

The Relationship between Ambient Fine Particulate Matter (PM2.5) Pollution and Depression: An Analysis of Data from 185 Countries

Abstract
:1. Introduction
- (a)
- At least some of these interacting or confounding factors were taken into account;
- (b)
- Individual pollutants were examined individually;
- (c)
- A longitudinal study design was adopted;
- (d)
- Data from low- and middle-income countries, where air pollution is often above acceptable levels, were included.
2. Materials and Methods
- Reliable and recent cross-national data on levels of PM2.5 are available from a reliable source for the years 2010 and 2018 [30].
2.1. Data Sources
2.2. Data Analysis
3. Results
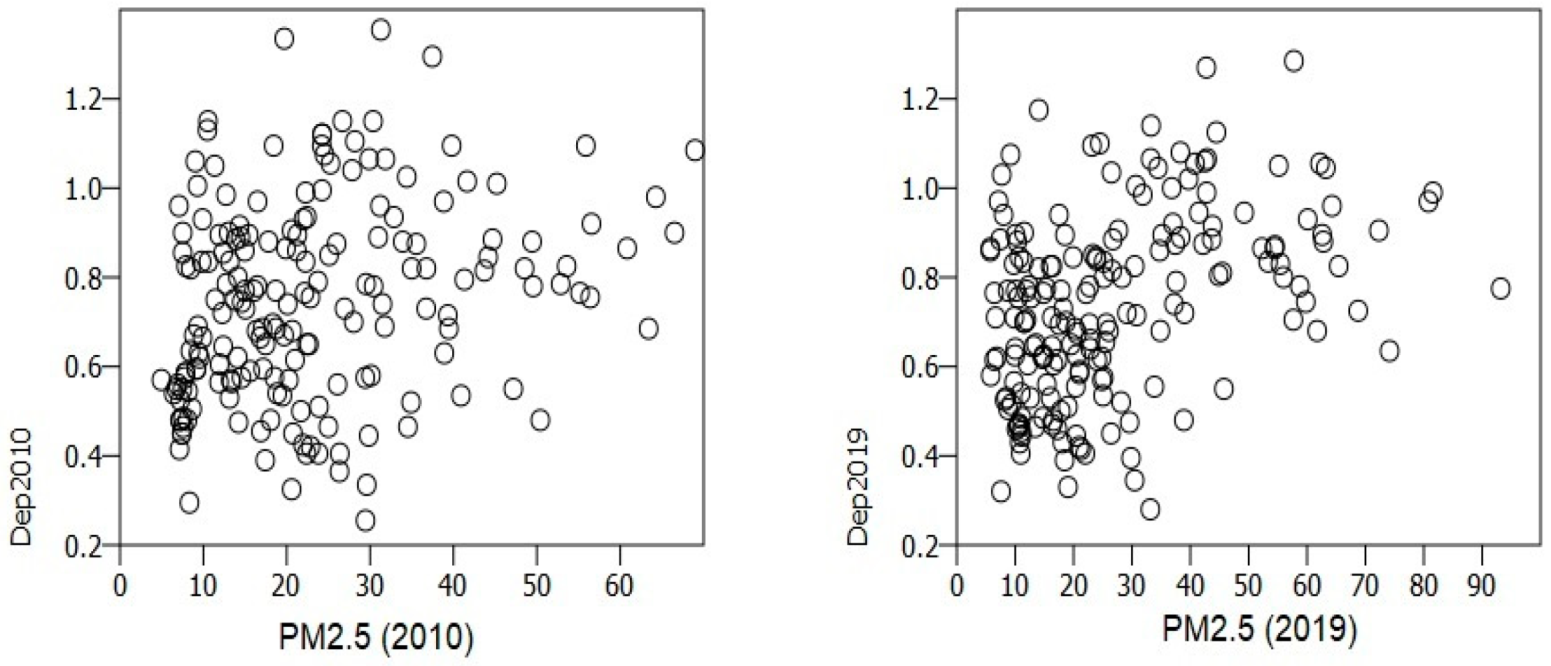
3.1. Bivariate Correlations between PM2.5 and the Incidence of Depression
3.2. Evaluation of a Possible Threshold Effect
3.3. Longitudinal Associations between PM2.5 and the Incidence of Depression
3.3.1. Cross-Lagged Regression
3.3.2. General Linear Model
3.4. Additional Analyses
4. Discussion
5. Conclusions
- There is a cross-sectional, positive correlation between PM2.5 levels and the incidence of depression, but this relationship is of a linear or monotonic nature only to a limited extent, and was weakened after correcting for possible confounders;
- The strength of the association between PM2.5 and depression increased over time in countries with a PM2.5 level above the WHO-recommended threshold of 15 µg/m3; these countries also experienced a significant increase in PM2.5 levels over the study period;
- On the other hand, in countries with a PM2.5 level below this threshold, the relationship between PM2.5 and depression weakened over time; these countries showed a slight but significant reduction in PM2.5 over the study period;
- Linear methods of analysis did not reveal a clear-cut longitudinal relationship between PM2.5 levels; however, these results should be interpreted in light of the preceding three findings.
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.M.; Adams, M.J.; Clarke, T.; Hafferty, J.D.; Gibson, J.; Shirali, M.; Coleman, J.R.I.; Hagenaars, S.P.; Ward, J.; Wigmore, E.M.; et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat. Neurosci. 2019, 22, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, A.E.; Munafo, M.R. Triangulating meta-analyses: The example of the serotonin transporter gene, stressful life events and major depression. BMC Psychol. 2016, 4, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristobal-Narvaez, P.; Haro, J.M.; Koyanagi, A. Perceived stress and depression in 45 low- and middle-income countries. J. Affect. Disord. 2020, 274, 799–805. [Google Scholar] [CrossRef]
- Bakusic, J.; Schaufeli, W.; Claes, S.; Godderis, L. Stress, burnout and depression: A systematic review on DNA methylation mechanisms. J. Psychosom. Res. 2017, 92, 34–44. [Google Scholar] [CrossRef]
- Rautio, N.; Filatova, S.; Lehtiniemi, H.; Miettunen, J. Living environment and its relationship to depressive mood: A systematic review. Int. J. Soc. Psychiatry 2018, 64, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Latham, R.M.; Kieling, C.; Arseneault, L.; Rocha, T.B.; Beddows, A.; Beevers, S.D.; Danese, A.; De Oliveira, K.; Kohrt, B.A.; Moffitt, T.E.; et al. Childhood exposure to ambient air pollution and predicting individual risk of depression onset in UK adolescents. J. Psychiatr. Res. 2021, 138, 60–67. [Google Scholar] [CrossRef]
- Gladka, A.; Zatonski, T.; Rymaszewska, J. Association between the long-term exposure to air pollution and depression. Adv. Clin. Exp. Med. 2022, 31, 1139–1152. [Google Scholar] [CrossRef]
- Khosrorad, R.; Aval, H.E.; Najafi, M.L.; Rezai, H.; Dovlatabadi, A.; Estiri, E.H.; Hesari, M.H.; Behmanesh, M.; Miri, M. The association of exposure to air pollution and depression in women: A cross-sectional study of a middle-income country. Environ. Res. 2022, 215, 114266. [Google Scholar] [CrossRef]
- Duan, C.; Li, C.; Xu, J.; He, Y.; Xu, H.; Zhang, D.; Yang, J.; Yu, J.; Zeng, W.; Wang, Y.; et al. Association between prenatal exposure to ambient air pollutants and postpartum depressive symptoms: A multi-city cohort study. Environ. Res. 2022, 209, 112786. [Google Scholar] [CrossRef]
- Bastain, T.M.; Chavez, T.; Habre, R.; Hernandez-Castro, I.; Grubbs, B.; Toledo-Corral, C.M.; Farzan, S.F.; Lurvey, N.; Lerner, D.; Eckel, S.P.; et al. Prenatal ambient air pollution and maternal depression at 12 months postpartum in the MADRES pregnancy cohort. Environ. Health 2021, 20, 121. [Google Scholar] [CrossRef]
- Wu, M.; Xie, J.; Zhou, Z.; Wang, L.; Hu, Y.; Sun, Y.; Wang, Y.; Tian, Y. Fine particulate matter, vitamin D, physical activity, and major depressive disorder in elderly adults: Results from UK Biobank. J. Affect. Disord. 2022, 299, 233–238. [Google Scholar] [CrossRef]
- Hwang, I.Y.; Choi, D.; Kim, J.A.; Choi, S.; Chang, J.; Goo, A.J.; Ko, A.; Lee, G.; Kim, K.H.; Son, J.S.; et al. Association of short-term particulate matter exposure with suicide death among major depressive disorder patients: A time-stratified case-crossover analysis. Sci. Rep. 2022, 12, 8471. [Google Scholar] [CrossRef]
- Newbury, J.B.; Stewart, R.; Fisher, H.L.; Beevers, S.; Dajnak, D.; Broadbent, M.; Pritchard, M.; Shiode, N.; Heslin, M.; Hammoud, R.; et al. Association between air pollution exposure and mental health service use among individuals with first presentations of psychotic and mood disorders: Retrospective cohort study. Br. J. Psychiatry 2021, 219, 678–685. [Google Scholar] [CrossRef]
- Vlaanderen, J.; Vermeulen, R.; Whitaker, M.; Chadeau-Hyam, M.; Hottenga, J.; de Geus, E.; Willemsen, G.; Penninx, B.W.J.H.; Jansen, R.; Boomsma, D.I. Impact of long-term exposure to PM2.5 on peripheral blood gene expression pathways involved in cell signaling and immune response. Environ. Int. 2022, 168, 107491. [Google Scholar] [CrossRef]
- Mac Giollabhui, N.; Ng, T.H.; Ellman, L.M.; Alloy, L.B. The longitudinal associations of inflammatory biomarkers and depression revisited: Systematic review, meta-analysis, and meta-regression. Mol. Psychiatry 2021, 26, 3302–3314. [Google Scholar] [CrossRef]
- Gasparini, A.; Callegari, C.; Lucca, G.; Bellini, A.; Caselli, I.; Ielmini, M. Inflammatory biomarker and response to antidepressant in major depressive disorder: A systematic review and meta-analysis. Psychopharmacol. Bull. 2022, 52, 36–52. [Google Scholar]
- Ji, X.; Liu, R.; Guo, J.; Li, Y.; Cheng, W.; Pang, Y.; Zheng, Y.; Zhang, R.; Tang, J. Olfactory bulb microglia activation mediated neuronal death in real-ambient particulate matter exposure mice with depression-like behaviors. Sci. Total Environ. 2022, 821, 153456. [Google Scholar] [CrossRef]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory markers in depression: A meta-analysis of mean differences and variability in 5166 patients and 5083 controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef]
- Li, Z.; Yan, H.; Zhang, X.; Shah, S.; Yang, G.; Chen, Q.; Han, S.; Zhang, D.; Weinberger, D.R.; Yue, W.; et al. Air pollution interacts with genetic risk to influence cortical networks implicated in depression. Proc. Natl. Acad. Sci. USA 2021, 118, e2109310118. [Google Scholar] [CrossRef]
- Fu, Z.; Liu, Q.; Liang, J.; Weng, Z.; Li, W.; Xu, J.; Zhang, X.; Xu, C.; Huang, T.; Gu, A. Air pollution, genetic factors and the risk of depression. Sci. Total Environ. 2022, 850, 158001. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Hoek, G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ. Int. 2020, 143, 105974. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Heinrich, J.; Bloom, M.S.; Zhao, T.; Shi, T.; Feng, W.; Sun, Y.; Shen, J.; Yang, Z.; Yang, B.; et al. Ambient air pollution and depression: A systematic review with meta-analysis up to 2019. Sci. Total Environ. 2020, 701, 134721. [Google Scholar] [CrossRef] [PubMed]
- Borroni, E.; Pesatori, A.C.; Bollati, V.; Buoli, M.; Carugno, M. Air pollution exposure and depression: A comprehensive updated systematic review and meta-analysis. Environ. Pollut. 2022, 292, 118245. [Google Scholar] [CrossRef]
- Petrowski, K.; Buhrer, S.; Strauβ, B.; Decker, O.; Brahler, E. Examining air pollution (PM10), mental health and well-being in a representative German sample. Sci. Rep. 2021, 11, 18436. [Google Scholar] [CrossRef]
- Hu, Q.; Feng, Y.; Xu, M. Are there heterogeneous impacts of air pollution on mental health? Front. Public Health 2022, 9, 780022. [Google Scholar] [CrossRef]
- Kim, H.-J.; Kim, H.-S.; Kim, S.; Hwang, J.; Lee, H.; Park, B.; Kim, B. Effects of vitamin D on associations between air pollution and mental health outcomes in Korean adults: Results from the Korea National Health and Nutrition Examination Survey (KNHANES). J. Affect. Disord. 2023, 320, 390–396. [Google Scholar] [CrossRef]
- Hautekiet, P.; Saenen, N.D.; Demarest, S.; Keune, H.; Pelgrims, I.; Van der Heyden, J.; De Clercq, E.M.; Nawrot, T.S. Air pollution in association with mental and self-rated health and the mediating effect of physical activity. Environ. Health 2022, 21, 29. [Google Scholar] [CrossRef]
- Bergmann, S.; Li, B.; Pilot, E.; Chen, R.; Wang, B.; Yang, J. Effect modification of the short-term effects of air pollution on morbidity by season: A systematic review and meta-analysis. Sci. Total Environ. 2020, 716, 136985. [Google Scholar] [CrossRef]
- SDG Indicator 11.6.2 Concentrations of Fine Particulate Matter (PM2.5). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/concentrations-of-fine-particulate-matter-(pm2-5) (accessed on 25 November 2022).
- Global Burden of Disease Study 2019 (GBD 2019) Data Resources. Available online: https://ghdx.healthdata.org/gbd-2019 (accessed on 26 November 2022).
- Charlson, F.J.; Ferrari, A.J.; Flaxman, A.D.; Whiteford, H.A. The epidemiological modelling of dysthymia: Application for the Global Burden of Disease Study 2010. J. Affect. Disord. 2013, 151, 111–120. [Google Scholar] [CrossRef]
- GNI per Capita, PPP (Current International $)|The World Bank. Available online: https://data.worldbank.org/indicator/NY.GNP.PCAP.PP.CD (accessed on 25 November 2022).
- Average Years of Schooling, 2017|Our World in Data. Available online: https://ourworldindata.org/grapher/mean-years-of-schooling-long-run?tab=table&time=2017..latest (accessed on 26 November 2022).
- Prevalence of Insufficient Physical Activity among Adults Aged 18+ Years (Age-Standardized Estimate) (%). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-insufficient-physical-activity-among-adults-aged-18-years-(age-standardized-estimate)-(-) (accessed on 26 November 2022).
- Countries by Population Density|Countries by Density 2022. Available online: https://worldpopulationreview.com/country-rankings/countries-by-density (accessed on 26 November 2022).
- Hagenau, T.; Vest, R.; Gissel, T.N.; Poulsen, C.S.; Erlandsen, M.; Mosekilde, L.; Vestergaard, P. Global vitamin D levels in relation to age, gender, skin pigmentation and latitude: An ecologic meta-regression analysis. Osteoporos. Int. 2009, 20, 133–140. [Google Scholar] [CrossRef]
- Google Earth. Available online: https://www.google.com/earth/index.html (accessed on 28 November 2022).
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Ambient (Outdoor) Air Pollution|World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 28 November 2022).
- Petscher, Y.; Quinn, J.M.; Wagner, R.K. Modeling the co-development of correlated processes with longitudinal and cross-construct effects. Dev. Psychol. 2016, 52, 1690–1704. [Google Scholar] [CrossRef]
- Gao, X.; Jiang, W.; Liao, J.; Li, J.; Yang, L. Attributable risk and economic cost of hospital admissions for depression due to short-exposure to ambient air pollution: A multi-city time-stratified case-crossover study. J. Affect. Disord. 2022, 304, 150–158. [Google Scholar] [CrossRef]
- Qiu, X.; Shi, L.; Kubzansky, L.D.; Wei, Y.; Castro, E.; Li, H.; Weisskopf, M.G.; Schwartz, J.D. Association of long-term exposure to air pollution with late-life depression in older adults in the U.S. JAMA Netw. Open 2023, 6, e2253668. [Google Scholar] [CrossRef]
- Gao, X.; Jiang, M.; Huang, N.; Guo, X.; Huang, T. Long-term air pollution, genetic susceptibility, and the risk of depression and anxiety: A prospective study in the UK Biobank cohort. Environ. Health Perspect. 2023, 131, 17002. [Google Scholar] [CrossRef]
- Sakhvidi, M.J.Z.; Lafontaine, A.; Lequy, E.; Berr, C.; de Hoogh, K.; Vienneau, D.; Goldberg, M.; Zins, M.; Lemogne, C.; Jacquemin, B. Ambient air pollution exposure and depressive symptoms: Findings from the French CONSTANCES cohort. Environ. Int. 2022, 170, 107622. [Google Scholar] [CrossRef]
- Yao, Y.; Lu, T.; Liu, Y.; Qin, Q.; Jiang, J.; Xiang, H. Association of depressive symptoms with ambient PM2.5 in middle-aged and elderly Chinese adults: A cross-sectional study from the China Health and Retirement Longitudinal Study wave 4. Environ. Res. 2022, 203, 111889. [Google Scholar] [CrossRef]
- Niu, Z.; Zhai, M.; Dong, Y.; Wen, W.; Xue, L.; Aosiman, M.; Qin, W.; Duan, Z. Association between air quality satisfaction, family relationships, and depression symptoms among middle-aged and elderly Chinese people: The mediation role of perceived health status. BMC Public Health 2022, 22, 2439. [Google Scholar] [CrossRef]
- Zhu, Z.; Zhao, Y. Severe air pollution and psychological distress in China: The interactive effects of coping and perceived controllability. Front. Psychol. 2021, 12, 601964. [Google Scholar] [CrossRef]
- Clark, D.A.; Beck, A.T. Cognitive theory and therapy of anxiety and depression: Convergence with neurobiological findings. Trends Cogn. Sci. 2010, 14, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Veronese, N.; Sanchez, G.F.L.; Butler, L.; Barnett, Y.; Shin, J.I.; Lee, S.; Oh, J.W.; Soysal, P.; Oh, H.; et al. The association of cooking fuels with depression and anxiety symptoms among adults aged ≥ 65 years from low- and middle-income countries. J. Affect. Disord. 2022, 311, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhou, Y.; Ding, L. Effects of long-term household air pollution exposure from solid fuel use on depression: Evidence from national longitudinal surveys from 2011 to 2018. Environ. Pollut. 2021, 283, 117350. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Li, X.; Qian, P.; Wu, H. Indoor air pollution from solid fuels use, inflammation, depression and cognitive function in middle-aged and older Chinese adults. J. Affect. Disord. 2022, 319, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Erdsiek, F.; Brzoska, P. Is exposure to secondhand smoke associated with current depression (PHQ-8) among never-smokers? Results from a survey among German adults. BMC Public Health 2020, 20, 1880. [Google Scholar] [CrossRef]
- Noguchi, T.; Nakagawa-Senda, H.; Tamai, Y.; Nishiyama, T.; Watanabe, M.; Hosono, A.; Shibata, K.; Ichikawa, M.; Wakabayashi, R.; Nagaya, K.; et al. Association between second-hand smoke exposure and depressive symptoms among Japanese adults: A cross-sectional study. J. Epidemiol. 2020, 30, 566–573. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Xia, Y.; Cao, L.; Chang, Q.; Zhao, Y. Associations between long term exposure to outdoor air pollution and indoor solid fuel use and depression in China. J. Environ. Manag. 2022, 302, 113982. [Google Scholar] [CrossRef]
- Shi, W.; Li, T.; Zhang, Y.; Sun, Q.; Chen, C.; Wang, J.; Fang, J.; Zhao, F.; Du, P.; Shi, X. Depression and anxiety associated with exposure to fine particulate matter constituents: A cross-sectional study in North China. Environ. Sci. Technol. 2020, 54, 16006–16016. [Google Scholar] [CrossRef]
- Liao, Y.-A.; Garcia-Mondragon, L.; Konac, D.; Liu, X.; Ing, A.; Goldblatt, R.; Yu, L.; Barker, E.D. Nighttime lights, urban features, household poverty, depression, and obesity. Curr. Psychol. 2022, 16, 1–12. [Google Scholar] [CrossRef]
- Hao, G.; Zuo, L.; Xiong, P.; Chen, L.; Liang, X.; Jing, C. Associations of PM2.5 and road traffic noise with mental health: Evidence from UK Biobank. Environ. Res. 2022, 207, 112221. [Google Scholar] [CrossRef]
- Wei, F.; Wu, M.; Qian, S.; Li, D.; Jin, M.; Wang, J.; Shui, L.; Lin, H.; Tang, M.; Chen, K. Association between short-term exposure to ambient air pollution and hospital visits for depression in China. Sci. Total Environ. 2020, 724, 138207. [Google Scholar] [CrossRef]
- Wang, R.; Liu, Y.; Xue, D.; Yao, Y.; Liu, P.; Helbich, M. Cross-sectional associations between long-term exposure to particulate matter and depression in China: The mediating effects of sunlight, physical activity, and neighborly reciprocity. J. Affect. Disord. 2019, 249, 8–14. [Google Scholar] [CrossRef]
- Kim, S.Y.; Bang, M.; Wee, J.H.; Min, C.; Yoo, D.M.; Han, S.-M.; Kim, S.; Choi, H.G. Short- and long-term exposure to air pollution and lack of sunlight are associated with an increased risk of depression: A nested case-control study using meteorological data and national sample cohort data. Sci. Total Environ. 2021, 757, 143960. [Google Scholar] [CrossRef]
- Hu, J.; Liu, Y.; Ma, Y.; Gao, M.; Wan, N.; Li, L.; Liu, B.; Wen, D. Sweet foods dietary pattern enhances negative associations of perceived indoor air quality during pregnancy with postpartum depression. Indoor Air 2022, 32, e13124. [Google Scholar] [CrossRef]
- Sampson, L.; Ettman, C.K.; Galea, S. Urbanization, urbanicity, and depression: A review of the recent global literature. Curr. Opin. Psychiatry 2020, 33, 233–244. [Google Scholar] [CrossRef]
- Lin, H.; Guo, Y.; Kowal, P.; Airihenbuwa, C.O.; Di, Q.; Zheng, Y.; Zhao, X.; Vaughn, M.G.; Howard, S.; Schootman, M.; et al. Exposure to air pollution and tobacco smoking and their combined effects on depression in six low- and middle-income countries. Br. J. Psychiatry 2017, 211, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Dores, A.K.; Fick, G.H.; MacMaster, F.P.; Williams, J.V.A.; Bulloch, A.G.M.; Patten, S.B. Outdoor air pollution and depression in Canada: A population-based cross-sectional study from 2011 to 2016. Int. J. Environ. Res. Public Health 2021, 18, 2450. [Google Scholar] [CrossRef]
- Kocot, K.; Zejda, J.E. The relationship between ambient air pollution and life expectancy—An ecological fallacy revisited. Przegl. Epidemiol. 2022, 76, 58–66. [Google Scholar] [CrossRef]
- Brhlikova, P.; Pollock, A.M.; Manners, R. Global Burden of Disease estimates of depression—How reliable is the epidemiological evidence. J. R. Soc. Med. 2011, 104, 25–35. [Google Scholar] [CrossRef] [Green Version]
- Braithwaite, I.; Zhang, S.; Kirkbride, J.B.; Osborn, D.P.J.; Hayes, J.F. Air pollution (particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: A systematic review and meta-analysis. Environ. Health Perspect. 2019, 127, 126002. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Liu, X.; Luo, Z.; Wang, Y.; Fan, K.; Tu, R.; Wu, X.; Chen, G.; Hou, J.; Mao, Z.; et al. Long-term exposure to ambient PM1 strengthened the association of depression/anxiety symptoms with poor sleep quality: The Henan Rural Cohort study. Ecotoxicol. Environ. Saf. 2021, 211, 111932. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.-M.; Malig, B.J.; Basu, R. The association between ozone and fine particles and mental health-related emergency department visits in California, 2005–2013. PLoS ONE 2021, 16, e0249675. [Google Scholar] [CrossRef] [PubMed]
- Jorcano, A.; Lubczynska, M.J.; Pierotti, L.; Altug, H.; Ballester, F.; Cesaroni, G.; El Marroun, H.; Fernandez-Somoano, A.; Freire, C.; Hanke, W.; et al. Prenatal and postnatal exposure to air pollution and emotional and aggressive symptoms in children from 8 European birth cohorts. Environ. Int. 2019, 131, 104927. [Google Scholar] [CrossRef] [PubMed]
- Allaouat, S.; Yli-Tuomi, T.; Tiitanen, P.; Turunen, A.W.; Siponen, T.; Kukkonen, J.; Kangas, L.; Kauhaniemi, M.; Aarnio, M.; Ngandu, T.; et al. Long-term exposure to ambient fine particulate matter originating from traffic and residential wood combustion and the prevalence of depression. J. Epidemiol. Community Health 2021, 75, 1111–1116. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Rationale for Inclusion | Data Source |
|---|---|---|
| Gross national income (GNI) per capita | Income levels may mediate the link between air pollution and mental health [26] | World Bank database [33] |
| Average years of education per adult | Within income groups, education may influence the link between air pollution and depression [26] | Our World in Data [34] |
| Prevalence of insufficient physical activity in adults (%) | Physical activity may moderate the impact of air pollution on depression [27] | WHO Global Health Observatory [35] |
| Population density | Population density may influence the links between air pollution and mental health [26] | World Population Review [36] |
| Distance from the equator (absolute value of the latitude) | Climatic conditions can influence the impact of air pollution, and may also influence vitamin D levels [29,37] | Google Earth [38] |
| Variable | Correlation with PM2.5 Levels, 2010 | Correlation with PM2.5 Levels, 2019 |
|---|---|---|
| Depression, incidence (unadjusted) | ||
| Total Male Female | 0.28 (<0.001) 0.27 (<0.001) 0.27 (<0.001) | 0.37 (<0.001) 0.40 (<0.001) 0.32 (<0.001) |
| Depression, incidence (adjusted) * | ||
| Total Male Female | 0.21 (0.011) 0.21 (0.011) 0.19 (0.020) | 0.33 (<0.001) 0.34 (<0.001) 0.29 (<0.001) |
| Variable | Correlation with PM2.5 Levels, 2010 | Correlation with PM2.5 Levels, 2019 |
|---|---|---|
| Depression, incidence (2010) | ||
| Total Male Female | 0.22 (0.015) 0.21 (0.025) 0.21 (0.019) | 0.38 (0.002) 0.39 (0.001) 0.35 (0.005) |
| Depression, incidence (2019) | ||
| Total Male Female | 0.48 (<0.001) 0.48 (<0.001) 0.43 (<0.001) | −0.13 (0.318) −0.16 (0.238) −0.11 (0.400) |
| Variable | Correlation with PM2.5 Levels, 2010 | Correlation with PM2.5 Levels, 2019 | Cross-Lagged Regression Coefficient | Significance Level |
|---|---|---|---|---|
| Depression, incidence (%) | ||||
| Total Male Female | 0.29 (<0.001) 0.28 (<0.001) 0.27 (<0.001) | 0.34 (<0.001) 0.37 (<0.001) 0.30 (<0.001) | −0.051 −0.061 −0.018 | 0.491 0.409 0.807 |
| Depression, incidence (%) * | ||||
| Total Male Female | 0.23 (0.006) 0.23 (0.005) 0.21 (0.013) | 0.30 (<0.001) 0.31 (<0.001) 0.26 (0.001) | −0.068 −0.049 −0.055 | 0.357 0.507 0.457 |
| Variable | Test Statistic (F) | Significance Level |
|---|---|---|
| Depression, total Depression, total × PM2.5 Depression, male Depression, male × PM2.5 Depression, female Depression, female × PM2.5 | 6.66 0.26 7.76 0.03 4.95 0.49 | 0.011 0.610 0.006 0.986 0.027 0.483 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajkumar, R.P. The Relationship between Ambient Fine Particulate Matter (PM2.5) Pollution and Depression: An Analysis of Data from 185 Countries. Atmosphere 2023, 14, 597. https://doi.org/10.3390/atmos14030597
Rajkumar RP. The Relationship between Ambient Fine Particulate Matter (PM2.5) Pollution and Depression: An Analysis of Data from 185 Countries. Atmosphere. 2023; 14(3):597. https://doi.org/10.3390/atmos14030597
Chicago/Turabian StyleRajkumar, Ravi Philip. 2023. "The Relationship between Ambient Fine Particulate Matter (PM2.5) Pollution and Depression: An Analysis of Data from 185 Countries" Atmosphere 14, no. 3: 597. https://doi.org/10.3390/atmos14030597