

Air Pollution and Tear Lactoferrin among Dry Eye Disease Modifications by Stress and Allergy: A Case–Control Study of Taxi Drivers

Abstract
:1. Introduction
2. Materials and Methods
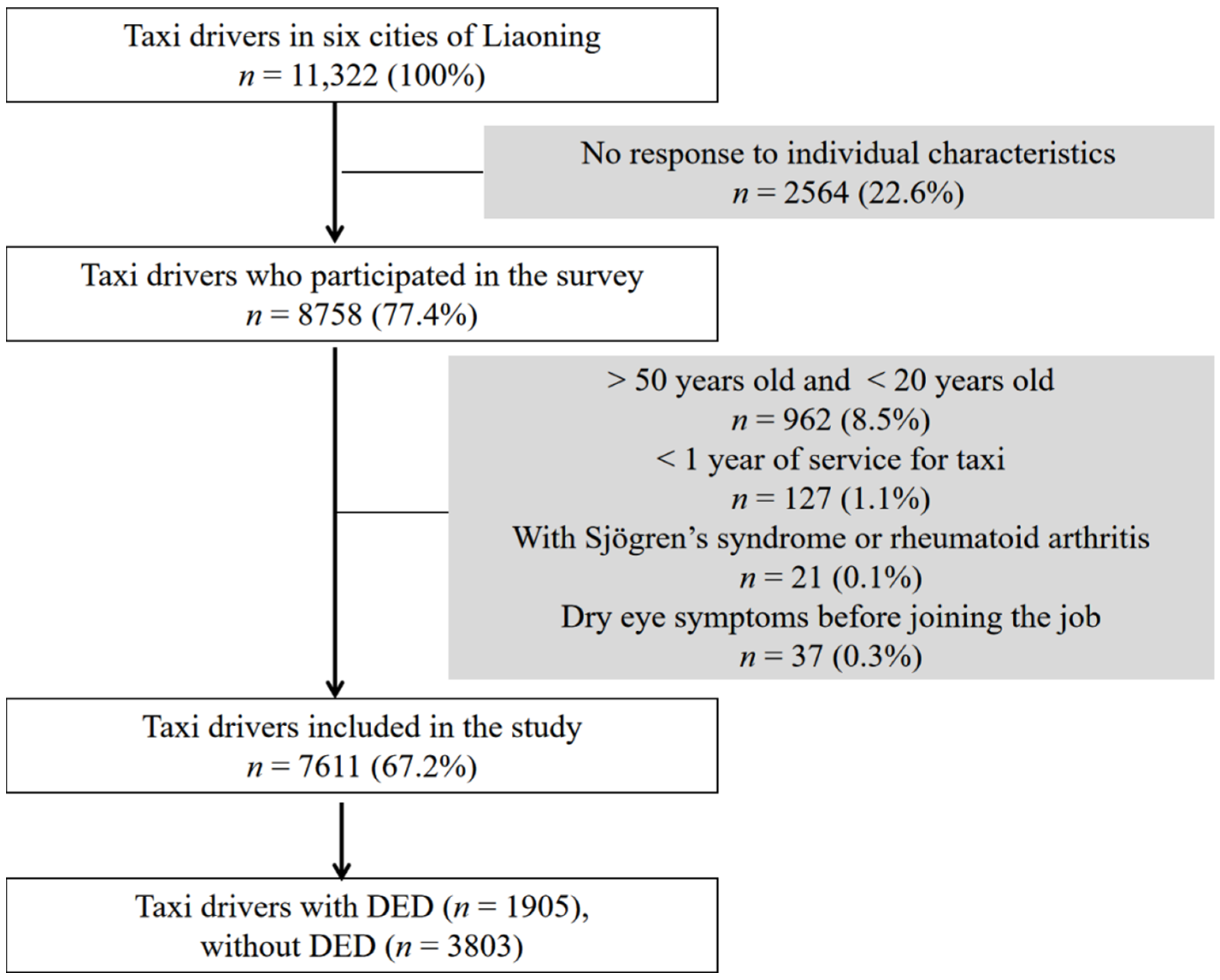
2.1. Study Participants
2.2. Air Pollution Exposure Assessment
2.3. Covariates
2.4. Statistical Analysis
3. Results
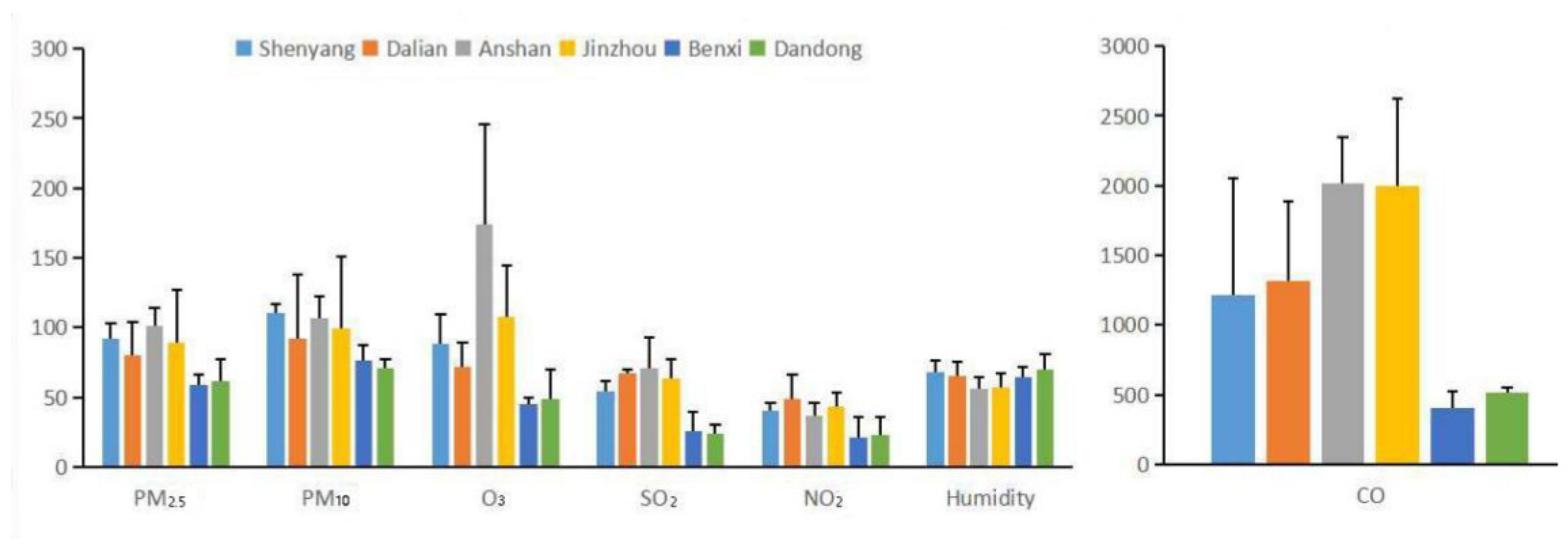
3.1. Characteristics of the Subjects Exposed to Air Pollution
3.2. The Relationship between PM10, NO2, Humidity and DED
3.3. Associations between Tear Lf and PM10, NO2, Humidity
4. Discussion
4.1. Model Performance
4.2. PM10 or NO2 and Lower Humidity Were Risk Factors for DED
4.3. Stress or Allergies Increased the Risks of PM10, NO2 Exposure or Low Humidity on DED
4.4. Tear Lf Has Inverse Associations with PM10, NO2, and Low Humidity
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holgate, S.T.; Samet, J.M.; Koren, H.S.; Maynard, R.L. (Eds.) Air Pollution and Health; Academic Press: London, UK, 1999. [Google Scholar]
- Pu, S.; Shao, Z.; Fang, M.; Yang, L.; Liu, R.; Bi, J.; Ma, Z. Spatial distribution of the public’s risk perception for air pollution: A nationwide study in China. Sci. Total Environ. 2018, 655, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Zheng, H.; Wang, S.; Smith, K.R.; Lu, X.; Aunan, K.; Gu, Y.; Wang, Y.; Ding, D.; Xing, J.; et al. Change in household fuels dominates the decrease in PM2.5 exposure and premature mortality in China in 2005–2015. Proc. Natl. Acad. Sci. USA 2018, 115, 12401–12406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Guan, P.; Cheng, C. Paying more attention on keeping eye health in dust-haze weather in China. Environ. Pollut. 2017, 231, 1211. [Google Scholar] [CrossRef] [PubMed]
- Hessen, M.; Akpek, E.K. Dry eye: An inflammatory ocular disease. J. Ophthalmic Vis. Res. 2014, 9, 240–250. [Google Scholar] [PubMed]
- Liu, N.N.; Liu, L.; Li, J.; Sun, Y.Z. Prevalence of and risk factors for dry eye symptom in mainland China: A systematic review and meta-analysis. J. Ophthalmol. 2014, 2014, 748654. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.F.; Hong, J.X.; Mu, Z.; Peng, L.; Zhou, J.; Yang, D.D.; Xu, J.M. Acute effects of meteorological environmental factors on dry eyes. In Proceedings of the 31th Annual Meeting of China Meteorological Society, Beijing, China, 3 November 2014. [Google Scholar]
- Hwang, S.H.; Choi, Y.H.; Paik, H.J.; Wee, W.R.; Kim, M.K.; Kim, D.H. Potential importance of ozone in the association between outdoor air pollution and dry eye disease in South Korea. JAMA Ophthalmol. 2016, 134, 503–510. [Google Scholar] [CrossRef] [Green Version]
- Caffery, B.E.; Josephson, J.E. Corneal staining after sequential instillations of fluorescein over 30 days. Optom. Vis. Sci. 1991, 68, 467–469. [Google Scholar] [CrossRef]
- Jung, S.J.; Mehta, J.S.; Tong, L. Effects of environment pollution on the ocular surface. Ocul. Surf. 2018, 16, 198–205. [Google Scholar] [CrossRef]
- Ponzin, E.; Scotti, L.; Grandori, R.; Tavazzi, S.; Zambon, A. Lactoferrin concentration in human tears and ocular diseases: A meta-analysis. Investig. Ophthalmol. Vis. Sci. 2020, 61, 9. [Google Scholar] [CrossRef]
- Lemp, M.A. Report of the national eye institute/industry workshop on clinical trials in dry eyes. CLAO J. 1995, 21, 221–232. [Google Scholar]
- Kangari, H.; Eftekhari, M.H.; Sardari, S.; Hashemi, H.; Salamzadeh, J.; Ghassemi-Broumand, M.; Khabazkhoob, M. Short-term consumption of oral omega-3 and dry eye syndrome. Ophthalmology 2013, 120, 2191–2196. [Google Scholar] [CrossRef]
- Bhargava, R.; Kumar, P.; Phogat, H.; Kaur, A.; Kumar, M. Oral omega-3 fatty acids treatment in computer vision syndrome related dry eye. Cont. Lens Anterior Eye 2015, 38, 206–210. [Google Scholar] [CrossRef]
- Hetherington, S.V.; Spitznagel, J.K.; Quie, P.G. An enzyme-linked immunoassay (ELISA) for measurement of lactoferrin. J. Immunol. Methods 1983, 65, 183–190. [Google Scholar] [CrossRef]
- Dong, G.H.; Wang, J.; Zeng, X.W.; Chen, L.; Qin, X.D.; Zhou, Y.; Li, M.; Yang, M.; Zhao, Y.; Ren, W.H.; et al. Interactions between air pollution and obesity on blood pressure and hypertension in Chinese children. Epidemiology 2015, 26, 740–747. [Google Scholar] [CrossRef]
- Cho, J.J.; Kim, J.Y.; Chang, S.J.; Fiedler, N.; Koh, S.B.; Crabtree, B.F.; Kang, D.M.; Kim, Y.K.; Choi, Y.H. Occupational stress and depression in Korean employees. Int. Arch. Occup. Environ. Health 2008, 82, 47–57. [Google Scholar] [CrossRef]
- Hammen, C. Generation of stress in the course of unipolar depression. J. Abnorm. Psychol. 1991, 100, 555–561. [Google Scholar] [CrossRef]
- Malerbi, F.K.; Martins, L.C.; Saldiva, P.H.; Braga, A.L. Ambient levels of air pollution induce clinical worsening of blepharitis. Environ. Res. 2012, 112, 199–203. [Google Scholar] [CrossRef]
- Mo, Z.; Fu, Q.; Lyu, D.; Zhang, L.; Qin, Z.; Tang, Q.; Yin, H.; Xu, P.; Wu, L.; Wang, X.; et al. Impacts of air pollution on dry eye disease among residents in Hangzhou, China: A case-crossover study. Environ. Pollut. 2019, 246, 183–189. [Google Scholar] [CrossRef]
- Song, C.; Wu, L.; Xie, Y.; He, J.; Chen, X.; Wang, T.; Lin, Y.; Jin, T.; Wang, A.; Liu, Y.; et al. Air pollution in China: Status and spatiotemporal variations. Environ. Pollut. 2017, 227, 334–347. [Google Scholar] [CrossRef]
- Torricelli, A.A.; Novaes, P.; Matsuda, M.; Braga, A.; Saldiva, P.H.; Alves, M.R.; Monteiro, M.L. Correlation between signs and symptoms of ocular surface dysfunction and tear osmolarity with ambient levels of air pollution in a large metropolitan area. Cornea 2013, 32, e11–e15. [Google Scholar] [CrossRef]
- Deng, X.; Zhang, F.; Rui, W.; Long, F.; Wang, L.; Feng, Z.; Chen, D.; Ding, W. PM2.5-induced oxidative stress triggers autophagy in human lung epithelial A549 cells. Toxicol. In Vitro 2013, 27, 1762–1770. [Google Scholar] [CrossRef] [PubMed]
- Leung, P.Y.; Wan, H.T.; Billah, M.B.; Cao, J.J.; Ho, K.F.; Wong, C.K.C. Chemical and biological characterization of air particulate matter 2.5, collected from five cities in China. Environ. Pollut. 2014, 194, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Liu, G.; Zhang, H.; Hu, R.; Wang, X. Similarities and differences in PM10 and PM2.5 concentrations, chemical compositions and sources in Hefei City, China. Chemosphere 2019, 220, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Burki, T. WHO introduces ambitious new air quality guidelines. Lancet 2021, 398, 1117. [Google Scholar] [CrossRef] [PubMed]
- US EPA. Final Assessment: Integrated Science Assessment for Carbon Monoxide. US Patent EPA/600/R-09/019F, 29 January 2010. [Google Scholar]
- Resch, H.; Zawinka, C.; Weigert, G.; Schmetterer, L.; Garhöfer, G. Inhaled carbon monoxide increases retinal and choroidal blood flow in healthy humans. Investig. Ophthalmol. Vis. Sci. 2005, 46, 4275–4280. [Google Scholar] [CrossRef]
- Berg, E.J.; Ying, G.S.; Maguire, M.G.; Sheffield, P.E.; Szczotka-Flynn, L.B.; Asbell, P.A.; Shen, J.F.; DREAM, Study Research Group. Climatic and environmental correlates of dry eye disease severity: A report from the dry eye assessment and management (DREAM) study. Transl. Vis. Sci. Technol. 2020, 9, 25. [Google Scholar] [CrossRef]
- Leonardi, A.; Lanier, B. Urban eye allergy syndrome: A new clinical entity? Curr. Med. Res. Opin. 2008, 24, 2295–2302. [Google Scholar] [CrossRef]
- Novaes, P.; Saldiva, P.H.; Matsuda, M.; Macchione, M.; Rangel, M.P.; Kara-José, N.; Berra, A. The effects of chronic exposure to traffic derived air pollution on the ocular surface. Environ. Res. 2010, 110, 372–374. [Google Scholar] [CrossRef]
- Smith, D.W.; Gamble, K.R.; Heil, T.A. A novel psychophysical method for estimating the time course of olfactory rapid adaptation in humans. Chem. Senses 2010, 35, 717–725. [Google Scholar] [CrossRef] [Green Version]
- Clapp, L.J.; Jenkin, M.E. Analysis of the relationship between ambient levels of O3, NO2 and NO as a function of NOx in the UK. Atmos. Environ. 2001, 35, 6391–6405. [Google Scholar] [CrossRef]
- Jerrett, M.; Arain, A.; Kanaroglou, P.; Beckerman, B.; Potoglou, D.; Sahsuvaroglu, T.; Morrison, J.; Giovis, C. A review and evaluation of intraurban air pollution exposure models. J. Expo. Anal. Environ. Epidemiol. 2005, 15, 185–204. [Google Scholar] [CrossRef]
- Zhong, J.Y.; Lee, Y.C.; Hsieh, C.J.; Tseng, C.C.; Yiin, L.M. Association between dry eye disease, air pollution and weather changes in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 2269. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Air Quality Guidelines: Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide; World Health Organization: Geneva, Switzerland, 2006.
- Knol, M.J.; VanderWeele, T.J. Recommendations for presenting analyses of effect modification and interaction. Int. J. Epidemiol. 2012, 41, 514–520. [Google Scholar] [CrossRef] [Green Version]
- Mirpuri, S.; Ocampo, A.; Narang, B.; Roberts, N.; Gany, F. Discrimination as a social determinant of stress and health among New York City taxi drivers. J. Health Psychol. 2020, 25, 1384–1395. [Google Scholar] [CrossRef]
- Shahrukh, M.; Pervaiz, M.; Khatoon, N. Stress-inducing factors among occupational drivers in Karachi, Pakistan. East. Mediterr. Health J. 2020, 26, 1233–1241. [Google Scholar] [CrossRef]
- Desrosiers, M.; Baroody, F.M.; Proud, D.; Lichtenstein, L.M.; Kagey-Sobotka, A.; Naclerio, R.M. Treatment with hot, humid air reduces the nasal response to allergen challenge. J. Allergy Clin. Immunol. 1997, 99, 77–86. [Google Scholar] [CrossRef]
- Ghio, A.J.; Richards, J.H.; Dittrich, K.L.; Samet, J.M. Metal storage and transport proteins increase after exposure of the rat lung to an air pollution particle. Toxicol. Pathol. 1998, 26, 388–394. [Google Scholar] [CrossRef]
- Janssen, N.A.; Strak, M.; Yang, A. Associations between three specific a-cellular measures of the oxidative potential of particulate matter and markers of acute airway and nasal inflammation in healthy volunteers. Occup. Environ. Med. 2015, 72, 49–56. [Google Scholar] [CrossRef]
- Seen, S.; Tong, L. Dry eye disease and oxidative stress. Acta Ophthalmol. 2018, 96, e412–e420. [Google Scholar] [CrossRef] [Green Version]
- Cong, Y.L.; Jin, D.M.; Wang, H.L.; Okada, T.; Peng, Z.H. Coordination Group for Reference Range of Venous Blood Examination in Chinese Adults. Establishing the reference range of venous blood measured by automated haematology analyzer in Chinese adults. Zhonghua Yi Xue Za Zhi 2003, 3, 1201–1205. [Google Scholar]
- Vagge, A.; Senni, C.; Bernabei, F.; Pellegrini, M.; Scorcia, V.; Traverso, C.E.; Giannaccare, G. Therapeutic Effects of Lactoferrin in Ocular Diseases: From Dry Eye Disease to Infections. Int. J. Mol. Sci. 2020, 21, 6668. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kang, B.; Eom, Y.; Lee, H.K.; Kim, H.M.; Song, J.S. The Protective Effect of an Eye Wash Solution on the Ocular Surface Damage Induced by Airborne Carbon Black Exposure. Cornea 2020, 39, 1040–1047. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Included n (%) | Not Included n (%) | p-Value |
|---|---|---|---|
| Male sex | 7276 (95.6) | 1092 (95.2) | 0.92 |
| Day-time drivers | 4156 (54.6) | 617 (53.8) | 0.78 |
| <CNY 5000/month | 5480 (72.0) | 848 (73.9) | 0.80 |
| ≧10 h/day | 4353 (57.2) | 630 (54.9) | 0.53 |
| Smoking | 6667 (87.6) | 1015 (88.5) | 0.98 |
| Alcohol | 4818 (63.3) | 760 (66.3) | 0.83 |
| Allergic tendencies * | 2658 (35.1) | 413 (37.6) | 0.89 |
| Obesity | 4346 (57.1) | 650 (56.7) | 0.59 |
| Iron deficiency anemia | 2679 (35.2) | 414 (36.1) | 0.77 |
| Hypertension | 3889 (51.1) | 571 (49.8) | 0.65 |
| Hypercholesterolemia | 2839 (37.3) | 472 (41.2) | 0.70 |
| Hypertriglyceridemia | 3311 (43.5) | 535 (46.6) | 0.72 |
| High blood sugar | 1659 (21.8) | 221 (19.3) | 0.42 |
| Self-employed | 571 (7.5) | 83 (7.2) | 0.97 |
| Education (college) | 175 (2.3) | 7 (0.6) | 0.50 |
| Stress (occupation and family) * | 6439 (84.6) | 1000 (87.2) | 0.90 |
| Characteristics | Cases (n = 1905), n (%) or Mean ± SD | Controls (n = 3803), n (%) or Mean ± SD | p-Value |
|---|---|---|---|
| Sex | 0.940 | ||
| Males Females | 1822 (95.6) 83 (4.4) | 3636 (95.6) 167 (4.4) | |
| Age | 0.948 | ||
| 21–30 | 446 (23.4) | 887 (23.3) | |
| 31–40 | 882 (46.3) | 1740 (45.8) | |
| 41–50 | 577 (30.3) | 1176 (30.9) | |
| BMI | 0.213 | ||
| <18.5 | 130 (6.8) | 422 (11.1) | |
| 18.5~23.9 | 689 (36.2) | 1213 (31.9) | |
| 24~ | 1086 (57.0) | 2168 (56.9) | |
| Shift drivers | 0.033 | ||
| Day-time | 1128 (59.2) | 1871 (49.2) | |
| Night-time | 777 (40.8) | 1932 (50.8) | |
| Myopia | 0.904 | ||
| No | 1775 (93.2) | 3567 (93.8) | |
| Yes | 130 (6.8) | 236 (6.2) | |
| CNY/month | 0.500 | ||
| <5000 | 1393 (73.1) | 2722 (71.6) | |
| 5000~8000 | 396 (20.8) | 757 (19.9) | |
| 8000~ | 116 (6.1) | 324 (8.5) | |
| Working h/day | |||
| 8~10 | 853 (45.8) | 1468 (38.6) | 0.206 |
| ≥10 | 1052 (55.2) | 2335 (61.4) | |
| Smoking | |||
| Never | 236 (12.8) | 354 (9.3) | 0.236 |
| Former | 1667 (23.7) | 3449 (26.3) | |
| Current | 1667 (63.5) | 3449 (64.4) | |
| Alcohol | 0.320 | ||
| No | 607 (31.9) | 1373 (36.1) | |
| Yes | 1296 (68.1) | 2430 (63.9) | |
| Allergic tendencies | 0.011 | ||
| No | 1090 (57.3) | 2578 (67.8) | |
| Yes | 813 (42.7) | 1225 (32.2) | |
| Hypertension | 0.514 | ||
| No | 942 (49.5) | 1784 (46.9) | |
| Yes | 961 (50.5) | 2019 (53.1) | |
| Hypercholesterolemia | 0.143 | ||
| No | 1106 (58.1) | 2426 (63.8) | |
| Yes | 798 (41.9) | 1377 (36.2) | |
| Hypertriglyceridemia | 0.069 | ||
| No | 961 (50.5) | 2232 (58.7) | |
| Yes | 942 (49.5) | 1571 (41.3) | |
| High blood sugar | 0.276 | ||
| No Yes | 1448 (76.1) 455 (23.9) | 3039 (79.9) 764 (20.1) | |
| Self-employed | 0.026 | ||
| No Yes | 1821 (95.7) 82 (4.3) | 3442 (90.5) 361 (9.5) | |
| Education | 0.151 | ||
| ≤High school | 1869 (98.2) | 3712 (97.6) | |
| College | 34 (1.8) | 91 (2.4) | |
| Stress events (occupation and family) during the 2 years a | 0.000 | ||
| No | 183 (9.6) | 870 (22.9) | |
| Yes | 1720 (90.4) | 2932 (77.1) | |
| Ln-Lf (mg/mL)b | 0.41 (0.39–0.43) | 0.69 (0.67–0.71) | 0.000 |
| OSDI score | 9.11 ± 8.05 | 8.40 ± 12.11 | 0.206 |
| CFS | 1.06 ± 0.98 | 0.98 ± 0.42 | 0.152 |
| TBUT (sec) | 2.65 ± 1.94 | 4.51 ± 2.36 | 0.021 |
| Schirmer’s test (mm/5 min) | 12.10 ± 7.66 | 10.85 ± 7.09 | 0.089 |
| Hb (g/L) | |||
| Male | 116 ± 12 | 119 ± 13 | 0.081 |
| Female | 105 ± 11 | 110 ± 12 | 0.069 |
| Single a | Multi b | |
|---|---|---|
| PM2.5 | 1.01 (0.98, 1.02) | --- |
| PM10 | 1.32 (1.15, 1.70) * | 1.33 (1.07, 1.90) * |
| O3 | 0.98 (0.78, 1.19) | 0.95 (0.76, 1.21) |
| SO2 | 1.10 (0.63, 1.81) | 1.08 (0.54, 1.72) |
| NO2 | 2.61 (1.67, 3.56) * | 2.64 (1.30, 4.37) * |
| CO | 1.08 (0.78, 1.82) | 1.04 (0.62, 2.16) |
| Humidity | 0.44 (0.54, 0.34) * | 0.40 (0.83, 0.27) * |
| Quartile | NO | Stress | |||||||
|---|---|---|---|---|---|---|---|---|---|
| With DED (n = 183) | Without DED (n = 870) | With DED (n = 1720) | Without DED (n = 2932) | ||||||
| β (95% CI) | R2 | β (95% CI) | R2 | β (95% CI) | R2 | β (95% CI) | R2 | ||
| PM10 | 1 | Reference | Reference | Reference | Reference | ||||
| 2 | 0.113 (−0.398, 0.571) | 0.11 | −0.174 (−0.371, 0.123) | 0.20 | −0.512 (−1.065, −0.041) | 0.31 | −0.365 (−0.779, 0.051) | 0.27 | |
| 3 | −0.255 (−0.248, 0.770) | 0.19 | −0.300 (−0.693, 0.013) | 0.23 | −0.531 (−0.978, 0.086) | 0.41 | −0.538 (−1.163, 0.128) | 0.48 | |
| 4 | −0.315 (−0.642, −0.140) | 0.14 | −0.329 (−0.756, 0.105) | 0.09 | −0.912 (−1.374, −0.413) | 0.59 | −0.586 (−0.888, −0.300) | 0.33 | |
| NO2 | 1 | Reference | Reference | Reference | Reference | ||||
| 2 | 0.020 (−0.654, 0.693) | 0.02 | −0.030 (−0.800, 0.737) | 0.02 | −0.445 (−0.744, −0.151) | 0.29 | −0.086 (−0.400, 0.261) | 0.06 | |
| 3 | −0.049 (−0.673, 0.579) | 0.09 | −0.301 (−0.802, 0.198) | 0.14 | −0.495 (−1.089, −0.094) | 0.30 | −0.131 (−0.994, 0.720) | 0.12 | |
| 4 | −0.451 (−0.920, 0.020) | 0.30 | −0.525 (−0.997, −0.049) | 0.39 | −0.668 (−1.141, −0.199) | 0.49 | −0.329 (−0.613, −0.039) | 0.15 | |
| Humidity | 1 | Reference | Reference | Reference | Reference | ||||
| 2 | 0.288 (−0.419, 0.994) | 0.12 | 0.616 (−0.344, 1.561) | 0.48 | 1.309 (0.095, 2.507) | 0.62 | 0.139 (−0.142, 0.416) | 0.11 | |
| 3 | 0.777 (−0.207, 1.772) | 0.52 | 0.971 (0.507, 1.430) | 0.42 | 1.373 (−0.036, 2.626) | 0.80 | 0.616 (−0.432, 1.724) | 0.49 | |
| 4 | 1.070 (−0.148, 2.159) | 0.76 | 1.897 (0.494, 3.020) | 0.84 | 1.994 (1.572, 2.303) | 0.92 | 1.734 (0.872, 2.659) | 0.82 | |
| Quartile | No | Allergic tendencies | |||||||
| With DED (n = 1090) | Without DED (n = 2578) | With DED (n = 813) | Without DED (n = 1225) | ||||||
| β (95% CI) | R2 | β (95% CI) | R2 | β (95% CI) | R2 | β (95% CI) | R2 | ||
| PM10 | 1 | Reference | Reference | Reference | Reference | ||||
| 2 | 0.010 (−0.277, 0.288) | 0.05 | −0.083 (−0.580, 0.412) | 0.09 | −0.240 (−0.457, 0.028) | 0.17 | −0.223 (−0.562, 0.117) | 0.17 | |
| 3 | −0.068 (−0.327, 0.252) | 0.10 | −0.117 (−0.377, 0.236) | 0.11 | −0.489 (−0.761, −0.244) | 0.31 | −0.588 (−0.613, −0.072) | 0.16 | |
| 4 | −0.148 (−0.316, 0.032) | 0.16 | −0.140 (−0.355, 0.024) | 0.16 | −0.751 (−1.597, 0.094) | 0.46 | −0.615 (−1.075, 0.157) | 0.37 | |
| NO2 | 1 | Reference | Reference | Reference | Reference | ||||
| 2 | −0.174 (−0.448, 0.109) | 0.03 | −0.207 (−0.441, 0.058) | 0.10 | −0.336 (−0.616, −0.040) | 0.20 | −0.199 (−0.654, 0.288) | 0.19 | |
| 3 | −0.432 (−0.551, 0.015) | 0.06 | −0.382 (−0.863, −0.164) | 0.29 | −0.582 (−0.856, −0.230) | 0.34 | −0.446 (−0.715, −0.204) | 0.29 | |
| 4 | −0.454 (−0.978, 0.049) | 0.09 | −0.551 (−0.984, 0.012) | 0.33 | −0.658 (−1.243, 0.046) | 0.42 | −0.507 (−1.102, 0.062) | 0.39 | |
| Humidity | 1 | Reference | Reference | Reference | Reference | ||||
| 2 | 0.486 (−0.157, 0.921) | 0.32 | 0.583 (−0.096, 1.055) | 0.49 | 1.054 (0.157, 1.956) | 0.59 | 0.751 (−0.020, 1.375) | 0.50 | |
| 3 | 0.755 (−0.045, 1.533) | 0.51 | 0.721 (−0.065, 1.420) | 0.53 | 1.404 (−0.217, 2.977) | 0.72 | 1.073 (−0.193, 2.212) | 0.66 | |
| 4 | 0.994 (−0.051, 1.926) | 0.61 | 1.204 (0.020, 2.408) | 0.71 | 1.470 (0.247, 2.619) | 0.74 | 1.109 (0.329, 1.859) | 0.62 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hao, W.; Kong, F.; Song, W.; Zhang, L.; Xu, X.; Ren, Z.; Li, J.; Yu, F. Air Pollution and Tear Lactoferrin among Dry Eye Disease Modifications by Stress and Allergy: A Case–Control Study of Taxi Drivers. Atmosphere 2022, 13, 2003. https://doi.org/10.3390/atmos13122003
Hao W, Kong F, Song W, Zhang L, Xu X, Ren Z, Li J, Yu F. Air Pollution and Tear Lactoferrin among Dry Eye Disease Modifications by Stress and Allergy: A Case–Control Study of Taxi Drivers. Atmosphere. 2022; 13(12):2003. https://doi.org/10.3390/atmos13122003
Chicago/Turabian StyleHao, Wei, Fanxue Kong, Wei Song, Lei Zhang, Xueying Xu, Zhongjuan Ren, Jing Li, and Fei Yu. 2022. "Air Pollution and Tear Lactoferrin among Dry Eye Disease Modifications by Stress and Allergy: A Case–Control Study of Taxi Drivers" Atmosphere 13, no. 12: 2003. https://doi.org/10.3390/atmos13122003