
Near-Infrared Spectroscopy (NIRS) versus Hyperspectral Imaging (HSI) to Detect Flap Failure in Reconstructive Surgery: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction
2.2. Data Synthesis
3. Results
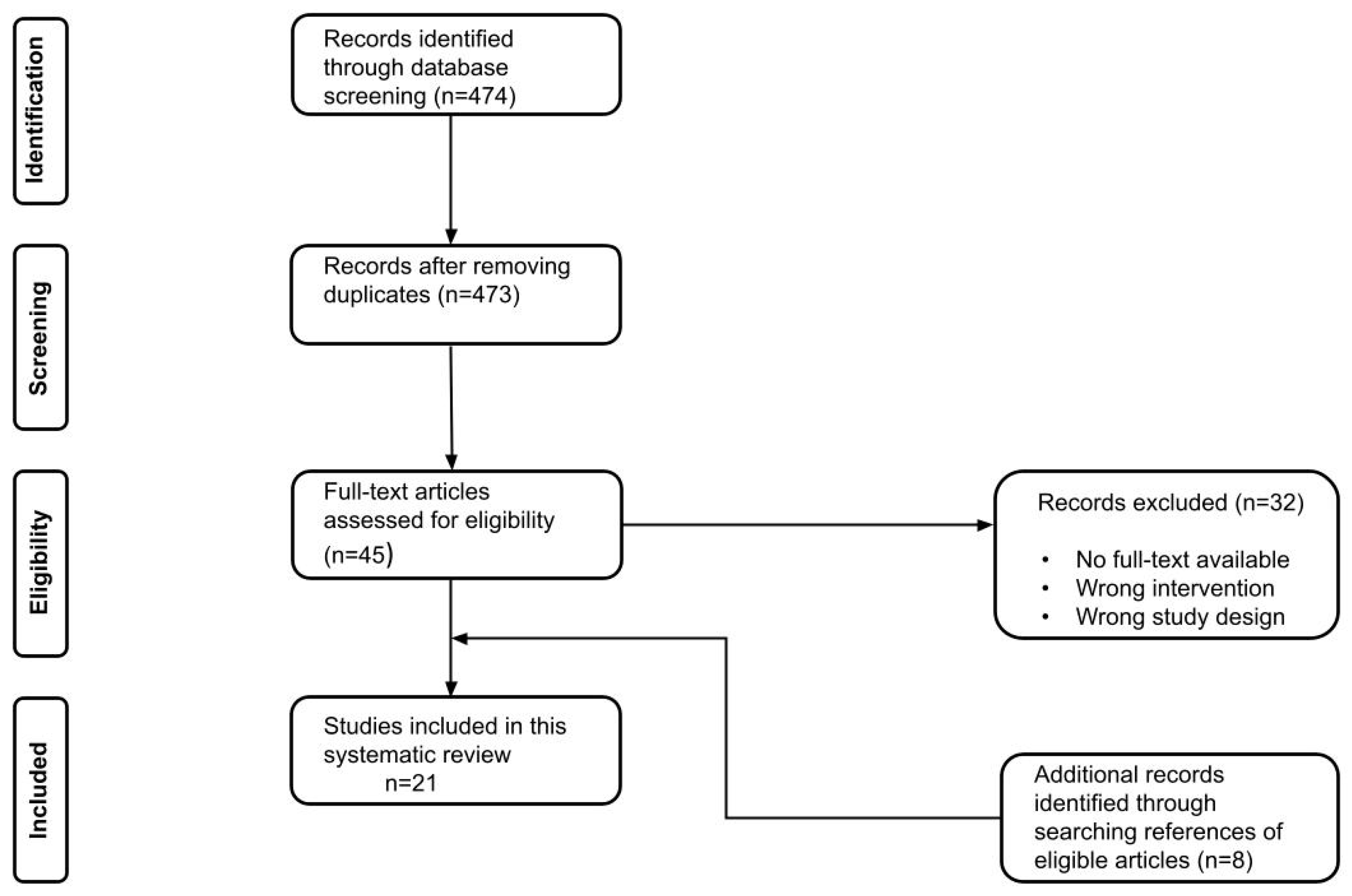
3.1. Literature Search
3.2. Overall Flap Surgery Patient Profiles
3.3. Flap-Related Characteristics
3.4. Detection of Flap Failure

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Year of Publication | Study Type | Study Period | Researched Monitoring Tool (model) | Objective | Patients (N) | Flaps (N) | Age (years) | Female (N, %) | Body Mass Index (kg/m2) | Flap Survival (%) | Monitoring Control Technique |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cai [30] | China | 2007 | Prospective | Na | NIRS (TSNIR-3) first 24 h every 4 h, 2 per day in the following 5 days | Test sensibility and precision | 41 | 41 | 42 (14–73) | 11 (26.8) | Na | 97.6 | CE |
| Carruthers [25] | USA | 2019 | Retrospective | 24 months | NIRS (T.Ox ViOptix) until discharge | Reduce monitoring time | 196 | 301 | 50.7 ± 8.3 | 196 (100) | 30.7 ± 5.5 | 100 | CE, pD every hour first 12 h, every 4 h |
| Guye [31] | France | 2017 | Prospective | 7 months | NIRS (InSpectra Model 650) | Reassess risk factors for free flap complications | 40 | 40 | NC 53.3 ± 13.6, C 58 ± 15.9 | 18 (45) | C 26 ± 1.7, NC 22 ± 0.7 | 90 | CE |
| Keller [23] | USA | 2009 | Prospective | Jan 2005– Jan 2008 | NIRS (T.Ox ViOptix) for 36 h | Continuation of an earlier preliminary study | 145 | 208 | Na | 145 (100) | Na | 100 | CE, hD; hourly for first night, every 2 h for the next 36 h |
| Koolen [26] | USA | 2016 | Retrospective | Feb 2004–Jun 2008, Jun 2008–Feb 2014 | Control, NIRS (T.Ox ViOptix) for 72 h | Compare standard monitoring with NIRS | Co 288, Ni 451 | Co 380, Ni 670 | Co 47.7 ± 7.9, Ni 49.9 ± 8.5 | Co 288 (100), Ni 451 (100) | Co 26.9 ± 5, Ni 28.9 ± 5.6 | Co 57.7, Ni 96.6 | CE |
| Lin [32] | USA | 2010 | Retrospective | Jan 2004–Dec 2007, Jan 2008–Dec 2010 | Control, NIRS (T.Ox ViOptix) for 72 h | Compare monitoring with and without tissue oximetry | Co 288, Ni 164 | Co 380, Ni 234 | Co 47.69 ± 8.44, Ni 49.85 ± 7.88 | Co 288 (100), Ni 164 (100) | Na | Co 97.1, Ni 99.6 | CE, hD; every 15min first hr, every 30 min second hr, every hour for next 10 h. Surgical resident every 4 h CE. |
| Lindelauf [24] | NL | 2021 | Prospective | Na | NIRS (FORE-SIGHT MC-2030) for 24 h | Confirm the usefulness of NIRS in postoperative monitoring | 30 | 42 | 51 ± 13 | 30 (100) | 27.5 ± 4.3 | 100 | CE, Doppler according to hospital protocol |
| Lohman [8] | USA | 2013 | Prospective | Jan 2006–Feb 2007 | NIRS (ViOptix) for 72 h | Determine the most useful method | 38 | 38 | 38.5 (21–84) | 27 (71.1) | Na | 100 | CE, hD, hourly;iD |
| Pelletier [33] | USA | 2011 | Prospective | Aug 2006–Jan 2010 | NIRS (ViOptix ODIsey) for 72 h | Evaluate the costs of autologous free tissue breast reconstruction | 50; ICU 25, Floor 25 | 54 | ICU 49.4 (31–67), Floor 49 (28–75) | 50 (100) | ICU 27.9 (19.5–43), Floor 28.5 (21.8–36.3) | 98 | CE, hD; ICU every hour, Floor every 4–6 h |
| Repez [11] | Slovenia | 2007 | Prospective | Aug 2004–Sep 2005 | NIRS (InSpectra Model 325) for 72 h | Ascertain whether NIRS could be trustworthy | 48 | 50 | 47 (31–64) | 48 (100) | 26 (22–35) | 94 | CE hourly for 72 h |
| Ricci [34] | USA | 2017 | Retrospective | May 2008–Aug 2014 | NIRS (ViOptix T.Ox) for 72 h | Earlier transfer of patients to a standard surgical inpatient floor | 595 | 900 | 50.3 ± 8.6 | 595 (100) | 28.8 ± 5.6 | 99.7 | CE first 24 h, hD; every 15 min for first hr, every 30 min for second hr, every hr for the next 22 h |
| Salgarello [35] | Italy | 2018 | Retrospective | Jan 2015–Jan 2016 | NIRS (INVOS 5100C) for 48 h | Identify patient- and flap related variables that can affect rSO2 | 45 | 45 | 52.6 (34–69) | 45 (100) | ** | 100 | ICG imaging |
| Steele [36] | USA | 2011 | Retrospective | Jan 2007–May 2010 | Control, NIRS (ViOptix T.Ox) for 4.5d average | Examine outcomes using a tissue oximeter | Co 50, Ni 63 | Co 53, Ni 75 | Co 57.6 (11–85), Ni 58 (17–89) | Co 18 (36), Ni 29 (46) | Na | Co 90.6, Ni 98.7 | CE, hD, hourly for 48 h, then every 2 h for the following 48 h, then every 4 h * |
| Vranken [27] | NL | 2017 | Prospective | Na | NIRS (INVOS 5000C) for 24 h | Suitability for the assessment of tissue perfusion | 29 | 29 | 50 ± 10 | 29 (100) | 26.4 ± 3.3 | 100 | CE, Doppler ultrasonography |
| Whitaker [37] | UK | 2012 | Prospective | Na | NIRS (InSpectra Model 650) for 72 h | Investigate NIRS technology | 10 | 10 | 46 (28–61) | 10 (100) | Na | 90 | CE, hD (hourly), capillary bleeding (25 gauge needle) |
| Yano [28] | Japan | 2020 | Prospective | Sep 2011–Jan 2016 | NIRS (TOS-96/TOS-OR) for 72 h | Investigate the feasibility of perioperative NIRS monitoring | 25 | 25 | 63.5 (39–85) | 2 (8) | Na | 100 | CE, ICG imaging |
| Calin [20] | Romania | 2017 | Case report | Na | HSI (ImSpector V8E) 0, 2, 4, 24 and 48 h postoperatively | Assess value as a monitoring tool | 1 | 1 | 61 | 0 | Na | 100 | CE |
| Kohler [29] | Germany | 2021 | Prospective | Mar 2019–Jan 2020 | HSI (TIVITA) at t0(0), t1(16–28), t2(39–77) hrs postoperatively | Show the superiority of HSI | 22 | 22 | 55 (26–92) | 5 (22.7) | Na | 81.8 | CE, Doppler ultrasound every 2 h within 24 h, every 4 h until 72 h postoperatively |
| Schulz (‘20) [38] | Germany | 2020 | Retrospective | Dec 2017–Apr 2018 | HSI (TIVITA) for 7 days | Evaluate HSI as a monitoring method for pedicled flaps | 16 | 16 | 58 (25–78) | 2 (12.5) | Na | 93.8 | Na |
| Schulz (‘21) [39] | Germany | 2021 | Prospective | Jul 2017–Sep 2018 | HSI (TIVITA) for 7 days | Investigate HSI as a method for free flap monitoring | 18 | 18 | 54 (24–87) | 4 (22.2) | Na | 94.4 | CE |
| Thiem [22] | Germany | 2020 | Prospective | Na | HSI (TIVITA) at t1(0), t2(0–1), t3(4–8), t4(8–12), t5(12–24), t6(24–48), t7(>48) | Feasibility of HSI for objective and reproducible monitoring | 33 | 33 | Na | Na | Na | 97 | CE 72 h |
| Author | Mean Ischaemia Time (min) | Types of Flaps (N) | Vascular Disease (N, %) | DM (N, %) | Smoker (N, %) | XRT (N, %) | Chemo (N, %) |
|---|---|---|---|---|---|---|---|
| Cai [30] | Na | Fibular 41 | Na | Na | Na | Na | Na |
| Carruthers [25] | Na | DIEP 301 (111 delayed, 36.9%) | Na | 8 (4.1) | 9 (4.6) | 78 (25.9) | Na |
| Guye [31] | NC 74 ± 4.5, C 70 ± 6.8 | Fibular 15, Radial 20, gastro-omental 5 | 5 (12.5) | 5 (12.5) | Na | 9 (22.5) | Na |
| Keller [23] | Na | DIEP 197, SIEA 1, SGAP 10 | Na | Na | Na | Na | Na |
| Koolen [26] | Na | Co; DIEP 336, SIEA 15, Free TRAM 9, SGAP 20 Ni; DIEP 646, SIEA 1, Free TRAM 3, SGAP 20 | CAD Co 1 (0.3), Ni 5 (0.7) | Co 8 (2.1), Ni 28 (4.2) | Co 30 (7.9), Ni 85 (12.7) | Co 105 (27.6), Ni 235 (35.1) | Co 157 (41.4), Ni 379 (58.2) |
| Lin [32] | Na | Co; DIEP 336, SIEA 15, SGAP 20, Free TRAM 9 Ni; DIEP 222, SGAP 9, Free TRAM 3 | Na | Na | Na | Na | Na |
| Lindelauf [24] | 42 (35–51) | DIEP 42 (17 secondary) | Na | Na | 2 (7) | Na | Na |
| Lohman [8] | Na | DIEP 18, ALT 15, MS-TRAM 5 | Na | Na | Na | Na | Na |
| Pelletier [33] | ICU 86.7 (46–157), Floor 78.5 (48–138) | DIEP 21, DIEP + DIEP 1, DIEP/SIEV 2, DIEP + SIEA 3, SIEA 9, Free TRAM 3, Free MS-TRAM 11 | 0 | Floor 1, ICU 0 | Floor 1, ICU 0 | Floor 12, ICU 12 | Floor 11, ICU 12 |
| Repez [11] | Na | DIEP 37 (13 secondary), SIEA 5, SGAP 8 (5 secondary) | 0 | 1 (2) | 7 (14) | Na | Na |
| Ricci [34] | Na | DIEP 872, SIEA 2, SGAP 23, TRAM 3 | CAD 5 (<0.1) | 32 (3.6) | 89 (9.9) | 265 (29.4) | 414 (46) |
| Salgarello [35] | Na | DIEP 45 | Na | Na | Na | Na | Na |
| Steele [36] | Na | Co; DIEP 5, ALT 7, Fibular 5, LD 3, Scapula osteocutaneous 1, Free TRAM 14, Radial 14, gracilis 4 Ni; DIEP 26, ALT 20, Fibular 8, Free TRAM 2, MS-TRAM 4, Radial 15 | Na | Na | Na | Na | Na |
| Vranken [27] | 48 ± 12 | DIEP 29 | Na | Na | Na | Na | Na |
| Whitaker [37] | Na | DIEP 10 | Na | Na | Na | Na | Na |
| Yano [28] | Na | FJG 25 | Na | Na | Na | 6 (24) | 20 (80) |
| Calin [20] | Na | Fasciocutaneous sural flap 1 | 1 (100) | 1 (100) | Na | Na | Na |
| Kohler [29] | Na | DIEP 3, ALT 11, LD 4, Scapula osteocutaneous 1 (parascapular), MS2-TRAM 2, Rectus abdominis 1 (18 with, 4 without skin island) | PAD 4 (18.2), CAD 3 (13.6) | 5 (22.7) | 4 (18.2) | Na | Na |
| Schulz (‘20) [38] | Na | Suralis 3, LD 5, Radial 2, gastrocnemius 2, TFL 1, Foucher 1, MCPA 1, Crossfinger 1 | Na | Na | Na | Na | Na |
| Schulz (‘21) [39] | Na | ALT 10, LD 8 | PAD 7 (38.9), CAD 5 (27.8) | 8 (44.4) | 12 (66.7) | Na | Na |
| Thiem [22] | Na | 25 FF; ALT 3, Radial 12, Osteocutaneous fibula 4, Osteocutaneous scapular 3, Unknown 3 8 PF; PM 3, LD 2, NL 1, LSS 2 | Na | Na | Na | Na | Na |
| Author | Decisive Monitoring | Warning Value | Description | Flaps with Vascular Crisis (N, %) | Flaps Returned to OR (N, %) | Salvage Rate (%) | Average Time to Discharge (days) | Total Loss Rate (N, %) | Partial Loss Rate (N, %) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cai [30] | NIRS | rSO2 70% | Anastomosis vein again, intraoral infection day 7, necrosis 1 | venous 1 (2.4) | 1 (2.4) | 0 | Na | 1 (2.4) | 0 | 100 | 100 |
| Carruthers [25] | NIRS (5 microvascular) | rSO2 | Microvascular 5 (3 immediate reconstructions, 2 delayed cases), Nonvascular 9 (1 positive margin required reexcision, 8 hematoma) | 5 (1.7); venous congestion 3, arterial thrombus 2 | 14 (4.7) | 100 | 3.4 ± 1.1 | 0 | 0 | Na | Na |
| Guye [31] | Na | Na | Venous thrombosis 2, Partial or total necrosis of the flap 8 ( arterial thrombosis 3) | venous thrombosis 2 (5) | Na | Na | Na | 4 (10) | 4 (10) | Na | Na |
| Keller [23] | NIRS | ΔStO2/Δt ≥ 20%/h sustained >30 min | Hematoma, superficial vein thrombosis and vein kink 1, Deep vein thrombosis 2, Arterial thrombosis 2 | 5 (2.4); venous 3, arterial 2 | 5 (2.4, 1 triple) | 100 | Na | 0 | 0 | 100 | 100 |
| Koolen [26] | Na | Co Na, Ni 20-point drop in 1 h OR absolute reading <30% | Na | Na | Co 26 (6.8), Ni 29 (4.3) | Co 57.7, Ni 96.6 | Na | Co 11(2.9), Ni 1(0.1) | Co 8 (2.1) Ni 7 (1) | Co Na, Ni 96.5 | Co Na, Ni 99.8 |
| Lin [32] | Co CE/hD, Ni NIRS | Co Na, Ni 20-point drop in 1 h OR absolute reading <30% | Co; Na, Ni; Venous thrombosis resulted in total loss 1 | Co 26 (6.8), Ni 16 (6.8) | Co 26 (6.8), Ni 16 (6.8) | Co 57.7, Ni 93.8 | Na | Co 11 (2.9), Ni 1 (0.43) | Co 8 (2.1), Ni 4 (1.7) | Co Na, Ni 100 | Co Na, Ni 100 |
| Lindelauf [24] | Na | Na | Minor complication 13, Major complication 5 (debridement for fat necrosis 1, arterial kinking 1, evacuation hematoma 1, insufficient perfusion resulting in partial loss 1, venous kinking 1) | 3 (7.1) | 5 (12) | 100 | no/minor c 5 [4,5] | 0 | 1 (2.4) | 100 | 100 |
| Lohman [8] | NIRS ( in ⅘) | StO2 ≤30% | Hematomas 2, Venous thrombosis 1, Venous kinking and clotting 1, Venous clotting 1 | 4 (13.2); 3 venous, 1 arteriovenous | 5 (13.2) | 100 | Na | 0 | 0 | 100 | 100 |
| Pelletier [33] | NIRS | StO2 <30% OR StO2 >20%/h drop for 30 min | Venous thrombosis 3, No reoperation 1 | 4 (8); ICU venous 3, Floor 1 | 3 (6) | 75 | Na | ICU 1 (2) | 0 | 100 | 100 |
| Repez [11] | NIRS | StO2 <50% of initial value | Venous thrombosis 8, Arterial thrombosis 2 | 10 (20); arterial 2, venous 11 | 10 (20, 1 twice, 1 triple) | 70 | Na | 3 (6) | 0 | 100 | 100 |
| Ricci [34] | Na | 20-point drop in 1 h OR absolute reading <30% | Venous thrombosis, pedicle kinking or hematoma causing compression 25, Arterial thrombosis or kinking 6, Arteriovenous thrombus 1 | 32 (3.6); venous 25, arterial 6, combined 1 | 32 (3.6, 16 within 24 h) | 90.6 | Na | 3 (<0.1) | 10 (1.1) | 96.5 | 99.8 |
| Salgarello [35] | Na | rSO2 ≤30% OR drop rate in rSO2 ≥ 20% | Na | 0 | 0 | Na | Na | 0 | 0 | Na | Na |
| Steele [36] | Co CE/hD, Ni NIRS | Co Na, Ni StO2 ≤40% OR drop rate StO2 ≥15%/h | Ni; Arterial thrombosis resulting in total loss 1 Hematomas with venous congestion/thrombosis 3 Vascular pedicle kinked during the inset and closure 2 Arterial spasm 1 | Co 5 (9.4), Ni 7 (9.3) | Co 4 (7.5), Ni 3 (4) | Co 0, Ni 85.7 | Co 14.5, Ni 10.7 | Co 5 (9.4), Ni 1 (1.3) | 0 | Co Na, Ni 100 | Co Na, Ni 100 |
| Vranken [27] | CE/Doppler | Proposed; enlarged ΔStO2 ≥ 38%, decreased StO2 ≤ 43% | StO2 43%; Second anastomosis 1, StO2 44%; partial necrosis (day 5) 1 | 2 (6.9); venous congestion 1 | 2 (7) | 100 | 5 | 0 | 1 (3.4) | Na | Na |
| Whitaker [37] | NIRS | StO2/THI ≤50% of starting value | Venous thrombosis requiring revision anastomosis 3, Minor debridement (after 3–5 days) 2, Evacuation hematoma; flap loss 1 | 4 (40); venous 3 | 3 (30) | 75 | 6–13 | 1 (10) | 0 | 100 | 100 |
| Yano [28] | ICG/CE | Proposed; rSO2 < 55% | Subcutaneous hematoma (detachment anastomosis 3 weeks later) 1, Anastomosis revision; suspected inadequate venous drainage 1 | venous 1 (4) | 1 (4) | 100 | Na | 0 | 0 | Na | Na |
| Calin [20] | Na | Na | Na | 0 | 0 | Na | Na | 0 | 0 | Na | Na |
| Kohler [29] | HSI | Proposed; StO2 <40% and NIR <40 | Venous thrombosis 4 | venous 4 (18.2) | 6 (27.3) | 33.3 | Nr 12 ± 6.6, partial 11.5 ± 2.1, Cr 30 ± 14.5 | 4 (18.2) | 2 (9.1) | 100 | 100 |
| Schulz (‘20) [38] | Na | venous value change; THI 43% → 57%, StO2 45 → 31%, NIR 43 → 25%, TWI 33 → 24% | Minor complication (e.g. wound edge necrosis) 15, Venous congestion radial flap resulting in loss 1 | venous congestion 1 (6.3) | Na | 0 | Na | 1 (6.3) | Na | Na | Na |
| Schulz (‘21) [39] | Na | Proposed; venous THI ≥53%, NIR ≤25%, TWI ≤43%, StO2 ≤22% arterial drop of StO2 ≤3%, THI ≤3% | Arterial embolism resulting in flap loss 1, partial flap necrosis caused by local impaired perfusion 9 | arterial 1 (5.6) | 1 (5.6, triple) | 0 | Na | 1 (5.6) | 9 (50) | Na | Na |
| Thiem [22] | HSI | Proposed; StO2 <45%, NIR <25% | Venous thrombosis 2, Arterial occlusion 1 | 3 (9.1); venous 2, arterial 1 | 3 (9.1, all FF) | 33 | Na | 2 (6.1) | 0 | 100 | 100 |
| Technique | Model | Proposed Warning Value | Vascular Crisis | Venous Congestion | Arterial Occlusion |
|---|---|---|---|---|---|
| NIRS | ViOptix [23] (ViOptix Inc., Fremont, Ca, USA) InSpectra [11] (Hutchinson Technology Inc., Hutchinson, Mn, USA) | rSO2 ≤ 30% OR drop rate in rSO2 ≥ 20% StO2 < 50% of initial value | HbO2, StO2 drop Hb rise | HbT rise | HbT drop |
| HSI | TIVITA [22,39] (Diaspective Vision GmbH, Am Salzhaff, Germany) | Venous THI ≥ 53%, NIR ≤ 25%, TWI ≤ 43%, StO2 ≤ 22% Arterial Drop of StO2 ≤ 3%, THI ≤ 3% | StO2, NIR low | THI high | THI low |
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

| Author | Inclusion Criteria |
|---|---|
| Cai [30] | All patients undergoing autogenous mandibular reconstruction by vascular fibular flap transplantation. |
| Calin [20] | Chosen for case report after receiving informed consent. |
| Carruthers [25] | All patients who underwent microsurgical breast reconstruction with free DIEP flaps over 24 consecutive months. |
| Guye [31] | Patients undergoing resection of a cervicofacial tumour and immediate reconstruction with a free flap. |
| Keller [23] | Patients undergoing autologous tissue perforator free flap breast reconstruction. |
| Kohler [29] | Patients aged 18 and older who underwent soft tissue reconstruction using a free flap between March 2019 and January 2020 and had given informed consent. |
| Koolen [26] | All immediate and delayed autologous microsurgical free tissue transfers for breast reconstruction from February of 2004 to February of 2014. |
| Lin [32] | All patients undergoing microsurgical breast reconstruction between 2004 and 2010 at Beth Israel Deaconess Medical Center were identified. |
| Lindelauf [24] | Female patients undergoing unilateral or bilateral, immediate or delayed DIEP flap breast reconstructive surgery at one university medical center were included. |
| Lohman [8] | Consecutive patients with free flaps - including external skin paddles - performed between January 2006 and February 2007 were monitored. |
| Pelletier [33] | Any patient scheduled to undergo unilateral autologous free tissue breast reconstruction. |
| Repez [11] | Consecutive free flap autologous breast reconstruction. |
| Ricci [34] | All autologous microsurgical free tissue transfers for breast reconstruction from May 2008 until August 2014. |
| Salgarello [35] | Consecutive patients undergoing breast reconstruction with DIEP flap. |
| Schulz (‘20) [38] | All patients undergoing soft tissue reconstruction and who had given informed consent. |
| Schulz (‘21) [39] | All patients who underwent free tissue transfer at our department from July 2017 to September 2018 were eligible for inclusion. |
| Steele [36] | The author’s microsurgical cases between January 2007 and May 2010. |
| Thiem [22] | Patients with either free or pedicled flaps for reconstruction in the oro-maxillofacial area were included. |
| Vranken [27] | Female patients undergoing unilateral secondary DIEP-flap surgery were included. |
| Whitaker [37] | All women who were undergoing autologous breast reconstruction following mastectomy, aged between 18 and 65 years old. |
| Yano [28] | Consecutive patients who underwent reconstructive surgery using FJG following the resection of cancer of the pharynx or cervical esophagus. |
Appendix B

| Category | Query |
|---|---|
| #1: Population | ((((((((((Free flap) OR (Free tissue flap)) OR (Surgical flaps)) OR (Mastectomy)) OR (Free tissue transfer flaps)) OR (Perforator flap)) OR (Mastectomy skin flap)) OR (Mastectomy flap)) OR ("surgical flaps"[MeSH Terms])) OR ("mas-tectomy"[MeSH Terms])) OR ("perforator flap"[MeSH Terms]) |
| #2: Intervention | (((((((((((((((((Near infrared spectroscopy) OR (Non invasive flap monitoring)) OR (Flap monitoring)) OR (Nirs)) OR (Hyperspectral imaging)) OR (Hsi)) OR (Tissue oximetry)) OR (Tivita tissue system)) OR (tivita)) OR (Near infrared spectroscopies)) OR (Near infrared spectrometry)) OR (Near infrared spectrometries)) OR (Spectrometries, near in-frared)) OR (Nir spectroscopies)) OR (Nir spectroscopy)) OR (“spectroscopy, near infrared”[MeSH Terms])) OR (“hy-perspectral imaging”[MeSH Terms])) OR (Spectroscopies[MeSH Terms]) |
| #3: Comparators | (((((((((Flap loss) OR (Partial flap loss)) OR (Ischemia)) OR (Necrosis)) OR (Venous congestion)) OR (Venous insuffi-ciency)) OR (Post operative complication)) OR (surgical wound dehiscence)) OR ("venous insufficiency"[MeSH Terms])) OR ("surgical wound dehiscence"[MeSH Terms]) |
| #1, #2 and #3: PIC | #1 AND #2 AND #3 |
References
- Chen, K.-T.; Mardini, S.; Chuang, D.C.-C.; Lin, C.-H.; Cheng, M.-H.; Lin, Y.-T.; Huang, W.-C.; Tsao, C.-K.; Wei, F.-C. Timing of presentation of the first signs of vascular compromise dictates the salvage outcome of free flap transfers. Plast. Reconstr. Surg. 2007, 120, 187–195. [Google Scholar] [CrossRef]
- Hidalgo, D.A.; Jones, C.S. The role of emergent exploration in free-tissue transfer: A review of 150 consecutive cases. Plast. Reconstr. Surg. 1990, 86, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Mirzabeigi, M.N.; Wang, T.; Kovach, S.J.; Taylor, J.A.; Serletti, J.M.; Wu, L.C. Free flap take-back following postoperative microvascular compromise: Predicting salvage versus failure. Plast. Reconstr. Surg. 2012, 130, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Creech, B.; Miller, S. Evaluation of circulation in skin flaps. In Skin Flaps; Grabb, W.C., Myers, M., Eds.; Little, Brown: Boston, MA, USA, 1975; Volume 21. [Google Scholar]
- Sloan, G.M.; Sasaki, G.H. Noninvasive monitoring of tissue viability. Clin. Plast. Surg. 1985, 12, 185–195. [Google Scholar] [CrossRef]
- Yuen, J.C.; Feng, Z. Monitoring free flaps using the laser Doppler flowmeter: Five-year experience. Plast. Reconstr. Surg. 2000, 105, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Keller, A. Noninvasive tissue oximetry for flap monitoring: An initial study. J. Reconstr. Microsurg. 2007, 23, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Lohman, R.F.; Langevin, C.-J.; Bozkurt, M.; Kundu, N.; Djohan, R. A prospective analysis of free flap monitoring techniques: Physical examination, external Doppler, implantable Doppler, and tissue oximetry. J. Reconstr. Microsurg. 2013, 29, 051–056. [Google Scholar] [CrossRef]
- Smit, J.M.; Zeebregts, C.J.; Acosta, R.; Werker, P.M. Advancements in free flap monitoring in the last decade: A critical review. Plast. Reconstr. Surg. 2010, 125, 177–185. [Google Scholar] [CrossRef]
- Colwell, A.S.; Craft, R.O. Near-infrared spectroscopy in autologous breast reconstruction. Clin. Plast. Surg. 2011, 38, 301–307. [Google Scholar] [CrossRef]
- Repež, A.; Oroszy, D.; Arnež, Z.M. Continuous postoperative monitoring of cutaneous free flaps using near infrared spectroscopy. J. Plast. Reconstr. Aesthetic Surg. 2008, 61, 71–77. [Google Scholar] [CrossRef]
- Machens, H.G.; Mailaender, P.; Rieck, B.; Berger, A. Techniques of postoperative blood flow monitoring after free tissue transfer: An overview. Microsurgery 1994, 15, 778–786. [Google Scholar] [CrossRef]
- Irwin, M.; Thorniley, M.; Dore, C.; Green, C. Near infra-red spectroscopy: A non-invasive monitor of perfusion and oxygenation within the microcirculation of limbs and flaps. Br. J. Plast. Surg. 1995, 48, 14–22. [Google Scholar] [CrossRef]
- Thorniley, M.S.; Sinclair, J.; Barnett, N.; Shurey, C.; Green, C. The use of near-infrared spectroscopy for assessing flap viability during reconstructive surgery. Br. J. Plast. Surg. 1998, 51, 218–226. [Google Scholar] [CrossRef]
- Lu, G.; Fei, B. Medical hyperspectral imaging: A review. J. Biomed. Opt. 2014, 19, 010901. [Google Scholar] [CrossRef]
- Goetz, A.F.; Vane, G.; Solomon, J.E.; Rock, B.N. Imaging spectrometry for earth remote sensing. Science 1985, 228, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Grambow, E.; Dau, M.; Holmer, A.; Lipp, V.; Frerich, B.; Klar, E.; Vollmar, B.; Kämmerer, P.W. Hyperspectral imaging for monitoring of perfusion failure upon microvascular anastomosis in the rat hind limb. Microvasc. Res. 2018, 116, 64–70. [Google Scholar] [CrossRef]
- Holmer, A.; Marotz, J.; Wahl, P.; Dau, M.; Kämmerer, P.W. Hyperspectral imaging in perfusion and wound diagnostics–methods and algorithms for the determination of tissue parameters. Biomed. Eng. Biomed. Tech. 2018, 63, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Kulcke, A.; Holmer, A.; Wahl, P.; Siemers, F.; Wild, T.; Daeschlein, G. A compact hyperspectral camera for measurement of perfusion parameters in medicine. Biomed. Eng. Biomed. Tech. 2018, 63, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Calin, M.-A.; Coman, T.; Parasca, S.V.; Bercaru, N.; Savastru, R.S.; Manea, D. Hyperspectral imaging-based wound analysis using mixture-tuned matched filtering classification method. J. Biomed. Opt. 2015, 20, 046004. [Google Scholar] [CrossRef]
- Pruimboom, T.; Schols, R.M.; Van Kuijk, S.M.; Van der Hulst, R.R.; Qiu, S.S. Indocyanine green angiography for preventing postoperative mastectomy skin flap necrosis in immediate breast reconstruction. Cochrane Database Syst. Rev. 2020, 4, CD013280. [Google Scholar] [CrossRef]
- Thiem, D.G.; Frick, R.W.; Goetze, E.; Gielisch, M.; Al-Nawas, B.; Kämmerer, P.W. Hyperspectral analysis for perioperative perfusion monitoring—a clinical feasibility study on free and pedicled flaps. Clin. Oral Investig. 2021, 25, 933–945. [Google Scholar] [CrossRef]
- Keller, A. A new diagnostic algorithm for early prediction of vascular compromise in 208 microsurgical flaps using tissue oxygen saturation measurements. Ann. Plast. Surg. 2009, 62, 538–543. [Google Scholar] [CrossRef]
- Lindelauf, A.A.; Vranken, N.; Schols, R.M.; Bouman, E.A.; Weerwind, P.W.; van der Hulst, R.R. Exploring personalized postoperative non-invasive tissue oximetry in DIEP flap breast reconstruction. Eur. J. Plast. Surg. 2021, 1–9. [Google Scholar] [CrossRef]
- Carruthers, K.H.; Tiwari, P.; Yoshida, S.; Kocak, E. Inpatient flap monitoring after deep inferior epigastric artery perforator flap breast reconstruction: How long is long enough? J. Reconstr. Microsurg. 2019, 35, 682–687. [Google Scholar] [CrossRef]
- Koolen, P.G.; Vargas, C.R.; Ho, O.A.; Ibrahim, A.; Ricci, J.A.; Tobias, A.M.; Winters, H.A.; Lin, S.J.; Lee, B.T. Does increased experience with tissue oximetry monitoring in microsurgical breast reconstruction lead to decreased flap loss? The learning effect. Plast. Reconstr. Surg. 2016, 137, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Vranken, N.; Weerwind, P.; Van Onna, M.; Bouman, E.; Van der Hulst, R. Non-invasive tissue oximetry following unilateral DIEP-flap reconstruction: A pilot evaluation. JPRAS Open 2017, 12, 59–65. [Google Scholar] [CrossRef]
- Yano, A.; Orihashi, K.; Yoshida, Y.; Kuriyama, M. Near-infrared spectroscopy for monitoring free jejunal flap. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Kohler, L.H.; Köhler, H.; Kohler, S.; Langer, S.; Nuwayhid, R.; Gockel, I.; Spindler, N.; Osterhoff, G. Hyperspectral Imaging (HSI) as a new diagnostic tool in free flap monitoring for soft tissue reconstruction: A proof of concept study. BMC Surg. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Cai, Z.-g.; Zhang, J.; Zhang, J.-g.; Zhao, F.-y.; Yu, G.-y.; Li, Y.; Ding, H.-s. Evaluation of near infrared spectroscopy in monitoring postoperative regional tissue oxygen saturation for fibular flaps. J. Plast. Reconstr. Aesthetic Surg. 2008, 61, 289–296. [Google Scholar] [CrossRef]
- Guye, M.-L.; Motamed, C.; Chemam, S.; Leymarie, N.; Suria, S.; Weil, G. Remote peripheral tissue oxygenation does not predict postoperative free flap complications in complex head and neck cancer surgery: A prospective cohort study. Anaesth. Crit. Care Pain Med. 2017, 36, 27–31. [Google Scholar] [CrossRef]
- Lin, S.J.; Nguyen, M.-D.; Chen, C.; Colakoglu, S.; Curtis, M.S.; Tobias, A.M.; Lee, B.T. Tissue oximetry monitoring in microsurgical breast reconstruction decreases flap loss and improves rate of flap salvage. Plast. Reconstr. Surg. 2011, 127, 1080–1085. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, A.; Tseng, C.; Agarwal, S.; Park, J.; Song, D. Cost analysis of near-infrared spectroscopy tissue oximetry for monitoring autologous free tissue breast reconstruction. J. Reconstr. Microsurg. 2011, 27, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Ricci, J.A.; Vargas, C.R.; Ho, O.A.; Lin, S.J.; Tobias, A.M.; Lee, B.T. Evaluating the use of tissue oximetry to decrease intensive unit monitoring for free flap breast reconstruction. Ann. Plast. Surg. 2017, 79, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Salgarello, M.; Pagliara, D.; Rossi, M.; Visconti, G.; Barone-Adesi, L. Postoperative monitoring of free DIEP flap in breast reconstruction with near-infrared spectroscopy: Variables affecting the regional oxygen saturation. J. Reconstr. Microsurg. 2018, 34, 383–388. [Google Scholar] [CrossRef]
- Steele, M.H. Three-year experience using near infrared spectroscopy tissue oximetry monitoring of free tissue transfers. Ann. Plast. Surg. 2011, 66, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, I.S.; Pratt, G.F.; Rozen, W.M.; Cairns, S.A.; Barrett, M.D.; Hiew, L.Y.; Cooper, M.A.; Leaper, D.J. Near infrared spectroscopy for monitoring flap viability following breast reconstruction. J. Reconstr. 2012, 28, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Schulz, T.; Marotz, J.; Stukenberg, A.; Reumuth, G.; Houschyar, K.S.; Siemers, F. Hyperspectral imaging for postoperative flap monitoring of pedicled flaps. Handchir. Mikrochir. Plast. Chir. Organ. Der Dtsch. Arb. Fur Handchir.:Organ. Der Dtsch. Arb. Fur Mikrochir. Der Peripher. Nerven Und Gefasse Organ. Der V. 2020, 52, 316–324. [Google Scholar]
- Schulz, T.; Leuschner, S.; Siemers, F.; Marotz, J.; Houschyar, K.; Corterier, C.C. Assessing flap perfusion after free tissue transfer using hyperspectral imaging (HSI). Eur. J. Plast. Surg. 2021, 1–10. [Google Scholar] [CrossRef]
- Keller, A. Noninvasive tissue oximetry. Clin. Plast. Surg. 2011, 38, 313–324. [Google Scholar] [CrossRef]
- Thiem, D.G.; Römer, P.; Blatt, S.; Al-Nawas, B.; Kämmerer, P.W. New Approach to the Old Challenge of Free Flap Monitoring—Hyperspectral Imaging Outperforms Clinical Assessment by Earlier Detection of Perfusion Failure. J. Pers. Med. 2021, 11, 1101. [Google Scholar] [CrossRef]
- Yoshitani, K.; Kawaguchi, M.; Tatsumi, K.; Kitaguchi, K.; Furuya, H. A comparison of the INVOS 4100 and the NIRO 300 near-infrared spectrophotometers. Anesth. Analg. 2002, 94, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Bevan, P.J. Should cerebral near-infrared spectroscopy be standard of care in adult cardiac surgery? Heart Lung Circ. 2015, 24, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Hyttel-Sorensen, S.; Hessel, T.W.; Greisen, G. Peripheral tissue oximetry: Comparing three commercial near-infrared spectroscopy oximeters on the forearm. J. Clin. Monit. Comput. 2014, 28, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Jafari-Saraf, L.; Wilson, S.E.; Gordon, I.L. Hyperspectral image measurements of skin hemoglobin compared with transcutaneous PO2 measurements. Ann. Vasc. Surg. 2012, 26, 537–548. [Google Scholar] [CrossRef]
- Ricci, J.A.; Vargas, C.R.; Lin, S.J.; Tobias, A.M.; Taghinia, A.H.; Lee, B.T. A novel free flap monitoring system using tissue oximetry with text message alerts. J. Reconstr. Microsurg. 2016, 32, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Lindelauf, A.A.; Vranken, N.P.; Rutjens, V.G.; Schols, R.M.; Heijmans, J.H.; Weerwind, P.W.; van der Hulst, R.R. Economic Analysis of Noninvasive Tissue Oximetry for Postoperative Monitoring of Deep Inferior Epigastric Perforator Flap Breast Reconstruction: A Review. Surg. Innov. 2020, 27, 534–542. [Google Scholar] [CrossRef]


| Category | MeSH Term | Free Search Term |
|---|---|---|
| #1: Population | Surgical flaps, or mastectomy, or perforator flap | Free flap OR Free tissue flap OR Surgical flaps OR Mastectomy OR Free tissue transfer flaps OR Perforator flap OR Mastectomy skin flap OR Mastectomy flap |
| #2: Intervention | Spectroscopy, near infrared, or hyperspectral imaging, or spectroscopies | Near infrared spectroscopy OR Noninvasive flap monitoring OR Flap monitoring OR Nirs OR Hyperspectral imaging OR Hsi OR Tissue oximetry OR Tivita tissue system OR Tivita OR Near infrared spectroscopies OR Near infrared spectrometry OR Near infrared spectrometries OR Spectrometries, near infrared OR Nir spectroscopies OR Nir spectroscopy |
| #3: Comparators | Venous insufficiency, or surgical wound dehiscence | Flap loss OR Partial flap loss OR Ischemia OR Necrosis OR Venous congestion OR Venous insufficiency OR Post operative complication OR surgical wound dehiscence |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindelauf, A.A.M.A.; Saelmans, A.G.; van Kuijk, S.M.J.; van der Hulst, R.R.W.J.; Schols, R.M. Near-Infrared Spectroscopy (NIRS) versus Hyperspectral Imaging (HSI) to Detect Flap Failure in Reconstructive Surgery: A Systematic Review. Life 2022, 12, 65. https://doi.org/10.3390/life12010065
Lindelauf AAMA, Saelmans AG, van Kuijk SMJ, van der Hulst RRWJ, Schols RM. Near-Infrared Spectroscopy (NIRS) versus Hyperspectral Imaging (HSI) to Detect Flap Failure in Reconstructive Surgery: A Systematic Review. Life. 2022; 12(1):65. https://doi.org/10.3390/life12010065
Chicago/Turabian StyleLindelauf, Anouk A. M. A., Alexander G. Saelmans, Sander M. J. van Kuijk, René R. W. J. van der Hulst, and Rutger M. Schols. 2022. "Near-Infrared Spectroscopy (NIRS) versus Hyperspectral Imaging (HSI) to Detect Flap Failure in Reconstructive Surgery: A Systematic Review" Life 12, no. 1: 65. https://doi.org/10.3390/life12010065