Rapidly Progressive Pauci-Immune Glomerulonephritis with Aberrant Fibrinoid Necrosis Associated with Atezolizumab, an Immune Check Point Inhibitor: A Case Report and Review of Literature

 ,
,
Abstract
:1. Introduction
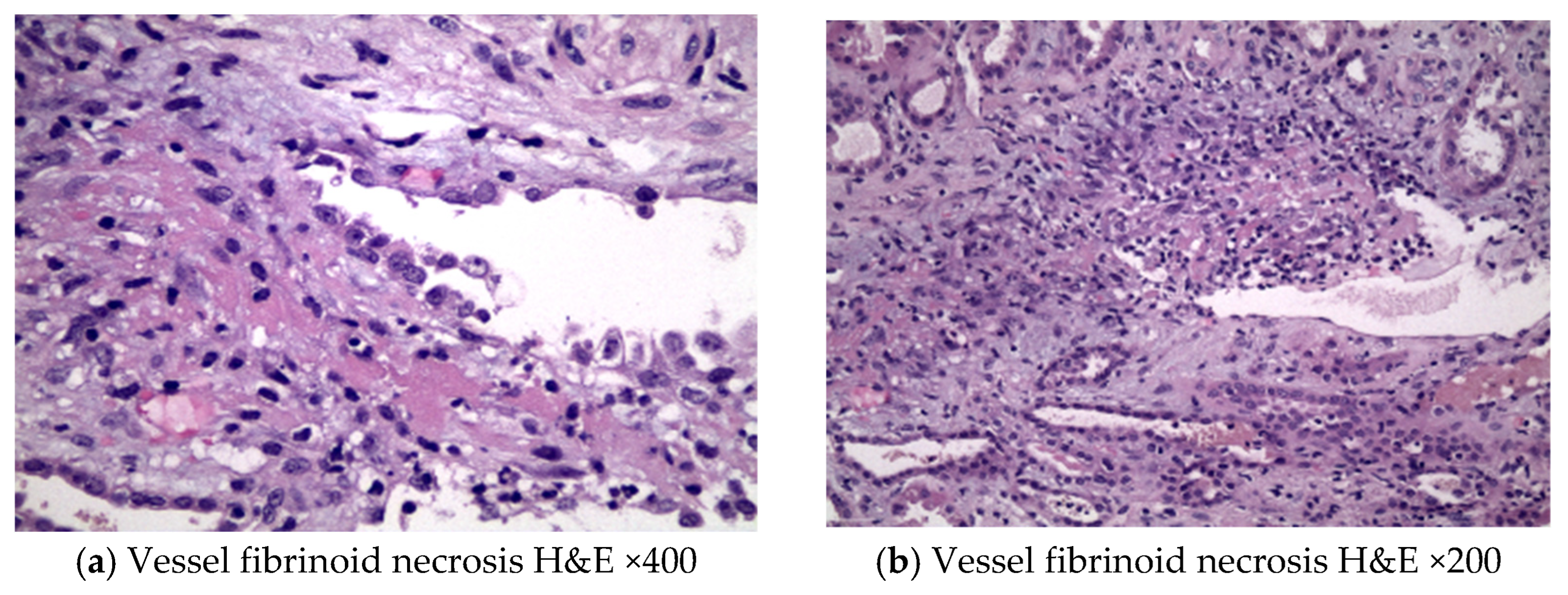
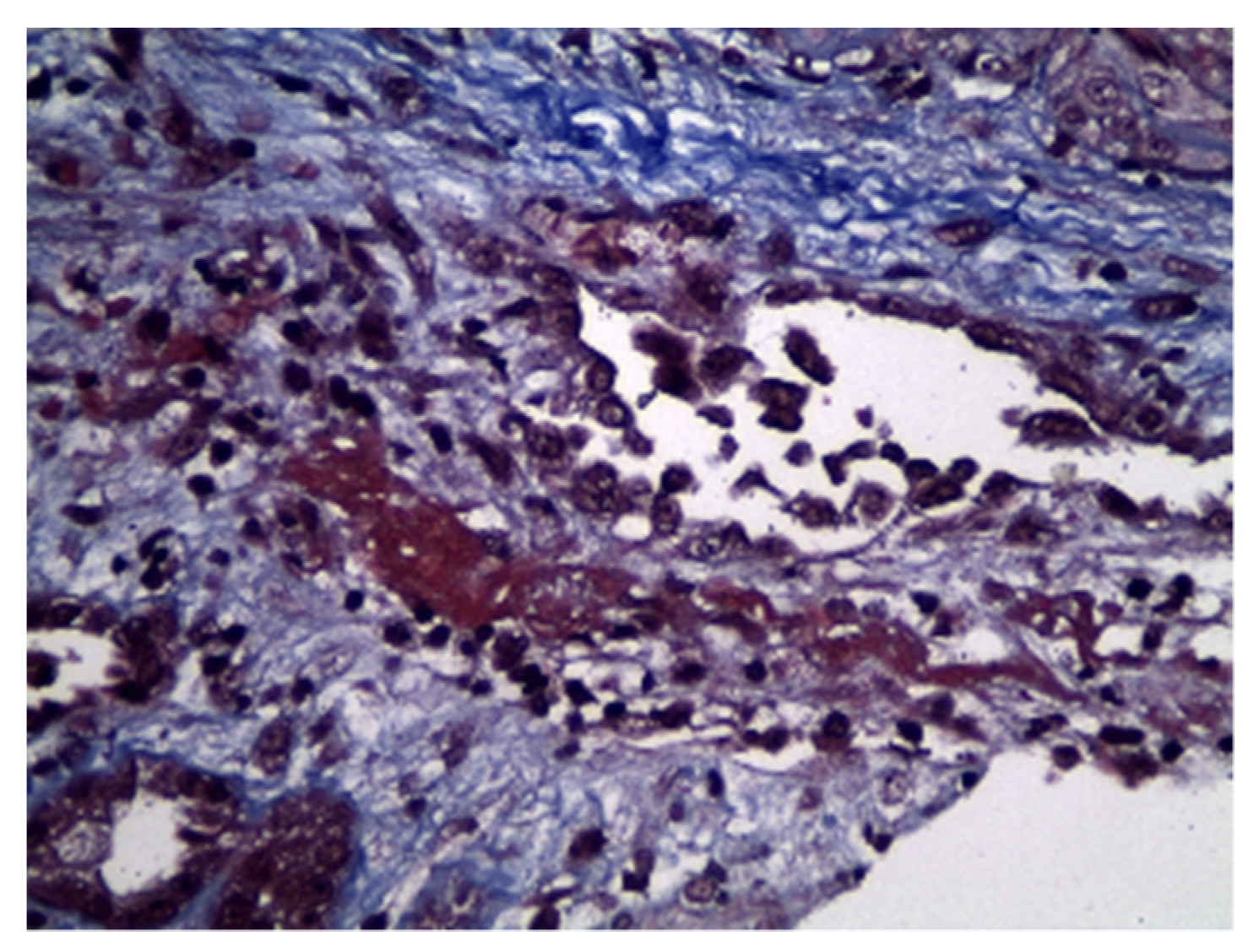
2. Case Description
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weber, J.; Mandalà, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dine, J.; Gordon, R.; Shames, Y.; Kasler, M.K.; Barton-Burke, M. Immune checkpoint inhibitors: An innovation in immunotherapy for the treatment and management of patients with cancer. Asia Pac. J. Oncol. Nurs. 2017, 4, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Abdel-Rahman, O.; Fouad, M. Risk of pneumonitis in cancer patients treated with immune checkpoint inhibitors: A me-ta-analysis. Ther. Adv. Respir. Dis. 2016, 10, 183–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xipell, M.; Victoria, I.; Hoffmann, V.; Villarreal, J.; Garcia-Herrera, A.; Reig, O.; Rodas, L.; Blasco, M.; Poch, E.; Mellado, B.; et al. Acute tubulointerstitial nephritis associated with atezolizumab, an anti-programmed death-ligand 1 (pd-l1) antibody therapy. Oncoimmunology 2018, 7, e1445952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haanen, J.B.A.G.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K. Management of toxicities from Immunotherapy. Ann. Oncol. 2017, 28 (Suppl. S4), i119–i142. [Google Scholar] [CrossRef]
- Inman, B.A.; Longo, T.A.; Ramalingam, S.; Harrison, M.R. Atezolizumab: A PD-L1–Blocking Antibody for Bladder Cancer. Clin. Cancer Res. 2017, 23, 1886–1890. [Google Scholar] [CrossRef] [Green Version]
- Deng, R.; Bumbaca, D.; Pastuskovas, C.V.; Boswell, C.A.; West, D.; Cowan, K.J.; Chiu, H.; McBride, J.; Johnson, C.; Xin, Y.; et al. Preclinical pharmacokinetics, pharmacodynamics, tissue distribution, and tu-mor penetration of anti-PD-L1 monoclonal antibody, an immune checkpoint inhibitor. MAbs 2016, 8, 593–603. [Google Scholar] [CrossRef] [Green Version]
- Hahn, A.W.; Gill, D.M.; Agarwal, N.; Maughan, B.L. PD-1 checkpoint inhibition: Toxicities and management. Urol. Oncol. Semin. Orig. Investig. 2017, 35, 701–707. [Google Scholar] [CrossRef]
- Hagerty, D.T.; Allen, P.M. Processing and presentation of self and foreign antigens by the renal proximal tubule. J. Immunol. 1992, 148, 2324–2330. [Google Scholar] [CrossRef] [PubMed]
- Menke, J.; Lucas, J.A.; Zeller, G.C.; Keir, M.E.; Huang, X.R.; Tsuboi, N.; Mayadas, T.N.; Lan, H.Y.; Sharpe, A.H.; Kelley, V.R. Programmed Death 1 Ligand (PD-L) 1 and PD-L2 Limit Autoimmune Kidney Disease: Distinct Roles. J. Immunol. 2007, 179, 7466–7477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, A.; Watanabe, M.; Nawata, A.; Ikari, Y.; Sasaki, M.; Shigemoto, K.; Hisano, S.; Nakashima, H. Tubulointerstitial nephritis as adverse effect of programmed cell death 1 inhibitor, nivolumab, showed distinct histological findings. CEN Case Rep. 2017, 6, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Izzedine, H.; Mateus, C.; Boutros, C.; Robert, C.; Rouvier, P.; Amoura, Z.; Mathian, A. Renal effects of immune checkpoint inhibitors. Nephrol. Dial. Transplant. 2017, 32, 936–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortazar, F.B.; Marrone, K.A.; Troxell, M.L.; Ralto, K.M.; Hoenig, M.P.; Brahmer, J.R.; Le, D.T.; Lipson, E.J.; Glezerman, I.G.; Wolchok, J.; et al. Clinicopathological features of acute kidney injury associated with immune checkpoint inhibitors. Kidney Int. 2016, 90, 638–647. [Google Scholar] [CrossRef] [Green Version]
- Baxi, S.; Yang, A.; Gennarelli, R.L.; Khan, N.; Wang, Z.; Boyce, L.; Korenstein, D. Immune-related adverse events for anti-PD-1 and anti-PD-L1 drugs: Systematic review and meta-analysis. BMJ 2018, 360, k793. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.F.; Chen, Y.; Song, S.Y.; Wang, T.J.; Ji, W.J.; Li, S.W.; Liu, N.; Yan, C.X. Immune-related adverse events associated with anti-PD-1/PD-L1 treatment for malignan-cies: A meta-analysis. Front. Pharmacol. 2017, 8, 730. [Google Scholar] [CrossRef] [PubMed]
- Mamlouk, O.; Selamet, U.; Machado, S.; Abdelrahim, M.; Glass, W.F.; Tchakarov, A.; Gaber, L.; Lahoti, A.; Workeneh, B.; Chen, S. Nephrotoxicity of immune checkpoint inhibitors beyond tubulointerstitial nephritis: Single-center experience. J. Immunother. Cancer 2019, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Xu, J.; Bai, Y.; Zhang, S.; Cheng, M.; Jin, J. Nephrotoxicity in patients with solid tumors treated with anti-PD-1/PD-L1 monoclonal antibodies: A systematic review and meta-analysis. Investig. New Drugs 2021, 39, 860–870. [Google Scholar] [CrossRef]
- Gallan, A.J.; Alexander, E.; Reid, P.; Kutuby, F.; Chang, A.; Henriksen, K.J. Renal Vasculitis and Pauci-immune Glomerulonephritis Associated With Immune Checkpoint Inhibitors. Am. J. Kidney Dis. 2019, 74, 853–856. [Google Scholar] [CrossRef]
- Cho, J.; Kim, H.S.; Ku, B.M.; Choi, Y.-L.; Cristescu, R.; Han, J.; Sun, J.-M.; Lee, S.-H.; Ahn, J.S.; Park, K.; et al. Pembrolizumab for Patients With Refractory or Relapsed Thymic Epithelial Tumor: An Open-Label Phase II Trial. J. Clin. Oncol. 2019, 37, 2162–2170. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, M.; Dilly, B.; Curie, A.; Hébert, V.; Laurent, C.; Hanoy, M.; Grangé, S.; Guerrot, D.; François, A.; Bertrand, D. Ipilimumab-induced renal granulomatous arteritis: A case report. BMC Nephrol. 2019, 20, 1–5. [Google Scholar] [CrossRef]
- Person, F.; Chahoud-Schriefer, T.; Fehrle, W.; Janneck, M.; Huber, T.B.; Wiech, T. Severe acute kidney injury due to nivolumab/ipilimumab-induced granulo-matosis and fibrinoid vascular necrosis. J. Immunother. 2020, 43, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Heo, M.H.; Kim, H.K.; Lee, H.; Ahn, M.-J. Antineutrophil Cytoplasmic Antibody–Associated Rapid Progressive Glomerulonephritis after Pembrolizumab Treatment in Thymic Epithelial Tumor: A Case Report. J. Thorac. Oncol. 2017, 12, e103–e105. [Google Scholar] [CrossRef] [PubMed]
- Kitchlu, A.; Jhaveri, K.D.; Wadhwani, S.; Deshpande, P.; Harel, Z.; Kishibe, T.; Henriksen, K.; Wanchoo, R. A systematic review of immune checkpoint inhibitor-associated glomerular disease. Kidney Int. Rep. 2020, 6, 66–77. [Google Scholar] [CrossRef]
- Gupta, S.; Cortazar, F.B.; Riella, L.V.; Leaf, D.E. Immune checkpoint inhibitor nephrotoxicity: Update 2020. Kidney360 2020, 1, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Short, S.A.P.; Sise, M.E.; Prosek, J.M.; Madhavan, S.M.; Soler, M.J.; Ostermann, M.; Herrmann, S.M.; Abudayyeh, A.; Anand, S.; et al. ICPi-AKI Consortium Investigators: Acute kidney injury in patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2021, 9, e003467. [Google Scholar] [CrossRef]
- Lee, M.D.; Seethapathy, H.; Strohbehn, I.A.; Zhao, S.H.; Boland, G.M.; Fadden, R.; Sullivan, R.; Reynolds, K.L.; Sise, M.E. Rapid corticosteroid taper versus standard of care for immune checkpoint inhibitor induced nephritis: A single-center retrospective cohort study. J. Immunother. Cancer 2021, 9, e002292. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference, Year | Immune Check Point Received | ANCA Serology | Initial Corticosteroid Therapy | Other Immunosuppressive Treatment | AKI Outcome |
|---|---|---|---|---|---|
| Cortazar et al. [15], 2020 | Nivolumab | Negative | Corticosteroid, NOS | Rituximab | Full |
| Mamlouk et al. [18], 2019 | Nivolumab | Negative | Prednisone 1 mg/kg | Rituximab | Complete |
| Mamlouk et al. [18], 2019 | Ipilimumab plus nivolumab | Negative | Prednisone 1 mg/kg | Rituximab | Complete |
| Mamlouk et al. [18], 2019 | Tremelimumab | NA | Methyl-prednisolone 2 mg/kg | Rituximab | Partial |
| Gallan et al. [20], 2019 | Pembrolizumab | Negative | Pulse steroid, high-dose oral steroid | None | NA |
| Gallan et al. [20], 2019 | Nivolumab | NA | NA | NA | NA |
| Gallan et al. [20], 2019 | Nivolumab | Negative | Corticosteroid, NOS | None | Partial |
| Gallan et al. [20], 2019 | Nivolumab | Negative | Pulse steroid, then oral steroid | IMCgp100 | Complete |
| Cho et al. [21], 2018 | Pembrolizumab | Positive | Corticosteroid, NOS | Cyclophosphamide | Partial |
| Lemoine et al. [22], 2019 | Ipilimumab | Negative | Prednisone 1 mg/kg ×1 month, tapered over 4 weeks | None | Partial |
| Person et al. [23], 2020 | Ipilimumab plus nivolumab | Negative | Methyl-prednisolone 200 mg IV daily | MMF | ESKD |
| Heo et al. [24], 2017 | Pembrolizumab | Positive | Methyl-prednisolone 500 mg IV daily × 3 days, p.o taper | Cyclophosphamide | Partial |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikolopoulos, P.; Liapis, G.; Giannakopoulos, P.; Kotsantis, I.; Drouzas, K.; Lionaki, S. Rapidly Progressive Pauci-Immune Glomerulonephritis with Aberrant Fibrinoid Necrosis Associated with Atezolizumab, an Immune Check Point Inhibitor: A Case Report and Review of Literature. Antibodies 2023, 12, 10. https://doi.org/10.3390/antib12010010
Nikolopoulos P, Liapis G, Giannakopoulos P, Kotsantis I, Drouzas K, Lionaki S. Rapidly Progressive Pauci-Immune Glomerulonephritis with Aberrant Fibrinoid Necrosis Associated with Atezolizumab, an Immune Check Point Inhibitor: A Case Report and Review of Literature. Antibodies. 2023; 12(1):10. https://doi.org/10.3390/antib12010010
Chicago/Turabian StyleNikolopoulos, Petros, George Liapis, Panagiotis Giannakopoulos, Ioannis Kotsantis, Konstantinos Drouzas, and Sophia Lionaki. 2023. "Rapidly Progressive Pauci-Immune Glomerulonephritis with Aberrant Fibrinoid Necrosis Associated with Atezolizumab, an Immune Check Point Inhibitor: A Case Report and Review of Literature" Antibodies 12, no. 1: 10. https://doi.org/10.3390/antib12010010