine-Induced Methaemoglobinaemia The Aftermath of Dysuria Treatment. Eur. J. Case Rep. Intern. Med. 2022, 9, 003191. [Google Scholar] [CrossRef]
- Wen, L.; Feil, S.; Feil, R. cGMP Signaling in Platelets. In Platelets, Haemostasis and Inflammation; Zirlik, A., Bode, C., Gawaz, M., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 231–252. [Google Scholar]
- Farkas, J. Internet Book of Critical Care, Inhaled Pulmonary Vasodilators. Available online: https://emcrit.org/ibcc/pulmvaso/#nitric_oxide (accessed on 10 September 2022).
- Saiki, Y.; Nitta, Y.; Tsuru, Y.; Tabayashi, K. Successful weaning from inhaled nitric oxide using dipyridamole. Eur. J. Cardio-Thorac. Surg. 2003, 24, 837–839. [Google Scholar] [CrossRef]
- Ruan, S.-Y.; Huang, T.-M.; Wu, H.-Y.; Wu, H.-D.; Yu, C.-J.; Lai, M.-S. Inhaled nitric oxide therapy and risk of renal dysfunction: A systematic review and meta-analysis of randomized trials. Crit. Care 2015, 19, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. INOmax. Available online: https://www.ema.europa.eu/en/documents/product-information/inomax-epar-product-information_en.pdf (accessed on 10 May 2022).
- Puybasset, L.; Rouby, J.J. Pulmonary uptake and modes of administration of inhaled nitric oxide in mechanically-ventilated patients. Crit. Care 1998, 2, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panel, C.-T.G. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 10 September 2022).
- CDC COVID-19 Response Team. Severe Outcomes among Patients with Coronavirus Disease 2019 (COVID-19), United States, 12 February–16 March 2020; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020; pp. 343–346.
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef]
- Sorensen, R.J.; Barber, R.M.; Pigott, D.M.; Carter, A.; Spencer, C.N.; Ostroff, S.M.; Reiner, R.C.; Abbafati, C.; Adolph, C.; Allorant, A.; et al. Variation in the COVID-19 infection–fatality ratio by age, time, and geography during the pre-vaccine era: A systematic analysis. Lancet 2022, 399, 1469–1488. [Google Scholar] [CrossRef]
- Wu, Z.; Wang, Q.; Zhao, J.; Yang, P.; McGoogan, J.M.; Feng, Z.; Huang, C. Time Course of a Second Outbreak of COVID-19 in Beijing, China, June–July 2020. JAMA 2020, 324, 1458. [Google Scholar] [CrossRef]
- Lentz, S.; Roginski, M.A.; Montrief, T.; Ramzy, M.; Gottlieb, M.; Long, B. Initial emergency department mechanical ventilation strategies for COVID-19 hypoxemic respiratory failure and ARDS. Am. J. Emerg. Med. 2020, 38, 2194–2202. [Google Scholar] [CrossRef]
- Navas-Blanco, J.R.; Dudaryk, R. Management of Respiratory Distress Syndrome due to COVID-19 infection. BMC Anesthesiol. 2020, 20, 177. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit. Care Med. 2020, 48, e440–e469. [Google Scholar] [CrossRef]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir. Res. 2019, 6, e000420. [Google Scholar] [CrossRef]
- Gebistorf, F.; Karam, O.; Wetterslev, J.; Afshari, A. Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) in children and adults. Cochrane Database Syst. Rev. 2016, 2018, CD002787. [Google Scholar] [CrossRef] [PubMed]
- Buckley, M.S.; Agarwal, S.K.; Garcia-Orr, R.; Saggar, R.; MacLaren, R. Comparison of Fixed-Dose Inhaled Epoprostenol and Inhaled Nitric Oxide for Acute Respiratory Distress Syndrome in Critically Ill Adults. J. Intensive Care Med. 2021, 36, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Aubron, C.; Brochard, L.; Chiche, J.-D.; Combes, A.; Dreyfuss, D.; Forel, J.-M.; Guérin, C.; Jaber, S.; Mekontso-Dessap, A.; et al. Formal guidelines: Management of acute respiratory distress syndrome. Ann. Intensive Care 2019, 9, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, E.; Mehta, S. High-frequency oscillatory ventilation and adjunctive therapies: Inhaled nitric oxide and prone positioning. Crit. Care Med. 2005, 33, S182–S187. [Google Scholar] [CrossRef] [PubMed]
- Alessandri, F.; Pugliese, F.; Ranieri, V.M. The Role of Rescue Therapies in the Treatment of Severe ARDS. Respir. Care 2018, 63, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.; Hiyoshi, A.; Montgomery, S. COVID-19 case-fatality rate and demographic and socioeconomic influencers: Worldwide spatial regression analysis based on country-level data. BMJ Open 2020, 10, e043560. [Google Scholar] [CrossRef]
- Elezkurtaj, S.; Greuel, S.; Ihlow, J.; Michaelis, E.G.; Bischoff, P.; Kunze, C.A.; Sinn, B.V.; Gerhold, M.; Hauptmann, K.; Ingold-Heppner, B.; et al. Causes of death and comorbidities in hospitalized patients with COVID-19. Sci. Rep. 2021, 11, 4263. [Google Scholar] [CrossRef]
- Kolb, M.; Dinh-Xuan, A.T.; Brochard, L. Guideline-directed management of COVID-19: Do’s and Don’ts. Eur. Respir. J. 2021, 57, 2100753. [Google Scholar] [CrossRef]
- Chen, L.; Liu, P.; Gao, H.; Sun, B.; Chao, D.; Wang, F.; Zhu, Y.; Hedenstierna, G.; Wang, C.G. Inhalation of Nitric Oxide in the Treatment of Severe Acute Respiratory Syndrome: A Rescue Trial in Beijing. Clin. Infect. Dis. 2004, 39, 1531–1535. [Google Scholar] [CrossRef] [Green Version]
- Keyaerts, E.; Vijgen, L.; Chen, L.; Maes, P.; Hedenstierna, G.; Van Ranst, M. Inhibition of SARS-coronavirus infection in vitro by S-nitroso-N-acetylpenicillamine, a nitric oxide donor compound. Int. J. Infect. Dis. 2004, 8, 223–226. [Google Scholar] [CrossRef]
- Åkerström, S.; Mousavi-Jazi, M.; Klingström, J.; Leijon, M.; Lundkvist, Å.; Mirazimi, A. Nitric Oxide Inhibits the Replication Cycle of Severe Acute Respiratory Syndrome Coronavirus. J. Virol. 2005, 79, 1966–1969. [Google Scholar] [CrossRef] [Green Version]
- Akerström, S.; Gunalan, V.; Keng, C.T.; Tan, Y.J.; Mirazimi, A. Dual effect of nitric oxide on SARS-CoV replication: Viral RNA production and palmitoylation of the S protein are affected. Virology 2009, 395, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-Arab, O.; Huette, P.; Debouvries, F.; Dupont, H.; Jounieaux, V.; Mahjoub, Y. Inhaled nitric oxide for critically ill COVID-19 patients: A prospective study. Crit. Care 2020, 24, 645. [Google Scholar] [CrossRef] [PubMed]
- Lotz, C.; Muellenbach, R.M.; Meybohm, P.; Mutlak, H.; Lepper, P.M.; Rolfes, C.B.; Peivandi, A.; Stumpner, J.; Kredel, M.; Kranke, P.; et al. Effects of inhaled nitric oxide in COVID-19–induced ARDS—Is it worthwhile? Acta Anaesthesiol. Scand. 2021, 65, 629–632. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 and Inhaled NO. Available online: https://clinicaltrials.gov/ct2/results?cond=COVID-19&term=Nitric+oxide&cntry=&state=&city=&dist= (accessed on 10 September 2022).
- Longobardo, A.; Montanari, C.; Shulman, R.; Benhalim, S.; Singer, M.; Arulkumaran, N. Inhaled nitric oxide minimally improves oxygenation in COVID-19 related acute respiratory distress syndrome. Br. J. Anaesth. 2021, 126, e44–e46. [Google Scholar] [CrossRef] [PubMed]
- Kagima, J.; Stolbrink, M.; Masheti, S.; Mbaiyani, C.; Munubi, A.; Joekes, E.; Mortimer, K.; Rylance, J.; Morton, B. Diagnostic accuracy of combined thoracic and cardiac sonography for the diagnosis of pulmonary embolism: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235940. [Google Scholar] [CrossRef]
- Safaee Fakhr, B.; Wiegand, S.B.; Pinciroli, R.; Gianni, S.; Morais, C.C.A.; Ikeda, T.; Miyazaki, Y.; Marutani, E.; Di Fenza, R.; Larson, G.M.; et al. High Concentrations of Nitric Oxide Inhalation Therapy in Pregnant Patients With Severe Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2020, 136, 1109–1113. [Google Scholar] [CrossRef]
- Baek, Y.J.; Lee, Y.-J.; Yoon, J.S.; Sohn, Y.; Cho, Y.; Kim, M.H.; Hyun, J.H.; Lee, E.H.; Lee, K.H.; Kim, J.H.; et al. Duration of culturable SARS-CoV-2 within different specimens among mild and severe COVID-19 patients: A longitudinal study. J. Infect. 2021, 83, e29–e31. [Google Scholar] [CrossRef]
- Samrah, S.M.; Al-Mistarehi, A.-H.; Kewan, T.; Al-Khatib, S.M.; Ibnian, A.M.; Samrah, R.S.; Khassawneh, B.Y. Viral Clearance Course of COVID-19 Outbreaks. J. Multidiscip. Healthc. 2021, 14, 555–565. [Google Scholar] [CrossRef]
- Winchester, S.; John, S.; Jabbar, K.; John, I. Clinical efficacy of nitric oxide nasal spray (NONS) for the treatment of mild COVID-19 infection. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Parikh, R.; Wilson, C.; Weinberg, J.; Gavin, D.; Murphy, J.; Reardon, C.C. Inhaled nitric oxide treatment in spontaneously breathing COVID-19 patients. Ther. Adv. Respir. Dis. 2020, 14, 175346662093351. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, R.A.; Berra, L.; Gladwin, M.T. Home Nitric Oxide Therapy for COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Zamanian, R.T.; Pollack, C.V.; Gentile, M.A.; Rashid, M.; Fox, J.C.; Mahaffey, K.W.; De Jesus Perez, V. Outpatient Inhaled Nitric Oxide in a Patient with Vasoreactive Idiopathic Pulmonary Arterial Hypertension and COVID-19 Infection. Am. J. Respir. Crit. Care Med. 2020, 202, 130–132. [Google Scholar] [CrossRef] [PubMed]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality: Systematic review and meta-analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef]
- Khokher, W.; Malhas, S.-E.; Beran, A.; Iftikhar, S.; Burmeister, C.; Mhanna, M.; Srour, O.; Rashid, R.; Kesireddy, N.; Assaly, R. Inhaled Pulmonary Vasodilators in COVID-19 Infection: A Systematic Review and Meta-Analysis. J. Intensive Care Med. 2022, 37, 1370–1382. [Google Scholar] [CrossRef]
- Radovancevic, B.; Vrtovec, B.; Thomas, C.D.; Croitoru, M.; Myers, T.J.; Radovancevic, R.; Khan, T.; Massin, E.K.; Frazier, O.H. Nitric oxide versus prostaglandin E1 for reduction of pulmonary hypertension in heart transplant candidates. J. Heart Lung Transplant. 2005, 24, 690–695. [Google Scholar] [CrossRef]
- Wilkens, H.; Guth, A.; König, J.; Forestier, N.; Cremers, B.; Hennen, B.; Böhm, M.; Sybrecht, G.W. Effect of inhaled iloprost plus oral sildenafil in patients with primary pulmonary hypertension. Circulation 2001, 104, 1218–1222. [Google Scholar] [CrossRef] [Green Version]
- Gessler, T.; Seeger, W.; Schmehl, T. Inhaled Prostanoids in the Therapy of Pulmonary Hypertension. J. Aerosol Med. Pulm. Drug Deliv. 2008, 21, 1–12. [Google Scholar] [CrossRef]
- Stream, A.R.; Bull, T.M. Experiences with treprostinil in the treatment of pulmonary arterial hypertension. Ther. Adv. Respir. Dis. 2012, 6, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Laliberte, K.; Arneson, C.; Jeffs, R.; Hunt, T.; Wade, M. Pharmacokinetics and steady-state bioequivalence of treprostinil sodium (Remodulin) administered by the intravenous and subcutaneous route to normal volunteers. J. Cardiovasc. Pharmacol. 2004, 44, 209–214. [Google Scholar] [CrossRef]
- Van Heerden, P.V.; Barden, A.; Michalopoulos, N.; Bulsara, M.K.; Roberts, B.L. Dose-Response to Inhaled Aerosolized Prostacyclin for Hypoxemia Due to ARDS. Chest 2000, 117, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Alt, U.; Leigh, P.J.; Wilkins, A.J.; Morris, P.K.; MacDermot, J. Desensitization of iloprost responsiveness in human platelets follows prolonged exposure to iloprost in vitro. Br. J. Clin. Pharmacol. 1986, 22, 118–119. [Google Scholar] [PubMed]
- Gessler, T. lloprost delivered via the BREELIBTM nebulizer: A review of the clinical evidence for efficacy and safety. Ther. Adv. Respir. Dis. 2019, 13, 1753466619835497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, H.; Yeoh, H.L.; Fothergill, T.; Burns, A.; Humbert, M.; Williams, T. Prostacyclin for pulmonary arterial hypertension. Cochrane Database Syst. Rev. 2019, 5, CD012785. [Google Scholar] [CrossRef]
- De Wet, C.J.; Affleck, D.G.; Jacobsohn, E.; Avidan, M.S.; Tymkew, H.; Hill, L.L.; Zanaboni, P.B.; Moazami, N.; Smith, J.R. Inhaled prostacyclin is safe, effective, and affordable in patients with pulmonary hypertension, right heart dysfunction, and refractory hypoxemia after cardiothoracic surgery. J. Thorac. Cardiovasc. Surg. 2004, 127, 1058–1067. [Google Scholar] [CrossRef] [Green Version]
- Ivy, D.D. Prostacyclin in the intensive care setting. Pediatr. Crit. Care Med. 2010, 11, S41–S45. [Google Scholar] [CrossRef] [Green Version]
- Dzierba, A.L.; Abel, E.E.; Buckley, M.S.; Lat, I. A Review of Inhaled Nitric Oxide and Aerosolized Epoprostenol in Acute Lung Injury or Acute Respiratory Distress Syndrome. Pharmacotherapy J. Hum. Pharmacol. Drug Ther. 2014, 34, 279–290. [Google Scholar] [CrossRef]
- Pritchard, J.N.; Hatley, R.H.; Denyer, J.; Hollen, D.v. Mesh nebulizers have become the first choice for new nebulized pharmaceutical drug developments. Ther. Deliv. 2018, 9, 121–136. [Google Scholar] [CrossRef] [Green Version]
- Richter, M.J.; Stollfuß, B.; Roitenberg, A.; Kleinjung, F.; Graeff , V.; Berghaus, S.; Müller, C.; Ghofrani, H.-A. Switching inhaled iloprost formulations in patients with pulmonary arterial hypertension: The VENTASWITCH Trial. Pulm. Circ. 2018, 8, 2045894018798921. [Google Scholar] [CrossRef] [Green Version]
- Haeberle, H.; Prohaska, S.; Martus, P.; Straub, A.; Zarbock, A.; Marx, G.; Zago, M.; Giera, M.; Koeppen, M.; Rosenberger, P. Therapeutic iloprost for the treatment of acute respiratory distress syndrome (ARDS) (the ThIlo trial): A prospective, randomized, multicenter phase II study. Trials 2020, 21, 242. [Google Scholar] [CrossRef]
- TYVASO. Available online: https://www.tyvaso.com/?msclkid=6a9595f96d3c14abd1b1f6cc1647fce1&utm_source=bing&utm_medium=cpc&utm_campaign=DTC%20-%20General%20-%20Branded&utm_term=tyvaso%20medication&utm_content=General%20-%20Splash (accessed on 29 September 2022).
- Parker, D.K.; Shen, S.; Zheng, J.; Ivy, D.D.; Crotwell, D.N.; Hotz, J.C.; DiBlasi, R.M. Inhaled Treprostinil Drug Delivery During Mechanical Ventilation and Spontaneous Breathing Using Two Different Nebulizers. Pediatr. Crit. Care Med. 2017, 18, e253–e260. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Lu, B. The application of low tidal volume pressure-controlled ventilation in patients with acute respiratory distress syndrome. Hunan Yi Ke Da Xue Xue Bao 1998, 23, 57–58. [Google Scholar] [PubMed]
- Gattinoni, L.; Busana, M.; Giosa, L.; Macrì, M.; Quintel, M. Prone Positioning in Acute Respiratory Distress Syndrome. Semin. Respir. Crit. Care Med. 2019, 40, 094–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhazzani, W.; Belley-Cote, E.; Møller, M.H.; Angus, D.C.; Papazian, L.; Arabi, Y.M.; Citerio, G.; Connolly, B.; Denehy, L.; Fox-Robichaud, A.; et al. Neuromuscular blockade in patients with ARDS: A rapid practice guideline. Intensive Care Med. 2020, 46, 1977–1986. [Google Scholar] [CrossRef]
- Gu, S.X.; Tyagi, T.; Jain, K.; Gu, V.W.; Lee, S.H.; Hwa, J.M.; Kwan, J.M.; Krause, D.S.; Lee, A.I.; Halene, S.; et al. Thrombocytopathy and endotheliopathy: Crucial contributors to COVID-19 thromboinflammation. Nat. Rev. Cardiol. 2021, 18, 194–209. [Google Scholar] [CrossRef]
- Ammar, M.A.; Bauer, S.R.; Bass, S.N.; Sasidhar, M.; Mullin, R.; Lam, S.W. Noninferiority of Inhaled Epoprostenol to Inhaled Nitric Oxide for the Treatment of ARDS. Ann. Pharmacother. 2015, 49, 1105–1112. [Google Scholar] [CrossRef]
- Afshari, A.; Bastholm Bille, A.; Allingstrup, M. Aerosolized prostacyclins for acute respiratory distress syndrome (ARDS). Cochrane Database Syst. Rev. 2017, 7, Cd007733. [Google Scholar] [CrossRef]
- Riva, C.M.; Morganroth, M.L.; Ljungman, A.G.; Schoeneich, S.O.; Marks, R.M.; Todd, R.F., 3rd; Ward, P.A.; Boxer, L.A. Iloprost inhibits neutrophil-induced lung injury and neutrophil adherence to endothelial monolayers. Am. J. Respir. Cell Mol. Biol. 1990, 3, 301–309. [Google Scholar] [CrossRef]
- Woyke, S.; Mair, N.; Haller, T.; Ronzani, M.; Plunser, D.; Oberacher, H.; Gatterer, H.; Rugg, C.; Ströhle, M. The impact of nebulized Epoprostenol and Iloprost on hemoglobin oxygen affinity—An ex-vivo experiment. Am. J. Physiol. Lung Cell. Mol. Physiol. 2022, 322, L898–L903. [Google Scholar] [CrossRef]
- Ford, H.J.; Anderson, W.H.; Wendlandt, B.; Bice, T.; Ceppe, A.; Lanier, J.; Carson, S.S. Randomized, Placebo-controlled Trial of Inhaled Treprostinil for Patients at Risk for Acute Respiratory Distress Syndrome. Ann. Am. Thorac. Soc. 2021, 18, 641–647. [Google Scholar] [CrossRef]
- DeGrado, J.R.; Szumita, P.M.; Schuler, B.R.; Dube, K.M.; Lenox, J.; Kim, E.Y.; Weinhouse, G.L.; Massaro, A.F. Evaluation of the Efficacy and Safety of Inhaled Epoprostenol and Inhaled Nitric Oxide for Refractory Hypoxemia in Patients With Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0259. [Google Scholar] [CrossRef] [PubMed]
- Sonti, R.; Pike, C.W.; Cobb, N. Responsiveness of Inhaled Epoprostenol in Respiratory Failure due to COVID-19. J. Intensive Care Med. 2021, 36, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Fink, J.B.; Augustynovich, A.E.; Mirza, S.; Kallet, R.H.; Dhand, R. Effects of Inhaled Epoprostenol and Prone Positioning in Intubated Coronavirus Disease 2019 Patients with Refractory Hypoxemia. Crit. Care Explor. 2020, 2, e0307. [Google Scholar] [CrossRef] [PubMed]
- Mulia, E.P.B.; Luke, K. Inhaled prostacyclin analogues in COVID-19 associated acute respiratory distress syndrome: Scientific rationale. Egypt. Heart J. 2021, 73, 82. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| COVID-ARDS | Typical ARDS | |
|---|---|---|
| Onset | Within 8 to 12 days | Within 7 days |
| Immune cells | Peripheral ground glass opacities in early disease | Patchy diffuse bilateral dependent consolidations |
| Immune cells | Monocytes, lymphocytes, and neutrophils | Predominantly neutrophilic infiltrate |
| Immuno-thrombosis | More prevalent likely due to diffuse endothelial injury from a hyperinflammatory state | Less prevalent as compared to CARDs |
| Identifier | Brief Title | Severity | Study Design | Drug | Dose | Duration | Subjects | Follow-Ups | Study Phase | Status |
|---|---|---|---|---|---|---|---|---|---|---|
| NCT04388683 | Inhaled NO for preventing progression in COVID-19 | Moderate-severe | RCT | NO gas | 125 mcg/kg (20 ppm) | 24 h | 42 | 28 | Phase 2 | Completed |
| NCT04383002 | High dose inhaled NO for COVID-19 (ICU patients) | Moderate-severe | RCT | NO gas | 160 ppm, once | 6 h | 7 | 7 | Phase 1 | Recruiting |
| NCT04305457 | NO gas inhalation therapy for mild/moderate COVID-19 | Moderate-severe | RCT | NO gas | 140–180 ppm, twice | 20–30 min | 70 | 28 | Phase 2 | Recruiting |
| NCT04456088 | Inhaled NO for treatment of COVID-19 caused by SARSCoV2 (Canada trial) | Moderate-severe | RCT | NO gas | 80 ppm, four times | 40 min | 50 | 14 | Phase 2/1 | Not yet recruiting |
| NCT04337918 | NO-releasing solutions to prevent and treat mild/moderate COVID-19 infection | Mild-moderate | RCT | NO gas | Five times | 14 days | 200 | 14 | Phase 2 | Recruiting |
| NCT04421508 | A study to assess pulsed inhaled NO vs. placebo in subjects with mild or moderate COVID-19 | Mild-moderate | RCT | NO gas | 125 mcg/kg (20 ppm) | 24 h | 500 | 28 | Phase 2 | Recruiting |
| NCT04476992 | NO therapy for COVID-19 patients with oxygen supplementation | Mild-moderate | RCT | NO gas | 200 ppm, twice | 30 min | 20 | 14 | Phase 2/1 | Not yet recruiting |
| NCT04397692 | Inhaled NO for the treatment of COVID-19 caused by SARSCov-2 (US trial) | Mild-moderate | RCT | NO gas | 80 ppm, four times | 40 min | 20 | 14 | Phase 3 | Recruiting |
| NCT04306393 | NO gas inhalation in SARS in COVID-19 | Mild | RCT | NO gas | 80 40 | 48 h | 200 | 28 | Phase 2 | Recruiting |
| NCT04312243 | NO prevention of COVID-19 for healthcare providers | Close contact | RCT | NO gas | 160 ppm, twice | 15 min | 470 | 14 | Phase 2 | Recruiting |
| NCT04601077 | The evaluation of NO generating lozenges on the outcome of newly diagnosed COVID-19 African Americans patients | Mild | RCT | NO lozenges | 30 mg, twice | 30 days | 100 | 30 | Phase 1 | Not yet recruiting |
| NCT04388683 | Inhaled NO for preventing progression in COVID-19 | Moderate-severe | RCT | NO gas | 125mcg/kg (20 ppm) | 24 h | 42 | 28 | Phase 2 | completed |
| NCT04383002 | High dose Inhaled NO for COVID-19 (ICU patients) | Moderate-severe | RCT | NO gas | 160 ppm, once | 6 h | 7 | 7 | Phase 1 | Recruiting |
| NCT04305457 | NO gas inhalation therapy for mild/moderate COVID-19 | Moderate-severe | RCT | NO gas | 140–180 ppm, twice | 20–30 min | 70 | 28 | Phase 2 | Recruiting |
| NCT04456088 | Inhaled NO for treatment of COVID-19 caused by SARSCoV2 (Canada trial) | Moderate-severe | RCT | NO gas | 80 ppm, four times | 40 min | 50 | 14 | Phase 2/1 | Not yet Recruiting |
| NCT04337918 | NO-releasing solutions to prevent and treat mild/moderate COVID-19 infection | Mild-moderate | RCT | NO gas | five times | 14 days | 200 | 14 | Phase 2 | Recruiting |
| NCT04421508 | A study to assess pulsed inhaled NO vs. Placebo in subjects with mild or moderate COVID-19 | Mild-moderate | RCT | NO gas | 125 mcg/kg (20 ppm) | 24 h | 500 | 28 | Phase 2 | Recruiting |
| NCT04476992 | NO therapy for COVID-19 patients with oxygen supplementation | Mild-moderate | RCT | NO gas | 200 ppm, twice | 30 min | 20 | 14 | Phase 2/1 | Not yet Recruiting |
| NCT04397692 | Inhaled NO for the treatment of COVID-19 caused by SARSCov-2 (US trial) | Mild-moderate | RCT | NO gas | 80 ppm, four times | 40 min | 20 | 14 | Phase 3 | Recruiting |
| NCT04306393 | NO gas inhalation in SARS in COVID-19 | mild | RCT | NO gas | 80 40 | 48 h | 200 | 28 | Phase 2 | Recruiting |
| NCT04312243 | NO prevention of COVID-19 for healthcare providers | Close contact | RCT | NO gas | 160 ppm, twice | 15 min | 470 | 14 | Phase 2 | Recruiting |
| NCT04601077 | The evaluation of NO generating lozenges on the outcome of newly diagnosed COVID-19 patients in African Americans | mild | RCT | NO lozenges | 30 mg, twice | 30 days | 100 | 30 | Phase 1 | Not yet Recruiting |
| Identifier | Brief Title | Severity | Study Design | Drug | Dose | Duration | Subjects | Follow Ups | Study Phase | Status |
|---|---|---|---|---|---|---|---|---|---|---|
| NCT04388683 | VentaProst in subjects with COVID-19 requiring ventilation | Moderate-severe | RCT; Double-blind | Inhaled epoprostenol | N/A | 10 days | 11 | 10 days | Complete | Results pending |
| NCT04383002 | Infusion of iloprost vs. placebo for 72 h in COVID-19 respiratory failure | Moderate-severe | RCT | Iloprost | 1 ng/kg | 24 h | 80 | 28 days | Complete | Results pending |
| NCT04338828 | Inhaled iloprost for suspected COVID-19 respiratory failure | Moderate-severe | RCT | Iloprost | 20 mcg | Every 8 h | 40 | 5 days | Complete | Results pending |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasrullah, A.; Virk, S.; Shah, A.; Jacobs, M.; Hamza, A.; Sheikh, A.B.; Javed, A.; Butt, M.A.; Sangli, S. Acute Respiratory Distress Syndrome and the Use of Inhaled Pulmonary Vasodilators in the COVID-19 Era: A Narrative Review. Life 2022, 12, 1766. https://doi.org/10.3390/life12111766
Nasrullah A, Virk S, Shah A, Jacobs M, Hamza A, Sheikh AB, Javed A, Butt MA, Sangli S. Acute Respiratory Distress Syndrome and the Use of Inhaled Pulmonary Vasodilators in the COVID-19 Era: A Narrative Review. Life. 2022; 12(11):1766. https://doi.org/10.3390/life12111766
Chicago/Turabian StyleNasrullah, Adeel, Shiza Virk, Aaisha Shah, Max Jacobs, Amina Hamza, Abu Baker Sheikh, Anam Javed, Muhammad Ali Butt, and Swathi Sangli. 2022. "Acute Respiratory Distress Syndrome and the Use of Inhaled Pulmonary Vasodilators in the COVID-19 Era: A Narrative Review" Life 12, no. 11: 1766. https://doi.org/10.3390/life12111766