
Rethinking Chronic Kidney Disease in the Aging Population
 , , ,
, , ,
Abstract
:1. Introduction
2. Definition and Staging of Chronic Kidney Disease in Adults
3. Epidemiology of CKD
4. Risk Factors
5. Morbidity and Mortality of the CKD
6. The Cost of CKD
7. ESKD Trend
8. Kidney Transplantation in the Elderly Population
9. Perspectives
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mehta, R.L.; Cerdá, J.; Burdmann, E.A.; Tonelli, M.; García-García, G.; Jha, V.; Susantitaphong, P.; Rocco, M.; Vanholder, R.; Sever, M.S.; et al. International Society of Nephrology’s 0by25 Initiative for Acute Kidney Injury (Zero Preventable Deaths by 2025): A Human Rights Case for Nephrology. Lancet Lond. Engl. 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Cockwell, P.; Fisher, L.-A. The Global Burden of Chronic Kidney Disease. Lancet 2020, 395, 662–664. [Google Scholar] [CrossRef] [Green Version]
- Boenink, R.; Astley, M.E.; Huijben, J.A.; Stel, V.S.; Kerschbaum, J.; Ots-Rosenberg, M.; Åsberg, A.A.; Lopot, F.; Golan, E.; Castro de la Nuez, P.; et al. The ERA Registry Annual Report 2019: Summary and Age Comparisons. Clin. Kidney J. 2022, 15, 452–472. [Google Scholar] [CrossRef] [PubMed]
- United States Renal Data System. 2021 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2021. Available online: https://adr.usrds.org/ (accessed on 14 October 2022).
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, C.; Pasternack, B.; Shah, H.; Gallo, G. Age-Related Incidence of Sclerotic Glomeruli in Human Kidneys. Am. J. Pathol. 1975, 80, 227. [Google Scholar]
- Perazella, M.A.; Rosner, M.H. Drug-Induced Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2022, 17, 1220–1233. [Google Scholar] [CrossRef]
- United Nations. Ageing. Available online: https://www.un.org/en/global-issues/ageing (accessed on 16 September 2022).
- National Kidney Foundation K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2002, 39, S1–S266.
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; Francisco, A.L.M.D.; Jong, P.E.D.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.-U. The Definition, Classification, and Prognosis of Chronic Kidney Disease: A KDIGO Controversies Conference Report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [Green Version]
- Winearls, C.G.; Glassock, R.J. Classification of Chronic Kidney Disease in the Elderly: Pitfalls and Errors. Nephron Clin. Pract. 2011, 119, c2–c4. [Google Scholar] [CrossRef]
- Brück, K.; Jager, K.J.; Dounousi, E.; Kainz, A.; Nitsch, D.; Ärnlöv, J.; Rothenbacher, D.; Browne, G.; Capuano, V.; Ferraro, P.M.; et al. Methodology Used in Studies Reporting Chronic Kidney Disease Prevalence: A Systematic Literature Review. Nephrol. Dial. Transplant. 2015, 30, iv6–iv16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rijn, M.H.C.; Alencar de Pinho, N.; Wetzels, J.F.; van den Brand, J.A.J.G.; Stengel, B. Worldwide Disparity in the Relation Between CKD Prevalence and Kidney Failure Risk. Kidney Int. Rep. 2020, 5, 2284–2291. [Google Scholar] [CrossRef] [PubMed]
- Gaspari, F.; Perico, N.; Remuzzi, G. Measurement of Glomerular Filtration Rate. Kidney Int. Suppl. 1997, 63, S151–S154. [Google Scholar]
- Randers, E.; Erlandsen, E.J. Serum Cystatin C as an Endogenous Marker of the Renal Function—A Review. Clin. Chem. Lab. Med. 1999, 37, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Noronha, I.L.; Santa-Catharina, G.P.; Andrade, L.; Coelho, V.A.; Jacob-Filho, W.; Elias, R.M. Glomerular Filtration in the Aging Population. Front. Med. 2022, 9, 769329. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Lemoine, S.; Guebre-Egziabher, F.; Sens, F.; Nguyen-Tu, M.-S.; Juillard, L.; Dubourg, L.; Hadj-Aissa, A. Accuracy of GFR Estimation in Obese Patients. Clin. J. Am. Soc. Nephrol. CJASN 2014, 9, 720–727. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Schaeffner, E.S.; Ebert, N.; Delanaye, P.; Frei, U.; Gaedeke, J.; Jakob, O.; Kuhlmann, M.K.; Schuchardt, M.; Tölle, M.; Ziebig, R.; et al. Two Novel Equations to Estimate Kidney Function in Persons Aged 70 Years or Older. Ann. Intern. Med. 2012, 157, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Nyman, U.; Grubb, A.; Larsson, A.; Hansson, L.-O.; Flodin, M.; Nordin, G.; Lindström, V.; Björk, J. The Revised Lund-Malmö GFR Estimating Equation Outperforms MDRD and CKD-EPI across GFR, Age and BMI Intervals in a Large Swedish Population. Clin. Chem. Lab. Med. 2014, 52, 815–824. [Google Scholar] [CrossRef]
- Pottel, H.; Hoste, L.; Dubourg, L.; Ebert, N.; Schaeffner, E.; Eriksen, B.O.; Melsom, T.; Lamb, E.J.; Rule, A.D.; Turner, S.T.; et al. An Estimated Glomerular Filtration Rate Equation for the Full Age Spectrum. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2016, 31, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grubb, A.; Horio, M.; Hansson, L.-O.; Björk, J.; Nyman, U.; Flodin, M.; Larsson, A.; Bökenkamp, A.; Yasuda, Y.; Blufpand, H.; et al. Generation of a New Cystatin C–Based Estimating Equation for Glomerular Filtration Rate by Use of 7 Assays Standardized to the International Calibrator. Clin. Chem. 2014, 60, 974–986. [Google Scholar] [CrossRef] [PubMed]
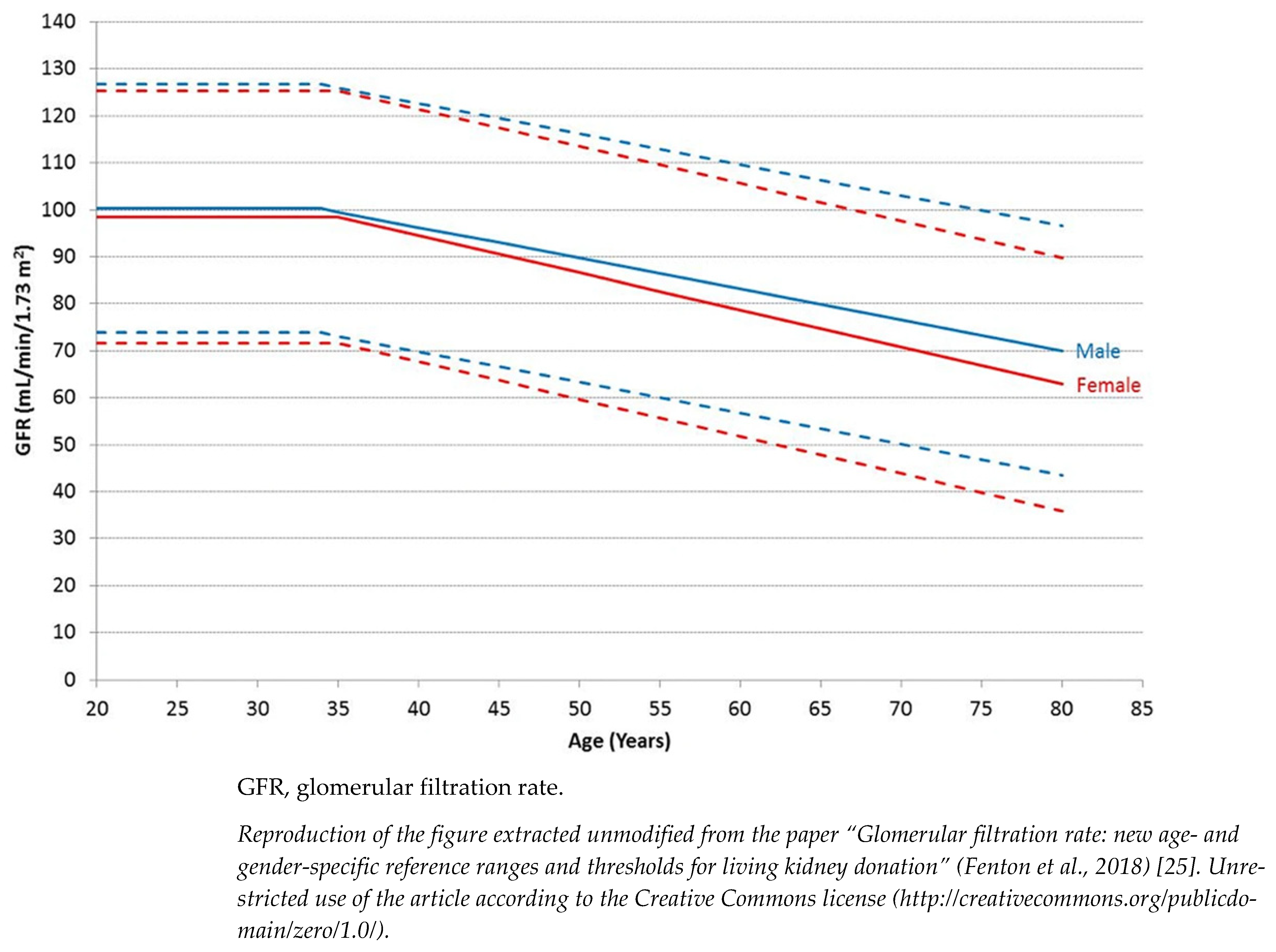
- Fenton, A.; Montgomery, E.; Nightingale, P.; Peters, A.M.; Sheerin, N.; Wroe, A.C.; Lipkin, G.W. Glomerular Filtration Rate: New Age- and Gender- Specific Reference Ranges and Thresholds for Living Kidney Donation. BMC Nephrol. 2018, 19, 336. [Google Scholar] [CrossRef] [PubMed]
- Denic, A.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes with the Aging Kidney. Adv. Chronic Kidney Dis. 2016, 23, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Hallan, S.I.; Matsushita, K.; Sang, Y.; Mahmoodi, B.K.; Black, C.; Ishani, A.; Kleefstra, N.; Naimark, D.; Roderick, P.; Tonelli, M.; et al. Age and Association of Kidney Measures with Mortality and End-Stage Renal Disease. JAMA 2012, 308, 2349–2360. [Google Scholar] [CrossRef]
- Tangri, N.; Stevens, L.A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A.S. A Predictive Model for Progression of Chronic Kidney Disease to Kidney Failure. JAMA 2011, 305, 1553–1559. [Google Scholar] [CrossRef] [Green Version]
- Shardlow, A.; McIntyre, N.J.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. Chronic Kidney Disease in Primary Care: Outcomes after Five Years in a Prospective Cohort Study. PLoS Med. 2016, 13, e1002128. [Google Scholar] [CrossRef] [Green Version]
- Delanaye, P.; Jager, K.J.; Bökenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; van der Giet, M.; Glassock, R.J.; et al. CKD: A Call for an Age-Adapted Definition. J. Am. Soc. Nephrol. JASN 2019, 30, 1785–1805. [Google Scholar] [CrossRef]
- Garg, N.; Poggio, E.D.; Mandelbrot, D. The Evaluation of Kidney Function in Living Kidney Donor Candidates. Kidney360 2021, 2, 1523–1530. [Google Scholar] [CrossRef]
- Guidelines for Living Donor Kidney Transplantation. British Transplantation Society. Www.Bts.Org.Uk. March 2018 Fourth Edition. Available online: https://Bts.Org.Uk/Wp-Content/Uploads/2018/07/FINAL_LDKT-Guidelines_June-2018.Pdf (accessed on 18 September 2022).
- Glassock, R.J.; Warnock, D.G.; Delanaye, P. The Global Burden of Chronic Kidney Disease: Estimates, Variability and Pitfalls. Nat. Rev. Nephrol. 2017, 13, 104–114. [Google Scholar] [CrossRef]
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.D.; Chen, C.-S.; Kelly, T.N.; Chen, J.; He, J. A Systematic Analysis of Worldwide Population-Based Data on the Global Burden of Chronic Kidney Disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brück, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Völzke, H.; Ärnlöv, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. JASN 2016, 27, 2135–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, H.H.; Perneger, T.V.; Klag, M.J.; Whelton, P.K.; Coresh, J. Familial Aggregation of Renal Disease in a Population-Based Case-Control Study. J. Am. Soc. Nephrol. 1998, 9, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Gumprecht, J.; Zychma, M.J.; Moczulski, D.K.; Gosek, K.; Grzeszczak, W. Family History of End-Stage Renal Disease among Hemodialyzed Patients in Poland. J. Nephrol. 2003, 16, 511–515. [Google Scholar] [PubMed]
- Satko, S.G.; Freedman, B.I.; Moossavi, S. Genetic Factors in End-Stage Renal Disease. Kidney Int. 2005, 67, S46–S49. [Google Scholar] [CrossRef] [Green Version]
- Prasad, N.; Patel, M.R. Infection-Induced Kidney Diseases. Front. Med. 2018, 5, 327. [Google Scholar] [CrossRef] [Green Version]
- Kuźma, Ł.; Małyszko, J.; Bachórzewska-Gajewska, H.; Kralisz, P.; Dobrzycki, S. Exposure to Air Pollution and Renal Function. Sci. Rep. 2021, 11, 11419. [Google Scholar] [CrossRef]
- Asghari, G.; Farhadnejad, H.; Mirmiran, P.; Dizavi, A.; Yuzbashian, E.; Azizi, F. Adherence to the Mediterranean Diet Is Associated with Reduced Risk of Incident Chronic Kidney Diseases among Tehranian Adults. Hypertens. Res. 2017, 40, 96–102. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Steffen, L.M.; Palmas, W.; Burke, G.L.; Jacobs, D.R. Associations between Microalbuminuria and Animal Foods, Plant Foods, and Dietary Patterns in the Multiethnic Study of Atherosclerosis. Am. J. Clin. Nutr. 2008, 87, 1825–1836. [Google Scholar] [CrossRef] [Green Version]
- De Nicola, L.; Donfrancesco, C.; Minutolo, R.; Lo Noce, C.; Palmieri, L.; De Curtis, A.; Iacoviello, L.; Zoccali, C.; Gesualdo, L.; Conte, G.; et al. Prevalence and Cardiovascular Risk Profile of Chronic Kidney Disease in Italy: Results of the 2008-12 National Health Examination Survey. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2015, 30, 806–814. [Google Scholar] [CrossRef]
- Nzerue, C.M.; Demissochew, H.; Tucker, J.K. Race and Kidney Disease: Role of Social and Environmental Factors. J. Natl. Med. Assoc. 2002, 94, 28S–38S. [Google Scholar]
- Iseki, K. Factors Influencing the Development of End-Stage Renal Disease. Clin. Exp. Nephrol. 2005, 9, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Song, E.-Y.; McClellan, W.M.; McClellan, A.; Gadi, R.; Hadley, A.C.; Krisher, J.; Clay, M.; Freedman, B.I. Effect of Community Characteristics on Familial Clustering of End-Stage Renal Disease. Am. J. Nephrol. 2009, 30, 499–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lackland, D.T.; Egan, B.M.; Fan, Z.J.; Syddall, H.E. Low Birth Weight Contributes to the Excess Prevalence of End-Stage Renal Disease in African Americans. J. Clin. Hypertens. Greenwich Conn. 2001, 3, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Brewster, U.C.; Perazella, M.A. A Review of Chronic Lead Intoxication: An Unrecognized Cause of Chronic Kidney Disease. Am. J. Med. Sci. 2004, 327, 341–347. [Google Scholar] [CrossRef]
- Sun, X.; Wang, Y.; Jiang, T.; Yuan, X.; Ren, Z.; Tuffour, A.; Liu, H.; Zhou, Y.; Gu, J.; Shi, H. Nephrotoxicity Profile of Cadmium Revealed by Proteomics in Mouse Kidney. Biol. Trace Elem. Res. 2021, 199, 1929–1940. [Google Scholar] [CrossRef]
- Lea, J.P.; Nicholas, S.B. Diabetes Mellitus and Hypertension: Key Risk Factors for Kidney Disease. J. Natl. Med. Assoc. 2002, 94, 7S–15S. [Google Scholar]
- Alfano, G.; Guaraldi, G.; Fontana, F.; Bellasi, A.; Cappelli, G. Therapeutic Management of HIV-Infected Patients with Chronic Kidney Disease. J. Nephrol. 2020, 33, 699–713. [Google Scholar] [CrossRef]
- Moody, E.C.; Coca, S.G.; Sanders, A.P. Toxic Metals and Chronic Kidney Disease: A Systematic Review of Recent Literature. Curr. Environ. Health Rep. 2018, 5, 453–463. [Google Scholar] [CrossRef]
- Mallappallil, M.; Friedman, E.A.; Delano, B.G.; McFarlane, S.I.; Salifu, M.O. Chronic Kidney Disease in the Elderly: Evaluation and Management. Clin. Pract. Lond. Engl. 2014, 11, 525–535. [Google Scholar] [CrossRef] [Green Version]
- Bellary, S.; Kyrou, I.; Brown, J.E.; Bailey, C.J. Type 2 Diabetes Mellitus in Older Adults: Clinical Considerations and Management. Nat. Rev. Endocrinol. 2021, 17, 534–548. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J.; et al. Heart Disease and Stroke Statistics—2015 Update: A Report From the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyama, T.; Kitagawa, K.; Oshima, M.; Kitajima, S.; Hara, A.; Iwata, Y.; Sakai, N.; Shimizu, M.; Hashiba, A.; Furuichi, K.; et al. Age Differences in the Relationships between Risk Factors and Loss of Kidney Function: A General Population Cohort Study. BMC Nephrol. 2020, 21, 477. [Google Scholar] [CrossRef]
- Rucci, P.; Mandreoli, M.; Gibertoni, D.; Zuccalà, A.; Fantini, M.P.; Lenzi, J.; Santoro, A.; Scarpioni, R.; De Amicis, S.; Buzio, C.; et al. A Clinical Stratification Tool for Chronic Kidney Disease Progression Rate Based on Classification Tree Analysis. Nephrol. Dial. Transplant. 2014, 29, 603–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schanstra, J.P.; Zürbig, P.; Alkhalaf, A.; Argiles, A.; Bakker, S.J.L.; Beige, J.; Bilo, H.J.G.; Chatzikyrkou, C.; Dakna, M.; Dawson, J.; et al. Diagnosis and Prediction of CKD Progression by Assessment of Urinary Peptides. J. Am. Soc. Nephrol. JASN 2015, 26, 1999–2010. [Google Scholar] [CrossRef] [Green Version]
- Moranne, O.; Froissart, M.; Rossert, J.; Gauci, C.; Boffa, J.-J.; Haymann, J.P.; M’rad, M.B.; Jacquot, C.; Houillier, P.; Stengel, B.; et al. Timing of Onset of CKD-Related Metabolic Complications. J. Am. Soc. Nephrol. 2009, 20, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirazian, S.; Radhakrishnan, J. Gastrointestinal Disorders and Renal Failure: Exploring the Connection. Nat. Rev. Nephrol. 2010, 6, 480–492. [Google Scholar] [CrossRef]
- Arnold, R.; Issar, T.; Krishnan, A.V.; Pussell, B.A. Neurological Complications in Chronic Kidney Disease. JRSM Cardiovasc. Dis. 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Alani, H.; Tamimi, A.; Tamimi, N. Cardiovascular Co-Morbidity in Chronic Kidney Disease: Current Knowledge and Future Research Needs. World J. Nephrol. 2014, 3, 156–168. [Google Scholar] [CrossRef]
- Cianciolo, G.; Donati, G.; La Manna, G.; Ferri, A.; Cuna, V.; Ubaldi, G.; Corsini, S.; Lanci, N.; Colì, L.; Stefoni, S. The Cardiovascular Burden of End-Stage Renal Disease Patients. Minerva Urol. Nefrol. 2010, 62, 51–65. [Google Scholar]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical Epidemiology of Cardiovascular Disease in Chronic Renal Disease. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 1998, 32, S112–S119. [Google Scholar] [CrossRef]
- Corsonello, A.; Freiberger, E.; Lattanzio, F. The Screening for Chronic Kidney Disease among Older People across Europe (SCOPE) Project: Findings from Cross-Sectional Analysis. BMC Geriatr. 2020, 20, 316. [Google Scholar] [CrossRef] [PubMed]
- Schrauben, S.J.; Chen, H.-Y.; Lin, E.; Jepson, C.; Yang, W.; Scialla, J.J.; Fischer, M.J.; Lash, J.P.; Fink, J.C.; Hamm, L.L.; et al. Hospitalizations among Adults with Chronic Kidney Disease in the United States: A Cohort Study. PLoS Med. 2020, 17, e1003470. [Google Scholar] [CrossRef] [PubMed]
- United States Renal Data System. 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2018; V1 CH3 Morbidity & Mortality. Available online: https://www.usrds.org/2018/view/v1_03.aspx (accessed on 30 October 2018).
- Kurella, M.; Covinsky, K.E.; Collins, A.J.; Chertow, G.M. Octogenarians and Nonagenarians Starting Dialysis in the United States. Ann. Intern. Med. 2007, 146, 177–183. [Google Scholar] [CrossRef]
- Manns, B.; Hemmelgarn, B.; Tonelli, M.; Au, F.; So, H.; Weaver, R.; Quinn, A.E.; Klarenbach, S. The Cost of Care for People With Chronic Kidney Disease. Can. J. Kidney Health Dis. 2019, 6, 2054358119835521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saran, R.; Robinson, B.; Abbott, K.C.; Bragg-Gresham, J.; Chen, X.; Gipson, D.; Gu, H.; Hirth, R.A.; Hutton, D.; Jin, Y.; et al. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2020, 75, A6–A7. [Google Scholar] [CrossRef]
- Cicchetti, A.; Ruggeri, M.; Codella, P.; Ridolfi, A. I costi socio-sanitari dell’insufficienza renale cronica. Farm. E Percorsi Ter. 2011, 12, 21–28. [Google Scholar]
- Turchetti, G.; Bellelli, S.; Amato, M.; Bianchi, S.; Conti, P.; Cupisti, A.; Panichi, V.; Rosati, A.; Pizzarelli, F.; On Behalf of the Tuscany CKD Study Group. The Social Cost of Chronic Kidney Disease in Italy. Eur. J. Health Econ. HEPAC Health Econ. Prev. Care 2017, 18, 847–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ERA-EDTA Registry: ERA-EDTA Registry Annual Report 2017; Amsterdam UMC, Location AMC, Department of Medical Informatics: Amsterdam, The Netherlands, 2019.
- Dare, A.J.; Fu, S.H.; Patra, J.; Rodriguez, P.S.; Thakur, J.S.; Jha, P.; Million Death Study Collaborators. Renal Failure Deaths and Their Risk Factors in India 2001-13: Nationally Representative Estimates from the Million Death Study. Lancet Glob. Health 2017, 5, e89–e95. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.-C.; Huang, H.-M.; Sun, L.; Tan, C.-M.; Gao, M.; Liu, H.; Tang, R.-N.; Wang, Y.-L.; Wang, B.; Ma, K.-L.; et al. Epidemiological Study of RRT-Treated ESRD in Nanjing—A Ten-Year Experience in Nearly Three Million Insurance Covered Population. PLoS ONE 2016, 11, e0149038. [Google Scholar] [CrossRef]
- ERA-EDTA Registry: ERA-EDTA Registry Annual Report 2016; Amsterdam UMC, Location AMC, Department of Medical Informatics: Amsterdam, The Netherlands, 2018.
- Lønning, K.; Midtvedt, K.; Leivestad, T.; Reisæter, A.V.; Line, P.-D.; Hartmann, A.; Heldal, K. Are Octogenarians With End-Stage Renal Disease Candidates for Renal Transplantation? Transplantation 2016, 100, 2705–2709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knoll, G.A. Kidney Transplantation in the Older Adult. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2013, 61, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crespo, M.; Mazuecos, A.; Domínguez-Gil, B. Global Perspective on Kidney Transplantation: Spain. Kidney360 2021, 2, 1840–1843. [Google Scholar] [CrossRef]
- Arcos, E.; Pérez-Sáez, M.J.; Comas, J.; Lloveras, J.; Tort, J.; Pascual, J.; Catalan Renal Registry. Assessing the Limits in Kidney Transplantation: Use of Extremely Elderly Donors and Outcomes in Elderly Recipients. Transplantation 2020, 104, 176–183. [Google Scholar] [CrossRef]
- Ojo, A.O.; Hanson, J.A.; Meier-Kriesche, H.-U.; Okechukwu, C.N.; Wolfe, R.A.; Leichtman, A.B.; Agodoa, L.Y.; Kaplan, B.; Port, F.K. Survival in Recipients of Marginal Cadaveric Donor Kidneys Compared with Other Recipients and Wait-Listed Transplant Candidates. J. Am. Soc. Nephrol. JASN 2001, 12, 589–597. [Google Scholar] [CrossRef]
- Berger, J.C.; Muzaale, A.D.; James, N.; Hoque, M.; Wang, J.M.G.; Montgomery, R.A.; Massie, A.B.; Hall, E.C.; Segev, D.L. Living Kidney Donors Ages 70 and Older: Recipient and Donor Outcomes. Clin. J. Am. Soc. Nephrol. CJASN 2011, 6, 2887–2893. [Google Scholar] [CrossRef] [Green Version]
- Yishak, A.A.; Rubenstein, K.; Clark, E.D.; Bhatia, M.; Vupputuri, S. Early Referral, Living Donation, and Preemptive Kidney Transplant. Transplant. Proc. 2022, 54, 615–621. [Google Scholar] [CrossRef]
- Levey, A.S.; Atkins, R.; Coresh, J.; Cohen, E.P.; Collins, A.J.; Eckardt, K.-U.; Nahas, M.E.; Jaber, B.L.; Jadoul, M.; Levin, A.; et al. Chronic Kidney Disease as a Global Public Health Problem: Approaches and Initiatives—A Position Statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007, 72, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Alfano, G.; Delrio, A.; Fontana, F.; Mori, G.; Cazzato, S.; Ferrari, A.; Perrone, R.; Giovanella, S.; Ligabue, G.; Magistroni, R.; et al. Clinical Presentation, Renal Histopathological Findings, and Outcome in Patients with Monoclonal Gammopathy and Kidney Disease. Int. J. Nephrol. 2021, 2021, 8859340. [Google Scholar] [CrossRef]
- Bomback, A.S.; Herlitz, L.C.; Markowitz, G.S. Renal Biopsy in the Elderly and Very Elderly: Useful or Not? Adv. Chronic Kidney Dis. 2012, 19, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Hogan, J.J.; Mocanu, M.; Berns, J.S. The Native Kidney Biopsy: Update and Evidence for Best Practice. Clin. J. Am. Soc. Nephrol. 2016, 11, 354–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bomback, A.S.; Appel, G.B.; Radhakrishnan, J.; Shirazian, S.; Herlitz, L.C.; Stokes, B.; D’Agati, V.D.; Markowitz, G.S. ANCA-Associated Glomerulonephritis in the Very Elderly. Kidney Int. 2011, 79, 757–764. [Google Scholar] [CrossRef] [Green Version]
- Corapi, K.M.; Chen, J.L.T.; Balk, E.M.; Gordon, C.E. Bleeding Complications of Native Kidney Biopsy: A Systematic Review and Meta-Analysis. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2012, 60, 62–73. [Google Scholar] [CrossRef] [Green Version]
- Kohli, H.S.; Jairam, A.; Bhat, A.; Sud, K.; Jha, V.; Gupta, K.L.; Sakhuja, V. Safety of Kidney Biopsy in Elderly: A Prospective Study. Int. Urol. Nephrol. 2006, 38, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S.; et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef] [Green Version]
- de Zeeuw, D. Albuminuria, Not Only a Cardiovascular/Renal Risk Marker, but Also a Target for Treatment? Kidney Int. Suppl. 2004, 66, S2–S6. [Google Scholar] [CrossRef]
- Turgut, F.; Balogun, R.A.; Abdel-Rahman, E.M. Renin-Angiotensin-Aldosterone System Blockade Effects on the Kidney in the Elderly: Benefits and Limitations. Clin. J. Am. Soc. Nephrol. 2010, 5, 1330–1339. [Google Scholar] [CrossRef] [Green Version]
- Georgianos, P.I.; Agarwal, R. Mineralocorticoid Receptor Antagonism in Chronic Kidney Disease. Kidney Int. Rep. 2021, 6, 2281–2291. [Google Scholar] [CrossRef]
- Wu, Y.; Yang, H.; Xu, S.; Cheng, M.; Gu, J.; Zhang, W.; Liu, S.; Zhang, M. AIM2 Inflammasome Contributes to Aldosterone-Induced Renal Injury via Endoplasmic Reticulum Stress. Clin. Sci. Lond. Engl. 1979 2022, 136, 103–120. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef] [PubMed]
- Mizobuchi, M.; Towler, D.; Slatopolsky, E. Vascular Calcification: The Killer of Patients with Chronic Kidney Disease. J. Am. Soc. Nephrol. JASN 2009, 20, 1453–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cianciolo, G.; La Manna, G.; Della Bella, E.; Cappuccilli, M.L.; Angelini, M.L.; Dormi, A.; Capelli, I.; Laterza, C.; Costa, R.; Alviano, F.; et al. Effect of Vitamin D Receptor Activator Therapy on Vitamin D Receptor and Osteocalcin Expression in Circulating Endothelial Progenitor Cells of Hemodialysis Patients. Blood Purif. 2013, 35, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B.; et al. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- Provenzano, M.; Puchades, M.J.; Garofalo, C.; Jongs, N.; D’Marco, L.; Andreucci, M.; De Nicola, L.; Gorriz, J.L.; Heerspink, H.J.L.; ROTATE-3 study group; et al. Albuminuria-Lowering Effect of Dapagliflozin, Eplerenone, and Their Combination in Patients with Chronic Kidney Disease: A Randomized Crossover Clinical Trial. J. Am. Soc. Nephrol. JASN 2022, 33, 1569–1580. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Anderson, S.; Eldadah, B.; Halter, J.B.; Hazzard, W.R.; Himmelfarb, J.; Horne, F.M.; Kimmel, P.L.; Molitoris, B.A.; Murthy, M.; O’Hare, A.M.; et al. Acute Kidney Injury in Older Adults. J. Am. Soc. Nephrol. 2011, 22, 28–38. [Google Scholar] [CrossRef] [Green Version]
- Iino, Y.; Hayashi, M.; Kawamura, T.; Shiigai, T.; Tomino, Y.; Yamada, K.; Kitajima, T.; Ideura, T.; Koyama, A.; Sugisaki, T.; et al. Renoprotective Effect of Losartan in Comparison to Amlodipine in Patients with Chronic Kidney Disease and Hypertension—A Report of the Japanese Losartan Therapy Intended for the Global Renal Protection in Hypertensive Patients (JLIGHT) Study. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2004, 27, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Bakris, G.L.; Ruilope, L.; Locatelli, F.; Ptaszynska, A.; Pieske, B.; de Champlain, J.; Weber, M.A.; Raz, I. Treatment of Microalbuminuria in Hypertensive Subjects with Elevated Cardiovascular Risk: Results of the IMPROVE Trial. Kidney Int. 2007, 72, 879–885. [Google Scholar] [CrossRef] [Green Version]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertens. Dallas Tex. 1979 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- Hemmingsen, B.; Lund, S.S.; Gluud, C.; Vaag, A.; Almdal, T.; Hemmingsen, C.; Wetterslev, J. Intensive Glycaemic Control for Patients with Type 2 Diabetes: Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomised Clinical Trials. BMJ 2011, 343, d6898. [Google Scholar] [CrossRef] [Green Version]
- Reaven, P.D.; Emanuele, N.V.; Wiitala, W.L.; Bahn, G.D.; Reda, D.J.; McCarren, M.; Duckworth, W.C.; Hayward, R.A. Intensive Glucose Control in Patients with Type 2 Diabetes—15-Year Follow-Up. N. Engl. J. Med. 2019, 380, 2215–2224. [Google Scholar] [CrossRef]
- Cianciaruso, B.; Pota, A.; Pisani, A.; Torraca, S.; Annecchini, R.; Lombardi, P.; Capuano, A.; Nazzaro, P.; Bellizzi, V.; Sabbatini, M. Metabolic Effects of Two Low Protein Diets in Chronic Kidney Disease Stage 4-5—A Randomized Controlled Trial. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2008, 23, 636–644. [Google Scholar] [CrossRef] [Green Version]
- NLA Recommendations & Statements|National Lipid Association Online. Available online: https://www.lipid.org/practicetools/documents (accessed on 16 September 2022).
- Authors/Task Force Members; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fellström, B.C.; Jardine, A.G.; Schmieder, R.E.; Holdaas, H.; Bannister, K.; Beutler, J.; Chae, D.-W.; Chevaile, A.; Cobbe, S.M.; Grönhagen-Riska, C.; et al. Rosuvastatin and Cardiovascular Events in Patients Undergoing Hemodialysis. N. Engl. J. Med. 2009, 360, 1395–1407. [Google Scholar] [CrossRef]
- De Brito-Ashurst, I.; Varagunam, M.; Raftery, M.J.; Yaqoob, M.M. Bicarbonate Supplementation Slows Progression of CKD and Improves Nutritional Status. J. Am. Soc. Nephrol. 2009, 20, 2075–2084. [Google Scholar] [CrossRef] [Green Version]
- Ruoff, G.; Edwards, N.L. Overview of Serum Uric Acid Treatment Targets in Gout: Why Less Than 6 Mg/DL? Postgrad. Med. 2016, 128, 706–715. [Google Scholar] [CrossRef] [Green Version]
- Hassan, W.; Shrestha, P.; Sumida, K.; Thomas, F.; Sweeney, P.L.; Potukuchi, P.K.; Rhee, C.M.; Streja, E.; Kalantar-Zadeh, K.; Kovesdy, C.P. Association of Uric Acid–Lowering Therapy With Incident Chronic Kidney Disease. JAMA Netw. Open 2022, 5, e2215878. [Google Scholar] [CrossRef]
- Kang, D.-H.; Nakagawa, T.; Feng, L.; Watanabe, S.; Han, L.; Mazzali, M.; Truong, L.; Harris, R.; Johnson, R.J. A Role for Uric Acid in the Progression of Renal Disease. J. Am. Soc. Nephrol. JASN 2002, 13, 2888–2897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaneda, C.; Gordon, P.L.; Uhlin, K.L.; Levey, A.S.; Kehayias, J.J.; Dwyer, J.T.; Fielding, R.A.; Roubenoff, R.; Singh, M.F. Resistance Training to Counteract the Catabolism of a Low-Protein Diet in Patients with Chronic Renal Insufficiency. A Randomized, Controlled Trial. Ann. Intern. Med. 2001, 135, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Toyama, K.; Sugiyama, S.; Oka, H.; Sumida, H.; Ogawa, H. Exercise Therapy Correlates with Improving Renal Function through Modifying Lipid Metabolism in Patients with Cardiovascular Disease and Chronic Kidney Disease. J. Cardiol. 2010, 56, 142–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, A.R.; Grams, M.E.; Navaneethan, S.D. Bariatric Surgery and Kidney-Related Outcomes. Kidney Int. Rep. 2017, 2, 261–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolignano, D.; Zoccali, C. Effects of Weight Loss on Renal Function in Obese CKD Patients: A Systematic Review. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2013, 28 (Suppl. 4), iv82–iv98. [Google Scholar] [CrossRef] [Green Version]
- McMahon, E.J.; Bauer, J.D.; Hawley, C.M.; Isbel, N.M.; Stowasser, M.; Johnson, D.W.; Campbell, K.L. A Randomized Trial of Dietary Sodium Restriction in CKD. J. Am. Soc. Nephrol. JASN 2013, 24, 2096–2103. [Google Scholar] [CrossRef] [Green Version]
- Garofalo, C.; Borrelli, S.; Provenzano, M.; De Stefano, T.; Vita, C.; Chiodini, P.; Minutolo, R.; De Nicola, L.; Conte, G. Dietary Salt Restriction in Chronic Kidney Disease: A Meta-Analysis of Randomized Clinical Trials. Nutrients 2018, 10, 732. [Google Scholar] [CrossRef]
- Lee, S.; Kang, S.; Joo, Y.S.; Lee, C.; Nam, K.H.; Yun, H.-R.; Park, J.T.; Chang, T.I.; Yoo, T.-H.; Kim, S.W.; et al. Smoking, Smoking Cessation, and Progression of Chronic Kidney Disease: Results From KNOW-CKD Study. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2021, 23, 92–98. [Google Scholar] [CrossRef]
- Lonnemann, G.; Duttlinger, J.; Hohmann, D.; Hickstein, L.; Reichel, H. Timely Referral to Outpatient Nephrology Care Slows Progression and Reduces Treatment Costs of Chronic Kidney Diseases. Kidney Int. Rep. 2016, 2, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Chandna, S.M.; Da Silva-Gane, M.; Marshall, C.; Warwicker, P.; Greenwood, R.N.; Farrington, K. Survival of Elderly Patients with Stage 5 CKD: Comparison of Conservative Management and Renal Replacement Therapy. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2011, 26, 1608–1614. [Google Scholar] [CrossRef] [Green Version]
- Carson, R.C.; Juszczak, M.; Davenport, A.; Burns, A. Is Maximum Conservative Management an Equivalent Treatment Option to Dialysis for Elderly Patients with Significant Comorbid Disease? Clin. J. Am. Soc. Nephrol. CJASN 2009, 4, 1611–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, S.P.Y.; Kreuter, W.; O’Hare, A.M. Treatment Intensity at the End of Life in Older Adults Receiving Long-Term Dialysis. Arch. Intern. Med. 2012, 172, 661–663, discussion 663-664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forzley, B.; Er, L.; Chiu, H.H.L.; Djurdjev, O.; Martinusen, D.; Carson, R.C.; Hargrove, G.; Levin, A.; Karim, M. External Validation and Clinical Utility of a Prediction Model for 6-Month Mortality in Patients Undergoing Hemodialysis for End-Stage Kidney Disease. Palliat. Med. 2018, 32, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Verberne, W.R.; Geers, A.B.M.T.; Jellema, W.T.; Vincent, H.H.; van Delden, J.J.M.; Bos, W.J.W. Comparative Survival among Older Adults with Advanced Kidney Disease Managed Conservatively Versus with Dialysis. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 633–640. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Therapeutic Intervention | KDIGO Recommendation | Results of Randomized Controlled Trial/Scientific Evidence |
|---|---|---|
| Slowing down the progression of CKD | No specific recommendations on the inhibition of the renin-angiotensin-aldosterone system | Inhibition of renin-angiotensin-aldosterone system [105,106] SGLT-2 inhibitor [103] Finerenone [69] |
| Diabetic patient with CKD | Inhibition of the renin-angiotensin-aldosterone system | Inhibition of renin-angiotensin-aldosterone system [66] SGLT-2 [100,101] |
| High blood pressure without microalbuminuria | Goal: ≤140/90 mmHg | <130/80 mmHg [107,108] |
| Diabetes | Glycated hemoglobin ≤7.0% (53 mmol/mol) | No benefit of intensive control of glycated hemoglobin [109,110] |
| Dietary intake of protein | 0.8 g/kg/die in patients with diabetes or GFR <30 mL/min/1.73 m2 | Low protein diet leads to better metabolic control [111] |
| Dyslipidemia | Statin or statin/ezetimibe: -in adults aged > 50 years with CKD regardless of cholesterol levels -in adults aged < 50 years only if they have had CV events, have diabetes or have a CV risk of more than 10% at 10 years. Statin is not recommended in dialysis patients; if already in therapy at the time of dialysis start, continue the current therapy | Lower LDL by >50% in those <75 years and a high or moderate intensity statin in those over age 75 [112] LDL-cholesterol <70 mg/dL in patients at high CV risk and <55 mg/dL in patients at very high CV risk [113]; no benefit in dialysis patients [114] |
| Acid-base balance | Serum bicarbonate ≥22 mEq/L | Bicarbonate supplementation (serum value ≥23 mEq/L) slows the rate of progression of CKD and improves nutritional status [115] |
| Hyperuricemia | No recommendations | Reduce uric acid below the saturation point (<6 mg/dL) [116] Possible implication of hyperuricemia on progression of CKD [117,118]. |
| Physical activity | Allowed (30 min 5 times a week) | Slight improvement in GFR [119,120] |
| BMI | Goal: BMI 20 to 25 | Weight loss can reduce glomerular hyperfiltration proteinuria and albuminuria [121,122] |
| Dietary salt intake | Na <90 mmol/daily (<2 g/daily) NaCl < 5 g/daily | Sodium restriction (goal 60–80 mmol/day)reduce cardiovascular risk for CKD progression [123] and proteinuria [124] |
| Smoking | Avoiding | Smoking is associated with CKD progression [125] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfano, G.; Perrone, R.; Fontana, F.; Ligabue, G.; Giovanella, S.; Ferrari, A.; Gregorini, M.; Cappelli, G.; Magistroni, R.; Donati, G. Rethinking Chronic Kidney Disease in the Aging Population. Life 2022, 12, 1724. https://doi.org/10.3390/life12111724
Alfano G, Perrone R, Fontana F, Ligabue G, Giovanella S, Ferrari A, Gregorini M, Cappelli G, Magistroni R, Donati G. Rethinking Chronic Kidney Disease in the Aging Population. Life. 2022; 12(11):1724. https://doi.org/10.3390/life12111724
Chicago/Turabian StyleAlfano, Gaetano, Rossella Perrone, Francesco Fontana, Giulia Ligabue, Silvia Giovanella, Annachiara Ferrari, Mariacristina Gregorini, Gianni Cappelli, Riccardo Magistroni, and Gabriele Donati. 2022. "Rethinking Chronic Kidney Disease in the Aging Population" Life 12, no. 11: 1724. https://doi.org/10.3390/life12111724