
Ocular Surface Changes Associated with Face Masks in Healthcare Personnel during COVID-19 Pandemic
 , ,
, ,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Questionnaire
2.3. Clinical Examination
2.4. Evaluation Method
2.5. Statistical Analysis
3. Results
3.1. Clinical Parameters
3.2. DED Diagnosis
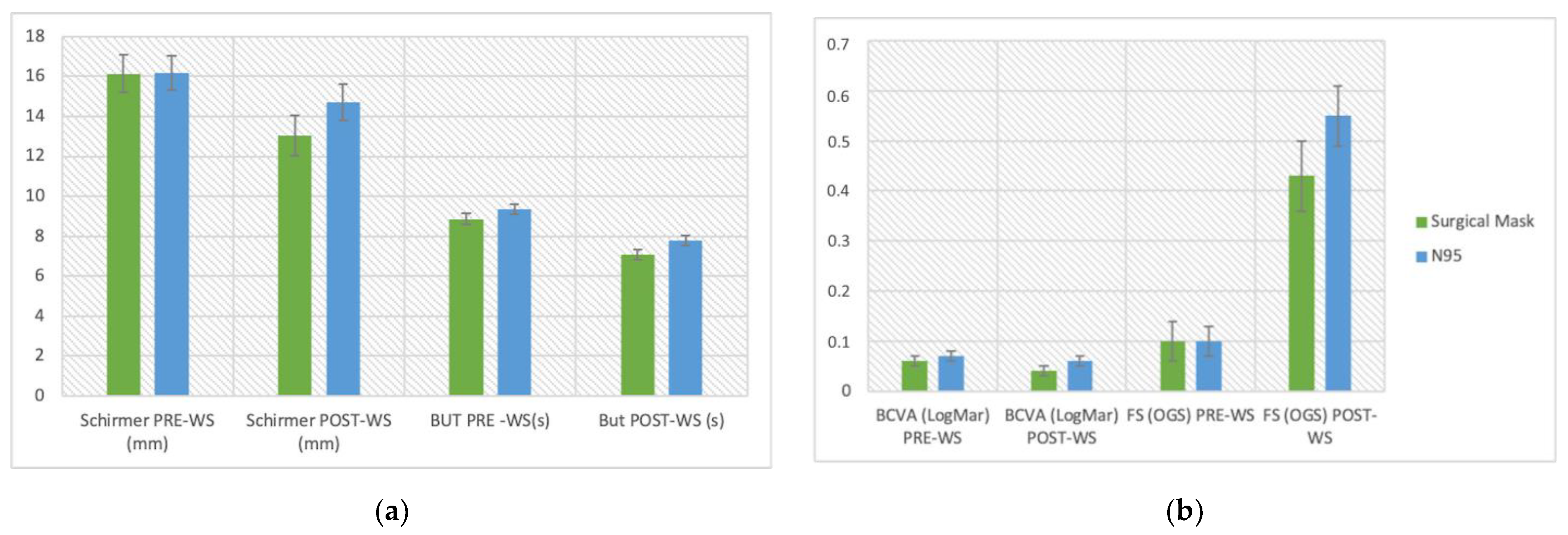
3.3. Type of Mask


{kind=link}
{kind=link}
| Variations in Clinical Parameters | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Schirmer (mm) | BUT (s) | BCVA (LogMar) | FS (OGS) | |||||||||||||
| FACE MASK TYPE | PRE-WS | SE | POST-WS | SE | PRE-WS | SE | POST-WS | SE | PRE-WS | SE | POST-WS | SE | PRE-WS | SE | POST-WS | SE |
| Surgical Mask | 16.14 | 0.94 | 13.05 | 1.02 | 8.86 | 0.28 | 7.06 | 0.25 | 0.06 | 0.01 | 0.07 | 0.01 | 0.1 | 0.04 | 0.43 | 0.07 |
| N95 | 16.18 | 0.85 | 14.70 | 0.92 | 9.34 | 0.26 | 7.78 | 0.24 | 0.04 | 0.01 | 0.06 | 0.01 | 0.1 | 0.03 | 0.55 | 0.06 |
3.4. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Torbati, E.; Krause, K.L.; Ussher, J.E. The immune response to SARS-CoV-2 and variants of concern. Viruses 2021, 13, 1911. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, P.B.; Aggarwal, R.; Jani, I.; Jawad, J.; Kochhar, S.; MacDonald, N.; Madhi, S.A.; Mohsni, E.; Mulholland, K.; Neuzil, K.M.; et al. COVID-19 vaccine strategies must focus on severe disease and global equity. Lancet 2022, 399, 406–410. [Google Scholar] [CrossRef]
- Napoli, P.E.; Nioi, M.; Fossarello, M. The “quarantine dry eye”: The lockdown for coronavirus disease 2019 and its implications for ocular surface health. Risk Manag. Healthc. Policy 2021, 14, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.K.; Sharma, V. Mask-associated dry eye disease and dry eye due to prolonged screen time: Are we heading towards a new dry eye epidemic during the COVID-19 era? Indian J. Ophthalmol. 2021, 69, 448–449. [Google Scholar] [CrossRef]
- Barabino, S. A Narrative Review of Current Understanding and Classification of Dry Eye Disease with New Insights on the Impact of Dry Eye during the COVID-19 Pandemic. Ophthalmol. Ther. 2021, 10, 495–507. [Google Scholar] [CrossRef]
- Koh, S.; Rhee, M.K. COVID-19 and Dry Eye. Eye Contact Lens 2021, 47, 317–322. [Google Scholar] [CrossRef]
- Messmer, E.M. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch. Arztebl. Int. 2015, 112, 71–81; quiz 82. [Google Scholar] [CrossRef]
- Craig, J.P.; Nelson, J.D.; Azar, D.T.; Belmonte, C.; Bron, A.J.; Chauhan, S.K.; de Paiva, C.S.; Gomes, J.A.P.; Hammitt, K.M.; Jones, L.; et al. TFOS DEWS II Report Executive Summary. Ocul. Surf. 2017, 15, 802–812. [Google Scholar] [CrossRef]
- Giannaccare, G.; Vaccaro, S.; Mancini, A.; Scorcia, V. Dry eye in the COVID-19 era: How the measures for controlling pandemic might harm ocular surface. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 2567–2568. [Google Scholar] [CrossRef] [PubMed]
- Krolo, I.; Blazeka, M.; Merdzo, I.; Vrtar, I.; Sabol, I.; Petric-Vickovic, I. Mask-Associated Dry Eye During COVID-19 Pandemic-How Face Masks Contribute to Dry Eye Disease Symptoms. Med. Arch. 2021, 75, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Moshirfar, M.; West, W.B.; Marx, D.P. Face Mask-Associated Ocular Irritation and Dryness. Ophthalmol. Ther. 2020, 9, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, L.; Lanzini, M.; Brescia, L.; D’Aloisio, R.; Nubile, M.; Ciancaglini, M.; D’Amario, C.; Agnifili, L.; Mastropasqua, R. Face mask-related ocular surface modifications during COVID-19 pandemic: A clinical, in vivo confocalmicroscopy, and immune-cytology study. Transl. Vis. Sci. Technol. 2021, 10, 22. [Google Scholar] [CrossRef]
- Viola, I.M.; Peterson, B.; Pisetta, G.; Pavar, G.; Akhtar, H.; Menoloascina, F.; Mangano, E.; Dunn, K.E.; Gabl, R.; Nila, A.; et al. Face coverings, aerosol dispersion and mitigation of virus transmission risk. arXiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.W.; Liebner, T.J.; Craven, B.A.; Settles, G.S. A schlieren optical study of the human cough with and without wearing masks for aerosol infection control. J. R. Soc. Interface 2009, 6, 727–736. [Google Scholar] [CrossRef]
- Verma, S.; Dhanak, M.; Frankenfield, J. Visualizing the effectiveness of face masks in obstructing respiratory jets. Phys. Fluids 2020, 32. [Google Scholar] [CrossRef]
- World Health Organization. Mask Use in the Context of COVID-19; World Health Organization: Geneva, Switzerland, 2020; pp. 1–10. [Google Scholar]
- Okumura, Y.; Inomata, T.; Iwata, N.; Sung, J.; Fujimoto, K.; Fujio, K.; Midorikawa-Inomata, A.; Miura, M.; Akasaki, Y.; Murakami, A. A review of dry eye questionnaires: Measuring patient-reported outcomes and health-related quality of life. Diagnostics 2020, 10, 559. [Google Scholar] [CrossRef]
- Bron, A.J.; Evans, V.E.; Smith, J.A. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea 2003, 22, 640–650. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Kumar, S.; Lee, H.P. The perspective of fluid flow behavior of respiratory droplets and aerosols through the facemasks in context of SARS-CoV-2. Phys. Fluids 2020, 32, 111301. [Google Scholar] [CrossRef] [PubMed]
- Clayton, J.A. Dry Eye. N. Engl. J. Med. 2018, 378, 2212–2223. [Google Scholar] [CrossRef] [PubMed]
- Wyon, N.M.; Wyon, D.P. Measurement of acute response to draught in the eye. Acta Ophthalmol. 1987, 65, 385–392. [Google Scholar] [CrossRef] [PubMed]
- McCulley, J.P.; Uchiyama, E.; Aronowicz, J.D.; Butovich, I.A. Impact of evaporation on aqueous tear loss. Trans. Am. Ophthalmol. Soc. 2006, 104, 121–128. [Google Scholar] [PubMed]
- Koh, S.; Tung, C.; Kottaiyan, R.; Zavislan, J.; Yoon, G.; Aquavella, J. Effect of airflow exposure on the tear meniscus. J. Ophthalmol. 2012, 2012, 983182. [Google Scholar] [CrossRef]
- Oncel, B.A.; Pinarci, E.; Akova, Y.A. Diurnal variation of the tear osmolarity in normal subjects measured by a new microchip system. Eur. J. Ophthalmol. 2012, 22, 10–13. [Google Scholar] [CrossRef]
- Pena-Verdeal, H.; García-Resúa, C.; Ramos, L.; Yebra-Pimentel, E.; Giráldez, M.J. Diurnal variations in tear film break-up time determined in healthy subjects by software-assisted interpretation of tear film video recordings. Clin. Exp. Optom. 2016, 99, 142–148. [Google Scholar] [CrossRef]
- Masmali, A.M.; Al-Bahlal, J.M.; El-Hiti, G.A.; Akhtar, S.; Purslow, C.; Murphy, P.J.; Almubrad, T. Repeatability and diurnal variation of tear ferning test. Eye Contact Lens 2015, 41, 262–267. [Google Scholar] [CrossRef]
- Ayaki, M.; Tachi, N.; Hashimoto, Y.; Kawashima, M.; Tsubota, K.; Negishi, K. Diurnal variation of human tear meniscus volume measured with tear strip meniscometry self-examination. PLoS ONE 2019, 14, e0215922. [Google Scholar] [CrossRef]
- Lira, M.; Oliveira, M.E.C.R.; Franco, S. Comparison of the tear film clinical parameters at two different times of the day. Clin. Exp. Optom. 2011, 94, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.M.; Lane, K.J.; Ousler, G.W.; Abelson, M.B. Diurnal variation of visual function and the signs and symptoms of dry eye. Cornea 2010, 29, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Read, S.A.; Collins, M.J.; Carney, L.G. The diurnal variation of corneal topography and aberrations. Cornea 2005, 24, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Wang, X.; Tong, Q.; Xia, J.; Shen, Y. Investigation of dry eye symptoms of medical staffs working in hospital during 2019 novel coronavirus outbreak. Medicine 2020, 99, e21699. [Google Scholar] [CrossRef] [PubMed]
- Korb, D.R.; Blackie, C.A. Using goggles to increase periocular humidity and reduce dry eye symptoms. Eye Contact Lens 2013, 39, 273–276. [Google Scholar] [CrossRef]
- World Health Organization. The Impact of COVID-19 on Health and Care Workers: A Closer Look at Deaths; Working Paper;1; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Lesage, M. Work-related diseases and occupational diseases: The ILO international list. Encycl. Occup. Health Saf. 1998, 1, 26-2. [Google Scholar]

| Study Group = 100 | Control Group = 20 | ||||
|---|---|---|---|---|---|
| Parameter | Value | SD | Value | SD | p |
| Mean age (years) | 44.56 | 14.87 | 40.9 | 13.93 | 0.069 |
| Sex | |||||
| M | 44 (44%) | 8 (40%) | 0.74 | ||
| F | 56 (56%) | 12 (60%) | |||
| Mean OSDI | 12.41 | 12.06 | 12.57 | 12.78 | 0.82 |
| Mean McMonnies | 10.22 | 5.25 | 11.28 | 5.38 | 0.53 |
| Mean VDT use (h) | 0.60 | 0.95 | 0.7 | 0.86 | 0.47 |
| Glasses/eye protection | |||||
| Yes | 49 (49%) | ||||
| No | 51 (51%) | ||||
| Parameter | Before Work Shift | SD | End of Work Shift | SD | p-Value |
|---|---|---|---|---|---|
| Mean BCVA (LogMar) | 0.05 | 0.09 | 0.07 | 0.10 | <0.001 |
| Mean Schirmer test value (mm) | 16.16 | 8.90 | 14.04 | 9.70 | <0.001 |
| Mean BUT (seconds) | 9.15 | 2.67 | 7.49 | 2.53 | <0.001 |
| Mean FS (OGS) | 0.10 | 0.35 | 0.51 | 0.66 | <0.001 |
| Pre-Shift Parameter | Control Group | Study Group | p-Value |
|---|---|---|---|
| Mean BCVA (LogMar) | 0.025 | 0.05 | 0.06 |
| Mean Schirmer Test Value (mm) | 18.68 | 16.16 | 0.12 |
| Mean BUT (seconds) | 10.38 | 9.15 | 0.24 |
| Mean FS (OGS) | 0.15 | 0.1 | 0.22 |
| Parameter | 8:00 a.m. Examination | SD | 3:00 p.m. Examination | SD | p-Value |
|---|---|---|---|---|---|
| Mean BCVA (LogMar) | 0.025 | 0.07 | 0.01 | 0.03 | 0.09 |
| Mean Schirmer Test Value (mm) | 18.68 | 6.94 | 18.35 | 7.34 | 0.69 |
| Mean BUT (seconds) | 10.38 | 3.64 | 10.25 | 3.40 | 0.59 |
| Mean FS (OGS) | 0.15 | 0.36 | 0.2 | 0.40 | 0.15 |
| N. Eyes (Mean Values ± SD) | ||
|---|---|---|
| Schirmer Test | Pre-WS | Post-WS |
| <10 mm/5 m | N. Eyes: 50 (4.9 ± 1.56) | N. eyes: 76 (4.32 ± 4.51) |
| <5 mm/5 m | N. Eyes: 9 (2.44 ± 1.24) | N. Eyes: 39 (1.56 ± 1.33) |
| BUT | ||
| <10 s | N. Eyes: 104 (7.01 ± 1.65) | N. Eyes: 153 (6.17 ± 1.97) |
| 5–10s | N. Eyes: 95 (7.35 ± 1.26) | N. Eyes: 130 (6.46 ± 1.79) |
| <5 s | N. Eyes: 9 (3.44 ± 0.72) | N. Eyes: 23 (3.11 ± 0.92) |
| Subjects | ||
| DED symptoms (OSDI score ≥ 13) | 33 | |
| Mild (13–22) | 17 | |
| Moderate (23–32) | 8 | |
| Severe (33–100) | 8 | |
| DED Diagnosis (OSDI score ≥ 13 and BUT < 10 s) | 21 | 32 |
| Surgical Mask Group (n = 40) | N95 Group (n = 60) | p-Value | |
|---|---|---|---|
| Age (y) | 45.2 ± 14.7 | 44.1 ± 15.1 | 0.72 |
| Gender (M:F) | 20:20 | 24:36 | 0.32 |
| OSDI | 9.5 ± 9.2 | 13.8 ± 13.6 | 0.06 |
| McMonnies | 9.2 ± 4.7 | 10.9 ± 5.5 | 0.10 |
| VDT use (h) | 0.7 ± 1.1 | 0.6 ± 0.8 | 0.61 |
| Wearing glasses | 17 | 34 | 0.16 |
| Test of within-Subjects Effect | ||||||||
|---|---|---|---|---|---|---|---|---|
| Schirmer (mm) | BUT (s) | BCVA (LogMar) | FS (OGS) | |||||
| SOURCE | F (1,198) | p-Value | F (1,198) | p-Value | F (1,198) | p-Value | F (1,198) | p-Value |
| Pre/Post Work Shift | 23.54 | <0.001 | 132.60 | <0.001 | 23.60 | <0.001 | 12.16 | <0.001 |
| Face Mask Type | 0.48 | 0.49 | 2.57 | 0.111 | 0.69 | 0.41 | 2.79 | 0.96 |
| Parameter | Age (y) | Gender | OSDI Score | McMonnies Score | VDT Use Time (h) | Wearing Glasses |
|---|---|---|---|---|---|---|
| BCVA Variation (LogMar) | −0.23 (p = 0.0047) | 0.15 (p = 0.0187) | −0.20 (p = 0.0303) | −0.13 (p = 0.1333) | −0.02 (p = 0.7077) | −0.07 (p = 0.1975) |
| Schirmer Test Variation (mm) | 0.09 (p = 0.2212) | −0.11 (p = 0.2265) | 0.05 (p = 0.1921) | 0.04 (p = 0.7628) | 0.12 (p = 0.1543) | −0.019 (p = 0.6985) |
| BUT Variation (s) | −0.08 (p = 0.0833) | −0.04 (p = 0.6917) | 0.02 (p = 0.5643) | −0.12 (p = 0.2213) | −0.08 (p = 0.0469) | 0.05 (p = 0.6157) |
| FS Variation (OGS) | −0.11 (p = 0.0859) | 0.06 (p = 0.4098) | 0.11 (p = 0.3813) | 0.08 (p = 0.1472) | −0.05 (p = 0.1970) | −0.11 (p = 0.1019) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatti, F.; Mangoni, L.; Pirodda, S.; Demarinis, G.; Iovino, C.; Siotto Pintor, E.; Orrù, G.; Lecca, L.I.; Campagna, M.; Denotti, G.; et al. Ocular Surface Changes Associated with Face Masks in Healthcare Personnel during COVID-19 Pandemic. Life 2022, 12, 1491. https://doi.org/10.3390/life12101491
Tatti F, Mangoni L, Pirodda S, Demarinis G, Iovino C, Siotto Pintor E, Orrù G, Lecca LI, Campagna M, Denotti G, et al. Ocular Surface Changes Associated with Face Masks in Healthcare Personnel during COVID-19 Pandemic. Life. 2022; 12(10):1491. https://doi.org/10.3390/life12101491
Chicago/Turabian StyleTatti, Filippo, Lorenzo Mangoni, Simone Pirodda, Giuseppe Demarinis, Claudio Iovino, Emanuele Siotto Pintor, Germano Orrù, Luigi Isaia Lecca, Marcello Campagna, Gloria Denotti, and et al. 2022. "Ocular Surface Changes Associated with Face Masks in Healthcare Personnel during COVID-19 Pandemic" Life 12, no. 10: 1491. https://doi.org/10.3390/life12101491