Effects of Electronic Health Record Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content

 , ,
, ,
Abstract
:1. Introduction
“Information relevant to the wellness, health and healthcare of an individual, in computer-processable form and represented according to a standardized information model, or the longitudinal electronic record of an individual that contains or virtually interlines to data in multiple EMRs and EPRs, which is to be shared and/or interoperable across healthcare settings and is patient-centric.”[5]
“…a representation of information regarding, or relevant to, the health, including wellness, development and welfare of that individual, which may be stand-alone or may integrate health information from multiple sources, and for which the individual, or the representative to whom the individual delegated his or her rights, manages and controls the PHR content and grants permissions for access by, and/or sharing with, other parties.”[6]
2. Materials and Methods
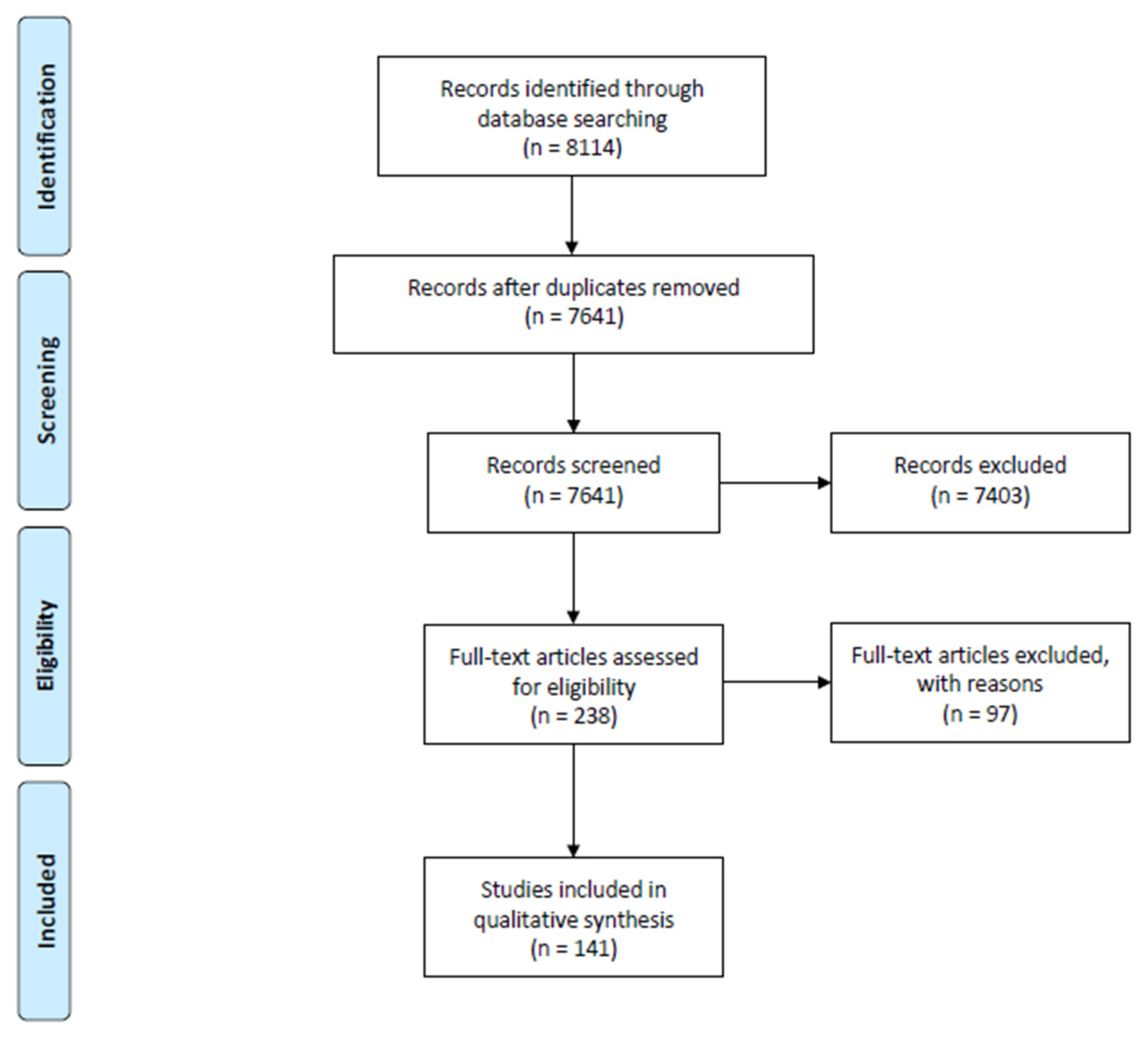
2.1. Study Retrieval
2.2. Study Selection
2.3. Data Analysis
3. Results
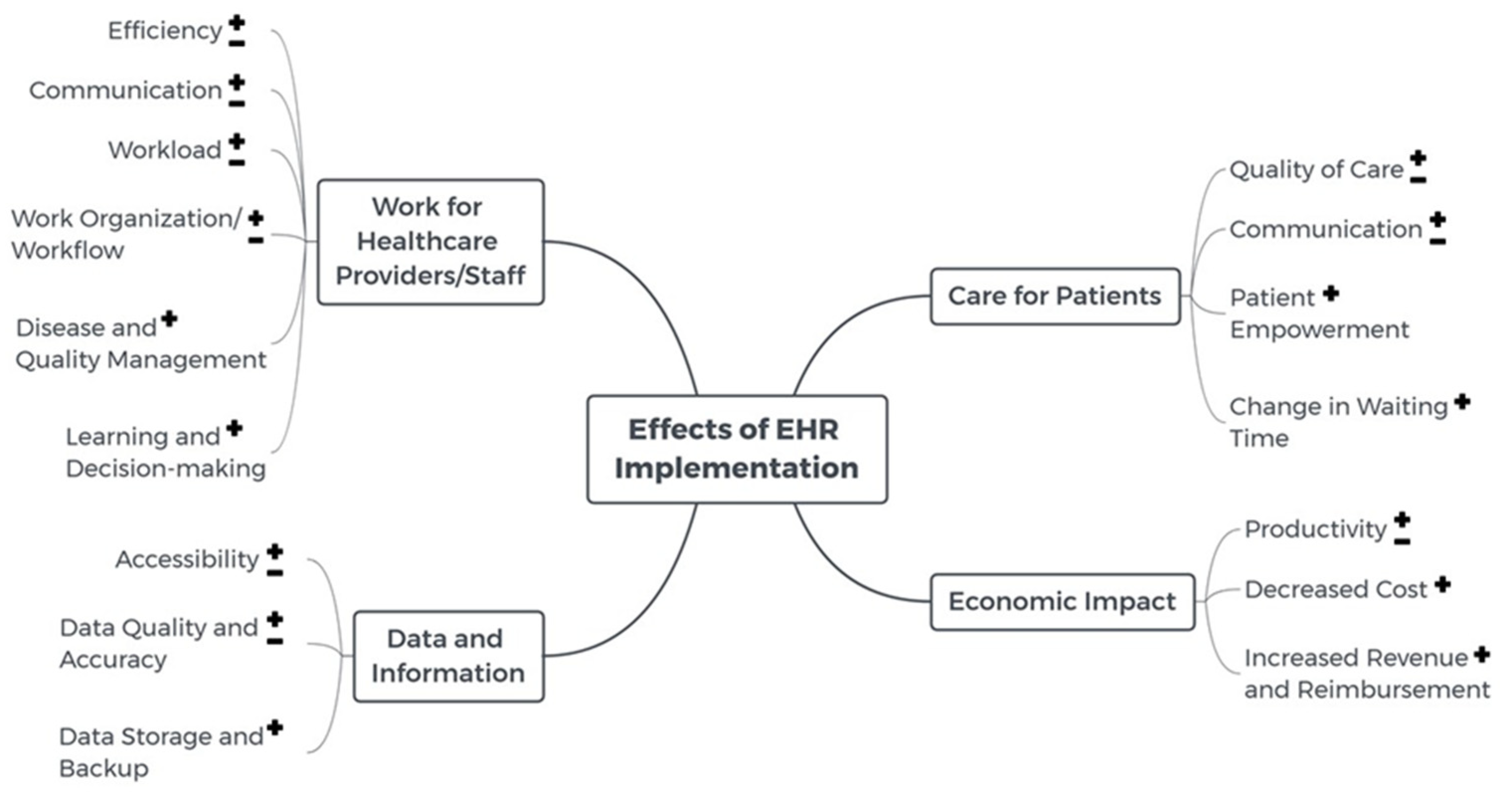
3.1. Effects of EHR Implementation
3.1.1. Work for Healthcare Providers/Staff
Efficiency
Communication
Workload
Work Organization/Workflow
Support Disease and Quality Management
Support Learning and Decision-Making
3.1.2. Data and Information
Accessibility
Data Quality and Accuracy
Data Storage and Backup
3.1.3. Care for Patients
Quality of Care
Communication
Patient Empowerment
Change in Time Spent
3.1.4. Economic Impact
Productivity
Decreased Cost
Increased Revenue and Reimbursement
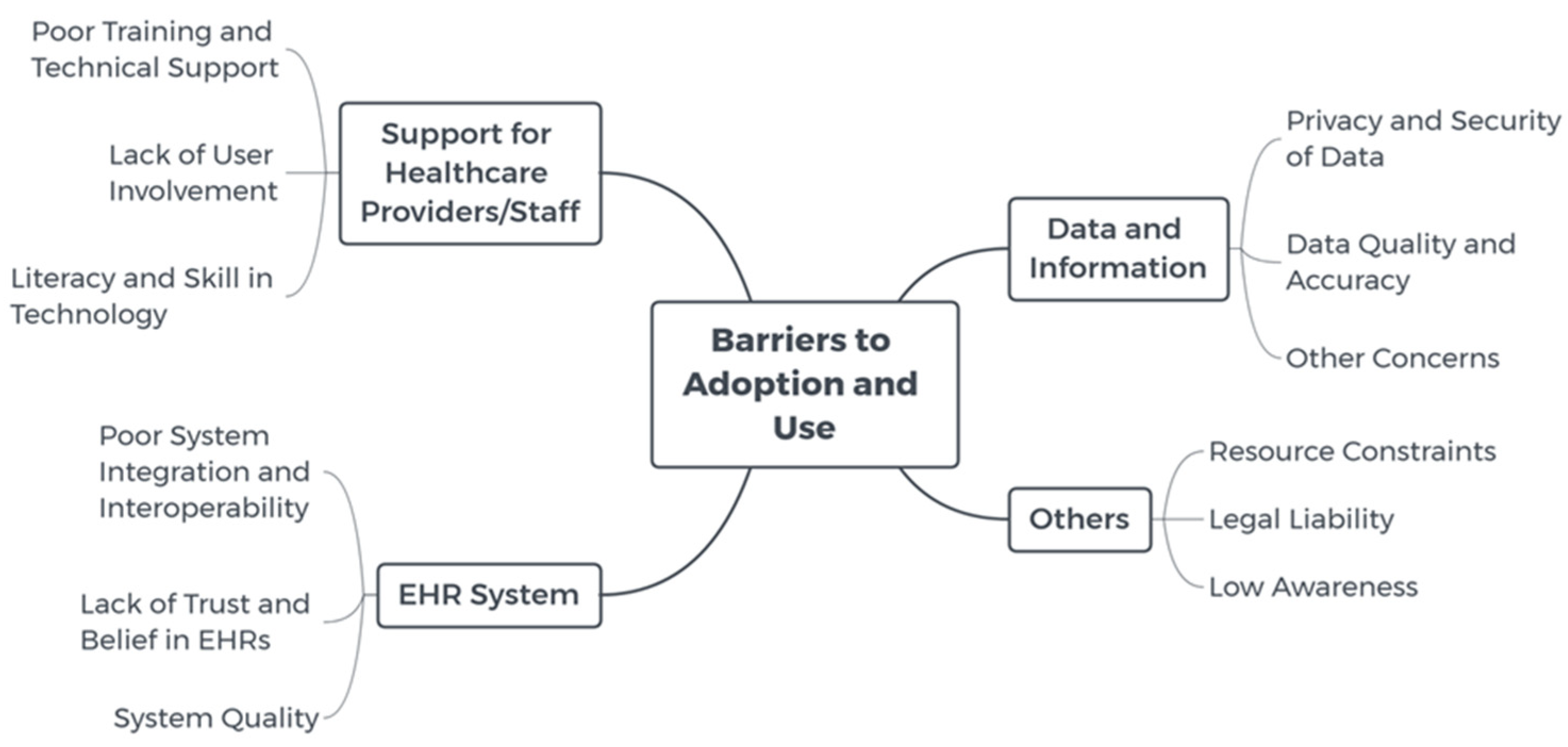
3.2. Barriers to Adoption and Use
3.2.1. Support for End Users
3.2.2. EHR/PHR System
3.2.3. Data and Information
3.2.4. Others
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Institute of Medicine—Committee on Improving the Patient Record. The Computer-Based Patient Record an Essential Technology for Health Care; Revised Edition; National Academy Press: Washington, DC, USA, 1997. [Google Scholar]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb. Med. Inform. 2016, 25, S48–S61. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, S.M.; Oates, R.B.; Fox, G.N. The computer-based medical record: Current status. J. Fam. Pract. 1992, 35, 556–565. [Google Scholar] [PubMed]
- Hoerbst, A.; Ammenwerth, E. Electronic health records. A systematic review on quality requirements. Methods Inf. Med. 2010, 49, 320–336. [Google Scholar] [PubMed]
- International Organization for Standardization. Health Informatics—Capacity-Based eHealth Architecture Roadmap—Part 1: Overview of National eHealth Initiatives; ISO: Geneva, Switzerland, 2012; Volume ISO/TR 14639-1:2012(en). [Google Scholar]
- International Organization for Standardization. Health Informatics—Personal Health Records—Definition, Scope and Context; ISO: Geneva, Switzerland, 2012; Volume ISO/TR 14292:2012(en). [Google Scholar]
- Burns, J. Product specification: The fifth discipline of health care. Manag. Care Q. 1993, 1, 29–33. [Google Scholar] [PubMed]
- Safran, C.; Bloomrosen, M.; Hammond, W.E.; Labkoff, S.; Markel-Fox, S.; Tang, P.C.; Detmer, D.E. Toward a National Framework for the Secondary Use of Health Data: An American Medical Informatics Association White Paper. J. Am. Med. Inform. Assoc. 2007, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Orfanidis, L.; Bamidis, P.D.; Eaglestone, B. Data Quality Issues in Electronic Health Records: An Adaptation Framework for the Greek Health System. Health Inform. J. 2004, 10, 23–36. [Google Scholar] [CrossRef]
- Voss, W.G. European Union Data Privacy Law Reform: General Data Protection Regulation, Privacy Shield, and the Right to Delisting. Bus. Lawyer 2016, 72, 221–233. [Google Scholar]
- Voss, W.G. Looking at European Union Data Protection Law Reform through a Different Prism: The Proposed EU General Data Protection Regulation Two Years Later. J. Internet Law 2014, 17, 12–24. [Google Scholar]
- McDonald, C.J.; Martin, D.K.; Overhage, J.M. Standards for the electronic transfer of clinical data: Progress and promises. Top. Health Rec. Manag. 1991, 11, 1–16. [Google Scholar]
- Rathert, C.; Porter, T.H.; Mittler, J.N.; Fleig-Palmer, M. Seven years after Meaningful Use: Physicians’ and nurses’ experiences with electronic health records. Health Care Manag. Rev. 2019, 44, 30–40. [Google Scholar] [CrossRef]
- Hyppönen, H.; Kangas, M.; Reponen, J.; Nøhr, C.; Villumsen, S.; Koch, S.; Hardardottir, G.A.; Gilstad, H.; Jerlvall, L.; Pehrsson, T.; et al. Nordic eHealth Benchmarking; Nordisk Ministerråd: Copenhagen, Denmark, 2015; p. 154. Available online: http://norden.diva-portal.org/smash/get/diva2:821230/PREVIEW01.jpg (accessed on 1 December 2020). [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Pizziferri, L.; Kittler, A.F.; Volk, L.A.; Honour, M.M.; Gupta, S.; Wang, S.; Wang, T.; Lippincott, M.; Li, Q.; Bates, D.W. Primary care physician time utilization before and after implementation of an electronic health record: A time-motion study. J. Biomed. Inform. 2005, 38, 176–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poissant, L.; Pereira, J.; Tamblyn, R.; Kawasumi, Y. The impact of electronic health records on time efficiency of physicians and nurses: A systematic review. J. Am. Med. Inform. Assoc. 2005, 12, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Koide, D.; Asonuma, M.; Naito, K.; Igawa, S.; Shimizu, S. Evaluation of electronic health records from viewpoint of patients. In Consumer-Centered Computer-Supported Care for Healthy People; Park, H.A., Murray, P., Delaney, C., Eds.; IOS Press: Amsterdam, The Netherlands, 2006; Volume 122, pp. 304–308. [Google Scholar]
- Kossman, S.P. Perceptions of impact of electronic health records on nurses’ work. In Consumer-Centered Computer-Supported Care for Healthy People; Park, H.A., Murray, P., Delaney, C., Eds.; IOS Press: Amsterdam, The Netherlands, 2006; Volume 122, pp. 337–341. [Google Scholar]
- Lo, H.G.; Newmark, L.P.; Yoon, C.; Volk, L.A.; Carlson, V.L.; Kittler, A.F.; Lippincott, M.; Wang, T.; Bates, D.W. Electronic health records in specialty care: A time-motion study. J. Am. Med. Inform. Assoc. 2007, 14, 609–615. [Google Scholar] [CrossRef]
- Banner, L.; Olney, C.M. Automated Clinical Documentation Does It Allow Nurses More Time for Patient Care? CIN Comput. Inform. Nurs. 2009, 27, 75–81. [Google Scholar] [CrossRef]
- Bloom, M.V.; Huntington, M.K. Faculty, resident, and clinic staff’s evaluation of the effects of EHR implementation. Fam. Med. 2010, 42, 562–566. [Google Scholar]
- de Veer, A.J.E.; Francke, A.L. Attitudes of nursing staff towards electronic patient records: A questionnaire survey. Int. J. Nurs. Stud. 2010, 47, 846–854. [Google Scholar] [CrossRef] [Green Version]
- El-Kareh, R.; Gandhi, T.K.; Poon, E.G.; Newmark, L.P.; Ungar, J.; Lipsitz, S.; Sequist, T.D. Trends in Primary Care Clinician Perceptions of a New Electronic Health Record. J. Gen. Intern. Med. 2009, 24, 464–468. [Google Scholar] [CrossRef] [Green Version]
- Hertzum, M.; Simonsen, J. Positive effects of electronic patient records on three clinical activities. Int. J. Med. Inform. 2008, 77, 809–817. [Google Scholar] [CrossRef]
- Jha, A.K.; Bates, D.W.; Jenter, C.; Orav, E.J.; Zheng, J.; Cleary, P.; Simon, S.R. Electronic health records: Use, barriers and satisfaction among physicians who care for black and Hispanic patients. J. Eval. Clin. Pract. 2009, 15, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Kossman, S.P.; Scheidenhelm, S.L. Nurses’ perceptions of the impact of electronic health records on work and patient outcomes. CIN Comput. Inform. Nurs. 2008, 26, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAlearney, A.S.; Robbins, J.; Hirsch, A.; Jorina, M.; Harrop, J.P. Perceived efficiency impacts following electronic health record implementation: An exploratory study of an urban community health center network. Int. J. Med. Inform. 2010, 79, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Uslu, A.M.; Stausberg, J. Value of the electronic patient record: An analysis of the literature. J. Biomed. Inform. 2008, 41, 675–682. [Google Scholar] [CrossRef] [Green Version]
- Witry, M.J.; Doucette, W.R.; Daly, J.M.; Levy, B.T.; Chrischilles, E.A. Family physician perceptions of personal health records. Perspect. Health Inf. Manag. 2010, 7, 1d. [Google Scholar]
- Archer, N.; Fevrier-Thomas, U.; Lokker, C.; McKibbon, K.A.; Straus, S.E. Personal health records: A scoping review. J. Am. Med. Inform. Assoc. 2011, 18, 515–522. [Google Scholar] [CrossRef] [Green Version]
- Galimany-Masclans, J.; Garrido-Aguilar, E.; Girbau-Garcia, M.R.; Lluch-Canut, T.; Fabrellas-Padres, N. New Technologies and Nursing: Use and Perception of Primary Healthcare Nurses about Electronic Health Record in Catalonia, Spain. Telemed. e-Health 2011, 17, 635–639. [Google Scholar] [CrossRef] [Green Version]
- Grabenbauer, L.; Skinner, A.; Windle, J. Electronic Health Record Adoption—Maybe It’s not about the Money Physician Super-Users, Electronic Health Records and Patient Care. Appl. Clin. Inform. 2011, 2, 460–471. [Google Scholar]
- Yau, G.L.; Williams, A.S.; Brown, J.B. Family physicians’ perspectives on personal health records: Qualitative study. Can. Fam. Physician 2011, 57, e178–e184. [Google Scholar]
- Zlabek, J.A.; Wickus, J.W.; Mathiason, M.A. Early cost and safety benefits of an inpatient electronic health record. J. Am. Med. Inform. Assoc. 2011, 18, 169–172. [Google Scholar] [CrossRef] [Green Version]
- Doyle, R.J.; Wang, N.; Anthony, D.; Borkan, J.; Shield, R.R.; Goldman, R.E. Computers in the examination room and the electronic health record: Physicians’ perceived impact on clinical encounters before and after full installation and implementation. Fam. Pract. 2012, 29, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Goetz Goldberg, D.; Kuzel, A.J.; Feng, L.B.; DeShazo, J.P.; Love, L.E. EHRs in primary care practices: Benefits, challenges, and successful strategies. Am. J. Manag. Care 2012, 18, e48–e54. [Google Scholar] [PubMed]
- Holanda, A.A.; Sa, H.; Vieira, A.; Catrib, A.M.F. Use and Satisfaction with Electronic Health Record by Primary Care Physicians in a Health District in Brazil. J. Med. Syst. 2012, 36, 3141–3149. [Google Scholar] [CrossRef] [PubMed]
- Sockolow, P.S.; Bowles, K.H.; Lehmann, H.P.; Abbott, P.A.; Weiner, J.P. Community-Based, Interdisciplinary Geriatric Care Team Satisfaction with an Electronic Health Record A Multimethod Study. CIN Comput. Inform. Nurs. 2012, 30, 300–311. [Google Scholar] [CrossRef]
- Waterson, P.; Glenn, Y.; Eason, K. Preparing the ground for the ‘paperless hospital’: A case study of medical records management in a UK outpatient services department. Int. J. Med. Inform. 2012, 81, 114–129. [Google Scholar] [CrossRef]
- Zhang, Y.T.; Yu, P.; Shen, J. The benefits of introducing electronic health records in residential aged care facilities: A multiple case study. Int. J. Med. Inform. 2012, 81, 690–704. [Google Scholar] [CrossRef] [Green Version]
- Chao, W.C.; Hu, H.; Ung, C.O.L.; Cai, Y. Benefits and Challenges of Electronic Health Record System on Stakeholders: A Qualitative Study of Outpatient Physicians. J. Med. Syst. 2013, 37, 9960. [Google Scholar] [CrossRef]
- Howard, J.; Clark, E.C.; Friedman, A.; Crosson, J.C.; Pellerano, M.; Crabtree, B.F.; Karsh, B.T.; Jaen, C.R.; Bell, D.S.; Cohen, D.J. Electronic health record impact on work burden in small, unaffiliated, community-based primary care practices. J. Gen. Intern. Med. 2013, 28, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Noblin, A.; Cortelyou-Ward, K.; Cantiello, J.; Breyer, T.; Oliveira, L.; Dangiolo, M.; Cannarozzi, M.; Yeung, T.; Berman, S. EHR Implementation in a New Clinic: A Case Study of Clinician Perceptions. J. Med. Syst. 2013, 37, 9955. [Google Scholar] [CrossRef]
- King, J.; Patel, V.; Jamoom, E.W.; Furukawa, M.F. Clinical benefits of electronic health record use: National findings. Health Serv. Res. 2014, 49, 392–404. [Google Scholar] [CrossRef] [Green Version]
- Laitinen, H.; Kaunonen, M.; Astedt-Kurki, P. The impact of using electronic patient records on practices of reading and writing. Health Inform. J. 2014, 20, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Bellucci, E.; Nguyen, L.T. Electronic health records implementation: An evaluation of information system impact and contingency factors. Int. J. Med. Inform. 2014, 83, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Secginli, S.; Erdogan, S.; Monsen, K.A. Attitudes of health professionals towards electronic health records in primary health care settings: A questionnaire survey. Inf. Health Soc. Care 2014, 39, 15–32. [Google Scholar] [CrossRef] [PubMed]
- Sockolow, P.S.; Bowles, K.H.; Adelsberger, M.C.; Chittams, J.L.; Liao, C. Impact of homecare electronic health record on timeliness of clinical documentation, reimbursement, and patient outcomes. Appl. Clin. Inform. 2014, 5, 445–462. [Google Scholar]
- Wells, S.; Rozenblum, R.; Park, A.; Dunn, M.; Bates, D.W. Personal Health Records for Patients with Chronic Disease. Appl. Clin. Inform. 2014, 5, 416–429. [Google Scholar]
- Barbarito, F.; Pinciroli, F.; Barone, A.; Pizzo, F.; Ranza, R.; Mason, J.; Mazzola, L.; Bonacina, S.; Marceglia, S. Implementing the lifelong personal health record in a regionalised health information system: The case of Lombardy, Italy. Comput. Biol. Med. 2015, 59, 164–174. [Google Scholar] [CrossRef]
- Carayon, P.; Wetterneck, T.B.; Alyousef, B.; Brown, R.L.; Cartmill, R.S.; McGuire, K.; Hoonakker, P.L.; Slagle, J.; Van Roy, K.S.; Walker, J.M.; et al. Impact of electronic health record technology on the work and workflow of physicians in the intensive care unit. Int. J. Med. Inform. 2015, 84, 578–594. [Google Scholar] [CrossRef] [Green Version]
- Colligan, L.; Potts, H.W.W.; Finn, C.T.; Sinkin, R.A. Cognitive workload changes for nurses transitioning from a legacy system with paper documentation to a commercial electronic health record. Int. J. Med. Inform. 2015, 84, 469–476. [Google Scholar] [CrossRef]
- Howley, M.J.; Chou, E.Y.; Hansen, N.; Dalrymple, P.W. The long-term financial impact of electronic health record implementation. J. Am. Med. Inform. Assoc. 2015, 22, 443–452. [Google Scholar] [CrossRef] [Green Version]
- O’Malley, A.S.; Draper, K.; Gourevitch, R.; Cross, D.A.; Scholle, S.H. Electronic health records and support for primary care teamwork. J. Am. Med. Inform. Assoc. 2015, 22, 426–434. [Google Scholar] [CrossRef] [Green Version]
- Yontz, L.S.; Zinn, J.L.; Schumacher, E.J. Perioperative Nurses’ Attitudes toward the Electronic Health Record. J. Perianesthesia Nurs. 2015, 30, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bani-issa, W.; Al Yateem, N.; Al Makhzoomy, I.K.; Ibrahim, A. Satisfaction of health-care providers with electronic health records and perceived barriers to its implementation in the United Arab Emirates. Int. J. Nurs. Pract. 2016, 22, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.A. The impact of electronic health records on collaborative work routines: A narrative network analysis. Int. J. Med. Inform. 2016, 94, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Unni, P.; Staes, C.; Weeks, H.; Kramer, H.; Borbolla, D.; Slager, S.; Taft, T.; Chidambaram, V.; Weir, C. Why aren’t they happy? An analysis of end-user satisfaction with Electronic health records. AMIA Annu. Symp. Proc. 2016, 2016, 2026–2035. [Google Scholar]
- Topaz, M.; Ronquillo, C.; Peltonen, L.M.; Pruinelli, L.; Sarmiento, R.F.; Badger, M.K.; Ali, S.; Lewis, A.; Georgsson, M.; Jeon, E.; et al. Nurse Informaticians Report Low Satisfaction and Multi-level Concerns with Electronic Health Records: Results from an International Survey. AMIA Annu. Symp. Proc. 2016, 2016, 2016–2025. [Google Scholar]
- Yuan, N.; Dudley, R.A.; Boscardin, W.J.; Lin, G.A. Electronic health records systems and hospital clinical performance: A study of nationwide hospital data. J. Am. Med. Inform. Assoc. 2019, 26, 999–1009. [Google Scholar] [CrossRef]
- Yeung, T. Local health department adoption of electronic health records and health information exchanges and its impact on population health. Int. J. Med. Inform. 2019, 128, 1–6. [Google Scholar] [CrossRef]
- Wass, S.; Vimarlund, V. Same, same but different: Perceptions of patients’ online access to electronic health records among healthcare professionals. Health Inform. J. 2019, 25, 1538–1548. [Google Scholar] [CrossRef]
- Walker, J.; Leveille, S.; Bell, S.; Chimowitz, H.; Dong, Z.; Elmore, J.G.; Fernandez, L.; Fossa, A.; Gerard, M.; Fitzgerald, P.; et al. OpenNotes After 7 Years: Patient Experiences with Ongoing Access to Their Clinicians’ Outpatient Visit Notes. J. Med. Internet Res. 2019, 21, e13876. [Google Scholar] [CrossRef]
- Vehko, T.; Hyppönen, H.; Puttonen, S.; Kujala, S.; Ketola, E.; Tuukkanen, J.; Aalto, A.M.; Heponiemi, T. Experienced time pressure and stress: Electronic health records usability and information technology competence play a role. BMC Med. Inform. Decis. Mak. 2019, 19, 160. [Google Scholar] [CrossRef] [Green Version]
- Tubaishat, A. The effect of electronic health records on patient safety: A qualitative exploratory study. Inform. Health Soc. Care 2019, 44, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Schopf, T.R.; Nedrebø, B.; Hufthammer, K.O.; Daphu, I.K.; Lærum, H. How well is the electronic health record supporting the clinical tasks of hospital physicians? A survey of physicians at three Norwegian hospitals. BMC Health Serv. Res. 2019, 19, 934. [Google Scholar] [CrossRef]
- Robinson, S.; Reed, M.; Quevillon, T.; Hirvi, E. Patient perceptions and interactions with their web portal-based laboratory results. BMJ Health Care Inform. 2019, 26, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, M.; Forman, J.; Harrod, M.; Winter, S.; Fowler, K.E.; Krein, S.L.; Gupta, A.; Saint, S.; Singh, H.; Chopra, V. Electronic health records, communication, and data sharing: Challenges and opportunities for improving the diagnostic process. Diagnosis 2019, 6, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Pyron, L.; Carter-Templeton, H. Improved Patient Flow and Provider Efficiency after the Implementation of an Electronic Health Record. CIN Comput. Inform. Nurs. 2019, 37, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.K.; Lin, M.F.; Chen, H.C. Do Electronic Health Records Affect Quality of Care? Evidence from the HITECH Act. Inf. Syst. Res. 2019, 30, 306–318. [Google Scholar] [CrossRef] [Green Version]
- Li, R.C.; Wang, J.K.; Sharp, C.; Chen, J.H. When order sets do not align with clinician workflow: Assessing practice patterns in the electronic health record. BMJ Qual. Saf. 2019, 28, 987–996. [Google Scholar] [CrossRef] [Green Version]
- Lemon, C.; De Ridder, M.; Khadra, M. Do Electronic Medical Records Improve Advance Directive Documentation? A Systematic Review. Am. J. Hosp. Palliat. Med. 2019, 36, 255–263. [Google Scholar] [CrossRef]
- Legler, A.; Price, M.; Parikh, M.; Nebeker, J.R.; Ward, M.C.; Wedemeyer, L.; Pizer, S.D. Effect on VA Patient Satisfaction of Provider’s Use of an Integrated Viewer of Multiple Electronic Health Records. J. Gen. Intern. Med. 2019, 34, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Kutney-Lee, A.; Sloane, D.M.; Bowles, K.H.; Burns, L.R.; Aiken, L.H. Electronic Health Record Adoption and Nurse Reports of Usability and Quality of Care: The Role of Work Environment. Appl. Clin. Inform. 2019, 10, 129–139. [Google Scholar] [CrossRef]
- Kariotis, T.C.; Harris, K.M. Clinician perceptions of My Health Record in mental health care: Medication management and sharing mental health information. Aust. J. Prim. Health 2019, 25, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Joukes, E.; de Keizerl, N.F.; de Bruijne, M.C.; Abu-Hanna, A.; Cornett, R. Impact of Electronic versus Paper-Based Record in before EHR Implementation on Health Care Professionals’ Perceptions of EHR Use, Data Quality, and Data Reuse. Appl. Clin. Inform. 2019, 10, 199–209. [Google Scholar] [PubMed]
- Jacobs, M.; Boersma, L.J.; Swart, R.; Mannens, R.; Reymen, B.; Korver, F.; van Merode, F.; Dekker, A. Electronic Health Record implementation in a large academic radiotherapy department: Temporarily disruptions but long-term benefits. Int. J. Med. Inform. 2019, 129, 342–348. [Google Scholar] [CrossRef]
- Huang, J.; Chen, Y.; Landis, J.R.; Mahoney, K.B. Difference between Users and Nonusers of a Patient Portal in Health Behaviors and Outcomes: Retrospective Cohort Study. J. Med. Internet Res. 2019, 21, e13146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, A.M.; Siwani, R.; Pickering, B.W.; Herasevich, V. Clinical impact of intraoperative electronic health record downtime on surgical patients. J. Am. Med. Inform. Assoc. 2019, 26, 928–933. [Google Scholar] [CrossRef]
- Graber, M.L.; Siegal, D.; Riah, H.; Johnston, D.; Kenyon, K. Electronic Health Record-Related Events in Medical Malpractice Claims. J. Patient Saf. 2019, 15, 77–85. [Google Scholar] [CrossRef]
- Gardner, R.L.; Cooper, E.; Haskell, J.; Harris, D.A.; Poplau, S.; Kroth, P.J.; Linzer, M. Physician stress and burnout: The impact of health information technology. J. Am. Med. Inform. Assoc. 2019, 26, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Eberts, M.; Capurro, D. Patient and Physician Perceptions of the Impact of Electronic Health Records on the Patient-Physician Relationship. Appl. Clin. Inform. 2019, 10, 729–734. [Google Scholar] [CrossRef]
- Dobrow, M.J.; Bytautas, J.P.; Tharmalingam, S.; Hagens, S. Interoperable Electronic Health Records and Health Information Exchanges: Systematic Review. JMIR Med. Inform. 2019, 7, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Dendere, R.; Slade, C.; Burton-Jones, A.; Sullivan, C.; Staib, A.; Janda, M. Patient Portals Facilitating Engagement with Inpatient Electronic Medical Records: A Systematic Review. J. Med. Internet Res. 2019, 21, e12779. [Google Scholar] [CrossRef]
- Dalal, A.K.; Dykes, P.; Samal, L.; McNally, K.; Mlaver, E.; Yoon, C.S.; Lipsitz, S.R.; Bates, D.W. Potential of an Electronic Health Record-Integrated Patient Portal for Improving Care Plan Concordance during Acute Care. Appl. Clin. Inform. 2019, 10, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Creber, R.M.M.; Grossman, L.V.; Ryan, B.; Qian, M.; Polubriaginof, F.C.G.; Restaino, S.; Bakken, S.; Hripcsak, G.; Vawdrey, D.K. Engaging hospitalized patients with personalized health information: A randomized trial of an inpatient portal. J. Am. Med. Inform. Assoc. 2019, 26, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Assis-Hassid, S.; Grosz, B.J.; Zimlichman, E.; Rozenblum, R.; Bates, D.W. Assessing EHR use during hospital morning rounds: A multi-faceted study. PLoS ONE 2019, 14, e0212816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoun, J.; Hamadeh, G.; Romani, M. Effect of computer use on physician-patient communication using interviews: A patient perspective. Int. J. Med. Inform. 2019, 125, 91–95. [Google Scholar] [CrossRef]
- Alsohime, F.; Temsah, M.H.; Al-Eyadhy, A.; Bashiri, F.A.; Househ, M.; Jamal, A.; Hasan, G.; Alhaboob, A.A.; Alabdulhafid, M.; Amer, Y.S. Satisfaction and perceived usefulness with newly-implemented Electronic Health Records System among pediatricians at a university hospital. Comp. Methods Prog. Biomed. 2019, 169, 51–57. [Google Scholar] [CrossRef]
- Al-Rayes, S.A.; Alumran, A.; AlFayez, W. The Adoption of the Electronic Health Record by Physicians. Methods Inf. Med. 2019, 58, 63–70. [Google Scholar] [CrossRef]
- Al-Rawajfah, O.; Tubaishat, A. Barriers and facilitators to using electronic healthcare records in Jordanian hospitals from the nurses’ perspective: A national survey. Inf. Health Soc. Care 2019, 44, 1–11. [Google Scholar] [CrossRef]
- Whalen, K.; Lynch, E.; Moawad, I.; John, T.; Lozowski, D.; Cummings, B.M. Transition to a new electronic health record and pediatric medication safety: Lessons learned in pediatrics within a large academic health system. J. Am. Med. Inform. Assoc. 2018, 25, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Taisan, E.A.A.; Seliaman, M.E. Perceived Barriers and Drivers of Health Information Systems Adoption by Public Hospitals in Alhasa. In Proceedings of the 2018 21st Saudi Computer Society National Computer Conference (NCC), Riyadh, Saudi Arabia, 25–26 April 2018; pp. 1–5. [Google Scholar]
- Strudwick, G.; Hall, L.M.; Nagle, L.; Trbovich, P. Acute care nurses’ perceptions of electronic health record use: A mixed method study. Nurs. Open 2018, 5, 491–500. [Google Scholar] [CrossRef] [Green Version]
- Schenk, E.; Schleyer, R.; Jones, C.R.; Fincham, S.; Daratha, K.B.; Monsen, K.A. Impact of Adoption of a Comprehensive Electronic Health Record on Nursing Work and Caring Efficacy. CIN Comput. Inform. Nurs. 2018, 36, 331–339. [Google Scholar] [CrossRef]
- Priestman, W.; Sridharan, S.; Vigne, H.; Collins, R.; Seamer, L.; Sebire, N.J. What to expect from electronic patient record system implementation; lessons learned from published evidence. J. Innov. Health Inform. 2018, 25, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Osop, H.; Sahama, T. Doctors’ perception of the potential of EHR: A Singapore insight. In Proceedings of the Australasian Computer Science Week Multiconference, Brisbane, Australia, 29 January–2 February 2018; pp. 1–6. [Google Scholar]
- O’Donnell, A.; Kaner, E.; Shaw, C.; Haighton, C. Primary care physicians’ attitudes to the adoption of electronic medical records: A systematic review and evidence synthesis using the clinical adoption framework. BMC Med. Inform. Decis. Mak. 2018, 18, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyerhoefer, C.D.; Sherer, S.A.; Deily, M.E.; Chou, S.Y.; Guo, X.H.; Chen, J.; Sheinberg, M.; Levick, D. Provider and patient satisfaction with the integration of ambulatory and hospital EHR systems. J. Am. Med. Inform. Assoc. 2018, 25, 1054–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, B.; Eastham, R.; Brown, B.; Fitton, R.; Dickinson, D. Primary Care Patient Records in the United Kingdom: Past, Present, and Future Research Priorities. J. Med. Internet Res. 2018, 20, e11293. [Google Scholar] [CrossRef] [PubMed]
- Marmor, R.A.; Clay, B.; Millen, M.; Savides, T.J.; Longhurst, C.A. The Impact of Physician EHR Usage on Patient Satisfaction. Appl. Clin. Inform. 2018, 9, 11–14. [Google Scholar] [CrossRef] [Green Version]
- Lim, M.C.; Boland, M.V.; McCannel, C.A.; Saini, A.; Chiang, M.F.; Epley, K.D.; Lum, F. Adoption of Electronic Health Records and Perceptions of Financial and Clinical Outcomes among Ophthalmologists in the United States. JAMA Ophthalmol. 2018, 136, 164–170. [Google Scholar] [CrossRef]
- Kuo, A.M.S.; Thavalathil, B.; Elwyn, G.; Nemeth, Z.; Dang, S. The Promise of Electronic Health Records to Promote Shared Decision Making: A Narrative Review and a Look Ahead. Med. Decis. Mak. 2018, 38, 1040–1045. [Google Scholar] [CrossRef]
- Krousel-Wood, M.; McCoy, A.B.; Ahia, C.; Holt, E.W.; Trapani, D.N.; Luo, Q.Y.; Price-Haywood, E.G.; Thomas, E.J.; Sittig, D.F.; Milani, R.V. Implementing electronic health records (EHRs): Health care provider perceptions before and after transition from a local basic EHR to a commercial comprehensive EHR. J. Am. Med. Inform. Assoc. 2018, 25, 618–626. [Google Scholar] [CrossRef]
- Khan, U.R.; Zia, T.A.; Pearce, C.; Perera, K. Perceptions and Experiences of General Practice Users about My Health Record. In Health Information Science; Siuly, S., Lee, I., Huang, Z., Zhou, R., Wang, H., Xiang, W., Eds.; Springer: Cham, Switzerland, 2018; Volume 11148, pp. 3–16. [Google Scholar]
- Khairat, S.; Burke, G.; Archambault, H.; Schwartz, T.; Larson, J.; Ratwani, R.M. Perceived Burden of EHRs on Physicians at Different Stages of Their Career. Appl. Clin. Inform. 2018, 9, 336–347. [Google Scholar]
- Kannampallil, T.G.; Denton, C.A.; Shapiro, J.S.; Patel, V.L. Efficiency of Emergency Physicians: Insights from an Observational Study using EHR Log Files. Appl. Clin. Inform. 2018, 9, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Harris, D.A.; Haskell, J.; Cooper, E.; Crouse, N.; Gardner, R. Estimating the association between burnout and electronic health record-related stress among advanced practice registered nurses. Appl. Nurs. Res. 2018, 43, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Graham, T.A.D.; Ballermann, M.; Lang, E.; Bullard, M.J.; Parsons, D.; Mercuur, G.; San Agustin, P.; Ali, S. Emergency Physician Use of the Alberta Netcare Portal, a Province-Wide Interoperable Electronic Health Record: Multi-Method Observational Study. JMIR Med. Inform. 2018, 6, e10184. [Google Scholar] [CrossRef] [PubMed]
- Entzeridou, E.; Markopoulou, E.; Mollaki, V. Public and physician’s expectations and ethical concerns about electronic health record: Benefits outweigh risks except for information security. Int. J. Med. Inform. 2018, 110, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Dudding, K.M.; Gephart, S.M.; Carrington, J.M. Neonatal Nurses Experience Unintended Consequences and Risks to Patient Safety with Electronic Health Records. CIN Comput. Inform. Nurs. 2018, 36, 167–176. [Google Scholar] [CrossRef]
- Despins, L.A.; Wakefield, B.J. The Role of the Electronic Medical Record in the Intensive Care Unit Nurse’s Detection of Patient Deterioration: A Qualitative Study. CIN Comput. Inform. Nurs. 2018, 36, 284–292. [Google Scholar] [CrossRef]
- Denton, C.A.; Soni, H.C.; Kannampallil, T.G.; Serrichio, A.; Shapiro, J.S.; Traub, S.J.; Patel, V.L. Emergency Physicians’ Perceived Influence of EHR Use on Clinical Workflow and Performance Metrics. Appl. Clin. Inform. 2018, 9, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Bruns, E.J.; Hook, A.N.; Parker, E.M.; Esposito, I.; Sather, A.; Parigoris, R.M.; Lyon, A.R.; Hyde, K.L. Impact of a Web-Based Electronic Health Record on Behavioral Health Service Delivery for Children and Adolescents: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e10197. [Google Scholar] [CrossRef]
- Baumann, L.A.; Baker, J.; Elshaug, A.G. The impact of electronic health record systems on clinical documentation times: A systematic review. Health Policy 2018, 122, 827–836. [Google Scholar] [CrossRef]
- Bae, J.; Rask, K.J.; Becker, E.R. The Impact of Electronic Medical Records on Hospital-Acquired Adverse Safety Events: Differential Effects between Single-Source and Multiple-Source Systems. Am. J. Med. Qual. 2018, 33, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Auefuea, S.; Nartthanarung, A.; Pronsawatchai, P.; Soontornpipit, P. The Perspective of Users after the Trial of the Electronic Record System in Home Health Care Unit. In Proceedings of the 2018 International Electrical Engineering Congress (iEECON), Krabi, Thailand, 7–9 March 2018; pp. 1–4. [Google Scholar]
- Asan, O.; Nattinger, A.B.; Gurses, A.P.; Tyszka, J.T.; Yen, T.W.F. Oncologists’ Views Regarding the Role of Electronic Health Records in Care Coordination. JCO Clin. Cancer Inform. 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Aljabri, D.; Dumitrascu, A.; Burton, M.C.; White, L.; Khan, M.; Xirasagar, S.; Horner, R.; Naessens, J. Patient portal adoption and use by hospitalized cancer patients: A retrospective study of its impact on adverse events, utilization, and patient satisfaction. BMC Med. Inform. Decis. Mak. 2018, 18, 70. [Google Scholar] [CrossRef] [PubMed]
- Akhu-Zaheya, L.; Al-Maaitah, R.; Hani, S.B. Quality of nursing documentation: Paper-based health records versus electronic-based health records. J. Clin. Nurs. 2018, 27, e578–e589. [Google Scholar] [CrossRef] [PubMed]
- Yung, A. Adoption of Electronic Health Record System in Community-Based Physiotherapy Clinics: A Pilot Case Study. Stud. Health Technol. Inform. 2017, 234, 395–400. [Google Scholar] [PubMed]
- Tubaishat, A. Evaluation of Electronic Health Record Implementation in Hospitals. CIN Comput. Inform. Nurs. 2017, 35, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Tsou, A.Y.; Lehmann, C.U.; Michel, J.; Solomon, R.; Possanza, L.; Gandhi, T. Safe Practices for Copy and Paste in the EHR. Systematic Review, Recommendations, and Novel Model for Health IT Collaboration. Appl. Clin. Inform. 2017, 8, 12–34. [Google Scholar]
- Snowden, A.; Kolb, H. Two years of unintended consequences: Introducing an electronic health record system in a hospice in Scotland. J. Clin. Nurs. 2017, 26, 1414–1427. [Google Scholar] [CrossRef] [Green Version]
- Robertson, S.L.; Robinson, M.D.; Reid, A. Electronic Health Record Effects on Work-Life Balance and Burnout within the I(3) Population Collaborative. J. Grad. Med. Educ. 2017, 9, 479–484. [Google Scholar] [CrossRef] [Green Version]
- Raglan, G.B.; Margolis, B.; Paulus, R.A.; Schulkin, J. Electronic Health Record Adoption among Obstetrician/Gynecologists in the United States: Physician Practices and Satisfaction. J. Healthc. Qual. 2017, 39, 144–152. [Google Scholar] [CrossRef]
- Powell, K.R. Patient-Perceived Facilitators of and Barriers to Electronic Portal Use: A Systematic Review. CIN Comput. Inform. Nurs. 2017, 35, 565–573. [Google Scholar] [CrossRef]
- Plantier, M.; Havet, N.; Durand, T.; Caquot, N.; Amaz, C.; Philip, I.; Biron, P.; Perrier, L. Does adoption of electronic health records improve organizational performances of hospital surgical units? Results from the French e-SI (PREPS-SIPS) study. Int. J. Med. Inform. 2017, 98, 47–55. [Google Scholar] [CrossRef]
- Ochoa, A.; Kitayama, K.; Uijtdehaage, S.; Vermillion, M.; Eaton, M.; Carpio, F.; Serota, M.; Hochman, M.E. Patient and provider perspectives on the potential value and use of a bilingual online patient portal in a Spanish-speaking safety-net population. J. Am. Med. Inform. Assoc. 2017, 24, 1160–1164. [Google Scholar] [CrossRef] [PubMed]
- McDowell, J.; Wu, A.; Ehrenfeld, J.M.; Urman, R.D. Effect of the Implementation of a New Electronic Health Record System on Surgical Case Turnover Time. J. Med. Syst. 2017, 41, 42. [Google Scholar] [CrossRef] [PubMed]
- Liew, C.L.; Harjadinata, J. Patient Portal Service: An Exploration of Patients’ Experience and Perception. In Proceedings of the ICDS 2017: The Eleventh International Conference on Digital Society, Nice, France, 19–23 March 2017; pp. 1–5. [Google Scholar]
- King, G.; Maxwell, J.; Karmali, A.; Hagens, S.; Pinto, M.; Williams, L.; Adamson, K. Connecting Families to Their Health Record and Care Team: The Use, Utility, and Impact of a Client/Family Health Portal at a Children’s Rehabilitation Hospital. J. Med. Internet Res. 2017, 19, e97. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.M.; Dean, S.M.; Carayon, P.; Wetterneck, T.B.; Hoonakker, P.L.T. Healthcare Team Perceptions of a Portal for Parents of Hospitalized Children Before and After Implementation. Appl. Clin. Inform. 2017, 8, 265–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaipio, J.; Lääveri, T.; Hyppönen, H.; Vainiomäki, S.; Reponen, J.; Kushniruk, A.; Borycki, E.; Vänskä, J. Usability problems do not heal by themselves: National survey on physicians’ experiences with EHRs in Finland. Int. J. Med. Inform. 2017, 97, 266–281. [Google Scholar] [CrossRef]
- Hanauer, D.A.; Branford, G.L.; Greenberg, G.; Kileny, S.; Couper, M.P.; Zheng, K.; Choi, S.W. Two-year longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: Does a J-curve of satisfaction really exist? J. Am. Med. Inform. Assoc. 2017, 24, E157–E165. [Google Scholar] [CrossRef]
- Hamamura, F.D.; Withy, K.; Hughes, K. Identifying Barriers in the Use of Electronic Health Records in Hawai’i. Hawaii. J. Med. Public Health 2017, 76, 28–35. [Google Scholar]
- Gregory, M.E.; Russo, E.; Singh, H. Electronic Health Record Alert-Related Workload as a Predictor of Burnout in Primary Care Providers. Appl. Clin. Inform. 2017, 8, 686–697. [Google Scholar]
- Gesulga, J.M.; Berjame, A.; Moquiala, K.S.; Galido, A. Barriers to Electronic Health Record System Implementation and Information Systems Resources: A Structured Review. In Proceedings of the 4th Information Systems International Conference, Bali, Indonesia, 6–8 November 2017; Volume 124, pp. 544–551. [Google Scholar]
- Gerber, D.E.; Beg, M.S.; Duncan, T.; Gill, M.; Lee, S.J.C. Oncology Nursing Perceptions of Patient Electronic Portal Use: A Qualitative Analysis. Oncol. Nurs. Forum 2017, 44, 165–170. [Google Scholar]
- Frogner, B.K.; Wu, X.L.; Ku, L.; Pittman, P.; Masselink, L.E. Do Years of Experience with Electronic Health Records Matter for Productivity in Community Health Centers? J. Ambul. Care Manag. 2017, 40, 36–47. [Google Scholar] [CrossRef]
- Fletcher, K.E.; Asan, O.; Tyszka, J. Residents’ Insights and Ideas about Screen-Sharing in Primary Care Clinics. Appl. Clin. Inform. 2017, 8, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Feblowitz, J.; Takhar, S.S.; Ward, M.J.; Ribeira, R.; Landman, A.B. A Custom-Developed Emergency Department Provider Electronic Documentation System Reduces Operational Efficiency. Ann. Emerg. Med. 2017, 70, 674–682.e1. [Google Scholar] [CrossRef] [PubMed]
- Doberne, J.W.; Redd, T.; Lattin, D.; Yackel, T.R.; Eriksson, C.O.; Mohan, V.; Gold, J.A.; Ash, J.S.; Chiang, M.F. Perspectives and Uses of the Electronic Health Record Among US Pediatricians A National Survey. J. Ambul. Care Manag. 2017, 40, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Bush, R.A.; Connelly, C.D.; Perez, A.; Chan, N.; Kuelbs, C.; Chiang, G.J. Physician Perception of the Role of the Patient Portal in Pediatric Health. J. Ambul. Care Manag. 2017, 40, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Bobadilla, J.L.; Roe, C.S.; Estes, P.; Lackey, J.; Steltenkamp, C.L. Leveraging Electronic Health Record Implementation to Facilitate Clinical and Operational Quality Improvement in an Ambulatory Surgical Clinic. J. Ambul. Care Manag. 2017, 40, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Blijleven, V.; Koelemeijer, K.; Jaspers, M. Identifying and eliminating inefficiencies in information system usage: A lean perspective. Int. J. Med. Inform. 2017, 107, 40–47. [Google Scholar] [CrossRef]
- Bjarnadottir, R.I.; Herzig, C.T.A.; Travers, J.L.; Castle, N.G.; Stone, P.W. Implementation of Electronic Health Records in US Nursing Homes. CIN Comput. Inform. Nurs. 2017, 35, 417–424. [Google Scholar] [CrossRef]
- Baudendistel, I.; Winkler, E.C.; Kamradt, M.; Brophy, S.; Langst, G.; Eckrich, F.; Heinze, O.; Bergh, B.; Szecsenyi, J.; Ose, D. Cross-sectoral cancer care: Views from patients and health care professionals regarding a personal electronic health record. Eur. J. Cancer Care 2017, 26, e12429. [Google Scholar] [CrossRef]
- Bartlett, K.W.; Parente, V.M.; Morales, V.; Hauser, J.; McLean, H.S. Improving the Efficiency of Care for Pediatric Patients Hospitalized with Asthma. Hosp. Pediatr. 2017, 7, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Arndt, B.G.; Beasley, J.W.; Watkinson, M.D.; Temte, J.L.; Tuan, W.J.; Sinsky, C.A.; Gilchrist, V.J. Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Event Log Data and Time-Motion Observations. Ann. Fam. Med. 2017, 15, 419–426. [Google Scholar] [CrossRef]
- Zanaboni, P.; Kummervold, P.E.; Sorensen, T.; Johansen, M.A. Patient Use and Experience with Online Access to Electronic Health Records in Norway: Results from an Online Survey. J. Med. Internet Res. 2020, 22, e16144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, R.M.; Burmeister, E.; Jeffrey, C.; Birgan, S.; Garrahy, E.; Andrews, J.; Hada, A.; Aitken, L.M. The impact of an integrated electronic health record on nurse time at the bedside: A pre-post continuous time and motion study. Collegian 2020, 27, 63–74. [Google Scholar] [CrossRef] [Green Version]
- Kaipio, J.; Kuusisto, A.; Hyppönen, H.; Heponiemi, T.; Lääveri, T. Physicians’ and nurses’ experiences on EHR usability: Comparison between the professional groups by employment sector and system brand. Int. J. Med. Inform. 2020, 134, 104018. [Google Scholar] [CrossRef] [PubMed]
- Jabour, A.M. The Impact of Electronic Health Records on the Duration of Patients’ Visits: Time and Motion Study. JMIR Med. Inform. 2020, 8, e16502. [Google Scholar] [CrossRef] [PubMed]
- Greysen, S.R.; Magan, Y.; Rosenthal, J.; Jacolbia, R.; Auerbach, A.D.; Harrison, J.D. Patient Recommendations to Improve the Implementation of and Engagement with Portals in Acute Care: Hospital-Based Qualitative Study. J. Med. Internet Res. 2020, 22, e13337. [Google Scholar] [CrossRef] [PubMed]
- Atasoy, H.; Greenwood, B.N.; McCullough, J.S. The Digitization of Patient Care: A Review of the Effects of Electronic Health Records on Health Care Quality and Utilization. Annu. Rev. Public Health 2019, 40, 487–500. [Google Scholar] [CrossRef] [Green Version]
- Alami, H.; Lehoux, P.; Gagnon, M.-P.; Fortin, J.-P.; Fleet, R.; Ag Ahmed, M.A. Rethinking the electronic health record through the quadruple aim: Time to align its value with the health system. BMC Med. Inform. Decis. Mak. 2020, 20, 32. [Google Scholar] [CrossRef] [Green Version]
- Kruse, C.S.; Mileski, M.; Vijaykumar, A.G.; Viswanathan, S.V.; Suskandla, U.; Chidambaram, Y. Impact of Electronic Health Records on Long-Term Care Facilities: Systematic Review. JMIR Med. Inform. 2017, 5, e35. [Google Scholar] [CrossRef]
- Kruse, C.S.; Kristof, C.; Jones, B.; Mitchell, E.; Martinez, A. Barriers to Electronic Health Record Adoption: A Systematic Literature Review. J. Med. Syst. 2016, 40, 252. [Google Scholar] [CrossRef] [Green Version]
- Kruse, C.S.; Kothman, K.; Anerobi, K.; Abanaka, L. Adoption Factors of the Electronic Health Record: A Systematic Review. JMIR Med. Inform. 2016, 4, e19. [Google Scholar] [CrossRef]
- Adler-Milstein, J.; Zhao, W.; Willard-Grace, R.; Knox, M.; Grumbach, K. Electronic health records and burnout: Time spent on the electronic health record after hours and message volume associated with exhaustion but not with cynicism among primary care clinicians. J. Am. Med. Inform. Assoc. 2020, 27, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Ammenwerth, E. Evidence-based Health Informatics: How Do We Know What We Know? Methods Inf. Med. 2015, 54, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Talmon, J.; Ammenwerth, E.; Brender, J.; de Keizer, N.; Nykanen, P.; Rigby, M. STARE-HI—Statement on reporting of evaluation studies in Health Informatics. Int. J. Med. Inform. 2009, 78, 1–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Databases | Search Details | Number of Papers |
|---|---|---|
| PubMed | (“electronic health record”[TIAB] OR “EHR”[TIAB] OR “personal health record”[TIAB] OR “PHR”[TIAB] OR “patient record”[TIAB]) AND (“care pathways”[TIAB] OR workflow[TIAB] OR “work routines”[TIAB] OR workload [TIAB] OR “work process”[TIAB]) AND ((hasabstract[text] AND “loattrfree full text”[sb] AND “loattrfull text”[sb]) AND (“2005/01/01”[PDAT]: “2020/05/31”[PDAT]) AND “humans”[MeSH Terms] AND English[lang]) | n = 275 |
| (“electronic health record”[TIAB] OR “EHR”[TIAB] OR “personal health record”[TIAB] OR “PHR”[TIAB] OR “patient record”[TIAB]) AND (efficiency[TIAB] OR advantages[TIAB] OR disadvantages[TIAB] OR satisfaction[TIAB] OR teamwork[TIAB] OR collaboration[TIAB] OR benefits[TIAB] OR challenges[TIAB]) AND ((hasabstract[text] AND “loattrfree full text”[sb] AND “loattrfull text”[sb]) AND (“2005/01/01”[PDAT]: “2020/05/31”[PDAT]) AND “humans”[MeSH Terms] AND English[lang]) | n = 824 | |
| Web of Science | TOPIC: ((“electronic health record*” OR “EHR*” OR “personal health record*” OR “PHR*” OR “patient record*”) AND (“care pathways” OR workflow OR “work routines” OR workload OR “work process”)) Refined by: Web of Science categories: (medical informatics OR health care sciences services OR computer science information systems OR information science library science OR nursing OR computer science theory methods OR computer science software engineering) AND document types: (article OR review OR proceedings paper) AND languages: (English) Timespan: 2005–2020. Indexes: SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, ESCI. | n = 701 |
| TOPIC: ((“electronic health record*” OR “EHR*” OR “personal health record*” OR “PHR*” OR “patient record*”) AND (efficiency OR advantages OR disadvantages OR satisfaction OR teamwork OR collaboration OR benefits OR challenges)) Refined by: Web of Science categories: (medical informatics OR health care sciences services OR computer science information systems OR computer science theory methods OR information science library science OR nursing OR computer science software engineering) AND languages: (English) Timespan: 2005–2020. Indexes: SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, ESCI. | n = 4146 | |
| IEEE | ((“electronic health record*” OR “EHR*” OR “personal health record*” OR “PHR*” OR “patient record*”) AND (“care pathways” OR workflow OR “work routines” OR workload OR “work process”)) | n = 111 |
| ((“electronic health record*” OR “EHR*” OR “personal health record*” OR “PHR*” OR “patient record*”) AND (efficiency OR advantages OR disadvantages OR satisfaction OR teamwork OR collaboration OR benefits OR challenges)) | n = 1748 | |
| ACM | (“electronic health record*” OR “EHR*” OR “personal health record*” OR “PHR*” OR “patient record*”) AND (“care pathways” OR workflow OR “work routines” OR workload OR “work process”) Articles available from 2005–2020 | n = 33 |
| (“electronic health record*” OR “EHR*” OR “personal health record*” OR “PHR*” OR “patient record*”) AND (efficiency OR advantages OR disadvantages OR satisfaction OR teamwork OR collaboration OR benefits OR challenges) Articles available from 2005–2020 | n = 276 |
| Characteristic | Number of Studies | Reference |
|---|---|---|
| Year | ||
| 2005–2007 | 5 | [17,18,19,20,21] |
| 2008–2010 | 10 | [22,23,24,25,26,27,28,29,30,31] |
| 2011–2013 | 14 | [32,33,34,35,36,37,38,39,40,41,42,43,44,45] |
| 2014–2016 | 16 | [46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61] |
| 2017–2019 | 91 | [62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152] |
| 2020 (until end of May) | 5 | [153,154,155,156,157] |
| Country of origin | ||
| Australia | 5 | [42,77,107,123,154] |
| Brazil | 1 | [39] |
| Canada | 5 | [35,69,85,96,111] |
| Denmark | 1 | [26] |
| Finland | 4 | [47,66,136,155] |
| France | 1 | [130] |
| Germany | 1 | [150] |
| Greece | 1 | [112] |
| Italy | 1 | [52] |
| Japan | 1 | [19] |
| Jordan | 4 | [67,93,122,124] |
| Lebanon | 1 | [90] |
| Macao | 1 | [43] |
| Netherlands | 4 | [24,78,79,148] |
| New Zealand | 1 | [133] |
| Norway | 2 | [68,153] |
| Saudi Arabia | 4 | [91,92,95,156] |
| Singapore | 1 | [99] |
| Spain | 1 | [33] |
| Sweden | 1 | [64] |
| Thailand | 1 | [119] |
| Turkey | 1 | [49] |
| UAE | 1 | [58] |
| UK | 2 | [41,126] |
| USA | 81 | [17,20,21,22,23,25,27,28,29,31,34,36,37,38,40,44,45,46,50,51,53,54,55,56,57,59,60,61,62,63,65,70,71,72,73,75,76,80,81,82,83,84,87,88,89,94,97,101,103,104,106,108,109,110,113,114,115,116,118,120,121,127,128,131,132,134,135,137,138,139,141,142,143,144,145,146,147,149,151,152,157] |
| Type/methodology | ||
| Focus group | 10 | [31,34,70,96,126,134,138,139,141,150] |
| Interview | 33 | [20,26,28,29,35,37,38,40,41,42,43,44,45,50,51,56,59,64,67,69,70,77,89,90,114,115,120,123,134,143,146,148,157] |
| Literature review | 15 | [18,30,32,48,74,85,86,98,100,102,105,117,125,129,140] |
| Measurement/analysis of EHR usage and/or other data | 27 | [36,40,50,55,62,63,71,72,73,76,79,80,81,82,94,103,109,113,118,121,122,130,132,144,147,149,151] |
| Measurement of mental workload | 3 | [26,54,108] |
| Observation | 16 | [20,26,28,38,40,44,47,50,59,70,71,89,108,111,148,152] |
| Questionnaire/survey | 63 | [19,20,23,24,25,27,28,33,38,39,40,46,49,50,51,54,57,58,59,60,61,64,65,66,68,71,75,78,83,84,87,89,91,92,93,95,96,99,101,104,106,107,108,110,112,119,124,126,127,128,131,133,134,135,136,137,139,142,145,146,149,153,155] |
| Time-motion observation | 7 | [17,21,22,53,97,154,156] |
| Randomized trial | 2 | [88,116] |
| Participants | ||
| Physicians | 61 | [17,21,23,25,26,27,29,31,34,35,37,38,39,40,43,44,45,46,47,49,51,53,56,58,59,60,64,68,70,77,78,83,84,91,92,95,99,101,104,106,107,108,111,112,115,120,126,127,128,131,135,136,137,138,143,145,146,148,150,152,155] |
| Patients/citizens | 23 | [19,21,44,47,65,69,75,80,81,84,87,88,90,101,107,112,121,131,133,150,153,156,157] |
| Registered nurses or nurse practitioners | 46 | [20,22,23,24,25,26,28,29,33,38,40,41,42,44,47,49,50,56,57,58,59,61,64,66,67,76,78,93,95,96,97,107,110,113,114,119,124,126,135,138,141,148,149,150,154,155] |
| Other clinicians (e.g., physician assistant, nursing assistant, midwife, lab staff, therapist etc.) | 24 | [23,24,25,29,38,40,42,45,49,50,56,58,64,101,106,107,116,123,126,131,135,138,139,150] |
| Non-clinicians (e.g., research assistant, administrative staff, personal care worker, manager, IT staff, quality improvement staff etc.) | 18 | [21,29,38,40,41,42,44,50,51,56,59,77,78,95,107,126,135,142] |
| Theme | Category | Sub-Category | Reference |
|---|---|---|---|
| Positive effects | |||
| Work for the healthcare providers | |||
| Better efficiency | [18,20,22,25,27,28,29,34,41,42,43,44,45,48,49,50,59,66,67,71,85,109,112,115,116,147,151] | ||
| Better communication | [17,25,27,34,38,42,43,44,45,50,56,85,110,134,155] | ||
| More organized at work | [20,28,38,42,56,91,110,119] | ||
| Decreased workload | [26,44] | ||
| Support disease and quality management | [38,42,43,44,151] | ||
| Support learning and decision-making | [27,42,49,85,99,105] | ||
| Data and information | |||
| Increased accessibility | [17,20,25,28,32,34,37,38,42,43,44,45,46,48,56,65,69,75,90,91,99,101,119,128,147,150,153] | ||
| Data quality and accuracy | [30,38,42,48,50,51,57,67,78,91,119,122,147] | ||
| Better data storage and backup | [42,43,67,150] | ||
| Care for patients | |||
| Quality of care | [17,19,22,24,25,27,28,33,42,43,45,46,47,48,49,53,57,62,63,64,67,72,74,75,76,80,84,85,86,88,91,97,99,106,107,110,111,112,115,116,118,125,128,131,133,135,146,150,153] | ||
| Better communication | [32,34,38,42,44,45,64,69,84,86,102,106,131,134,143,146,147,153] | ||
| Patient empowerment | [32,37,45,51,64,65,69,86,153] | ||
| Change in time spent for patients | [19,116,156] | ||
| Economic impact | |||
| Better productivity | [48,50,53,85,130,142] | ||
| Decreased cost | [30,36,112,151] | ||
| Increased revenue and reimbursement | [55] | ||
| Negative effects | |||
| Work for the healthcare providers | |||
| Worse efficiency | [17,20,22,23,25,28,29,34,38,39,40,43,44,45,58,66,78,83,91,96,97,101,109,110,113,117,126,131,132,136,137,143,144,145,148,154] | ||
| Increased workload | [29,38,44,45,54,68,83,91,96,108,110,112,113,127,135,139,141,146,148,152] | ||
| Poor communication | [34,40,47,48,70,78,120] | ||
| Dysfunctional workflow | [29,38,44,45,47,61,73,89,91,112,113,114,115,141,148] | ||
| Data and information | |||
| Data quality and accuracy | [40,48,78,91,122,137,145] | ||
| Decreased accessibility | [39,40,43,70,106,126] | ||
| Care for patients | |||
| Face-to-face or direct communication | [43,45,84,137] | ||
| Quality of care | [20,28,34,38,81,82,94,106,116,126,137,141,149] | ||
| Economic impact | |||
| Worse productivity | [27,38,48,53,55,104] | ||
| Barriers | |||
| Support for users | |||
| Poor training and technical support | [27,32,38,43,45,48,52,58,66,93,98,100,107,128,129,138,140,157] | ||
| Lack of user involvement | [32,40,48,51,66,98,138,140] | ||
| Literacy and skill in technology | [27,31,32,43,44,58,66,77,98,100,107,138,140] | ||
| EHR/PHR system | |||
| Poor system integration and interoperability | [44,47,48,51,56,61,93,98,133,138,140] | ||
| Lack of trust and belief in EHRs/PHRs | [43,58,66,86,92,93,98,114,123,138,140] | ||
| System quality | [29,32,38,39,40,43,45,48,61,77,98,100,128,138] | ||
| Data and information | |||
| Privacy and security of data | [27,31,32,35,43,48,77,93,98,100,112,129,138,140,150] | ||
| Data quality and accuracy | [31,35,77,100,107,138] | ||
| Other concerns | [35,56] | ||
| Others | |||
| Resource constraints | [27,29,38,39,44,47,48,77,93,100,128,140,157] | ||
| Legal liability | [43,150] | ||
| Low awareness | [32,107,129,140] | ||
| Lack of policy support | [98,140] | ||
| No major barrier | [95] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.H.; Eghdam, A.; Davoody, N.; Wright, G.; Flowerday, S.; Koch, S. Effects of Electronic Health Record Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content. Life 2020, 10, 327. https://doi.org/10.3390/life10120327
Tsai CH, Eghdam A, Davoody N, Wright G, Flowerday S, Koch S. Effects of Electronic Health Record Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content. Life. 2020; 10(12):327. https://doi.org/10.3390/life10120327
Chicago/Turabian StyleTsai, Chen Hsi, Aboozar Eghdam, Nadia Davoody, Graham Wright, Stephen Flowerday, and Sabine Koch. 2020. "Effects of Electronic Health Record Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content" Life 10, no. 12: 327. https://doi.org/10.3390/life10120327