
Uncovering the Roles of MicroRNAs in Major Depressive Disorder: From Candidate Diagnostic Biomarkers to Treatment Response Indicators

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
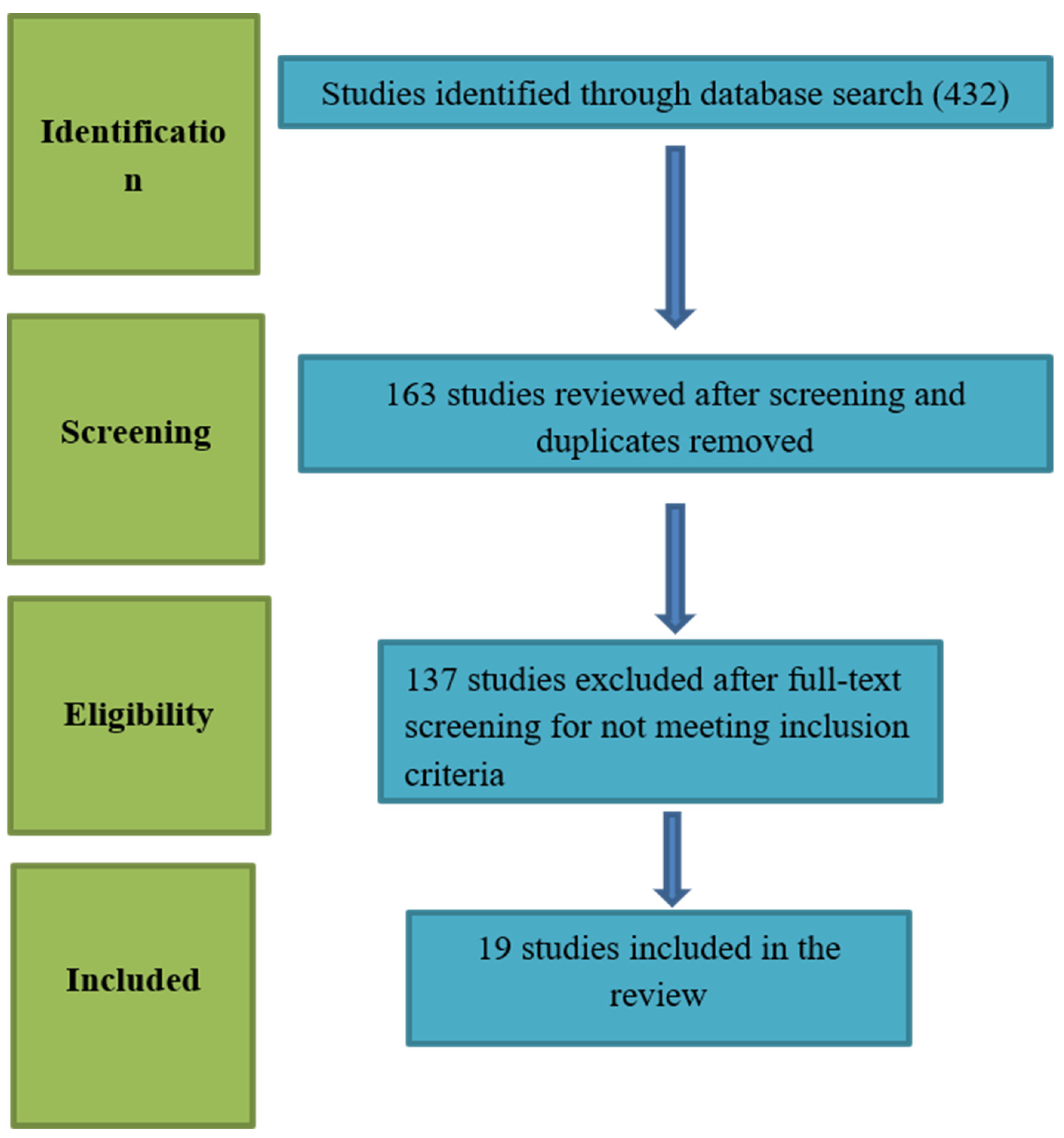
2.1. Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Characteristics of the Included Studies
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weissman, M.M.; Bland, R.C.; Canino, G.J.; Faravelli, C.; Greenwald, S.; Hwu, H.G.; Joyce, P.R.; Karam, E.G.; Lee, C.K.; Lellouch, J.; et al. Cross-national epidemiology of major depression and bipolar disorder. JAMA 1996, 276, 293–299. [Google Scholar] [CrossRef]
- Friedrich, M.J. Depression Is the Leading Cause of Disability Around the World. JAMA 2017, 317, 1517. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [Green Version]
- Fava, M. Definition and epidemiology of treatment-resistant depression. Psychiatr. Clin. N. Am. 1996, 19, 179–200. [Google Scholar] [CrossRef]
- Hashimoto, K. Metabolomics of Major Depressive Disorder and Bipolar Disorder: Overview and Future Perspective. Adv. Clin. Chem. 2018, 84, 81–99. [Google Scholar]
- Singh, T. Misdiagnosis of bipolar disorder. Psychiatry (Edgmont) 2006, 3, 57–63. [Google Scholar] [PubMed]
- Zajecka, J.M. Treating depression to remission. J. Clin. Psychiatry 2003, 64, 7–12. [Google Scholar] [PubMed]
- Schmidt, H.D.; Shelton, R.C. Functional biomarkers of depression: Diagnosis, treatment, and pathophysiology. Neuropsychopharmacology 2011, 36, 2375–2394. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Kitamura, T.; Okano, T.; Tomita, T.; Kikuchi, A. Structured Clinical Interview for DSM-IV Axis I Disorders Version 2.0; Nippon Hyouron Sha: Tokyo, Japan, 2003. [Google Scholar]
- Andreasen, N.C. Linking mind and brain in the study of mental illnesses: A project for a scientific psychopathology. Science 1997, 275, 1586–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honer, W.G. Assessing the machinery of mind: Synapses in neuropsychiatric disorders. J. Psychiatry Neurosci. 1999, 24, 116–121. [Google Scholar] [PubMed]
- Anand, A.; Li, Y.; Wang, Y.; Wu, J.W.; Gao, S.J.; Bukhari, L.; Mathews, V.P.; Kalnin, A.; Lowe, M.J. Activity and connectivity of brain mood regulating circuit in depression: A functional magnetic resonance study. Biol. Psychiatry 2005, 57, 1079–1088. [Google Scholar] [CrossRef]
- Toni, N.; Buchs, P.A.; Nikonenko, I.; Bron, C.R.; Muller, D. LTP promotes formation of multiple spine synapses between a single axon terminal and a dendrite. Nature 1999, 402, 421–425. [Google Scholar] [CrossRef]
- Hajsza, T.; MacLusky, N.J.; Leranth, C. Short-term treatment with the antidepressant fluoxetine triggers pyramidal dendritic spine synapse formation in rat hippocampus. Eur. J. Neurosci. 2005, 21, 1299–1303. [Google Scholar] [CrossRef]
- McEwen, B.S. Effects of adverse experiences for brain structure and function. Biol. Psychiatry 2000, 48, 721–731. [Google Scholar] [CrossRef]
- Sheline, Y.I. 3D MRI studies of neuroanatomic changes in unipolar major depression: The role of stress and medical comorbidity. Biol. Psychiatry 2000, 48, 791–800. [Google Scholar] [CrossRef]
- Sala, M.; Perez, J.; Soloff, P.; Ucelli di Nemi, S.; Caverzasi, E.; Soaresd, J.C.; Brambillab, P. Stress and hippocampal abnormalities in psychiatric disorders. Eur. Neuropsychopharmacol. 2004, 14, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Rajkowska, G.; Miguel-Hidalgo, J.J. Gliogenesis and glial pathology in depression. CNS Neurol. Disord.-Drug Targets 2007, 6, 219–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bushati, N.; Cohen, S.M. microRNA functions. Annu. Rev. Cell Dev. Biol. 2007, 23, 175–205. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Target recognition and regulatory functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef] [Green Version]
- Malphettes, L.; Fussenegger, M. Impact of RNA interference on gene networks. Metab. Eng. 2006, 8, 672–683. [Google Scholar] [CrossRef]
- Li, M.; Marin-Muller, C.; Bharadwaj, U.; Chow, K.W.; Yao, Q.Z.; Chen, C.Y. MicroRNAs: Control and loss of control in human physiology and disease. World J. Surg. 2009, 33, 667–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Qin, L.; Tang, B. MicroRNAs in Alzheimer’s Disease. Front. Genet. 2019, 10, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, K.; Guo, C.; He, L.; Shi, Y. MiRNAs of peripheral blood as the biomarker of schizophrenia. Hereditas 2017, 155, 9. [Google Scholar] [CrossRef]
- Goh, S.Y.; Chao, Y.X.; Dheen, S.T.; Tan, E.K.; Tay, S.S.W. Role of MicroRNAs in Parkinson’s Disease. Int. J. Mol. Sci. 2019, 20, 5649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwivedi, Y. Emerging role of microRNAs in major depressive disorder: Diagnosis and therapeutic implications. Dialogues Clin. Neurosci. 2014, 16, 43–61. [Google Scholar]
- Serafini, G.; Pompili, M.; Innamorati, M.; Giordano, G.; Montebovi, F.; Sher, L.; Dwivedi, Y.; Girardi, P. The role of microRNAs in synaptic plasticity, major affective disorders and suicidal behavior. Neurosci. Res. 2012, 73, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Saavedra, K.; Molina-Márquez, A.M.; Saavedra, N.; Zambrano, T.; Salazar, L.A. Epigenetic modifications of major depressive disorder. Int. J. Mol. Sci. 2016, 17, 1279. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.X.; Rothenberg, M.E. MicroRNA. J. Allergy Clin. Immunol. 2018, 141, 1202–1207. [Google Scholar] [CrossRef] [Green Version]
- Enatescu, V.R.; Papava, I.; Enatescu, I.; Antonescu, M.; Anghel, A.; Seclaman, E.; Sirbu, I.O.; Marian, C. Circulating Plasma Miro RNAs in Patients with Major Deppresive Disorder Treated with Antidepressants: A Pilot Study. Psychiatry Investig. 2016, 13, 549–557. [Google Scholar] [CrossRef] [Green Version]
- Dwivedi, Y. microRNAs as Biomarker in Depression Pathogenesis. Ann. Psychiatry Ment. Health 2013, 1, 1003. [Google Scholar]
- Belzeaux, R.; Bergon, A.; Jeanjean, V.; Loriod, B.; Formisano-Tréziny, C.; Verrier, L.; Loundou, A.; Baumstarck-Barrau, K.; Boyer, L.; Gall, V.; et al. Responder and nonresponder patients exhibit different peripheral transcriptional signatures during major depressive episode. Transl. Psychiatry 2012, 2, e185. [Google Scholar] [CrossRef]
- Li, Y.J.; Xu, M.; Gao, Z.H.; Wang, Y.Q.; Yue, Z.; Zhang, Y.X.; Li, X.X.; Zhang, C.; Xie, S.Y.; Wang, P.Y. Alterations of serum levels of BDNF-related miRNAs in patients with depression. PLoS ONE 2013, 8, e63648. [Google Scholar] [CrossRef] [Green Version]
- Fan, H.M.; Sun, X.Y.; Guo, W.; Zhong, A.F.; Niu, W.; Zhao, L.; Dai, Y.H.; Guo, Z.M.; Zhang, L.Y.; Lu, J. Differential expression of microRNA in peripheral blood mononuclear cells as specific biomarker for major depressive disorder patients. J. Psychiatr. Res. 2014, 59, 45–52. [Google Scholar] [CrossRef]
- Li, J.; Meng, H.; Cao, W.; Qiu, T. MiR-335 is involved in major depression disorder and antidepressant treatment through targeting GRM4. Neurosci. Lett. 2015, 606, 167–172. [Google Scholar] [CrossRef]
- Camkurt, M.A.; Acar, S.; Coskun, S.; Güneş, M.; Güneş, S.; Yılmaz, M.F.; Görür, A.; Tamer, L. Comparison of plasma MicroRNA levels in drug naive, first episode depressed patients and healthy controls. J. Psychiatr. Res. 2015, 69, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Liu, Y.; Wang, X.; Wu, J.L.; Liu, K.Z.; Zhou, J.; Liu, L.; Zhang, C.H. Identification of differential microRNAs in cerebrospinal fluid and serum of patients with major depressive disorder. PLoS ONE 2015, 10, e0121975. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Sundquist, K.; Hedelius, A.; Palmér, K.; Memon, A.A.; Sundquist, J. Circulating microRNA-144-5p is associated with depressive disorders. Clinical. Epigenet. 2015, 7, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffioletti, E.; Cattaneo, A.; Rosso, G.; Maina, G.; Maj, C.; Gennarellia, M.; Tardito, D.; Bocchio-Chiavetto, L. Peripheral whole blood microRNA alterations in major depression and bipolar disorder. J. Affect. Disord. 2016, 200, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Sun, N.; Lei, L.; Wang, Y.; Yang, C.X.; Liu, Z.F.; Li, X.R.; Zhang, K. Preliminary comparison of plasma notch-associated microRNA-34b and -34c levels in drug naive, first episode depressed patients and healthy controls. J. Affect. Disord. 2016, 194, 109–114. [Google Scholar] [CrossRef]
- He, S.; Liu, X.; Jiang, K.; Peng, D.H.; Hong, W.; Fang, Y.R.; Qian, Y.P.; Yu, S.Y.; Li, H.F. Alterations of microRNA-124 expression in peripheral blood mononuclear cells in pre- and post-treatment patients with major depressive disorder. J. Psychiatr. Res. 2016, 78, 65–71. [Google Scholar] [CrossRef]
- Roy, B.; Dunbar, M.; Shelton, R.; Dwivedi, Y. Identification of MicroRNA-124-3p as a Putative Epigenetic Signature of Major Depressive Disorder. Neuropsychopharmacol 2017, 42, 864–875. [Google Scholar] [CrossRef] [Green Version]
- Kuang, W.H.; Dong, Z.Q.; Tian, L.T.; Li, J. MicroRNA-451a, microRNA-34a-5p, and microRNA-221-3p as predictors of response to antidepressant treatment. Braz. J. Med. Biol. Res. 2018, 51, e7212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.; Qiu, Q.; Zhang, S.; Sun, L.; Li, G.J.; Xiao, S.F.; Lia, X. Changes in miRNA-132 and miR-124 levels in non-treated and citalopram-treated patients with depression. J. Affect. Disord. 2018, 227, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Gheysarzadeh, A.; Sadeghifard, N.; Afraidooni, L.; Pooyan, F.; Mofid, M.R.; Valadbeigi, H.; Bakhtiari, H.; Keikhavani, S. Serum-based microRNA biomarkers for major depression: MiR-16, miR-135a, and miR-1202. J. Res. Med. Sci. 2018, 23, 69. [Google Scholar] [CrossRef] [PubMed]
- Hung, Y.Y.; Wu, M.K.; Tsai, M.C.; Huang, Y.L.; Kang, H.Y. Aberrant Expression of Intracellular let-7e, miR-146a, and miR-155 Correlates with Severity of Depression in Patients with Major Depressive Disorder and Is Ameliorated after Antidepressant Treatment. Cells 2019, 8, 647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocchio-Chiavetto, L.; Maffioletti, E.; Bettinsoli, P.; Giovannini, C.; Bignotti, S.; Tardito, D.; Corrada, D.; Milanesi, L.; Gennarellie, M. Blood microRNA changes in depressed patients during antidepressant treatment. Eur. Neuropsychopharmacol. 2013, 23, 602–611. [Google Scholar] [CrossRef]
- Zhang, Q.L.; Lu, J.; Sun, X.Y.; Guo, W.; Zhao, L.; Fan, H.M.; Zhong, A.F.; Niu, W.; Dai, Y.H.; Zhang, L.Y.; et al. A preliminary analysis of association between plasma microRNA expression alteration and symptomatology improvement in Major Depressive Disorder (MDD) patients before and after antidepressant treatment. Eur. J. Psychiatry 2014, 28, 252–264. [Google Scholar]
- Lopez, J.P.; Fiori, L.M.; Cruceanu, C.; Lin, R.; Labonte, B.; Cates, H.M.; Heller, A.E.; Vialou, V.; Ku, S.M.; Gerald, C.; et al. MicroRNAs 146a/b-5 and 425-3p and 24-3p are markers of antidepressant response and regulate MAPK/Wnt-system genes. Nat. Commun. 2017, 8, 15497. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.C.; Tsai, M.C.; Lee, C.T.; Sun, M.H.; Huang, T.L. Antidepressant treatment increased serum miR-183 and miR-212 levels in patients with major depressive disorder. Psychiatry Res. 2018, 270, 232–237. [Google Scholar] [CrossRef]
- Scott, H.L.; Tamagnini, F.; Narduzzo, K.E.; Howarth, J.L.; Lee, Y.B.; Wong, L.F.; Brown, M.W.; Warburton, E.C.; Bashir, Z.I.; Uney, J.B. MicroRNA-132 regulates recognition memory and synaptic plasticity in the perirhinal cortex. Eur. J. Neurosci. 2012, 36, 2941–2948. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, S.; Scott, H.; Glover, C.; Bienemann, A.; Ghorbel, M.T.; Uney, J.; Brown, M.W.; Warburton, E.C.; Bashir, Z.I. Expression of long-term depression underlies visual recognition memory. Neuron 2008, 58, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Li, S.; Yan, J.; Wang, D.Q.; Yin, R.G.; Zhao, L.; Zhu, Y.; Zhu, X.L. miR-182 (microRNA-182) suppression in the hippocampus evokes antidepressant-like effects in rats. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 65, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Mu, R.H.; Li, C.F.; Dong, S.Q.; Geng, D.; Liu, Q.; Yi, L.T. microRNA-124 targets glucocorticoid receptor and is involved in depression-like behaviors. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 79, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, Y. microRNA-124: A putative therapeutic target and biomarker for major depression. Expert Opin. Ther. Targets 2017, 21, 653–656. [Google Scholar] [CrossRef] [Green Version]
- Launay, J.M.; Mouillet-Richard, S.; Baudry, A.; Pietri, M.; Kellermann, O. Raphe-mediated signals control the hippocampal response to SRI antidepressants via miR-16. Transl. Psychiatry 2011, 1, e56. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Study (Year, Reference No) | Patients | Controls | Blood Compartment | Upregulated miRs | Downregulated miRs | Unchanged miRs | Total |
|---|---|---|---|---|---|---|---|
| Belzeaux et al., 2012 [32] | 16 | 13 | PBMCs | miR-107 miR-133a miR-148a miR-425-3p miR-494 miR-579 miR-652 miR-941 miR-589 | miR-200c miR-381 miR-571 miR-636 miR-1243 | - | 9 upregulated, 5 downregulated |
| Li YJ et al., 2013 [33] | 40 | 40 | Serum | miR-132 miR-182 | - | - | 2 upregulated |
| Fan et al., 2014 [34] | 81 | 46 | PBMCs | miR-26b miR-1972 miR-4485 miR-4498 miR-4743 | - | - | 5 upregulated |
| Li J et al., 2015 [35] | 18 | 18 | Whole blood | miR-644 miR-450b miR-328 miR-182 | miR-335 miR-583 miR-708a miR-650 miR-654a | miR-541 miR-663 miR-578 | 4 upregulated, 5 downregulated, 3 unchanged |
| Camkurt et al., 2015 [36] | 50 | 41 | Plasma | miR-451a miR-17-5p miR-223-3p | miR-320a | miR-25-3p miR-126-3p miR-16-5p miR-93-5p | 3 upregulated, 1 downregulated, 4 unchanged |
| Wan et al., 2015 [37] | 38 | 27 | Serum | let-7d-3p miR-34a-5p miR-221-3p miR-125a-5p miR-30a-5p miR-29b-3p miR-10a-5p miR-375 miR-155–5p miR-33a-5p miR-139–5p | miR-451a miR-15b-5p miR-106-5p miR-590-5p miR-185-5p | - | 11 upregulated, 5 downregulated |
| Wang X et al., 2015 [38] | 169 | 52 | Plasma | - | miR-144-5p | - | 1 downregulated |
| Mafioletti et al., 2016 [39] | 20 | 20 | Peripheral venous blood | hsa-miR-199a-5p hsa-miR-24-3p hsa-miR-425-3p hsa-miR-29c-5p hsa-miR-330-3p hsamiR-345-5p | hsa-let-7a-5p hsa-let-7d-5p has-let-7f-5p has-miR-1915-3p | hsa-miR-720 hsa-miR-140-3p hsa-miR-1973 hsa-miR-30d-5p hsa-miR-3158-3p hsa-miR-330-5p hsa-miR-378a-5p hsa-miR-1915-5p hsa-miR-1972 hsa-miR-21-3p hsa-miR-4521 hsa-miR-4793-3p hsa-miR-4440 | 6 upregulated, 4 downregulated, 13 unchanged |
| Sun et al., 2016 [40] | 32 | 32 | Peripheral blood leukocytes | miR-34b-5p miR-34c-5p | - | miR-369–3p miR-381 miR-107 | 2 upregulated, 3 unchanged |
| He et al., 2016 [41] | 32 | 30 | PBMCs | miR-124 | - | - | 1 upregulated |
| Roy et al., 2017 [42] | 18 | 17 | Serum | miR-124-3p | - | - | 1 upregulated |
| Kuang et al., 2018 [43] | 84 | 78 | Serum | miR-34a-5p miR-221-3p | miR-451a | - | 2 upregulated, 1 downregulated |
| Fang Y et al., 2018 [44] | 45 | 32 | Plasma | miR-124 miR-132 | - | - | 2 upregulated |
| Gheysarzadeh et al., 2018 [45] | 39 | 36 | Serum | - | miR-16 miR-135a miR-1202 | - | 3 downregulated |
| Hung et al., 2019 [46] | 84 | 43 | PBMCs | miR-21-5p miR-145 miR-223 | miR-146a miR-155 let-7e | - | 3 upregulated, 3 downregulated |
| Upregulated miRs | Downregulated miRs |
|---|---|
| miR-107 | miR-200c |
| miR-133a | miR-381 |
| miR-148a | miR-571 |
| miR-425-3p | miR-636 |
| miR-494 | miR-1243 |
| miR-579 | hsa-let-7f-5p |
| miR-652 | hsa-miR-1285-5p |
| miR-941 | hsa-miR-107 |
| miR-589 | hsa-miR-26a-5p |
| hsa-miR-5010-3p | hsa-miR-26b-5p |
| hsa-miR-151a-3p | brain-miR-161 |
| miR-132 | brain-miR-112 |
| miR-182 | hsa-let-7d-3p |
| miR-26b | hsa-miR-103a-3p |
| miR-1972 | hsa-miR-532-5p |
| miR-4485 | miR-335 |
| miR-4498 | miR-583 |
| miR-4743 | miR-708a |
| miR-644 | miR-650 |
| miR-450b | miR-320a |
| miR-328 | miR-15b-5p |
| miR-451a | miR-106-5p |
| miR-17-5p | miR-590-5p |
| let-7d-3p | miR-185-5p |
| miR-223-3p | miR-144-5p |
| miR-34a-5p | hsa-let-7a-5p |
| miR-221-3p | hsa-let-7d-5p |
| miR-125a-5p | has-let-7f-5p |
| miR-30a-5p | has-miR-1915-3p |
| miR-29b-3p | miR-451a |
| hsa-miR-199a-5p | miR-16 |
| hsa-miR-24-3p | miR-135a |
| hsa-miR-425-3p | miR-1202 |
| hsa-miR-29c-5p | miR-146a |
| hsa-miR-330-3p | miR-155 |
| miR-10a-5p | let-7e |
| miR-375 | |
| hsamiR-345-5p | |
| miR-155–5p | |
| miR-33a-5p | |
| miR-139–5p | |
| miR-34b-5p | |
| miR-34c-5p | |
| miR-124 | |
| miR-124-3p | |
| miR-34a-5p | |
| miR-221-3p | |
| miR-21-5p | |
| miR-145 | |
| miR-223 |
| Study | Patients | AD Treatment and Duration | Blood Compartment | Upregulated miRs | Downregulated miR | Unchanged miRs | Total |
|---|---|---|---|---|---|---|---|
| Enatescu et al., 2016 [30] | 5 | Escitalopram 12 weeks | Plasma | miR-1193 miR-3173-3p miR-3154 miR-129-5p miR-3661 miR-1287 miR-532-3p miR-2278 miR-3150a-3p miR-3909 miR-937 miR-676 miR-489 miR-637 miR-608 miR-4263 miR-382 miR-3691-5p miR-375 miR-433 miR-1298 miR-1909 miR-1471 | miR-99b miR-151-5p miR-223 miR-181b miR-26a miR-744 miR-301b miR-27a miR-24 miR-146a- miR-146b-5p miR-126 miR-151-3p let-7d miR-221 miR-125a-5p miR-652 | - | 23 upregulated, 17 downregulated |
| Li J et al., 2015 [35] | 18 | Citalopram, 1 week | Whole blood | miR-335 | - | - | 1 upregulated |
| Wang X et al., 2015 [38] | 169 | Not mentioned, 8 weeks | Plasma | miR-144-5p miR-30a-5p | - | - | 2 upregulated |
| He et al., 2016 [41] | 32 | Venlafaxine (N = 7), paroxetine (N = 7), fluoxetine (N = 3), escitalopram (N = 11), duloxetine (N = 1), sertraline (N = 3), mirtazapine (N = 2) | PBMCs | - | miR-124 | - | 1 downregulated |
| Kuang et al., 2018 [43] | 84 | Paroxetine 8 weeks | Serum | miR-34a-5p miR-221a-3p | miR-451a | - | 2 upregulated, 1 downregulated |
| Fang Y et al., 2018 [44] | 32 | Citalopram 8 weeks | Plasma | miR-124 | miR-132 | - | 1 upregulated, 1 downregulated |
| Hung YY et al., 2019 [46] | 84 | Not mentioned, 4 weeks | PBMCs | miR-146a miR-155 let-7e | - | - | 3 upregulated |
| Bocchio-Chiavetto et al., 2013 [47] | 10 | Escitalopram 10 weeks | Whole blood | miR-130b miR-505 miR-29b-2 miR-26b miR-22 miR-26a miR-64 miR-494 let-7d let-7g let-7e let-7f miR-629 miR-106b miR-103 miR-191 miR-128 miR-502-3p miR-374b miR-132 miR-30d miR-500 miR-589 miR-183 miR-574-3p miR-140-3p miR-335 miR-361-5p | miR-34c-5p miR-770-5p | - | 26 upregulated, 2 downregulated |
| Zhang et al., 2014 [48] | 20 | Venlafaxine, sertraline, mirtazapine 6 weeks | PBMCs | - | miR-1972 miR-4485 miR-4498 miR-4743 | miR-26b | 4 upregulated, 1 downregulated |
| Lopez et al., 2017 [49] | 23 | Escitalopram 8 weeks | Peripheral blood | miR-1202 | - | - | 1 upregulated |
| Lin CC et al., 2018 [50] | 33 | Not mentioned, 4 weeks | Whole blood | miR-16 miR-183 miR-212 | - | - | 3 upregulated |
| Common miRs in MDD (No Treatment and After ADT) | miRs of MDD Patients Before Antidepressant Treatment vs. Controls | miRs of MDD Patients After Antidepressant Treatment vs. Controls |
|---|---|---|
| let-7d | up, down | up, down |
| let-7e | down | up |
| let-7f | down | up |
| miR-16 | down | up |
| miR-24 | up | down |
| miR-26a | down | up, down |
| miR-26b | up | up |
| miR-29b | up | up |
| miR-30a-5p | up | up |
| miR-34a-5p | up | up |
| miR-34c-5p | up | down |
| miR-106b | down | up |
| miR-124 | up | up, down |
| miR-125a-5p | up | down |
| miR-132 | up | up, down |
| miR-144-5p | down | up |
| miR-146a-3p | down | up, down |
| miR-151-3p | up | down |
| miR-155 | up, down | up, down |
| miR-221 | up | up, down |
| miR-223 | up | down |
| miR-335 | down | up |
| miR-375 | up | up |
| miR-425-3p | up | down |
| miR-451a | up, down | down |
| miR-494 | up | up |
| miR-532 | down | up |
| miR-589 | up | up |
| miR-652 | up | down |
| miR-1202 | down | up |
| miR-1972 | down | down |
| miR-4485 | up | down |
| miR-4498 | up | down |
| miR-4743 | up | down |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Homorogan, C.; Nitusca, D.; Seclaman, E.; Enatescu, V.; Marian, C. Uncovering the Roles of MicroRNAs in Major Depressive Disorder: From Candidate Diagnostic Biomarkers to Treatment Response Indicators. Life 2021, 11, 1073. https://doi.org/10.3390/life11101073
Homorogan C, Nitusca D, Seclaman E, Enatescu V, Marian C. Uncovering the Roles of MicroRNAs in Major Depressive Disorder: From Candidate Diagnostic Biomarkers to Treatment Response Indicators. Life. 2021; 11(10):1073. https://doi.org/10.3390/life11101073
Chicago/Turabian StyleHomorogan, Claudia, Diana Nitusca, Edward Seclaman, Virgil Enatescu, and Catalin Marian. 2021. "Uncovering the Roles of MicroRNAs in Major Depressive Disorder: From Candidate Diagnostic Biomarkers to Treatment Response Indicators" Life 11, no. 10: 1073. https://doi.org/10.3390/life11101073