
Exploring the Diet-Gut Microbiota-Epigenetics Crosstalk Relevant to Neonatal Diabetes


Heart, Mind & Body Research Group, Griffith University, Gold Coast, QLD P.O. Box 4222, Australia
Genes 2023, 14(5), 1017; https://doi.org/10.3390/genes14051017
Submission received: 13 March 2023
/
Revised: 24 April 2023
/
Accepted: 28 April 2023
/
Published: 29 April 2023
(This article belongs to the Special Issue Human Microbiota: Current Updates on Pathogenetic Mechanisms and Methodological Advances)
{kind=link}
{kind=link}
Abstract
:Neonatal diabetes (NDM) is a rare monogenic disorder that presents as hyperglycemia during the first six months of life. The link between early-life gut microbiota dysbiosis and susceptibility to NDM remains uncertain. Experimental studies have demonstrated that gestational diabetes mellitus (GDM) could develop into meconium/gut microbiota dysbiosis in newborns, and thus, it is thought to be a mediator in the pathogenesis of NDM. Epigenetic modifications have been considered as potential mechanisms by which the gut microbiota and susceptibility genes interact with the neonatal immune system. Several epigenome-wide association studies have revealed that GDM is associated with neonatal cord blood and/or placental DNA methylation alterations. However, the mechanisms linking diet in GDM with gut microbiota alterations, which may in turn induce the expression of genes linked to NDM, are yet to be unraveled. Therefore, the focus of this review is to highlight the impacts of diet, gut microbiota, and epigenetic crosstalk on altered gene expression in NDM.
Keywords:
neonatal diabetes; gestational diabetes; gut microbiota; diet; gene expression; epigenetic1. Introduction
Diabetes development in the first months of life is unlikely to be related to Type 1 diabetes (T1D) autoimmunity [1,2]. Neonatal diabetes (NDM), also termed congenital diabetes, is rare and presents in infants up to 6 months of age. It has more than 20 different monogenic causes, for example, mutations in signal transducer and activator of transcription 3 (STAT3) and LPS-responsive beige-like anchor (LRBA) genes [3,4]. NDM has been diagnosed in extremely preterm infants [5,6,7,8], particularly those with mutations in chromosome 6q24, GATA binding protein 6 (GATA6), and potassium inwardly rectifying channel, subfamily J, member 11 (KCNJ11) [7,8]. Infants diagnosed with NDM with no mutation in the KCNJ11 gene were less likely to have T1D-associated high-risk human leukocyte antigen (HLA) genotypes (DR3-DQ2/X, DR4-DQ8/X, and DR4-DQ8/DR3-DQ2) [1]. Gestational diabetes mellitus (GDM), characterized by increased peripheral insulin resistance (IR), may cause fetal complications, including weight gain, glucose intolerance, and death. However, its effect on NDM remains uncertain [9].
The colonization of the gut with microbes starts prenatally, in utero, after birth, and during breastfeeding. According to the sterile womb hypothesis, microbes are transported from the mother through the lymphatic system or blood stream into the placenta and then translocated to the fetal gut [10,11,12]. The maternal gut microbiota during pregnancy is crucial in shaping the composition of the gut microbiota and immune functions early in life, where diet and other factors (e.g., gestational age, maternal obesity, antibiotic usage) are found to influence the infant gut microbial diversity and richness, which in turn may enhance gut dysbiosis and disease susceptibility later in life [12,13,14,15,16]. Gut microbial dysbiosis in early life plays a significant role in the development of inflammation-related diseases, such as obesity, asthma, inflammatory bowel disease, and necrotizing enterocolitis [17,18,19,20].
The gut microbiota dysbiosis involved in NDM remains unclear. Compelling experimental studies reported that GDM could result in maternal gut and/or neonatal meconium microbiota dysbiosis, characterized by an increased abundance of Actinobacteria and Proteobacteria, Streptococcus, Bacteroides, Lachnospiraceae, Clostridium, Klebsiella, Desulfovibrio, Rothia, Shigella, Escherichia, Collinsella, and Proteus [21,22,23,24,25]. Diet has been shown to induce gut dysbiosis in women with GDM, along with gut dysbiosis in their newborns [26,27]. However, the exact mechanisms by which diet in GDM alters gut microbiota composition, which may in turn influence gene expression in NDM, are not well understood. A potential hypothesis is that epigenetic mechanisms mediate the effects of diet-microbiota interactions on altering gene expression in NDM. In general, there is a complex interaction between epigenetics, diet, and gut microbiota that can influence gene expression profiles in NDM. Therefore, this review highlights the epigenetic mechanisms mediating the relationships between diet-microbiota interactions and gene expression changes in NDM.
2. Methods
A literature search was performed in the PubMed/MEDLINE database and Google Scholar up to February 2023 for studies published in English exploring the impacts of diet, gut microbiota, and epigenetic crosstalk on altering gene expression in NDM. The following keywords were searched: “GDM”, “NDM”, “IR”, “pancreatic β-cells”, “neonates/newborns”, “gut microbiota”, “diet”, “epigenetic”, and “gene expression”. Studies with the main focus on the associations between diet and gut microbiota in GDM and/or their newborns were considered. Human and in vitro studies were considered without study design restrictions.
3. An Overview of NDM
NDM is classified into transient (TNDM), permanent (PNDM), or syndrome types, which have expressed significant genetic changes causing persistent hyperglycemia, reduced β-cell mass or replication, delayed pancreatic islet development, and impaired insulin secretion [28]. Autosomal recessive or dominant mutations in the preproinsulin (INS) and the ATP-sensitive potassium (KATP) channel (very common to KCNJ11 or ATP-binding cassette transporter subfamily C member 8, ABCC8) are the major genes responsible for TNDM and PNDM. PNDM can also result from autosomal recessive mutations in the glucokinase (GCK) and pancreatic and duodenal homeobox l (PDX1) genes. Compound heterozygous or homozygous mutations in GCK and PDX1 may cause β-cell glucose sensing impairment and hypoplasia or pancreas agenesis. Insulin or sulfonylurea therapy can often be used for infants with mutations in KCNJ11, ABCC8, and INS [29,30,31,32,33,34,35]. A previous study identified a novel imprinted gene (protein phosphatase 1 regulatory subunit 13 like, PPP1R13L) on chromosome 19q13.32 that is hypomethylated in TNDM and associated with the zinc finger protein 57 homolog (ZFP57) [36]. TNDM is seen most often in cases of hyperglycemia and intrauterine growth retardation and may cause IR later in life [37]. An experimental study demonstrated that the CC dinucleotide sequence of the human INS gene’s active chromatin during pancreas development is mutated in TNDM. The CC dinucleotide mutation also results in disrupted GLI-similar 3 (GLIS3)-dependent activation of an episomal INS gene [38].
The most common cause of syndrome NDM is autosomal recessive mutations in eukaryotic translation initiation factor 2-α kinase 3 (EIF2Ak3) (diabetes associated with renal dysfunction/epiphyseal dysplasia), Solute carrier family 2 member 2 (SLC2A2) (diabetes associated with facilitated glucose transporter), Solute carrier family 19, member 2 (SLC19A2) (diabetes associated with megaloblastic anemia syndrome), Insulin receptor (INSR) (diabetes associated with severe IR), and Forkhead box P3 (FOXP3) (diabetes associated with polyendocrinopathy/immunodysregulation) [29,30,31,34,35]. NDM causes insulin deficiency as a result of β-cell destruction or the impaired function of β-cells [2]. Monogenic NDM is associated with growth restriction in utero because of insulin insufficiency that relies on gene mutations in the brain, which may lead to neurodevelopmental disability [39]. There is recent evidence for severe insulin deficiency, increased islet β-cell destruction, and low birthweight and C-peptide levels in infants diagnosed with a high polygenic risk in the first six months of life [40].
4. Epigenetic Modifications and NDM Gene Expression Profiles in Neonates Exposed to GDM
Epigenetic changes in several genes involved in GDM are thought to impact newborn metabolic disease susceptibility [41,42,43]. A recent genome-wide methylation analysis identified many enriched pathways for hypo/hyper-differential methylation genes (DMGs) in the placenta and/or the umbilical cord blood of newborns exposed to maternal GDM. The top-ranking pathway enriched in 84 DMGs was the “insulin secretion/IR” pathway [44]. It has been shown that alterations of DNA methylation characterized by significant hypermethylation at two cytosine-phosphate-guanine dinucleotide (CpG) sites and hypomethylation at all CpG sites in adipose tissues of women with GDM and fetal cord blood cells are responsible for reduced adiponectin mRNA expression associated negatively with blood glucose and homeostatic model assessment-IR (HOMA-IR) [45]. This suggests that reduced adipose tissue adiponectin expression may be considered a pathogenic factor in GDM offspring [45]. A study analyzing the DNA methylation profile in the cord blood of newborns exposed to women with GDM has identified 200 differentially methylated loci. Some metabolic disease/T1D-related genes (interleukins 6 and 10; IL-6, IL-10) and pathways enriched by differentially methylated loci were identified. The top metabolically related signaling pathways, including mitogen-activated protein kinase (MAPK), Janus kinase (JAK), phosphatidylinositol-3 kinase (PI3K), and STAT3, were identified [46].
Epigenetics is considered a key mechanism that affects glucose metabolism genes involved in GDM, and their dysregulation leads to differential DNA methylation of the tribbles homolog 1 (TRIB1) gene and vasoactive intestinal peptide receptor (VIPR1) in the placenta and fetal cord blood [47]. VIPR1 is highly expressed in pancreatic β-cells, which may activate adenylate cyclase and insulin secretion by increasing intracellular cyclic AMP (cAMP) production, which in turn stimulates protein kinase A (PKA) and increases optimal calcium influx. Genetic deletion of VIPR1 could lead to glucose intolerance [48]. The TRIB1 gene, mapped to chromosome 8q24 [49], was found to be influenced by GDM exposure in the umbilical vein endothelial cells of newborns [50]. An experimental study showed that the TRIB1 gene was associated with pro-inflammatory gene cyclooxygenase-2 (COX-2) overexpression by the action of regulated early growth response gene-1 (EGR-1), which resulted in increased glucose levels in small for gestational age neonate-derived mesenchymal stem cells [51]. In pancreatic islet β-cells, COX-2 expression was associated with downregulation of PDX1-related NDM by increasing the IL-1β autostimulation [52].
The placental tissue of women with GDM induces pro-inflammatory gene expression (tumor necrosis factor-α, TNF-α) that dysregulates insulin signaling and reduces insulin secretion from β-cells under the condition of hyperglycemia [53]. Placental GDM is the major secretion site of growth hormones (e.g., insulin-like growth factor, IGF) that play a role in stimulating pro-inflammatory cytokine production by activation of inflammatory pathways, such as PI3K [53], which increases glucose levels in the fetal cord blood and may result in NDM. The results of previous studies suggest an association between the GDM intrauterine environment and placental DNA methylation [53,54]. Higher placental DNA methylation of the PPAR-γ coactivator-1-α (PGC1α) gene was associated with IR and insulin secretion in women with GDM [54]. High maternal glucose levels were reported to be associated with placental DNA methylation changes to the PGC1α gene on chromosome 4p15.1 in GDM, suggesting that PGC-1α disturbs placental functions, which may increase the risk of diabetes in offspring [55]. PGC1α mRNA expression in human adipocytes has been linked to IR markers. Patients with IR and visceral obesity have demonstrated reduced PGC1α mRNA expression in adipose tissue, which leads to increased adiponectin and IL-6 serum levels [56]. In one longitudinal study, maternal GDM was shown to induce high DNA methylation variations at the PGC1α gene locus, and such variations may mediate the impact of GDM on increasing fetal cord blood glucose levels [57]. PGC1α mRNA expression in both adipose and placenta tissue of GDM women has an impact on glucose and lipid homeostasis by increasing adiponectin and low density lipoprotein (LDL) cholesterol levels and decreasing tryglycerides and glucose levels [58]. Levels of PGC1α and PDX1 were reported to be reduced in placental tissue of women with GDM, which may lead to abnormal glucose metabolism in newborns [59]. Upregulating PGC1α activity in the brain and lungs of preterm infants has a significant role in activating the transcription factors implicated in mitochondrial biogenesis and increasing mitochondrial antioxidant enzymes, which in turn may reduce inflammation and oxidative stress (OS) by downregulating pro-inflammatory cytokines and chemokines [60]. Overexpression of the forkhead box O 1 (FoxO1) in pancreatic β-cells regulated by glucagon-like peptide 1 (GLP-1) stimulation results in inhibited PGC1α and its target gene, PDX1-related NDM [61].
The imprinted mesoderm-specific transcript (MEST) gene showed significant DNA methylation at five CpG sites in the cord blood of GDM newborns, which in turn led to decreased MEST methylation, thus influencing obesity and diabetes susceptibility [62]. A large-scale, genome-wide study has identified a total of 4485 hypermethylated and hypomethylated CpG sites in 2198 differentially methylated genes (e.g., MEST) enriched in the T1D pathway in the cord blood of infants born to GDM women [63]. MEST, located on chromosome 7q32, a gene belonging to a cluster of carboxypeptidase A (CPA) genes, has been implicated in postnatal and intrauterine growth restriction related to congenital Silver-Russell syndrome (SRS) [64]. Evidence suggests that paternal inherited H19/IGF2:IG-DMR deletions interfering with ZFP57 involved in NDM may result in SRS [65]. A case report has shown that maternal inheritance at chromosomes 2, 8, and 21 in the region of PLAG1 like zinc finger 1 (PLAG1)-associated NDM is responsible for SRS [66].
A pilot study has identified differentially methylated regions of POU class 2 homeobox 1 (POU2F1), paraoxonase 1 (PON1), and NF-E2 related factor 2 (NRF2) in the cord blood of newborns of GDM women [67]. POU2F1 is found on chromosome 1q24, a locus with evidence of strong linkage disequilibrium for its relationship to type 2 diabetes (T2D) [68]. Treatment of pancreatic β-cells with hydrogen peroxide (H2O2) results in enhanced POU2F1 activity as well as other inflammatory signaling pathway activation, such as c-jun N-terminal kinase (JNK) and DNA-dependent protein kinase (DNA-PK) [69], which in turn may increase IR and diabetes susceptibility. Methylation for the PON1 gene in mothers, which is localized on chromosome 7q21-22 [70], has been observed in children of mothers exposed to adverse life events, which coincides with the presence of the ZFP57 gene implicated in NDM [71]. The Q192R polymorphism of the PON1 gene was reported to increase GDM susceptibility, which could be a marker for IR [72]. High PON1 levels and PON1 lactonase activity were associated with increased OS, which causes alterations of the glycolipid metabolic profiles in infants born to GDM women [73]. Neonates demonstrate increased free PON1, decreased PON1 lactonase activity, and different PON1 distribution in the high-density lipoprotein (HDL) subclasses in cord blood. PON1 lactonase activity was observed to be lower in the large HDL group than in the small HDL group [74]. Impaired NRF2 activity was reported to increase IR and OS associated with diabetes, which can contribute to decreased antioxidant enzyme activity in pancreatic β-cells [75]. GDM contributes to fetal NRF2-mediated antioxidant signaling dysregulation in fetal endothelial cells by increasing OS, protein carbonylation, and mitochondrial reactive oxygen species (ROS) generation [76]. NRF2 has been shown to restore PDX1 levels in pancreatic β-cells by reducing OS-mediated JNK-dependent FOXO1 activation [77]. A candidate gene study showed that downregulation of PDX1 mRNA expression in the placentas of women with GDM resulted in increased blood glucose levels in fetal cord blood [59].
A recent meta-analysis of epigenome-wide association studies showed that maternal hyperglycemia during pregnancy is associated with reduced offspring DNA methylation at two CpG sites located in the thioredoxin interacting protein (TXNIP) gene [78]. Overexpression of TXNIP, also termed α-arrestin, in pancreatic β-cells increases glucose levels by binding to and suppressing the antioxidant protein thioredoxin (TXN), which may lead to impaired activity of the angiogenic cytokine vascular endothelial growth factor (VEGF), increased ROS expression, induction of apoptosis, and decreased insulin production [79,80]. Overexpression of TXNIP mRNA in the placenta increases ROS production and mitochondrial dysfunction as a result of decreasing TXN expression levels [81]. In one study, TXNIP mRNA expression was reported to increase in GDM women but not in neonates. On the other hand, TXN mRNA expression in the placenta was high. The thioredoxin (TXN)/TXNIP ratio increases in the placenta and neonatal cord blood of GDM women, concurrent with increased expression of nuclear factor-kappa B (NF-kB), as well as STAT3 and its target protein suppressor of cytokine signaling 3 (SOCS3) [82]. This indicates that TXN expression in the placenta may exert a protective role in protecting the newborn from oxidative effects. Another study has linked NDM with an aberrant activation of STAT3, which leads to pancreatic β-cell dysfunction and reduced insulin expression [83].
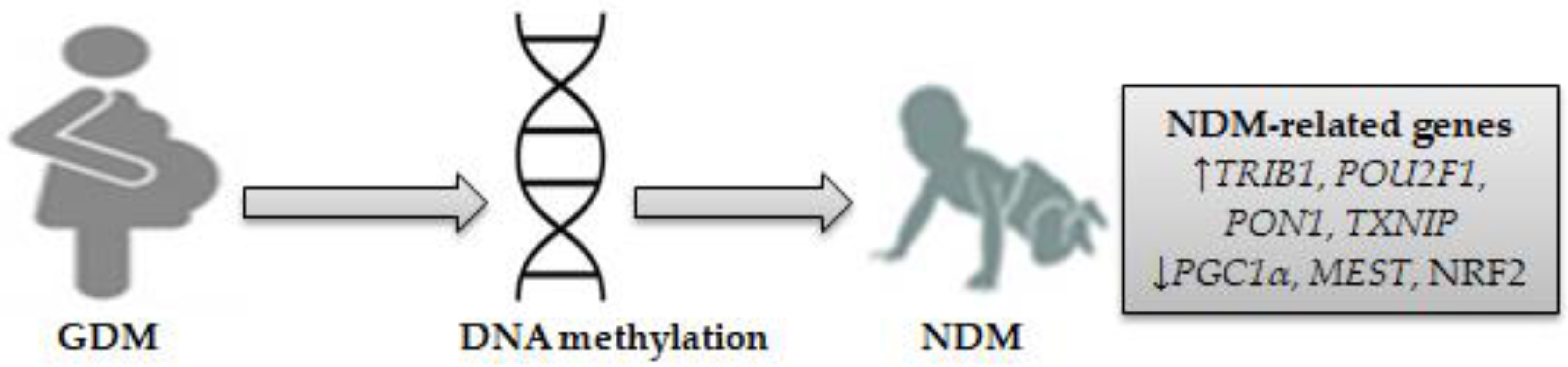
These findings suggest that exposure to GDM causes alterations in placental and/or fetal cord blood DNA methylation, which in turn may impact fetal glucose metabolism genes involved in NDM. Differentially expressed genes might be enriched in the PI3K, STAT3, JAK, and MAPK signaling pathways and other inflammatory genes, such as COX-2, IL-6, and IL-10. On this basis, seven genes related to NDM were identified: TRIB1, PGC1α, MEST, POU2F1, PON1, NRF2, and TXNIP. Figure 1 shows NDM-related gene-specific DNA methylation in neonates exposed to GDM.
5. Diet, Gut Microbiota, and Epigenetic Crosstalk Alters Gene Expression in NDM
Gut microbiota, as one environmental factor, may modulate epigenetic mechanisms through DNA methylation alterations in response to diet, which may affect glucose metabolism genes involved in NDM. This section focuses on the crosstalk between diet, gut microbiota, and microbial-derived metabolites (short-chain fatty acids, SCFAs), considered epigenetic modifiers, which could in turn influence gene expression profiles in NDM.
5.1. Diet Alters Gut Microbiota in GDM and NDM
Diet is considered the key environmental factor contributing to the pathogenesis of islet autoimmunity by modulating the gut microbiota, which may lead to dysbiosis, characterized by increased intestinal inflammation, permeability, and reduced mucosal barrier integrity [84]. The intestinal permeability as a result of increased levels of tight junction (TJ)-related proteins (e.g., zonulin, occludin, and claudin-2) influenced by microbial colonization could trigger autoimmunity by allowing microbial or dietary antigens to be transferred to the circulation, leading to pancreatic β-cell destruction that can contribute to intestinal inflammation [85].
A few studies have shown that diet may influence gut microbiota in women with GDM and their infants. A prospective study of GDM women showed that dietary fat intake (polyunsaturated fatty acid, PUFA; saturated fatty acid, SFA) is associated with a higher abundance of gut Bacteroidetes Alistipes, while dietary fiber intake is associated with a higher abundance of gut Firmicute Roseburia [26]. In another prospective study, GDM women consuming a complex carbohydrate (CHO) and low-fat diet (choice diet) showed a higher abundance of gut Bifidobacterium spp. (particularly B. adolescentis) than those consuming a high-fat diet (conventional diet). The study also revealed a high relative abundance of Prevotella copri (P. copri), Enterobacter cloacae (E. cloacae), Enterococcus faecalis (E. faecalis), and Bacteroides in the guts of infants aged ≤ 4 months born to women on a conventional diet [27]. This suggests that diet in women with GDM is associated with the composition of the neonatal gut microbiota.
5.2. Gut Microbiota and Its Metabolites Alter Gene Expression in NDM
The generation of metabolites produced by gut microbiota in response to diet, such as SCFAs, could be considered an epigenetic mechanism that may influence gene expression in NDM. SCFAs and butyrate in particular have been shown to alleviate inflammation in infant intestinal epithelial cells (IECs) through their ability to inhibit histone deacetylases (HDACs) and activate G-protein coupled/free fatty acid receptors (GPRs/FFAs) in dendritic cells (DCs), which promote differentiation of FOXP3+ regulatory T (Treg) cells. This result in inhibited NF-κB activation, lipopolysaccharide (LPS)-induced pro-inflammatory cytokine and chemokine secretion, and induced PPARγ-dependent pathway activation [17,18,19,20]. SCFAs enhance intestinal barrier integrity by reducing blood glucose levels, increasing protective GLP-1 production, and improving IR by activating NF-κB and STAT3 [86], identified as an NDM-related gene [82,83]. In human monocyte-macrophage cells, SCFAs were shown to inhibit the nucleotide-binding oligomerization domain-like receptor family pyrin domain containing 3 (NLRP3) inflammasome by increasing Nrf2-mediated TXN1, which reacts with TXNIP implicated in NDM, resulting in a decreased expression of TNF-α and IL-1β [87]. SCFAs were also reported to improve intestinal barrier function by reducing LPS-induced TXNIP-mediated NLRP3 activation and TJ-related proteins (zonulin and occludin) [88]. Butyrate has been found to increase Nrf2 mRNA levels and inhibit protein 53 (p53) mRNA levels in IECs [89].
Diets rich in dietary fiber, complex CHO, and/or dietary fat induce changes in the GDM and their newborn microbiome, with increases in the Gram-positive Actinobacteria (Bifidobacterium) and Firmicutes (Roseburia, E. faecalis) and the Gram-negative Bacteroidetes (Bacteroides, P. copri, Alistipes) and Enterobacteriaceae (Enterobacter cloacae, E. cloacae).
5.2.1. Actinobacteria
A few studies have shown that Bifidobacterium spp. (including B. adolescentis) are transferred from mothers to their neonates [90,91,92,93]. In one study, Bifidobacterium spp. were found to be enriched in the gut of breastfed infants born to GDM women [94], while in another study, Bifidobacterium spp. were depleted in the gut of GDM women [95]. In full-term infants born to GDM women, Bifidobacterium spp. was associated with reduced fecal propionate levels [96]. Bifidobacterium spp. are able to utilize human milk oligosaccharides (HMOs) (e.g., fructo-oligosaccharide and galacto-oligosaccharide) through glycoside hydrolase (GHs)-related degradation enzymes, resulting in increased production of butyrate, propionate, and acetate [20]. Bifidobacterium spp. are reported to ferment resistant starch in the newborn gut prior to the weaning period, which results in the production of SCFAs [97]. Probiotic-supplemented formulas increase Bifidobacterium spp. abundance in preterm gut microbiota [20]. Adherence to a very low-calorie ketogenic diet (VLCKD) during pregnancy, characterized by low CHO, moderate protein, and high fat intake, influences the infant gut microbiota composition and leads to an increase in the abundance of Bifidobacterium spp., which exerts protective effects against inflammation-related diseases by inhibiting several signaling pathways [17,18,19,20]. Butyrate and acetate-producing B. lactis spp. 420 resulted in reduced COX-2 expression in the enterocyte-like cell line Caco-2 [98]. In vitro, treatment of macrophage RAW264 cells with B. adolescentis and quercetin induced anti-inflammatory effects by reducing LPS-stimulated TNF-α and IL-1β production and inducible nitric oxide synthase (iNOS) and COX-2 expression [99]. Thus, B. adolescentis may exert its anti-inflammatory effects on NDM by reducing TRIB1 gene-mediated COX-2 expression.
5.2.2. Firnicutes
There is evidence to support vertical transmission of Roseburia from mother to infant by breastfeeding [100]. Gut dysbiosis in GDM women is characterized by a reduced abundance of Roseburia, which was associated with increased blood glucose levels and IR [101]. The VLCKD could be considered a contributing factor influencing the gut butyrate-producing Roseburia intestinalis (R. intestinalis) in infants and children, which exerts anti-inflammatory effects in IECs as indicated by increasing transforming growth factor-β (TGF-β) and inhibiting LPS-induced TNF-α and IL-17 secretion [19]. IL-17 is involved in the dysregulation of insulin production from β-cells by activation of NF-κB and STAT1 signaling pathways, resulting in increased interferon (IFN)γ and IL-1β-induced TNF-α production [53,102]. R. intestinalis and R. hominis are shown to upregulate the PGC1α gene in IECs [103], which is reported to be downregulated in adipose and placental tissue of GDM women, resulting in increased IR markers and fetal cord blood glucose levels [57,58]. It can be suggested that Roseburia spp. may exert anti-inflammatory effects in the IECs of GDM neonates, providing a potential therapeutic role for NDM by upregulating the PGC1α gene.
A previous study supports the notion of vertical transmission of Enterococcus spp. from the mother to her infant by vaginal delivery [104]. Enterococcus forms L(+)-lactic acid as the key end product of sugar fermentation [105]. Enterococcus is able to ferment resistant starch in pre-weaned or weaning infants, which in turn produces butyrate, propionate, and acetate [97]. Early probiotic supplementation with B. breve M-16V resulted in increased fecal Enterococcus proportions in preterm infants [20]. The presence of E. faecalis was shown to decrease blood glucose levels in the human IEC line Caco-2 after feeding with a diet containing glucose or sucrose [106]. E. faecalis induces anti-inflammatory effects in infant IECs through its ability to inhibit tumor-receptor associated factors by inhibiting JNK and MAPK signaling pathways [17]. In neonatal IEC, E. faecalis was reported to activate anti-inflammatory cytokine IL-10 production and DNA binding of the transcription factor PGC1α gene [107], which is known to regulate blood glucose levels in NDM. Thus, E. faecalis may exert a protective effect against NDM due to its ability to promote the PGC1α gene.
5.2.3. Bacteroidetes
Evidence from strain-level vaginal microbial detection using a metagenomic approach confirms the mother and the newborn shared Bacteroides spp. as a result of vertical transmission [91,92,93,108]. Recent studies have shown an increased abundance of gut Bacteroides spp. in GDM women and/or their newborns [109,110,111]. Bacteroides contain several GHs involved in mucin glycan degradation that maintain gut mucosal barrier integrity [112,113]. SCFAs are largely produced by Bacteroides in weaned infants’ feces in response to resistant starch fermentation [97], through the acetyl-CoA and succinate pathways [114]. Bacteroides spp., including B. thetaiotaomicron, B. vulgatus, and B. fragilis, are SCFA-producing bacteria that may exert anti-inflammatory effects in the inflamed IECs in infants in response to adherence to the VLCKD during pregnancy, resulting in reduced pro-inflammatory cytokine expression by epigenetic mechanisms related to DNA methylation and non-coding RNAs (lncRNA) [17,18,19,20]. In one study, B. vulgatus was shown to increase plasma IL-6 and IR in T2D patients [115], while in another study, unclassified Bacteroides were reduced in GDM women [110]. Evidence from an experimental study showed that B. fragilis promotes the Sulfiredoxin-1 (Srx-1) enzyme responsible for decreasing peroxiredoxin hyperoxidation by activating Nrf2 siRNA-related NDM in IECs treated with enterotoxin-induced OS and DNA damage [116]. This suggests that B. fragilis may protect against NDM by reducing oxidative damage in IECs through upregulation of the NRF2 gene.
There is evidence suggesting a vertical transmission of fecal Alistipes from mothers to infants following vaginal birth [93]. The genus Alistipes belongs to the GH family, which is essential for mucin degradation in the gut [113]. Compared to a plant-based diet, an animal-based diet had a greater influence on gut microbiota alterations by increasing the abundance of SCFA-producing Alistipes [117]. Decreases in Alistipes abundance may lead to gut dysbiosis and contribute to GDM. The results of previous studies demonstrated an increased abundance of Alistipes spp. in the gut microbiota of healthy pregnant women compared to GDM women, which was negatively associated with glucose tolerance and increased sensitivity to C-reactive proteins [95,118,119]. Alistipes was associated with reduced pancreatic exocrine dysfunction and mucin degradation in T1D patients with islet autoimmunity [120]. Alistipes exerts immunomodulatory activity in human peripheral blood mononuclear cells by inhibiting toll-like receptor 4 (TLR-4)-dependent IL-6, IL-1β, and TNF-α production elicited by Escherichia coli (E. coli) LPS [121]. This suggests that Alistipes may exert anti-inflammatory effects in GDM through their ability to enhance gut mucosal barrier function. An in vitro experimental study found an increase in the colonization of diverse gut microbiota, including Alistipes, after consumption of anthocyanin-rich fruit juice, which in turn reduced the basal level of NRF2 gene transcription in peripheral blood lymphocytes [122]. Short-term administration of COX-2 inhibitor celecoxib increases gut abundance of butyrate-producing Alistipes in vitro, resulting in decreased production of IL-8 and C-X-C motif chemokine ligand (CXCL-16) [123]. It can be suggested that Alistipes may exert immune-regulatory and anti-inflammatory effects on the neonatal gut through downregulating TRIB1 gene-mediated COX-2 expression, which contributes to a decreased risk of NDM.
A few studies have revealed a low abundance of Prevotella in the guts of GDM women and their infants [22,124]. Prevotella was shown to reduce fecal levels of branched SCFAs (isobutyrat and isovalerate) in GDM women [124] and acetate in neonates born to GDM women [96], suggesting that Prevotella may increase inflammatory activities and influence risk for GDM and NDM, in part by reducing SCFA levels. Prevotella was found to promote inflammation and reduce TJ integrity, as demonstrated by a study stimulating IECs to produce pro-inflammatory cytokines (e.g., IL-6, IL-8) [125]. Among Prevotella spp., P. copri was associated with HOMA-IR [126]. P. copri increases LPS-induced IL-6 production associated with IR and low-grade inflammation [115]. An increased abundance of P. copri was associated with adherence to an omnivorous dietary regimen, characterized by low levels of lipid metabolism-related miRNA expression [127], which is regulated by the activity of Nrf2-related NDM [128]. This suggests that P. copri drives unstable epigenetic changes in the gut of GDM newborns, which may increase NDM susceptibility.
5.2.4. Enterobacteriaceae
Few studies have confirmed the mother-to-infant transmission of Enterobacter spp. (E. cloacae and E. aerogenes) by vaginal delivery [91,108], which act as bacterial pathogens causing nosocomial infections [129]. Enterobacteriaceae, particularly E. cloacae, are dominant with a high relative abundance in the gut microbiota of GDM women [95]. In vitro, E. cloacae abundance is associated with the long-term glucose marker hemoglobin A1c (HbA1c), LPS binding protein (LBP), and C-reactive peptide (CRP). It also induces pancreatic β-cell inflammation through downregulation of the PDX1 gene, which coincides with an activation of TXNIP-mediated NLRP3 involved in NDM, resulting in increased pro-inflammatory cytokines TNF-α, IL-1β, and IL-6 [130]. This suggests that E. cloacae may induce changes in the gene patterns that coincide with increasing pro-inflammatory effects in the neonate’s gut, increasing NDM risk.
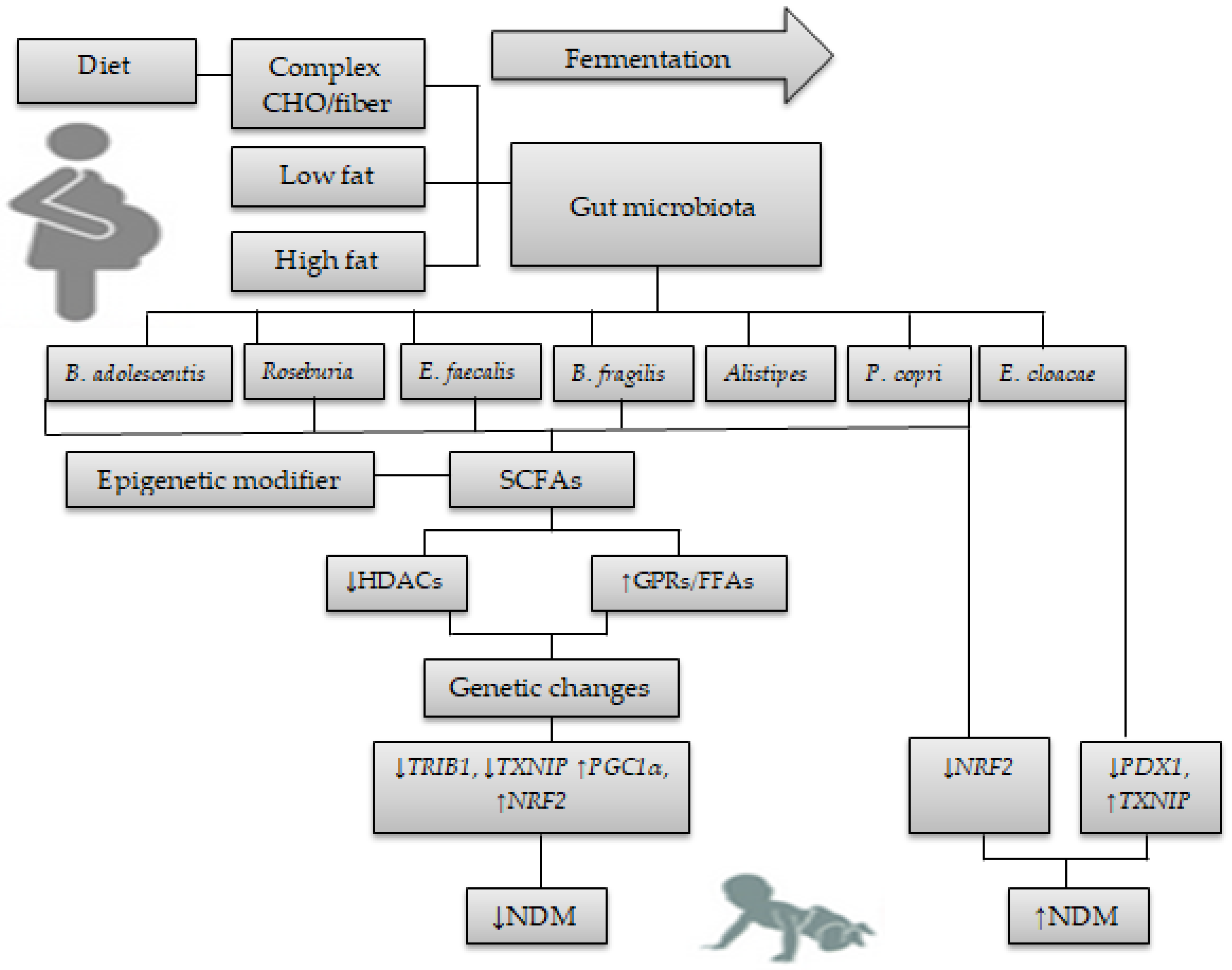
Figure 2 shows the interplay between diet, gut microbiota, and epigenetics relevant to NDM.
6. Conclusions
NDM is monogenic in etiology, with infants who have autosomal recessive or dominant mutations in genes responsible for TNDM, PNDM, and syndrome types. Epigenetics is implicated in NDM susceptibility, and previous studies suggest that the DNA methylation in the cord blood of newborns exposed to GDM is altered, which in turn may impact glucose metabolism genes. NDM is influenced by a comprehensive set of genes. This review identifies seven genes showing significant expression alterations in response to GDM exposure. These include four upregulated genes (TRIB1, POU2F1, PON1, and TXNIP) and three downregulated genes (PGC1α, MEST, and NRF2) with NDM.
Few studies have confirmed the potential for gut microbiota to be transmitted from mother to newborn. Gut microbiota dysbiosis in NDM remains largely unknown. GDM is associated with gut microbiota dysbiosis in newborns. Diet and gut microbiota dysbiosis in GDM may be a potential predictive biomarker of NDM. SCFAs are considered epigenome modifiers that alleviate intestinal inflammation and affect the expression of NDM-related genes.
Maternal diet in GDM was associated with alterations in gene expression in NDM. Interactions between complex CHO/low-fat diets and gut microbiota-derived SCFAs, such as Bifidobacterium and Roseburia, induce alterations in specific genes involved in the protective effects on NDM by downregulating the TRIB1 gene and upregulating the PGC1α gene. A high-fat diet increases the abundance of P. copri and E. cloacae, which may cause unstable genetic alterations in the neonate’s gut with implications for NDM. The NRF2 and PDX1 genes were downregulated, while the TXNIP gene was upregulated with a high-fat diet. Increased levels of Bacteroides, E. faecalis, and Alistipes in response to a high-fat diet may have a protective role against NDM, which results in upregulation of the NRF2 and PGC1α genes and downregulation of the TRIB1 gene. These bacteria have the ability to produce SCFAs, but further studies are needed to confirm their effects on reducing NDM. The epigenetic mechanisms by which Bacteroidetes P. copri and E. cloacae might be altering gene expression in NDM need to be fully elucidated in further studies. Further studies are also needed to explore the mechanisms for the pro- and anti-inflammatory effects of commensal and pathogenic bacteria on susceptibility to NDM-related genes in response to maternal diet in GDM.
Funding
This review received no financial support.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
| ABCC8 | ATP-binding cassette transporter subfamily C member 8 |
| cAMP | Cyclic AMP |
| CHO | Carbohydrate |
| COX-2 | Cyclooxygenase-2 |
| CPA | Carboxypeptidase A |
| CpG | Cytosine-phosphate-guanine dinucleotides |
| CRP | C-reactive peptide |
| CXCL | C-X-C motif chemokine ligand |
| DCs | Dendritic cells |
| DMGs | Differential methylation genes |
| DNA-PK | DNA-dependent protein kinase |
| EGR-1 | Early Growth Response Gene-1 |
| EIF2AK3 | Eukaryotic translation initiation factor 2-α kinase 3 |
| FFAs | Free fatty acid receptors |
| FoxO1 | Forkhead box O1 |
| FoxP3 | Forkhead box P3 |
| GATA6 | GATA binding protein 6 |
| GCK | Glucokinase |
| GDM | Gestational diabetes |
| GHs | Glycoside hydrolases |
| GLIS3 | GLI-similar 3 |
| GLP-1 | Glucagon-like peptide 1 |
| GPRs | Activate G-protein coupled receptors |
| H2O2 | Hydrogen peroxide |
| HbA1c | Hemoglobin A1c |
| HDACs | Histone deacetylases |
| HDL | High density lipoprotein |
| HLA | Human leukocyte antigen |
| HMOs | Human milk oligosaccharides |
| HOMA-IR | Homeostatic model assessment of insulin resistance |
| IECs | Intestinal epithelial cells |
| IGF | Insulin-like growth factor |
| IL | Interleukins |
| IFN-γ | Interferon-γ |
| lncRNA | Non-coding RNAs |
| INS | Preproinsulin |
| INSR | Insulin receptor |
| IR | Insulin resistance |
| JAK | Janus kinase |
| JNK | c-jun N-terminal kinase |
| KATP | ATP-sensitive potassium |
| KCNJ11 | Potassium inwardly rectifying channel, subfamily J, member 11 |
| LBP | LPS binding protein |
| LDL | Low density lipoprotein |
| LPS | Lipopolysaccharide |
| LRBA | LPS-responsive beige-like anchor |
| MAPK | Mitogen-activated protein kinase |
| MEST | Mesoderm-specific transcript |
| NDM | Neonatal diabetes |
| NF-kB | Nuclear factor-kappa B |
| NLRP3 | Nucleotide-binding oligomerization domain-like receptor family pyrin domain containing 3 |
| iNOS | Nitric oxide synthase |
| NRF2 | NF-E2 related factor 2 |
| OS | Oxidative stress |
| P53 | Protein 53 |
| PDX1 | Pancreatic and duodenal homeobox l |
| PGC1α | PPAR-γ coactivator-1-α |
| PI3K | Phosphatidylinositol-3 kinase |
| PKA PLAG1 | Protein kinase A PLAG1 like zinc finger 1 |
| PNDM | Permanent neonatal diabetes |
| PON1 | Paraoxonase 1 |
| POU2F1 PPP1R13L | POU class 2 homeobox 1 protein phosphatase 1 regulatory subunit 13 like |
| PUFA | Polyunsaturated fatty acid |
| ROS | Reactive oxygen species |
| SCFAs | Short-chain fatty acids |
| SFA | Saturated fatty acid |
| SLC2A2 | Solute carrier family 2 member 2 |
| SLC19A2 | Solute carrier family 19, member 2 |
| SOCS3 | Suppressor of cytokine signaling 3 |
| SRS | Silver-Russell syndrome |
| Srx-1 | Sulfiredoxin-1 |
| STAT3 | Signal transducer and activator of transcription 3 |
| T1D | Type 1 diabetes |
| T2D | Type 2 diabetes |
| TGF-β | Transforming growth factor-β |
| TJ | Tight junction |
| TLR | Toll like receptor |
| TNDM | Transient neonatal diabetes |
| TNF-α | Tumor necrosis factor-α |
| Treg | Regulatory T |
| TRIB1 | Tribbles homolog 1 |
| TXN | Thioredoxin |
| TXNIP | Thioredoxin interacting protein |
| VEGF | Vascular endothelial growth factor |
| VIPR1 | Vasoactive intestinal peptide receptor |
| VLCKD | Very low-calorie ketogenic diet |
| ZEP57 | Zinc finger protein 57 homolog |
References
- Edghill, E.L.; Dix, R.J.; Flanagan, S.E.; Bingley, P.J.; Hattersley, A.T.; Ellard, S.; Gillespie, K.M. HLA genotyping supports a nonautoimmune etiology in patients diagnosed with diabetes under the age of 6 months. Diabetes 2006, 55, 1895–1898. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Cabezas, O.; Ellard, S. Diabetes mellitus in neonates and infants: Genetic heterogeneity, clinical approach to diagnosis, and therapeutic options. Horm. Res. Paediatr. 2013, 80, 137–146. [Google Scholar] [CrossRef]
- Flanagan, S.E.; Haapaniemi, E.; Russell, M.A.; Caswell, R.; Allen, H.L.; De Franco, E.; McDonald, T.J.; Rajala, H.; Ramelius, A.; Barton, J.; et al. Activating germline mutations in STAT3 cause early-onset multi-organ autoimmune disease. Nat. Genet. 2014, 46, 812–814. [Google Scholar] [CrossRef]
- Johnson, M.B.; De Franco, E.; Allen, H.L.; Senani, A.A.; Elbarbary, N.; Siklar, Z.; Berberoglu, M.; Imane, Z.; Haghighi, A.; Razavi, Z.; et al. Recessively inherited LRBA mutations cause autoimmunity presenting as neonatal diabetes. Diabetes 2017, 66, 2316–2322. [Google Scholar] [CrossRef] [PubMed]
- Nishimaki, S.; Yukawa, T.; Makita, Y.; Honda, H.; Kikuchi, N.; Minamisawa, S.; Yokota, S. Transient neonatal diabetes mellitus in extremely preterm infant. Arch. Dis. Child.-Fetal Neonatal Ed. 2008, 93, F240–F241. [Google Scholar] [CrossRef]
- Busiah, K.; Auger, J.; Fauret-Amsellem, A.-L.; Dahan, S.; Pouvreau, N.; Cavé, H.; Polak, M.; Mitanchez, D. Differentiating transient idiopathic hyperglycaemia and neonatal diabetes mellitus in preterm infants. Horm. Res. Paediatr. 2015, 84, 68–72. [Google Scholar] [CrossRef]
- Siklar, Z.; Ellard, S.; Okulu, E.; Berberoğlu, M.; Young, E.; Erdeve, S.S.; Mungan, I.A.; Hacihamdioğlu, B.; Erdeve, O.; Arsan, S.; et al. Transient neonatal diabetes with two novel mutations in the KCNJ11 gene and response to sulfonylurea treatment in a preterm infant. J. Pediatr. Endocrinol. Metab. 2011, 24, 1077–1080. [Google Scholar] [CrossRef]
- Besser, R.E.J.; Flanagan, S.E.; Mackay, D.G.J.; Temple, I.K.; Shepherd, M.H.; Shields, B.M.; Ellard, S.; Hattersley, A.T. Prematurity and genetic testing for neonatal diabetes. Pediatrics 2016, 138, e20153926. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, I.; Iqbal, F.; Thorne, R.F. Editorial: Relationship between gestational and neonatal diabetes mellitus. Front. Endocrinol. 2022, 13, 1060147. [Google Scholar] [CrossRef]
- Perez-Muñoz, M.E.; Arrieta, M.C.; Ramer-Tait, A.E.; Walter, J. A critical assessment of the “sterile womb” and “in utero colonization” hypotheses: Implications for research on the pioneer infant microbiome. Microbiome 2017, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.W.; Clemente, J.C.; Peter, I.; Loos, R.J.F. The prenatal gut microbiome: Are we colonized with bacteria in utero? Pediatr. Obes. 2017, 12, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Senn, V.; Bassler, D.; Choudhury, R.; Scholkmann, F.; Righini-Grunder, F.; Vuille-dit-Bille, R.N.; Restin, T. Microbial colonization from the fetus to early childhood—A comprehensive review. Front. Cell Infect. Microbiol. 2020, 10, 573735. [Google Scholar] [CrossRef] [PubMed]
- Alsharairi, N.A. The infant gut microbiota and risk of asthma: The effect of maternal nutrition during pregnancy and lactation. Microorganisms 2020, 8, 1119. [Google Scholar] [CrossRef]
- Chu, D.M.; Meyer, K.M.; Prince, A.L.; Aagaard, K.M. Impact of maternal nutrition in pregnancy and lactation on offspring gut microbial composition and function. Gut Microbes 2016, 7, 459–470. [Google Scholar] [CrossRef]
- Nuriel-Ohayon, M.; Neuman, H.; Koren, O. Microbial changes during pregnancy, birth, and infancy. Front. Microbiol. 2016, 7, 1031. [Google Scholar] [CrossRef]
- Jeong, S. Factors influencing development of the infant microbiota: From prenatal period to early infancy. Clin. Exp. Pediatr. 2022, 65, 438–447. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The role of short-chain fatty acids in the interplay between a very low-calorie ketogenic diet and the infant gut microbiota and its therapeutic implications for reducing asthma. Int. J. Mol. Sci. 2020, 21, 9580. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The role of short-chain fatty acids in mediating very low-calorie ketogenic diet-infant gut microbiota relationships and its therapeutic potential in obesity. Nutrients 2021, 13, 3702. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The therapeutic role of short-chain fatty acids mediated very low-calorie ketogenic diet-gut microbiota relationships in paediatric inflammatory bowel diseases. Nutrients 2022, 14, 4113. [Google Scholar] [CrossRef] [PubMed]
- Alsharairi, N.A. Therapeutic potential of gut microbiota and its metabolite short-chain fatty acids in neonatal necrotizing enterocolitis. Life 2023, 13, 561. [Google Scholar] [CrossRef]
- Hu, J.; Nomura, Y.; Bashir, A.; Fernandez-Hernandez, H.; Itzkowitz, S.; Pei, Z.; Stone, J.; Loudon, H.; Peter, I. Diversified microbiota of meconium is affected by maternal diabetes status. PLoS ONE 2013, 8, e78257. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Nie, Y.; Shao, R.; Duan, S.; Jiang, Y.; Wang, M.; Xing, Z.; Sun, Q.; Liu, X.; Xu, W. Diversified gut microbiota in newborns of mothers with gestational diabetes mellitus. PLoS ONE 2018, 13, e0205695. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zheng, J.; Shi, W.; Du, N.; Xu, X.; Zhang, Y.; Ji, P.; Zhang, F.; Jia, Z.; Wang, Y.; et al. Dysbiosis of maternal and neonatal microbiota associated with gestational diabetes mellitus. Gut 2018, 67, 1614–1625. [Google Scholar] [CrossRef] [PubMed]
- Hasain, Z.; Mokhtar, N.M.; Kamaruddin, N.A.; Ismail, N.A.M.; Razalli, N.H.; Gnanou, J.V.; Ali, R.A.R. Gut microbiota and gestational diabetes mellitus: A review of host-gut microbiota interactions and their therapeutic potential. Front. Cell Infect. Microbiol. 2020, 10, 188. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Qin, Y.; Chen, M.; Zhang, Y.; Wang, X.; Dong, T.; Chen, G.; Sun, X.; Lu, T.; White, R.A.; et al. Gestational diabetes mellitus is associated with the neonatal gut microbiota and metabolome. BMC Med. 2021, 19, 120. [Google Scholar] [CrossRef]
- Ferrocino, I.; Ponzo, V.; Gambino, R.; Zarovska, A.; Leone, F.; Monzeglio, C.; Goitre, I.; Rosato, R.; Romano, A.; Grassi, G.; et al. Changes in the gut microbiota composition during pregnancy in patients with gestational diabetes mellitus (GDM). Sci. Rep. 2018, 8, 12216. [Google Scholar] [CrossRef]
- Sugino, K.Y.; Hernandez, T.L.; Barbour, L.A.; Kofonow, J.M.; Frank, D.N.; Friedman, J.E. A maternal higher-complex carbohydrate diet increases bifidobacteria and alters early life acquisition of the infant microbiome in women with gestational diabetes mellitus. Front. Endocrinol. 2022, 13, 921464. [Google Scholar] [CrossRef]
- Kocova, M. Genetic spectrum of neonatal diabetes. Balkan J. Med. Genet. 2020, 23, 5–15. [Google Scholar] [CrossRef]
- Greeley, S.A.W.; Tucker, S.E.; Naylor, R.N.; Bell, G.I.; Philipson, L.H. Neonatal diabetes mellitus: A model for personalized medicine. Trends Endocrinol. Metab. 2010, 21, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Greeley, S.A.W.; Naylor, R.N.; Philipson, L.H.; Bell, G.I. Neonatal diabetes: An expanding list of genes allows for improved diagnosis and treatment. Curr. Diabetes Rep. 2011, 11, 519–532. [Google Scholar] [CrossRef]
- Naylor, R.N.; Greeley, S.A.W.; Bell, G.I.; Philipson, L.H. Genetics and pathophysiology of neonatal diabetes mellitus. J. Diabetes Investig. 2011, 2, 158–169. [Google Scholar] [CrossRef]
- Vaxillaire, M.; Bonnefond, A.; Froguel, P. The lessons of early-onset monogenic diabetes for the understanding of diabetes pathogenesis. Best. Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 171–187. [Google Scholar] [CrossRef] [PubMed]
- Zübarioğlu, A.U.; Bülbül, A.; Uslu, H.S. Neonatal diabetes mellitus. Sisli Etfal Hastan. Tip Bülteni 2018, 52, 71–78. [Google Scholar] [CrossRef]
- Dahl, A.; Kumar, S. Recent Advances in Neonatal Diabetes. Diabetes Metab. Syndr. Obes. 2020, 13, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Colclough, K.; Gloyn, A.L.; Pollin, T.I. Monogenic diabetes: A gateway to precision medicine in diabetes. J. Clin. Investig. 2021, 131, e142244. [Google Scholar] [CrossRef] [PubMed]
- Bak, M.; Boonen, S.E.; Dahl, C.; Hahnemann, J.M.D.; Mackay, D.J.D.G.; Tümer, Z.; Grønskov, K.; Temple, I.K.; Guldberg, P.; Tommerup, N. Genome-wide DNA methylation analysis of transient neonatal diabetes type 1 patients with mutations in ZFP57. BMC Med. Genet. 2016, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Mackay, D.J.G.; Temple, I.K. Transient neonatal diabetes mellitus type 1. Am. J. Med. Genet. C Semin. Med. Genet. 2010, 154C, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Akerman, I.; Maestro, M.A.; De Franco, E.; Grau, V.; Flanagan, S.; García-Hurtado, J.; Mittler, G.; Ravassard, P.; Piemonti, L.; Ellard, S.; et al. Neonatal diabetes mutations disrupt a chromatin pioneering function that activates the human insulin gene. Cell Rep. 2021, 35, 108981. [Google Scholar] [CrossRef]
- Hammoud, B.; Greeley, S.A.W. Growth and development in monogenic forms of neonatal diabetes. Curr. Opin. Endocrinol. Diabetes Obes. 2022, 29, 65–77. [Google Scholar] [CrossRef]
- Johnson, M.B.; Patel, K.A.; De Franco, E.; Hagopian, W.; Killian, M.; McDonald, T.J.; Tree, T.I.M.; Domingo-Vila, C.; Hudson, M.; Hammersley, S.; et al. Type 1 diabetes can present before the age of 6 months and is characterized by autoimmunity and rapid loss of beta cells. Diabetologia 2020, 63, 2605–2615. [Google Scholar] [CrossRef]
- Yan, J.; Yang, H. Gestational diabetes mellitus, programing and epigenetics. J. Matern. Fetal Neonatal Med. 2014, 27, 1266–1269. [Google Scholar] [CrossRef] [PubMed]
- Hjort, L.; Martino, D.; Grunnet, L.G.; Naeem, H.; Maksimovic, J.; Olsson, A.H.; Zhang, C.; Ling, C.; Olsen, S.F.; Saffery, R.; et al. Gestational diabetes and maternal obesity are associated with epigenome-wide methylation changes in children. JCI Insight 2018, 3, e122572. [Google Scholar] [CrossRef] [PubMed]
- Hjort, L.; Novakovic, B.; Grunnet, L.G.; Maple-Brown, L.; Damm, P.; Desoye, G.; Saffery, R. Diabetes in pregnancy and epigenetic mechanisms-how the first 9 months from conception might affect the child’s epigenome and later risk of disease. Lancet Diabetes Endocrinol. 2019, 7, 796–806. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Wang, J.; Kakongoma, N.; Hua, W.; Xu, J.; Wang, Y.; He, S.; Gu, H.; Shi, J.; Hu, W. DNA methylation and expression profiles of placenta and umbilical cord blood reveal the characteristics of gestational diabetes mellitus patients and offspring. Clin. Epigenetics 2022, 14, 69. [Google Scholar] [CrossRef] [PubMed]
- Ott, R.; Stupin, J.H.; Melchior, K.; Schellong, K.; Ziska, T.; Dudenhausen, J.W.; Henrich, W.; Rancourt, R.C.; Plagemann, A. Alterations of adiponectin gene expression and DNA methylation in adipose tissues and blood cells are associated with gestational diabetes and neonatal outcome. Clin. Epigenetics 2018, 10, 131. [Google Scholar] [CrossRef]
- Kang, J.; Lee, C.-N.; Li, H.-Y.; Hsu, K.-H.; Lin, S.-Y. Genome-wide DNA methylation variation in maternal and cord blood of gestational diabetes population. Diabetes Res. Clin. Pract. 2017, 132, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Ruchat, S.-M.; Houde, A.-A.; Voisin, G.; St-Pierre, J.; Perron, P.; Baillargeon, J.-P.; Gaudet, D.; Hivert, M.-F.; Brisson, D.; Bouchard, L. Gestational diabetes mellitus epigenetically affects genes predominantly involved in metabolic diseases. Epigenetics 2013, 9, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Winzell, M.S.; Ahrén, B. Role of VIP and PACAP in islet function. Peptides 2007, 28, 1805–1813. [Google Scholar] [CrossRef]
- Soubeyrand, S.; Martinuk, A.; Naing, T.; Lau, P.; McPherson, R. Role of Tribbles Pseudokinase 1 (TRIB1) in human hepatocyte metabolism. Biochim. Biophys. Acta 2016, 1862, 223–232. [Google Scholar] [CrossRef]
- Popova, P.V.; Vasileva, L.B.; Tkachuk, A.S.; Puzanov, M.V.; Bolotko, Y.A.; Pustozerov, E.A.; Gerasimov, A.S.; Zazerskaya, I.E.; Li, O.A.; Vasilyeva, E.Y.; et al. Association of tribbles homologue 1 gene expression in human umbilical vein endothelial cells with duration of intrauterine exposure to hyperglycaemia. Genet. Res. 2018, 100, e3. [Google Scholar] [CrossRef]
- Sukarieh, R.; Joseph, R.; Leow, S.C.; Li, Y.; Löffler, M.; Aris, I.M.; Tan, J.H.; Teh, A.L.; Chen, L.; Holbrook, J.D.; et al. Molecular pathways reflecting poor intrauterine growth are found in Wharton’s jelly-derived mesenchymal stem cells. Hum. Reprod. 2014, 29, 2287–2301. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Liang, R.; Liu, T.; Wang, L.; Zou, J.; Liu, N.; Liu, Y.; Cai, X.; Liu, Y.; Ding, X.; et al. Opposing effects of IL-1β/COX-2/PGE2 pathway loop on islets in type 2 diabetes mellitus. Endocr. J. 2019, 66, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Dong, S.; Wu, L.; Bai, Y.; Bi, X.; Li, Y.; Shu, C. Maternal and placental DNA methylation changes associated with the pathogenesis of gestational diabetes mellitus. Nutrients 2023, 15, 70. [Google Scholar] [CrossRef]
- Hjort, L.; Novakovic, B.; Cvitic, S.; Saffery, R.; Damm, P.; Desoye, G. Placental DNA methylation in pregnancies complicated by maternal diabetes and/or obesity: State of the art and research gaps. Epigenetics 2022, 17, 2188–2208. [Google Scholar] [CrossRef]
- Xie, X.; Gao, H.; Zeng, W.; Chen, S.; Feng, L.; Deng, D.; Qiao, F.-Y.; Liao, L.; McCormick, K.; Ning, Q.; et al. Placental DNA methylation of peroxisome-proliferator-activated receptor-γ co-activator-1α promoter is associated with maternal gestational glucose level. Clin. Sci. 2015, 129, 385–394. [Google Scholar] [CrossRef]
- Ruschke, K.; Fishbein, L.; Dietrich, A.; Klöting, N.; Tönjes, A.; Oberbach, A.; Fasshauer, M.; Jenkner, J.; Schön, M.R.; Stumvoll, M.; et al. Gene expression of PPARgamma and PGC-1alpha in human omental and subcutaneous adipose tissues is related to insulin resistance markers and mediates beneficial effects of physical training. Eur. J. Endocrinol. 2010, 162, 515–523. [Google Scholar] [CrossRef]
- Côté, S.; Gagné-Ouellet, V.; Guay, S.-P.; Allard, C.; Houde, A.-A.; Perron, P.; Baillargeon, J.-P.; Gaudet, D.; Guérin, R.; Brisson, D.; et al. PPARGC1α gene DNA methylation variations in human placenta mediate the link between maternal hyperglycemia and leptin levels in newborns. Clin. Epigenetics 2016, 8, 72. [Google Scholar] [CrossRef]
- Gao, Y.; She, R.; Sha, W. Gestational diabetes mellitus is associated with decreased adipose and placenta peroxisome proliferator-activator receptor γ expression in a Chinese population. Oncotarget 2017, 8, 113928–113937. [Google Scholar] [CrossRef]
- Wang, L.; Fan, H.; Zhou, L.; Wu, Y.; Lu, H.; Luo, J. Altered expression of PGC-1α and PDX1 and their methylation status are associated with fetal glucose metabolism in gestational diabetes mellitus. Biochem. Biophys. Res. Commun. 2018, 501, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Higazy, R.; Gauda, E.B. PGC-1α activity and mitochondrial dysfunction in preterm infants. Front. Physiol. 2022, 13, 997619. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Leahy, A.A.; Monga, N.; Peshavaria, M.; Jetton, T.L.; Leahy, J.L. Peroxisome proliferator-activated receptor γ (PPARγ) and its target genes are downstream effectors of FoxO1 protein in islet β-cells: Mechanism of β-cell compensation and failure. J. Biol. Chem. 2013, 288, 25440–25449. [Google Scholar] [CrossRef]
- El Hajj, N.; Pliushch, G.; Schneider, E.; Dittrich, M.; Müller, T.; Korenkov, M.; Aretz, M.; Zechner, U.; Lehnen, H.; Haaf, T. Metabolic programming of MEST DNA methylation by intrauterine exposure to gestational diabetes mellitus. Diabetes 2013, 62, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Weng, X.; Liu, F.; Zhang, H.; Kan, M.; Wang, T.; Dong, M.; Liu, Y. Genome-wide DNA methylation profiling in infants born to gestational diabetes mellitus. Diabetes Res. Clin. Pract. 2018, 142, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Bentley, L.; Nakabayashi, K.; Monk, D.; Beechey, C.; Peters, J.; Birjandi, Z.; Khayat, F.E.; Patel, M.; Preece, M.A.; Stanier, P.; et al. The imprinted region on human chromosome 7q32 extends to the carboxypeptidase A gene cluster: An imprinted candidate for Silver-Russell syndrome. J. Med. Genet. 2003, 40, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Sparago, A.; Cerrato, F.; Riccio, A. Is ZFP57 binding to H19/IGF2:IG-DMR affected in Silver-Russell syndrome? Clin. Epigenetics 2018, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Brereton, R.E.; Nickerson, S.L.; Woodward, K.J.; Edwards, T.; Sivamoorthy, S.; Walters, F.R.V.; Chabros, V.; Marchin, V.; Grumball, T.; Kennedy, D.; et al. Further heterogeneity in Silver-Russell syndrome: PLAG1 deletion in association with a complex chromosomal rearrangement. Am. J. Med. Genet. A 2021, 185, 3136–3145. [Google Scholar] [CrossRef] [PubMed]
- Quilter, C.R.; Cooper, W.N.; Cliffe, K.M.; Skinner, B.M.; Prentice, P.M.; Nelson, L.; Bauer, J.; Ong, K.K.; Constância, M.; Lowe, W.L.; et al. Impact on offspring methylation patterns of maternal gestational diabetes mellitus and intrauterine growth restraint suggest common genes and pathways linked to subsequent type 2 diabetes risk. FASEB J. 2014, 28, 4868–4879. [Google Scholar] [CrossRef]
- Ng, M.C.Y.; Lam, V.K.L.; Tam, C.H.T.; Chan, A.W.H.; So, W.-Y.; Ma, R.C.W.; Zee, B.C.Y.; Waye, M.M.Y.; Mak, W.W.; Hu, C.; et al. Association of the POU class 2 homeobox 1 gene (POU2F1) with susceptibility to Type 2 diabetes in Chinese populations. Diabet. Med. 2010, 27, 1443–1449. [Google Scholar] [CrossRef]
- Wang, P.; Jin, T. Hydrogen peroxide stimulates nuclear import of the POU homeodomain protein Oct-1 and its repressive effect on the expression of Cdx-2. BMC Cell Biol. 2010, 11, 56. [Google Scholar] [CrossRef]
- Primo-Parmo, S.L.; Sorenson, R.C.; Teiber, J.; Du, B.N.L. The human serum paraoxonase/arylesterase gene (PON1) is one member of a multigene family. Genomics 1996, 33, 498–507. [Google Scholar] [CrossRef]
- León, I.; Roldán, S.H.; José Rodrigo, M.; Rodríguez, M.L.; Fisher, J.; Mitchell, C.; Lage-Castellanos, A. The shared mother-child epigenetic signature of neglect is related to maternal adverse events. Front. Physiol. 2022, 13, 966740. [Google Scholar] [CrossRef]
- Pappa, K.I.; Gazouli, M.; Anastasiou, E.; Loutradis, D.; Anagnou, N.P. The Q192R polymorphism of the paraoxonase-1 (PON1) gene is associated with susceptibility to gestational diabetes mellitus in the Greek population. Gynecol. Endocrinol. 2017, 33, 617–620. [Google Scholar] [CrossRef]
- Zhou, M.; Liu, X.-H.; Liu, Q.-Q.; Chen, M.; Bai, H.; Jiang, C.-Y.; Guan, L.-B.; Fan, P. Lactonase activity and status of paraoxonase 1 and oxidative stress in neonates of women with gestational diabetes mellitus. Pediatr. Res. 2021, 89, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Gugliucci, A.; Numaguchi, M.; Caccavello, R.; Kimura, S. Paraoxonase 1 lactonase activity and distribution in the HDL subclasses in the cord blood. Redox Rep. 2014, 19, 124–132. [Google Scholar] [CrossRef]
- Cheng, X.; Siow, R.C.M.; Mann, G.E. Impaired redox signaling and antioxidant gene expression in endothelial cells in diabetes: A role for mitochondria and the nuclear factor-E2-related factor 2-Kelch-like ECH-associated protein 1 defense pathway. Antioxid. Redox Signal. 2011, 14, 469–487. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Chapple, S.J.; Patel, B.; Puszyk, W.; Sugden, D.; Yin, X.; Mayr, M.; Siow, R.C.M.; Mann, G.E. Gestational diabetes mellitus impairs Nrf2-mediated adaptive antioxidant defenses and redox signaling in fetal endothelial cells in utero. Diabetes 2013, 62, 4088–4097. [Google Scholar] [CrossRef] [PubMed]
- Baumel-Alterzon, S.; Scott, D.K. Regulation of Pdx1 by oxidative stress and Nrf2 in pancreatic beta-cells. Front. Endocrinol. 2022, 13, 1011187. [Google Scholar] [CrossRef] [PubMed]
- Tobi, E.W.; Juvinao-Quintero, D.L.; Ronkainen, J.; Ott, R.; Alfano, R.; Canouil, M.; Geurtsen, M.L.; Khamis, A.; Küpers, L.K.; Lim, I.Y.; et al. Maternal glycemic dysregulation during pregnancy and neonatal blood DNA methylation: Meta-analyses of epigenome-wide association studies. Diabetes Care 2022, 45, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Wondafrash, D.Z.; Nire’a, A.T.; Tafere, G.G.; Desta, D.M.; Berhe, D.A.; Zewdie, K.A. Thioredoxin-interacting protein as a novel potential therapeutic target in diabetes mellitus and its underlying complications. Diabetes Metab. Syndr. Obes. 2020, 13, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Basnet, R.; Basnet, T.B.; Basnet, B.B.; Khadka, S. Overview on thioredoxin-interacting protein (TXNIP): A potential target for diabetes intervention. Curr. Drug. Targets 2022, 23, 761–767. [Google Scholar] [CrossRef]
- Sarina; Li, D.F.; Feng, Z.Q.; Du, J.; Zhao, W.H.; Huang, N.; Jia, J.C.; Wu, Z.Y.; Alamusi; Wang, Y.Y.; et al. Mechanism of placenta damage in gestational diabetes mellitus by investigating TXNIP of patient samples and gene functional research in cell line. Diabetes Ther. 2019, 10, 2265–2288. [Google Scholar] [CrossRef]
- Pasternak, Y.; Ohana, M.; Biron-Shental, T.; Cohen-Hagai, K.; Benchetrit, S.; Zitman-Gal, T. Thioredoxin, thioredoxin interacting protein and transducer and activator of transcription 3 in gestational diabetes. Mol. Biol. Rep. 2020, 47, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Velayos, T.; Martínez, R.; Alonso, M.; Garcia-Etxebarria, K.; Aguayo, A.; Camarero, C.; Urrutia, I.; Martínez de LaPiscina, I.; Barrio, R.; Santin, I.; et al. An activating mutation in STAT3 results in neonatal diabetes through reduced insulin synthesis. Diabetes 2017, 66, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, P.; Metos, J.; Babu, P.V.A. Impact of type 1 diabetes on the composition and functional potential of gut microbiome in children and adolescents: Possible mechanisms, current knowledge, and challenges. Gut Microbes 2021, 13, 1926841. [Google Scholar] [CrossRef] [PubMed]
- Del Chierico, F.; Rapini, N.; Deodati, A.; Matteoli, M.C.; Cianfarani, S.; Putignani, L. Pathophysiology of type 1 diabetes and gut microbiota role. Int. J. Mol. Sci. 2022, 23, 14650. [Google Scholar] [CrossRef]
- Yang, Q.; Ouyang, J.; Sun, F.; Yang, J. Short-chain fatty acids: A soldier fighting against inflammation and protecting from tumorigenesis in people with diabetes. Front. Immunol. 2020, 11, 590685. [Google Scholar] [CrossRef]
- Yi, C.; Sun, W.; Ding, L.; Yan, M.; Sun, C.; Qiu, C.; Wang, D.; Wu, L. Short-chain fatty acids weaken ox-LDL-induced cell inflammatory injury by inhibiting the NLRP3/Caspase-1 pathway and affecting cellular metabolism in THP-1 cells. Molecules 2022, 27, 8801. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, Y.; Wang, P.; Huang, Y.; Wang, F. Short-chain fatty acids manifest stimulative and protective effects on intestinal barrier function through the inhibition of NLRP3 inflammasome and autophagy. Cell Physiol. Biochem. 2018, 49, 190–205. [Google Scholar] [CrossRef]
- Yaku, K.; Enami, Y.; Kurajyo, C.; Matsui-Yuasa, I.; Konishi, Y.; Kojima-Yuasa, A. The enhancement of phase 2 enzyme activities by sodium butyrate in normal intestinal epithelial cells is associated with Nrf2 and p53. Mol. Cell Biochem. 2012, 370, 7–14. [Google Scholar] [CrossRef]
- Milani, C.; Mancabelli, L.; Lugli, G.A.; Duranti, S.; Turroni, F.; Ferrario, C.; Mangifesta, M.; Viappiani, A.; Ferretti, P.; Gorfer, V.; et al. Exploring vertical transmission of Bifidobacteria from mother to child. Appl. Environ. Microbiol. 2015, 81, 7078–7087. [Google Scholar] [CrossRef]
- Asnicar, F.; Manara, F.; Zolfo, M.; Truong, D.T.; Scholz, M.; Armanini, F.; Ferretti, P.; Gorfer, V.; Pedrotti, A.; Tett, A.; et al. Studying vertical microbiome transmission from mothers to infants by strain-level metagenomic profiling. mSystems 2017, 2, e00164-16. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, P.; Pasolli, E.; Tett, A.; Asnicar, F.; Gorfer, V.; Fedi, S.; Armanini, F.; Truong, D.T.; Manara, S.; Zolfo, M.; et al. Mother-to-infant microbial transmission from different body sites shapes the developing infant gut microbiome. Cell Host Microbe. 2018, 24, 133–145.e5. [Google Scholar] [CrossRef]
- Koo, H.; McFarland, B.C.; Hakim, J.A.; Crossman, D.K.; Crowley, M.R.; Rodriguez, J.M.; Benveniste, E.N.; Morrow, C.D. An individualized mosaic of maternal microbial strains is transmitted to the infant gut microbial community. R. Soc. Open. Sci. 2020, 7, 192200. [Google Scholar] [CrossRef] [PubMed]
- Ponzo, V.; Ferrocino, I.; Zarovska, A.; Amenta, M.B.; Leone, F.; Monzeglio, C.; Rosato, R.; Pellegrini, M.; Gambino, R.; Cassader, M.; et al. The microbiota composition of the offspring of patients with gestational diabetes mellitus (GDM). PLoS ONE 2019, 14, e0226545. [Google Scholar] [CrossRef] [PubMed]
- Kuang, Y.-S.; Lu, J.-H.; Li, S.-H.; Li, J.-H.; Yuan, M.-Y.; He, J.-R.; Chen, N.-N.; Xiao, W.-Q.; Shen, S.-Y.; Qiu, L.; et al. Connections between the human gut microbiome and gestational diabetes mellitus. Gigascience 2017, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Soderborg, T.K.; Carpenter, C.M.; Janssen, R.C.; Weir, T.L.; Robertson, C.E.; Ir, D.; Young, B.E.; Krebs, N.F.; Hernandez, T.L.; Barbour, L.A.; et al. Gestational diabetes is uniquely associated with altered early seeding of the infant gut microbiota. Front. Endocrinol. 2020, 11, 603021. [Google Scholar] [CrossRef]
- Gopalsamy, G.; Mortimer, E.; Greenfield, P.; Bird, A.R.; Young, G.P.; Christophersen, C.T. Resistant starch is actively fermented by infant faecal microbiota and increases microbial diversity. Nutrients 2019, 11, 1345. [Google Scholar] [CrossRef]
- Nurmi, J.T.; Puolakkainen, P.A.; Rautonen, N.E. Bifidobacterium lactis sp. 420 up-regulates cyclooxygenase (Cox)-1 and down-regulates Cox-2 gene expression in a Caco-2 cell culture model. Nutr. Cancer 2005, 51, 83–892. [Google Scholar] [CrossRef]
- Kawabata, K.; Baba, N.; Sakano, T.; Hamano, Y.; Taira, S.; Tamura, A.; Baba, S.; Natsume, M.; Ishii, T.; Murakami, S.; et al. Functional properties of anti-inflammatory substances from quercetin-treated Bifidobacterium adolescentis. Biosci. Biotechnol. Biochem. 2018, 82, 689–697. [Google Scholar] [CrossRef]
- Jost, T.; Lacroix, C.; Braegger, C.P.; Rochat, F.; Chassard, C. Vertical mother-neonate transfer of maternal gut bacteria via breastfeeding. Environ. Microbiol. 2014, 16, 2891–2904. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yu, D.; Wang, Y.; Yuan, H.; Ning, X.; Rui, B.; Lei, Z.; Yuan, J.; Yan, J.; Li, M. The intestinal dysbiosis of mothers with gestational diabetes mellitus (GDM) and its impact on the gut microbiota of their newborns. Can. J. Infect. Dis. Med. Microbiol. 2021, 2021, 3044534. [Google Scholar] [CrossRef] [PubMed]
- Arif, S.; Moore, F.; Marks, K.; Bouckenooghe, T.; Dayan, C.M.; Planas, R.; Vives-Pi, M.; Powrie, J.; Tree, T.; Marchetti, O.; et al. Peripheral and islet interleukin-17 pathway activation characterizes human autoimmune diabetes and promotes cytokine-mediated β-cell death. Diabetes 2011, 60, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Nepelska, M.; de Wouters, T.; Jacouton, E.; Béguet-Crespel, F.; Lapaque, N.; Doré, J.; Arulampalam, V.; Blottière, H.M. Commensal gut bacteria modulate phosphorylation-dependent PPARγ transcriptional activity in human intestinal epithelial cells. Sci. Rep. 2017, 7, 43199. [Google Scholar] [CrossRef] [PubMed]
- Bhagwat, A.; Annapure, U.S. Maternal-neonatal transmission of Enterococcus strains during delivery. Beni-Suef Univ. J. Basic. Appl. Sci. 2019, 8, 25. [Google Scholar] [CrossRef]
- Vitetta, L.; Coulson, S.; Thomsen, M.; Nguyen, T.; Hall, S. Probiotics D-lactic acidosis, oxidative stress and strain specificity. Gut Microbes 2017, 8, 311–322. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ishii, M.; Hasegawa, S.; Sekimizu, K. Enterococcus faecalis YM0831 suppresses sucrose-induced hyperglycemia in a silkworm model and in humans. Commun. Biol. 2019, 2, 157. [Google Scholar] [CrossRef]
- Are, A.; Aronsson, L.; Wang, S.; Greicius, G.; Lee, Y.K.; Gustafsson, J.-A.; Pettersson, S.; Arulampalam, V. Enterococcus faecalis from newborn babies regulate endogenous PPARgamma activity and IL-10 levels in colonic epithelial cells. Proc. Natl. Acad. Sci. USA 2008, 105, 1943–1948. [Google Scholar] [CrossRef]
- Maqsood, R.; Rodriguez, R.R.C.; Handley, S.A.; Ndao, I.M.; Tarr, P.I.; Warner, B.B.; Lim, E.S.; Holtz, L.R. Discordant transmission of bacteria and viruses from mothers to babies at birth. Microbiome 2019, 7, 156. [Google Scholar] [CrossRef]
- Chen, F.; Gan, Y.; Li, Y.; He, W.; Wu, W.; Wang, K.; Li, Q. Association of gestational diabetes mellitus with changes in gut microbiota composition at the species level. BMC Microbiol. 2021, 21, 147. [Google Scholar] [CrossRef]
- Su, Y.; Wang, H.K.; Gan, X.P.; Chen, L.; Cao, Y.N.; Cheng, D.C.; Zhang, D.Y.; Liu, W.Y.; Li, F.F.; Xu, X.M. Alterations of gut microbiota in gestational diabetes patients during the second trimester of pregnancy in the Shanghai Han population. J. Transl. Med. 2021, 19, 366. [Google Scholar] [CrossRef]
- Song, Z.; Li, S.; Li, R. An investigation into the correlation of intestinal flora with obesity and gestational diabetes mellitus. Comput. Math. Methods Med. 2022, 2022, 5677073. [Google Scholar] [CrossRef] [PubMed]
- Talford, L.E.; Crost, E.H.; Kavanaugh, D.; Juge, N. Mucin glycan foraging in the human gut microbiome. Front. Genet. 2005, 6, 81. [Google Scholar] [CrossRef]
- Glover, J.S.; Ticer, T.D.; Engevik, M.A. Characterizing the mucin-degrading capacity of the human gut microbiota. Sci. Rep. 2022, 12, 8456. [Google Scholar] [CrossRef] [PubMed]
- Koh, A.; De Vadder, F.; Kovatcheva-datchary, P.; Backhed, F. From dietary fiber to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef]
- Leite, A.Z.; de Campos Rodrigues, N.; Gonzaga, M.I.; Paiolo, J.C.C.; Arantes de Souza, C.; Stefanutto, N.A.V.; Omori, W.P.; Guariz Pinheiro, D.; Brisotti, J.L.; Junior, E.M.; et al. Detection of increased plasma interleukin-6 levels and prevalence of Prevotella copri and Bacteroides vulgatus in the feces of type 2 diabetes patients. Front. Immunol. 2017, 8, 1107. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.I.; Choi, J.H.; Lee, K.H.; Kim, J.M. Bacteroides fragilis enterotoxin induces sulfiredoxin-1 expression in intestinal epithelial cell lines through a mitogen-activated protein kinases- and Nrf2-dependent pathway, leading to the suppression of apoptosis. Int. J. Mol. Sci. 2020, 21, 5383. [Google Scholar] [CrossRef]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef]
- Crusell, M.K.W.; Hansen, T.H.; Nielsen, T.; Allin, K.H.; Rühlemann, M.C.; Damm, P.; Vestergaard, H.; Rørbye, C.; Jørgensen, N.R.; Christiansen, O.B.; et al. Gestational diabetes is associated with change in the gut microbiota composition in third trimester of pregnancy and postpartum. Microbiome 2018, 6, 89. [Google Scholar] [CrossRef]
- Wu, Y.; Bible, P.W.; Long, S.; Ming, W.-K.; Ding, W.; Long, Y.; Wen, X.; Li, X.; Deng, X.; Deng, Y.; et al. Metagenomic analysis reveals gestational diabetes mellitus-related microbial regulators of glucose tolerance. Acta Diabetol. 2020, 57, 569–581. [Google Scholar] [CrossRef]
- Gavin, P.G.; Mullaney, J.A.; Loo, D.; Lê Cao, K.-A.; Gottlieb, P.A.; Hill, M.M.; Zipris, D.; Hamilton-Williams, E.E. Intestinal metaproteomics reveals host-microbiota interactions in subjects at risk for type 1 diabetes. Diabetes Care 2018, 41, 2178–2186. [Google Scholar] [CrossRef]
- d’Hennezel, E.; Abubucker, S.; Murphy, L.O.; Cullen, T.W. Total lipopolysaccharide from the human gut microbiome silences toll-like receptor signaling. mSystems 2017, 2, e00046-17. [Google Scholar] [CrossRef] [PubMed]
- Groh, I.A.M.; Riva, A.; Braun, D.; Sutherland, H.G.; Williams, O.; Bakuradze, T.; Pahlke, G.; Richling, E.; Haupt, L.M.; Griffiths, L.R.; et al. Long-term consumption of anthocyanin-rich fruit juice: Impact on gut microbiota and antioxidant markers in lymphocytes of healthy males. Antioxidants 2020, 10, 27. [Google Scholar] [CrossRef]
- Hernandez-Sanabria, E.; Heiremans, E.; Arroyo, M.C.; Props, R.; Leclercq, L.; Snoeys, J.; Van de Wiele, T. Short-term supplementation of celecoxib-shifted butyrate production on a simulated model of the gut microbial ecosystem and ameliorated in vitro inflammation. NPJ Biofilms Microbiomes 2020, 6, 9. [Google Scholar] [CrossRef]
- Pinto, Y.; Frishman, S.; Turjeman, S.; Eshel, A.; Nuriel-Ohayon, M.; Shrossel, O.; Ziv, O.; Walters, W.; Parsonnet, J.; Ley, C.; et al. Gestational diabetes is driven by microbiota-induced inflammation months before diagnosis. Gut 2023, 72, 918–928. [Google Scholar] [CrossRef]
- Larsen, J.M. The immune response to Prevotella bacteria in chronic inflammatory disease. Immunology 2017, 151, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, H.K.; Gudmundsdottir, V.; Nielsen, H.B.; Hyotylainen, T.; Nielsen, T.; Jensen, B.A.H.; Forslund, K.; Hildebrand, F.; Prifti, E.; Falony, G.; et al. Human gut microbes impact host serum metabolome and insulin sensitivity. Nature 2016, 535, 376–381. [Google Scholar] [CrossRef]
- Tarallo, S.; Ferrero, G.; De Filippis, F.; Francavilla, A.; Pasolli, E.; Panero, V.; Cordero, F.; Segata, N.; Grioni, S.; Pensa, R.G.; et al. Stool microRNA profiles reflect different dietary and gut microbiome patterns in healthy individuals. Gut 2022, 71, 1302–1314. [Google Scholar] [CrossRef]
- Linna-Kuosmanen, S.; Bosch, V.T.; Moreau, P.R.; Bouvy-Liivrand, M.; Niskanen, H.; Kansanen, E.; Kivelä, A.; Hartikainen, J.; Hippeläinen, M.; Kokki, H.; et al. NRF2 is a key regulator of endothelial microRNA expression under proatherogenic stimuli. Cardiovasc. Res. 2021, 117, 1339–1357. [Google Scholar] [CrossRef] [PubMed]
- Davin-Regli, A.; Pagès, J.-M. Enterobacter aerogenes and Enterobacter cloacae; versatile bacterial pathogens confronting antibiotic treatment. Front. Microbiol. 2015, 6, 392. [Google Scholar] [CrossRef]
- Scheithauer, T.P.M.; Herrema, H.; Yu, H.; Bakker, G.J.; Winkelmeijer, M.; Soukhatcheva, G.; Dai, D.; Ma, C.; Havik, S.R.; Balvers, M.; et al. Gut-derived bacterial flagellin induces beta-cell inflammation and dysfunction. Gut Microbes. 2022, 14, 2111951. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
DNA methylation as a mechanism for NDM-related genes in neonates exposed to GDM. Seven differentially expressed genes involved in NDM were identified, consisting of four upregulated genes (TRIB1, POU2F1, PON1, TXNIP) and three downregulated genes (PGC1α, MEST, and NRF2). (↓) decrease, (↑) increase.
Figure 1.
DNA methylation as a mechanism for NDM-related genes in neonates exposed to GDM. Seven differentially expressed genes involved in NDM were identified, consisting of four upregulated genes (TRIB1, POU2F1, PON1, TXNIP) and three downregulated genes (PGC1α, MEST, and NRF2). (↓) decrease, (↑) increase.

Figure 2.
The diet-gut microbiota-epigenetics crosstalk relevant to gene expression alterations in NDM. Maternal diet in GDM (complex CHO/fiber, low/high fat) influences the newborn’s gut microbiota-derived SCFAs. SCFAs produced by B. adolescentis, Roseburia, E. faecalis, B. fragilis, and Alistipes may act as epigenetic modifiers by inhibiting HDACs and activating GPRs and FFAs, thereby reducing the risk of NDM by increasing gene expression levels of PGC1α and NRF2 and decreasing gene expression levels of TRIB1 and TXNIP. An increased abundance of P. copri was associated with reduced fecal levels of SCFAs, which drive unstable genetic changes in the offspring’s gut by reducing NRF2 gene expression. An increased abundance of E. cloacae was associated with an increased gene expression level of TXNIP and a decreased gene expression level of PDX1. (↓) decrease, (↑) increase.
Figure 2.
The diet-gut microbiota-epigenetics crosstalk relevant to gene expression alterations in NDM. Maternal diet in GDM (complex CHO/fiber, low/high fat) influences the newborn’s gut microbiota-derived SCFAs. SCFAs produced by B. adolescentis, Roseburia, E. faecalis, B. fragilis, and Alistipes may act as epigenetic modifiers by inhibiting HDACs and activating GPRs and FFAs, thereby reducing the risk of NDM by increasing gene expression levels of PGC1α and NRF2 and decreasing gene expression levels of TRIB1 and TXNIP. An increased abundance of P. copri was associated with reduced fecal levels of SCFAs, which drive unstable genetic changes in the offspring’s gut by reducing NRF2 gene expression. An increased abundance of E. cloacae was associated with an increased gene expression level of TXNIP and a decreased gene expression level of PDX1. (↓) decrease, (↑) increase.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alsharairi, N.A. Exploring the Diet-Gut Microbiota-Epigenetics Crosstalk Relevant to Neonatal Diabetes. Genes 2023, 14, 1017. https://doi.org/10.3390/genes14051017
AMA Style
Alsharairi NA. Exploring the Diet-Gut Microbiota-Epigenetics Crosstalk Relevant to Neonatal Diabetes. Genes. 2023; 14(5):1017. https://doi.org/10.3390/genes14051017
Chicago/Turabian StyleAlsharairi, Naser A. 2023. "Exploring the Diet-Gut Microbiota-Epigenetics Crosstalk Relevant to Neonatal Diabetes" Genes 14, no. 5: 1017. https://doi.org/10.3390/genes14051017
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.