
Lipoprotein Abnormalities in Chronic Kidney Disease and Renal Transplantation

 , , and
, , and
Abstract
:1. Introduction
2. Chronic Renal Failure (CRF)
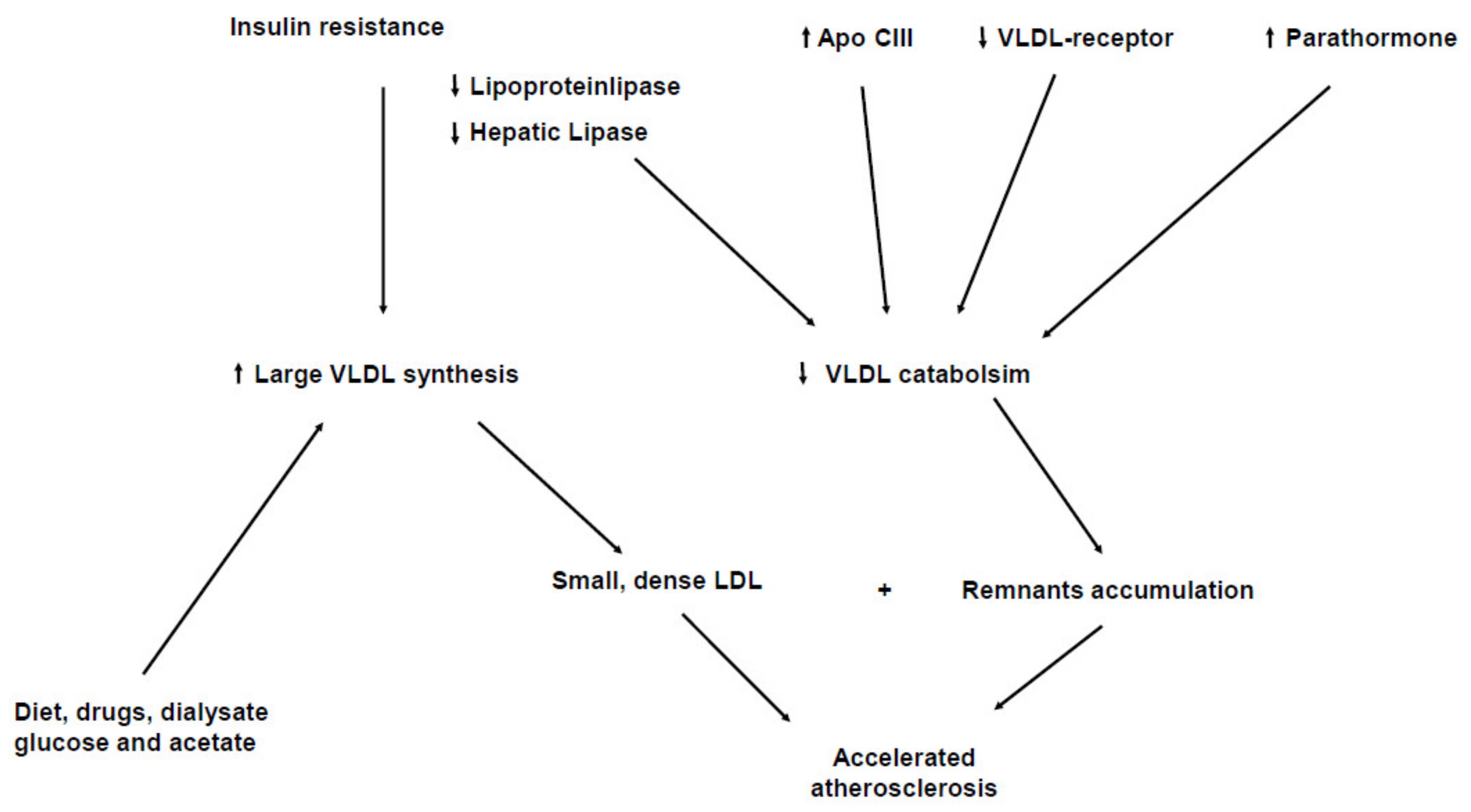
2.1. Triglyceride Rich Lipoprotein (TRL) Particles and CKD
2.2. Other Lipoprotein Abnormalities and CKD
2.3. Lipid Abnormalities in CKD Patients on Hemodialysis and Peritoneal Dialysis
3. Nephrotic Syndrome
4. Renal Transplantation
5. Hypolipidemic Treatments and CKD
6. Lipoprotein Abnormalities and Progression of CKD
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovas-cular events, and hospitalization. New Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Drüeke, T.B.; Massy, Z.A. Atherosclerosis in CKD: Differences from the general population. Nat. Rev. Nephrol. 2010, 6, 723–735. [Google Scholar] [CrossRef]
- Kwan, B.C.H.; Kronenberg, F.; Beddhu, S.; Cheung, A.K. Lipoprotein Metabolism and Lipid Management in Chronic Kidney Disease. J. Am. Soc. Nephrol. 2007, 18, 1246–1261. [Google Scholar] [CrossRef]
- Speer, T.; Zewinger, S.; Fliser, D. Uraemic dyslipidaemia revisited: Role of high-density lipoprotein. Nephrol. Dial. Transplant. 2013, 28, 2456–2463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, N.D. Dyslipidemia of chronic renal failure: The nature, mechanisms, and potential consequences. Am. J. Physiol. Physiol. 2006, 290, F262–F272. [Google Scholar] [CrossRef] [PubMed]
- Quaschning, T.; Krane, V.; Metzger, T.; Wanner, C. Abnormalities in uremic lipoprotein metabolism and its impact on cardiovascular disease. Am. J. Kidney Dis. 2001, 38, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Attman, P.O.; Alaupovic, P.; Tavella, M.; Knight-Gibson, C. Abnormal lipid and apolipoprotein composition of ma-jor lipoprotein density classes in patients with chronic renal failure. Nephrol. Dial. Transplant 1996, 11, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Deighan, C.J.; Caslake, M.J.; McConnell, M.; Boulton-Jones, J.; Packard, C.J. Atherogenic lipoprotein phenotype in end-stage renal failure: Origin and extent of small dense low-density lipoprotein formation. Am. J. Kidney Dis. 2000, 35, 852–862. [Google Scholar] [CrossRef]
- Hopewell, J.C.; Haynes, R.; Baigent, C. The role of lipoprotein (a) in chronic kidney disease. J. Lipid Res. 2018, 59, 577–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, S.; Devaraj, S.; Jialal, I. Accelerated atherosclerosis, dyslipidemia, and oxidative stress in end-stage renal disease. Curr. Opin. Nephrol. Hypertens. 2002, 11, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Quaschning, T. Dyslipidemia and renal disease: Pathogenesis and clinical consequences. Curr. Opin. Nephrol. Hypertens. 2001, 10, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, J.; Varela, A.; Medina, J.L. Dyslipidemia in renal disease: Causes, consequences and treatment. Endocrinol. Nutr. 2010, 57, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Averna, M.R.; Sparacino, V.; Galione, A.; Caputo, F.; Scafidi, V.; Amato, S.; Mancino, C.; Cefalù, A.B.; Notarbartolo, A. Lipoprotein (a) levels in end-stage renal failure and renal transplantation. Nephron 1993, 64, 560–564. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Moradi, H. Mechanisms of dyslipidemia of chronic renal failure. Hemodial. Int. 2006, 10, 1–7. [Google Scholar] [CrossRef]
- Lacquaniti, A.; Bolignano, D.; Donato, V.; Bono, C.; Fazio, M.R.; Buemi, M. Alterations of Lipid Metabolism in Chronic Nephropathies: Mechanisms, Diagnosis and Treatment. Kidney Blood Press. Res. 2010, 33, 100–110. [Google Scholar] [CrossRef]
- Chan, M.K.; Persaud, J.; Varghese, Z.; Moorhead, J.F. Pathogenic roles of post-heparin lipases in lipid abnormalities in hemodialysis patients. Kidney Int. 1984, 25, 812–818. [Google Scholar] [CrossRef] [Green Version]
- Keane, W.F.; Tomassini, J.E.; Neff, D.R. Lipid Abnormalities in Patients with Chronic Kidney Disease: Implications for the Pathophysiology of Atherosclerosis. J. Atheroscler. Thromb. 2013, 20, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, N.D. Causes of Dysregulation of Lipid Metabolism in Chronic Renal Failure. Semin. Dial. 2009, 22, 644–651. [Google Scholar] [CrossRef]
- Mahley, R.W.; Innerarity, T.L.; Rall, S.C., Jr.; Weisgraber, K.H. Plasma lipoproteins: Apolipoprotein structure and function. J. Lipid Res. 1984, 25, 1277–1294. [Google Scholar] [CrossRef]
- Beigneux, A.P.; Davies, B.; Gin, P.; Weinstein, M.M.; Farber, E.; Qiao, X.; Peale, F.; Bunting, S.; Walzem, R.L.; Wong, J.S.; et al. Glyco-sylphosphatidylinositol-anchored binding protein-1plays a critical role in the lipolytic processing of chylomicrons. Cell Metab. 2007, 5, 279–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dallinga-Thie, G.M.; Franssen, R.; Mooij, H.L.; Visser, M.E.; Hassing, H.C.; Peelman, F.; Kastelein, J.J.; Péterfy, M.; Nieuwdorp, M. The metabolism of triglyceride-rich lipoproteins revisited: New players, new insight. Atherosclerosis 2010, 211, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.S.; Marcoux, C.; Davignon, J. Detection, Quantification, and Characterization of Potentially Atherogenic Triglyceride-Rich Remnant Lipoproteins. Arter. Thromb. Vasc. Biol. 1999, 19, 2474–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordestgaard, B.G.; Tybjaerg-Hansen, A. IDL, VLDL, chylomicrons and atherosclerosis. Eur. J. Epidemiol. 1992, 8, 92–98. [Google Scholar] [CrossRef]
- Barbagallo, C.M.; Rizzo, M.; Noto, D.; Frasheri, A.; Pernice, V.; Rubino, A.; Pieri, D.; Pinto, V.; Cefalù, A.B.; Giordano, C.; et al. Accumulation of ApoE-enriched triglyceride-rich lipoproteins in patients with coro-nary artery disease. Metabolism 2006, 55, 662–668. [Google Scholar] [CrossRef]
- Reaven, G.M. Compensatory Hyperinsulinemia and the Development of an Atherogenic Lipoprotein Profile: The Price Paid to Maintain Glucose Homeostasis in Insulin-Resistant Individuals. Endocrinol. Metab. Clin. N. Am. 2005, 34, 49–62. [Google Scholar] [CrossRef]
- Samouilidou, E.C.; Karpouza, A.P.; Kostopoulos, V.; Bakirtzi, T.; Pantelias, K.; Petras, D.; Tzanatou-Exarchou, H.; Grapsa, E.J. Lipid abnormalities and oxidized LDL in chronic kidney disease patients on hemodialysis and peritoneal dialy-sis. Ren. Fail. 2012, 34, 724–727. [Google Scholar] [CrossRef] [Green Version]
- Stegmayr, B.; Olivecrona, T.; Olivecrona, G. Lipoprotein Lipase Disturbances Induced by Uremia and Hemodialysis. Semin. Dial. 2009, 22, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Huttunen, J.K.; Pasternack, A.; Vänttinen, T.; Ehnholm, C.; A Nikkilä, E. Lipoprotein metabolism in patients with chronic uremia. Effect of hemodialysis on serum lipoproteins and postheparin plasma triglyceride lipases. Acta Medica Scand. 1978, 204, 211–218. [Google Scholar] [CrossRef]
- Liang, K.; Oveisi, F.; Vaziri, N.D. Role of secondary hyperparathyroidism in the genesis of hypertriglyceridemia and VLDL receptor deficiency in chronic renal failure. Kidney Int. 1998, 53, 626–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, N.D.; Liang, K. Down-regulation of tissue lipoprotein lipase expression in experimental chronic renal failure. Kidney Int. 1996, 50, 1928–1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Näsström, B.; Stegmayr, B.; Gupta, J.; Olivecrona, G.; Olivecrona, T. A single bolus of a low molecular weight hepa-rin to patients on haemodialysis depletes lipoprotein lipase stores and retards triglyceride clearing. Nephrol. Dial. Transplant. 2005, 20, 1172–1179. [Google Scholar] [CrossRef] [Green Version]
- Cheung, A.K.; Parker, C.J.; Ren, K.; Iverius, P.H. Increased lipase inhibition in uremia: Identification of pre-beta-HDL as a major inhibitor in normal and uremic plasma. Kidney Int. 1996, 49, 1360–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Averna, M.R.; Barbagallo, C.M.; Galione, A.; Carroccio, A.; Labisi, M.; Marino, G.; Montalto, G.; Notarbartolo, A. Serum apolipoprotein profile of hypertriglyceridemic patients with chronic renal failure on hemodialysis: A comparison with type IV hyperlipoproteinemic patients. Metabolism 1989, 38, 601–602. [Google Scholar] [CrossRef]
- Ooi, E.M.; Chan, D.T.; Watts, G.F.; Chan, D.C.; Ng, T.W.; Dogra, G.K.; Irish, A.B.; Barrett, P.H.R. Plasma apolipoprotein C-III metabolism in patients with chronic kidney disease. J. Lipid Res. 2011, 52, 794–800. [Google Scholar] [CrossRef] [Green Version]
- Arnadottir, M.; Dallongeville, J.; Fruchart, J.C.; Nilsson-Ehle, P. Very-low-density lipoprotein of uremic patients is a poor substrate for bovine lipoprotein lipase in vitro. Metabolism 1996, 45, 686–690. [Google Scholar] [CrossRef]
- Chan, D.T.; Dogra, G.K.; Irish, A.B.; Ooi, E.M.; Barrett, P.H.; Chan, D.C.; Watts, G.F. Chronic kidney disease delays VLDL-apoB-100 particle catabolism: Potential role of apolipoprotein C-III. J. Lipid. Res. 2009, 50, 2524–2531. [Google Scholar] [CrossRef] [Green Version]
- Dautin, G.; Soltani, Z.; Ducloux, D.; Gautier, T.; De Barros, J.P.; Gambert, P.; Lagrost, L.; Masson, D. Hemodialysis reduces plasma apolipoprotein C-I concentration making VLDL a better substrate for lipoprotein lipase. Kidney Int. 2007, 72, 871–878. [Google Scholar] [CrossRef]
- Ikewaki, K.; Schaefer, J.R.; Frischmann, M.E.; Okubo, K.; Hosoya, T.; Mochizuki, S.; Dieplinger, B.; Trenkwalder, E.; Schweer, H.; Kronenberg, F.; et al. Delayed in vivo catabolism of intermediate-density lipoprotein and low-density lipoprotein in hemodialysis patients as potential cause of premature atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2615–2622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nguyen, S.; Nakamura, T.; Uematsu, M.; Fujioka, D.; Watanabe, K.; Watanabe, Y.; Obata, J.-E.; Nakamura, K.; Kugiyama, K. Remnant lipoproteinemia predicts cardiovascular events in patients with type 2 diabetes and chronic kidney disease. J. Cardiol. 2017, 69, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Vaziri, N.D.; Hoong, K.M.; Osratola, V.D. Aziri Down-regulation of hepatic LDL receptor-related protein (LRP) in chronic renal failure. Kidney Int. 2005, 67, 1028–1032. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Astor, B.C.; Stevens, L.A.; Coresh, J. Chronic kidney disease, diabetes, and hypertension: What’s in a name? Kidney Int. 2010, 78, 19–22. [Google Scholar] [CrossRef] [Green Version]
- Vega, G.-L.; Grundy, S.M. Effect of Statins on Metabolism of Apo-B–Containing Lipoproteins in Hypertriglyceridemic Men. Am. J. Cardiol. 1998, 81, 36B–42B. [Google Scholar] [CrossRef]
- Shurraw, S.; Tonelli, M. Statins for treatment of dyslipidemia in chronic kidney disease. Perit. Dial. Int. 2006, 26, 523–539. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.; Wang, A.Y.M.; Chan, I.H.S.; Chui, S.H.; Lam, C.W.K. Serum small-dense LDL abnormalities in chronic renal disease patients. Br. J. Biomed. Sci. 2012, 69, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Berneis, K.K.; Krauss, R.M. Metabolic origins and clinical significance of LDL heterogeneity. J. Lipid Res. 2002, 43, 1363–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbagallo, C.; Averna, M.; Scafidi, V.; Galione, A.; Notarbartolo, A. Increased Lipoprotein (a) Levels in Subjects with Chronic Renal Failure on Hemodialysis. Nephron 1992, 62, 471–472. [Google Scholar] [CrossRef]
- Bajaj, A.; Damrauer, S.M.; Anderson, A.H.; Xie, D.; Budoff, M.J.; Go, A.S.; He, J.; Lash, J.P.; Ojo, A.; Post, W.S.; et al. Chronic Renal Insufficiency Cohort Study I. Lipoprotein(a) and Risk of Myocardial Infarction and Death in Chronic Kidney Disease: Findings from the CRIC Study (Chronic Renal Insufficiency Cohort). Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1971–1978. [Google Scholar] [CrossRef] [Green Version]
- Nordestgaard, B.G.; Langsted, A. Lipoprotein (a) as a cause of cardiovascular disease: Insights from epidemiolo-gy, genetics, and biology. J. Lipid Res. 2016, 57, 1953–1975. [Google Scholar] [CrossRef] [Green Version]
- Frischmann, M.E.; Kronenberg, F.; Trenkwalder, E.; Schaefer, J.R.; Schweer, H.; Dieplinger, B.; Koenig, P.; Ikewaki, K.; Dieplinger, H. In vivo turnover study demonstrates diminished clearance of lipoprotein(a) in hemodialysis patients. Kidney Int. 2007, 71, 1036–1043. [Google Scholar] [CrossRef] [Green Version]
- Morena, M.; Le May, C.; Chenine, L.; Arnaud, L.; Dupuy, A.M.; Pichelin, M.; Leray-Moragues, H.; Chalabi, L.; Canaud, B.; Cristol, J.P.; et al. Plasma PCSK9 concentrations during the course of nondiabetic chronic kidney disease: Rela-tionship with glomerular filtration rate and lipid metabolism. J. Clin. Lipidol. 2017, 11, 87–93. [Google Scholar] [CrossRef]
- Kronenberg, F. HDL in CKD—The Devil Is in the Detail. J. Am. Soc. Nephrol. 2018, 29, 1356–1371. [Google Scholar] [CrossRef] [PubMed]
- Silbernagel, G.; Genser, B.; Drechsler, C.; Scharnagl, H.; Grammer, T.B.; Stojakovic, T.; Krane, V.; Ritz, E.; Wanner, C.; März, W. HDL Cholesterol, Apolipoproteins, and Cardiovascular Risk in Hemodialysis Patients. J. Am. Soc. Nephrol. 2014, 26, 484–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, N.D.; Liang, K.; Parks, J.S. Down-regulation of hepatic lecithin: Cholesterolacyltransferase gene expression in chronic renal failure. Kidney Int. 2001, 59, 2192–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolasevic, I.; Žutelija, M.; Mavrinac, V.; Orlic, L. Dyslipidemia in patients with chronic kidney disease: Etiology and management. Int. J. Nephrol. Renov. Dis. 2017, 10, 35–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Himmelfarb, J. Relevance of Oxidative Pathways in the Pathophysiology of Chronic Kidney Disease. Cardiol. Clin. 2005, 23, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Huang, J.C.; Wu, P.Y.; Chen, S.C.; Chiu, Y.W.; Chang, J.M.; Chen, H.C. Greater low-density lipoprotein cholester-ol variability is associated with increased progression to dialysis in patients with chronic kidney disease stage. Oncotarget 2018, 9, 3242–3253. [Google Scholar] [CrossRef] [PubMed]
- Ambrosch, A.; Domroese, U.; Westphal, S.; Dierkes, J.; Augustin, W.; Neumann, K.H.; Luley, C. Compositional and functional changes of low-density lipoprotein during hemodialysis in patients with ESRD11This work is dedicated to Professor Dr. Dietrich Seidel, Klinikum Groβhadern, University of Munich, on the occasion of his 60th birthday. Kidney Int. 1998, 54, 608–617. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Krane, V.; Metzger, T.; Quaschning, T. Lipid changes and statins in chronic renal insufficiency and di-alysis. J. Nephrol. 2001, 14, S76–S80. [Google Scholar]
- Attman, P.-O.; Samuelsson, O.; Johansson, A.-C.; Moberly, J.B.; Alaupovic, P. Dialysis modalities and dyslipidemia. Kidney Int. 2003, 63, S110–S112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrader, J.; Andersson, L.O.; Armstrong, V.W.; Kundt, M.; Stibbe, W.; Scheler, F. Lipolytic effects of heparin and low molecular weight heparin and their importance in hemodialysis. Semin. Thromb. Hemost. 1990, 16, 41–45. [Google Scholar] [PubMed]
- Näsström, B.; Olivecrona, G.; Olivecrona, T.; Stegmayr, B.G. Lipoprotein lipase during continuous heparin infusion: Tissue stores become partially depleted. J. Lab. Clin. Med. 2001, 138, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Näsström, B.; Olivecrona, G.; Olivecrona, T.; Stegmayr, B.G. Lipoprotein lipase during heparin infusion: Lower ac-tivity in hemodialysis patients. Scand. J. Clin. Lab. Investig. 2003, 63, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Noto, D.; Cefalu’, A.B.; Ganci, A.; Giammarresi, C.; Panno, D.; Cusumano, G.; Greco, M.; Di Gaudio, F.; Averna, M.R. Heparin induces an accumulation of atherogenic lipoproteins during hemodialysis in normolipidemic end-stage renal disease patients. Hemodial. Int. 2014, 19, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Ng, D. Heparin in hypertriglyceridemia: Friend or foe? J. Lab. Clin. Med. 2001, 138, 356–358. [Google Scholar] [CrossRef]
- O’Neal, D.; Lee, P.; Murphy, B.; Best, J. Low-density lipoprotein particle size distribution in end-stage renal disease treated with hemodialysis or peritoneal dialysis. Am. J. Kidney Dis. 1996, 27, 84–91. [Google Scholar] [CrossRef]
- Krediet, R.T.; Balafa, O. Cardiovascular risk in the peritoneal dialysis patient. Nat. Rev. Nephrol. 2010, 6, 451–460. [Google Scholar] [CrossRef]
- Fortes, P.C.; De Moraes, T.P.; Mendes, J.G.; Stinghen, A.E.; Ribeiro, S.C.; Pecoits-Filho, R. Insulin resistance and glucose homeostasis in peritoneal dialysis. Perit. Dial. Int. 2009, 29, 145–148. [Google Scholar] [CrossRef]
- Harmankaya, O.; Akalin, N.; Akay, H.; Okuturlar, Y.; Erturk, K.; Kaptanogullari, H.; Kocoglu, H. Comparison of risk factors for cardiovascular disease in hemodialysis and peritoneal dialysis patients. Clinics 2015, 70, 601–605. [Google Scholar] [CrossRef]
- Zamiah, S.A.K.S.; Draman, C.R.; Seman, M.R.; Safhan, A.F.; Rozalina, R.; Ruzni, N.I.N. The cardiovascular risk factor pro-files among end-stage renal failure patients treated with continuos ambulatory peritoneal dialysis and intermittent emodialysis. Saudi J. Kidney Dis. Transpl. 2018, 29, 114–119. [Google Scholar]
- Tonbul, Z.; Altintepe, L.; Sozlu, C.; Yeksan, M.; Yildiz, A.; Türk, S. Ambulatory blood pressure monitoring in haemo-dialysisand coninuos ambulatori peritoneal dialisi (CAPD) patients. J. Hum. Hypertens. 2002, 16, 585–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.W.; Yang, C.Y.; Wu, H.Y.; Liu, K.L.; Su, C.T.; Wu, C.K.; Lee, J.K.; Chiang, C.K.; Cheng, H.T.; Lien, Y.C.; et al. Metabolic syndrome and abdominal fat are associated with inflammation, but not with clinical outcomes, in peritoneal dialysis patients. Cardiovasc. Diabetol. 2013, 12, 86. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, F.M.; Yilmaz, G.; Duranay, M.; Parpucu, H.; Senes, M.; Tekeli, N.; Yücel, D. Cardiovascular risk factors in he-modialysis and peritoneal dialysis patients. Scan. J. Clin. Lab. Invest. 2005, 65, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, F. Dyslipidemia and nephrotic syndrome: Recent avances. J. Renal Nutr. 2005, 15, 195–203. [Google Scholar] [CrossRef]
- Vaziri, N.D. Disorders of lipid metabolism in nephrotic syndrome: Mechanisms and consequences. Kidney Int. 2016, 90, 41–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warwick, G.L.; Packard, C.J.; Demant, T.; Bedford, D.K.; Boulton-Jones, J.M.; Shepherd, J. Metabolism of apolipoprotein B-containing lipoproteins in subjects with nephrotic-range proteinuria. Kidney Int. 1991, 40, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Warwick, G.L.; Caslake, M.J.; Boulton-Jones, J.M.; Dagen, M.; Packard, C.J.; Shepherd, J. Low-density lipoprotein me-tabolism in the nephrotic syndrome. Metabolism 1990, 39, 187–192. [Google Scholar] [CrossRef]
- Liu, S.; Vaziri, N.D. Role of PCSK9 and IDOL in the pathogenesis of acquired LDL receptor deficiency and hy-percholesterolemia in nephritic syndrome. Nephrol. Dial. Transplant. 2014, 29, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, N.D.; Liang, K.H. Hepatic HMG-CoA reductase gene expression during the course of puromycin-induced nephrosis. Kidney Int. 1995, 48, 1979–1985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, N.D.; Yuan, J.; Ni, Z.; Nicholas, S.B.; Norris, K.C. Lipoprotein lipase deficiency in chronic kidney disease is compounded by downregulation of endothelial GPIHBP1 expression. Clin. Exp. Nephrol. 2012, 16, 238–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clement, L.C.; Macè, C.; Avila-Casado, C.; Joles, J.A.; Kersten, S.; Chugh, S.S. Circulating angiopoietin-like 4 links pro-teinuria with hypertrigliceridemia in nephrotic syndrome. Nat. Med. 2014, 20, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, K.; Vaziri, N.D. Down-regulation of hepatic lipase expression in experimental nephrotic syndrome. Kidney Int. 1997, 51, 1933–1937. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Liang, K.; Vaziri, N.D. Protein restriction and AST-120 improve lipoprotein lipase, hepatic lipase and VLDL receptor in focal glomerulosclerosis. Kidney Int. 2003, 64, 1780–1786. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, N.D. HDL abnormalities in nephrotic syndrome and chronic kidney disease. Nat. Rev. Nephrol. 2015, 12, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Kronenberg, F.; Utermann, G.; Dieplinger, H. Lipoprotein(a) in renal disease. Am. J. Kidney Dis. 1996, 27, 1–25. [Google Scholar] [CrossRef]
- Noto, D.; Barbagallo, C.M.; Cascio, A.L.; Cefalu’, A.B.; Cavera, G.; Caldarella, R.; Marino, G.; Travali, S.; Cutaia, I.; Maringhini, S.; et al. Lipoprotein(a) levels in relation to albumin concentration in childhood nephrotic syndrome. Kidney Int. 1999, 55, 2433–2439. [Google Scholar] [CrossRef] [Green Version]
- Cassader, M.; Ruiu, G.; Gambino, R.; Alemanno, N.; Triolo, G.; Pagano, G. Lipoprotein-apolipoprotein changes in renal transplant recipients: A 2-year follow-up. Metabolism 1991, 40, 922–925. [Google Scholar] [CrossRef]
- Chan, M.K.; Varghese, Z.; Persaud, J.W.; Fernando, O.N.; Moorhead, J.F. The role of multiple pharmaco-therapy in the pathogenesis of hyperlipidemia after renal transplantation. Clin. Nephrol. 1981, 15, 309–313. [Google Scholar]
- Moore, R.A.; Callahan, M.F.; Cody, M.; Adams, P.L.; Litchford, M.; Buckner, K.; Galloway, J. The Eeffect of the American Heart Association Step One Diet on Hyperlipidemia Following Renal Transplantation. Transplantation 1990, 49, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, W.H.; Bender, W.L.; Goldberg, A.P.; Hazzard, W.R. Lipoprotein lipid abnormalities in healthy renal trans-plant recipients: Persistence of low HDL2 cholesterol. Nephron 1987, 47, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Averna, M.R.; Sparacino, V.; Cefalù, A.B.; Caputo, F.; Noto, D.; Verghi, F.; Notarbartolo, A. HDL sub-fractions distribution in renal transplant recipients: Lack of evidence of a reduction of HDL2 particles. Nephron 1996, 72, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Cefalù, A.B.; Gallo, S.; Rizzo, M.; Noto, D.; Cavera, G.; Rao Camemi, A.; Marino, G.; Caldarella, R.; Notarbartolo, A.; et al. Effects of Mediterranean diet on lipid levels and cardiovascular risk in renal trans-plant recipients. Nephron 1999, 82, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Yu, M.Y.; Kim, Y.C.; Min, S.I.; Ha, J.; Lee, J.P.; Kim, D.K.; Oh, K.H.; Joo, K.W.; Ahn, C.; et al. Ratio of triglyc-eride to high-density lipoprotein cholesterol and risk of major cardiovascular events in kidney transplant recipients. Clin. Exp. Nephrol. 2019, 23, 1407–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fellstrom, B.C.; Jardine, A.G.; Schmieder, R.E.; Holdaas, H.; Bannister, K.; Beutler, J.; Chae, D.-W.; Chevaile, A.; Cobbe, S.M.; Grönhagen-Riska, C.; et al. Rosuvastatin and Cardiovascular Events in Patients Undergoing Hemodialysis. N. Engl. J. Med. 2009, 360, 1395–1407. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Krane, V.; Marz, W.; Olschewski, M.; Mann, J.F.; Ruf, G.; Ritz, E.; German, D.; German Diabetes and Dialysis Study Investigators. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N. Engl. J. Med. 2005, 353, 238–248. [Google Scholar] [CrossRef]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo controlledtrial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef] [Green Version]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Herrington, W.G.; Emberson, J.; Mihaylova, B.; Blackwell, L.; Reith, C.; Solbu, M.D.; Mark, P.B.; Fellström, B.; Jardine, A.G.; et al. Impact of renal function on the effects of LDL cholesterol lowering with statin-based regimens: A meta-analysis of individual participant data from 28 randomised trials. Lancet Diabetes Endocrinol. 2016, 4, 829–839. [Google Scholar]
- Ferro, C.J.; Mark, P.B.; Kanbay, M.; Sarafidis, P.; Heine, G.H.; Rossignol, P.; Massy, Z.A.; Mallamaci, F.; Valdivielso, J.M.; Malyszko, J.; et al. Lipid management in patients with chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 727–749. [Google Scholar] [CrossRef] [Green Version]
- Sarnak, M.J.; Bloom, R.; Muntner, P.; Rahman, M.; Saland, J.M.; Wilson, P.W.; Fried, L. KDOQI US Commentary on the 2013 KDIGO Clinical Practice Guideline for Lipid Management in CKD. Am. J. Kidney Dis. 2015, 65, 354–366. [Google Scholar] [CrossRef] [Green Version]
- Bulbul, M.C.; Dagel, T.; Afsar, B.; Ulusu, N.N.; Kuwabara, M.; Covic, A.; Kanbay, M. Disorders of Lipid Metabolism in Chronic Kidney Disease. Blood Purif. 2018, 46, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Schmit, D.; Fliser, D.; Speer, T. Proprotein convertase subtilisin/kexin type 9 in kidney disease. Nephrol. Dial. Transplant. 2019, 34, 1266–1271. [Google Scholar] [CrossRef]
- Charytan, D.M.; Sabatine, M.S.; Pedersen, T.R.; Im, K.; Park, J.-G.; Pineda, A.L.; Wasserman, S.M.; Deedwania, P.; Olsson, A.G.; Sever, P.S.; et al. Efficacy and Safety of Evolocumab in Chronic Kidney Disease in the FOURIER Trial. J. Am. Coll. Cardiol. 2019, 73, 2961–2970. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Zaritsky, J.J.; Fornoni, A.; Smoyer, W.E. Dyslipidemia in nephrotic syndrome: Mechanisms and treat-ment. Nat. Rev. Nephrol. 2018, 14, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Gyebi, L.; Soltani, Z.; Reisin, E. Lipid nephrotoxicity: New concept fora n old disease. Curr. Hypertens. Rep. 2012, 14, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D.; Sato, T.; Liang, K. Molecular mechanisms of altered cholesterol metabolism in rats with spontaneous focal glomerulosclerosis. Kidney Int. 2003, 63, 1756–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keane, W.F.; Mulcahy, W.S.; Kasiske, B.L.; Kim, Y.; O’Donnell, M.P. Hyperlipidemia and progressive renal disease. Kidney Int Suppl. 1991, 31, S41–S48. [Google Scholar]
- Kasiske, B.L.; O’Donnell, M.P.; Cleary, M.P.; Keane, W.F. Treatment of hyperlipidemia reduces glomerular injury in obese Zucker rats. Kidney Int. 1988, 33, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, A.; Inui, K.; Nemoto, T.; Uda, S.; Sugenoya, Y.; Watanabe, S.; Yokota, N.; Taira, T.; Iwasaki, S.; Ideura, T. Simvastatin suppresses glomerular cell proliferation and macrophage infiltration in rats with mesangial prolifera-tive nephritis. J. Am. Soc. Nephrol. 1998, 9, 2027–2039. [Google Scholar]
- Mänttäri, M.; Tiula, E.; Alikoski, T.; Manninen, V. Effects of Hypertension and Dyslipidemia on the Decline in Renal Function. Hypertension 1995, 26, 670–675. [Google Scholar] [CrossRef]
- Muntner, P.; Coresh, J.; Smith, J.C.; Eckfeldt, J.; Klag, M.J. Plasma lipids and risk of developing renal dysfunction: The Atherosclerosis Risk in Communities Study. Kidney Int. 2000, 58, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Schaeffner, E.S.; Kurth, T.; Curhan, G.C.; Glynn, R.J.; Rexrode, K.M.; Baigent, C.; Buring, J.E.; Gaziano, J.M. Cholesterol and the risk of renal dysfunction in apparently healthy men. J. Am. Soc. Nephrol. 2003, 14, 2084–2091. [Google Scholar]
- Haynes, R.; Lewis, D.; Emberson, J.; Reith, C.; Agodoa, L.; Cass, A.; Craig, J.C.; De Zeeuw, D.; Feldt-Rasmussen, B.; Fellström, B.; et al. Effects of Lowering LDL Cholesterol on Progression of Kidney Disease. J. Am. Soc. Nephrol. 2014, 25, 1825–1833. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.; Yang, W.; Akkina, S.; Alper, A.; Anderson, A.H.; Appel, L.J.; He, J.; Raj, D.S.; Schelling, J.; Strauss, L.; et al. Relation of Serum Lipids and Lipoproteins with Progression of CKD: The CRIC Study. Clin. J. Am. Soc. Nephrol. 2014, 9, 1190–1198. [Google Scholar] [CrossRef] [Green Version]
- Sanguankeo, A.; Upala, S.; Cheungpasitporn, W.; Ungprasert, P.; Knight, E.L. Effects of Statins on Renal Outcome in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0132970. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Zhang, L.; Lv, J.; Wang, J.; Hou, W.; Xie, X.; Zhang, H. Effect of Statins on Kidney Disease Outcomes: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2016, 67, 881–892. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| ↑ Triglycerides |
| ↑ TG-rich particles |
| = to ↑ LDL-cholesterol |
| ↓ HDL-cholesterol |
| ↑ Non HDL-cholesterol |
| ↑ Small, dense LDL |
| ↑ Remnants |
| ↑ Lipoprotein(a) |
| ↑ Modified LDL |
| ↑ Apo CIII (in VLDL) |
| ↓ Apo AI/AII |
| ↓ LPL |
| ↓ HL |
| ↓ L-CAT |
| ↑ CETP |
| = PCSK9 |
| ↓ Paraoxonase |
| Lipoproteins | Nephrotic Syndrome | Non-Nephrotic CKD | Diabetic CKD | HD | CAPD | Kidney Transplantation |
|---|---|---|---|---|---|---|
| TC | ↑↑ | ↓ | ↑ | ↑↑ | ↑↑ | ↑↑ |
| HDL-C | Normal or ↓ | ↓ | ↓ | ↓↓ | ↓↓ | Normal or ↑↑ |
| LDL-C | ↑↑ | ↓ | ↑ | ↑↑ | ||
| Triglycerides | ↑↑ | ↑↑ | ↑↑ | ↑↑ | ↑↑ | ↓↓ |
| VLDL | ↑↑ | ↑↑ | ↑↑ | ↑↑ | ↑↑ | ↓↓ |
| Chylomicrons | ↑↑ | ↑↑ | ↑↑ | ↑↑ | ↑↑ | ↓↓ |
| IDL | ↑↑ | ↑↑ | ↑ | ↑ | ↑ | ↓↓ |
| Lipoprotein(a) | ↑↑ | ↑↑ | ↑ | ↑ | ↑ | ↑ |
| ApoB | ↑↑ | ↑↑ | ↑ | ↑↑ | ↑↑ | ↑↑ |
| Apo-A1 | Normal or ↓ | ↓ | ↓ | ↓↓ | ↓↓ | ↑↑ |
| Trial | Population | No. Patients | Drug | Follow-Up (Years) | Ldl Reduction % | Cv Event Reduction % | p Value |
|---|---|---|---|---|---|---|---|
| SHARP | CKD patients | 9270 | Simvastatin 20 mg/ ezetimibe | 4.9 | 55% | 17% | 0.0021 |
| 4D | Hemodialysis | 1255 | Atorvastatin 20 mg | 4 | 42% | - | 0.35 |
| AURORA | Hemodialysis | 2776 | Rosuvastatin 10 mg | 3.8 | 43% | - | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbagallo, C.M.; Cefalù, A.B.; Giammanco, A.; Noto, D.; Caldarella, R.; Ciaccio, M.; Averna, M.R.; Nardi, E. Lipoprotein Abnormalities in Chronic Kidney Disease and Renal Transplantation. Life 2021, 11, 315. https://doi.org/10.3390/life11040315
Barbagallo CM, Cefalù AB, Giammanco A, Noto D, Caldarella R, Ciaccio M, Averna MR, Nardi E. Lipoprotein Abnormalities in Chronic Kidney Disease and Renal Transplantation. Life. 2021; 11(4):315. https://doi.org/10.3390/life11040315
Chicago/Turabian StyleBarbagallo, Carlo Maria, Angelo Baldassare Cefalù, Antonina Giammanco, Davide Noto, Rosalia Caldarella, Marcello Ciaccio, Maurizio Rocco Averna, and Emilio Nardi. 2021. "Lipoprotein Abnormalities in Chronic Kidney Disease and Renal Transplantation" Life 11, no. 4: 315. https://doi.org/10.3390/life11040315