
Genome-Wide Associations and Confirmatory Meta-Analyses in Diabetic Retinopathy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of DR GWASs and Data Extraction
2.2. Identification of Overlapping Signals between GWASs
2.3. Genetic Meta-Analysis
2.4. Functional Annotation of SNPs and Gene Loci
3. Results
3.1. Genome-Wide Associations of DR
3.2. Genome-Wide Associations of PDR and DME
3.3. Genetic Meta-Analysis of Top GWAS Signals
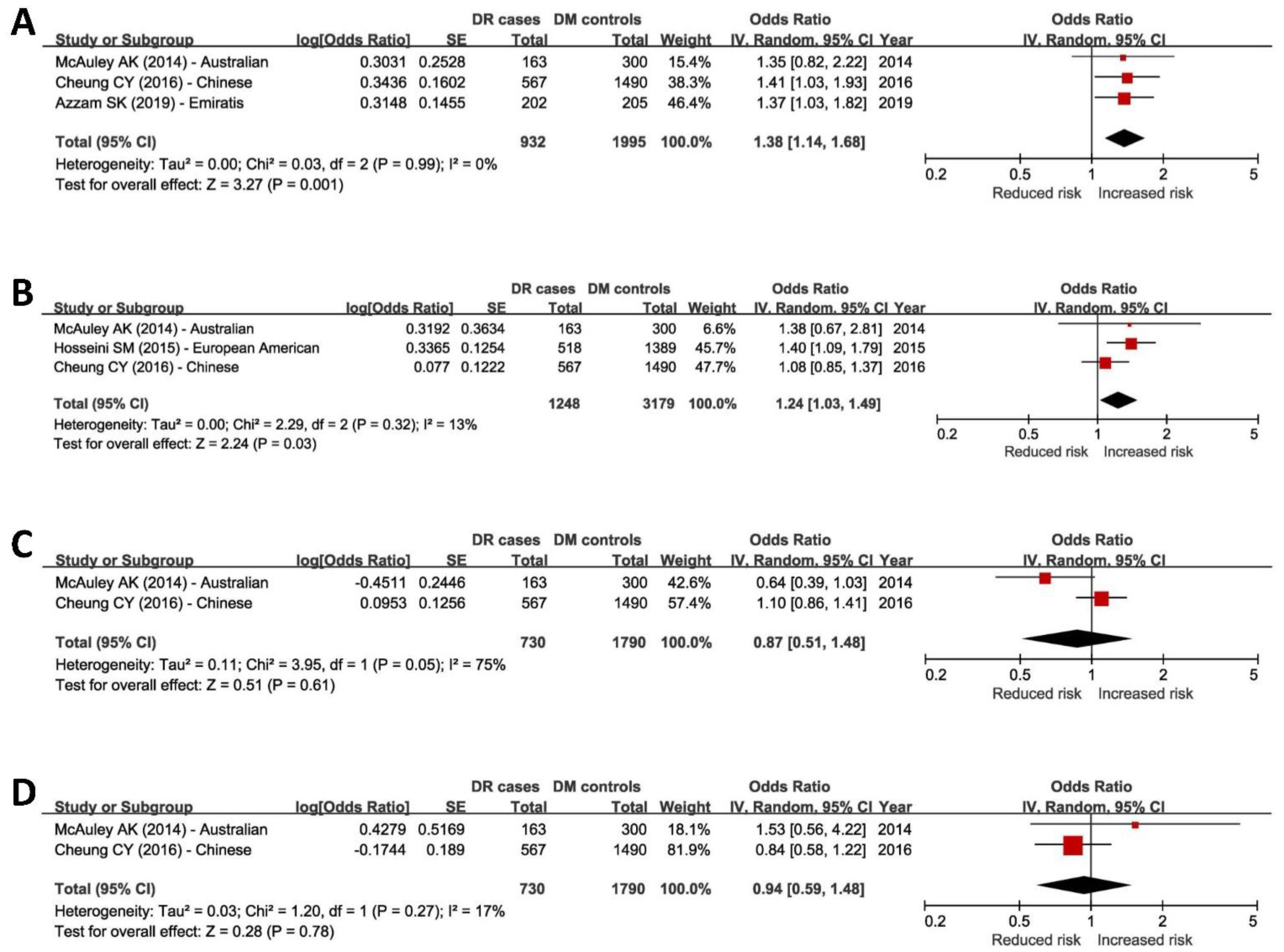
3.3.1. Meta-Analysis of Top DR-Associated SNPs
3.3.2. Meta-Analysis of Top PDR- and DME-Associated SNPs
3.4. Biological Relevance of rs4462262 and rs7903146 to DR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Newcastle—Ottawa Quality Assessment Scale Case Control Studies |
| (Accessed via http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) (accessed on 20 January 2023) Note: A study can be awarded a maximum of one star for each numbered item within the Selection and Exposure categories. A maximum of two stars can be given for Comparability. |
| Selection |
| 1. Is the case definition adequate? |
| a. yes, with independent validation |
| b. yes, e.g., record linkage or based on self reports |
| c. no description |
| 2. Representativeness of the cases |
| a. consecutive or obviously representative series of cases |
| b. potential for selection biases or not stated |
| 3. Selection of Controls |
| a. community controls |
| b. hospital controls |
| c. no description |
| 4. Definition of Controls |
| a. no history of disease (endpoint.) |
| b. no description of source |
| Comparability |
| 1. Comparability of cases and controls on the basis of the design or analysis |
| a. study controls for _______________ (Select the most important factor: ethnicity) |
| b. study controls for any additional factor (This criteria could be modified to indicate specific control for a second important factor.) |
| Exposure |
| 1. Ascertainment of exposure |
| a. secure record (e.g., surgical records) |
| b. structured interview where blind to case/control status |
| c. interview not blinded to case/control status |
| d. written self report or medical record only |
| e. no description |
| 2. Same method of ascertainment for cases and controls |
| a. yes |
| b. no |
| 3. Non-Response rate |
| a. same rate for both groups |
| b. non respondents described |
| c. rate different and no designation |
References
- Yau, J.W.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, I.U.; Flynn, H.W.; Smiddy, W.E.; Ophthalmology, A.A.O. Diabetes and Ocular Disease: Past, Present, and Future Therapies, 2nd ed.; Scott, I.U., Harry, W., Flynn, J., Smiddy, W.E., Eds.; Oxford University Press in cooperation with the American Academy of Ophthalmology: New York, NY, USA, 2010; p. 496. [Google Scholar]
- UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. Bmj 1998, 317, 703–713. [Google Scholar] [CrossRef] [Green Version]
- Diabetes, C.; Complications Trial/Epidemiology of Diabetes, I.; Complications Research, G.; Lachin, J.M.; Genuth, S.; Cleary, P.; Davis, M.D.; Nathan, D.M. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N. Engl. J. Med. 2000, 342, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Group, A.S.; Group, A.E.S.; Chew, E.Y.; Ambrosius, W.T.; Davis, M.D.; Danis, R.P.; Gangaputra, S.; Greven, C.M.; Hubbard, L.; Esser, B.A.; et al. Effects of medical therapies on retinopathy progression in type 2 diabetes. N. Engl. J. Med. 2010, 363, 233–244. [Google Scholar] [CrossRef] [Green Version]
- Keech, A.C.; Mitchell, P.; Summanen, P.A.; O’Day, J.; Davis, T.M.; Moffitt, M.S.; Taskinen, M.R.; Simes, R.J.; Tse, D.; Williamson, E.; et al. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): A randomised controlled trial. Lancet 2007, 370, 1687–1697. [Google Scholar] [CrossRef] [PubMed]
- The Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. Ophthalmology 1981, 88, 583–600. [Google Scholar]
- Hovind, P.; Tarnow, L.; Rossing, K.; Rossing, P.; Eising, S.; Larsen, N.; Binder, C.; Parving, H.H. Decreasing incidence of severe diabetic microangiopathy in type 1 diabetes. Diabetes Care 2003, 26, 1258–1264. [Google Scholar] [CrossRef] [Green Version]
- Rong, S.S.; Tam, P.O.S.; Pang, C.P.; Chen, L.J. Global Review and Meta-analysis of Diabetic Retinopathy Genetic Studies Highlight Gaps in the Pathogenesis between Various Populations. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6197. [Google Scholar]
- Bhatwadekar, A.D.; Shughoury, A.; Belamkar, A.; Ciulla, T.A. Genetics of Diabetic Retinopathy, a Leading Cause of Irreversible Blindness in the Industrialized World. Genes 2021, 12, 1200. [Google Scholar] [CrossRef]
- Cabrera, A.P.; Mankad, R.N.; Marek, L.; Das, R.; Rangasamy, S.; Monickaraj, F.; Das, A. Genotypes and Phenotypes: A Search for Influential Genes in Diabetic Retinopathy. Int. J. Mol. Sci. 2020, 21, 2712. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.P.; Hallman, D.M.; Gonzalez, V.H.; Klein, B.E.; Klein, R.; Hayes, M.G.; Cox, N.J.; Bell, G.I.; Hanis, C.L. Identification of Diabetic Retinopathy Genes through a Genome-Wide Association Study among Mexican-Americans from Starr County, Texas. J. Ophthalmol. 2010, 2010, 861291. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Lin, J.M.; Lin, H.J.; Chen, C.C.; Chen, S.Y.; Tsai, C.H.; Tsai, F.J. Genome-wide association study of diabetic retinopathy in a Taiwanese population. Ophthalmology 2011, 118, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Awata, T.; Yamashita, H.; Kurihara, S.; Morita-Ohkubo, T.; Miyashita, Y.; Katayama, S.; Mori, K.; Yoneya, S.; Kohda, M.; Okazaki, Y.; et al. A genome-wide association study for diabetic retinopathy in a Japanese population: Potential association with a long intergenic non-coding RNA. PLoS ONE 2014, 9, e111715. [Google Scholar] [CrossRef] [Green Version]
- Shtir, C.; Aldahmesh, M.A.; Al-Dahmash, S.; Abboud, E.; Alkuraya, H.; Abouammoh, M.A.; Nowailaty, S.R.; Al-Thubaiti, G.; Naim, E.A.; Alyounes, B.; et al. Exome-based case-control association study using extreme phenotype design reveals novel candidates with protective effect in diabetic retinopathy. Hum. Genet. 2016, 135, 193–200. [Google Scholar] [CrossRef]
- Hsieh, A.R.; Huang, Y.C.; Yang, Y.F.; Lin, H.J.; Lin, J.M.; Chang, Y.W.; Wu, C.M.; Liao, W.L.; Tsai, F.J. Lack of association of genetic variants for diabetic retinopathy in Taiwanese patients with diabetic nephropathy. BMJ Open Diabetes Res. Care 2020, 8, e000727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, M.; Takahashi, A.; Matsunami, M.; Horikoshi, M.; Iwata, M.; Araki, S.I.; Toyoda, M.; Susarla, G.; Ahn, J.; Park, K.H.; et al. Genome-wide association studies identify two novel loci conferring susceptibility to diabetic retinopathy in Japanese patients with type 2 diabetes. Hum. Mol. Genet. 2021, 30, 716–726. [Google Scholar] [CrossRef]
- Backman, J.D.; Li, A.H.; Marcketta, A.; Sun, D.; Mbatchou, J.; Kessler, M.D.; Benner, C.; Liu, D.; Locke, A.E.; Balasubramanian, S.; et al. Exome sequencing and analysis of 454,787 UK Biobank participants. Nature 2021, 599, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Zheng, Z.; Fang, H.; Yang, J. A generalized linear mixed model association tool for biobank-scale data. Nat. Genet. 2021, 53, 1616–1621. [Google Scholar] [CrossRef]
- Xue, Z.; Yuan, J.; Chen, F.; Yao, Y.; Xing, S.; Yu, X.; Li, K.; Wang, C.; Bao, J.; Qu, J.; et al. Genome-wide association meta-analysis of 88,250 individuals highlights pleiotropic mechanisms of five ocular diseases in UK Biobank. EBioMedicine 2022, 82, 104161. [Google Scholar] [CrossRef]
- Grassi, M.A.; Tikhomirov, A.; Ramalingam, S.; Below, J.E.; Cox, N.J.; Nicolae, D.L. Genome-wide meta-analysis for severe diabetic retinopathy. Hum. Mol. Genet. 2011, 20, 2472–2481. [Google Scholar] [CrossRef] [Green Version]
- Sheu, W.H.; Kuo, J.Z.; Lee, I.T.; Hung, Y.J.; Lee, W.J.; Tsai, H.Y.; Wang, J.S.; Goodarzi, M.O.; Klein, R.; Klein, B.E.; et al. Genome-wide association study in a Chinese population with diabetic retinopathy. Hum. Mol. Genet. 2013, 22, 3165–3173. [Google Scholar] [CrossRef] [Green Version]
- Burdon, K.P.; Fogarty, R.D.; Shen, W.; Abhary, S.; Kaidonis, G.; Appukuttan, B.; Hewitt, A.W.; Sharma, S.; Daniell, M.; Essex, R.W.; et al. Genome-wide association study for sight-threatening diabetic retinopathy reveals association with genetic variation near the GRB2 gene. Diabetologia 2015, 58, 2288–2297. [Google Scholar] [CrossRef] [PubMed]
- Graham, P.S.; Kaidonis, G.; Abhary, S.; Gillies, M.C.; Daniell, M.; Essex, R.W.; Chang, J.H.; Lake, S.R.; Pal, B.; Jenkins, A.J.; et al. Genome-wide association studies for diabetic macular edema and proliferative diabetic retinopathy. BMC Med. Genet. 2018, 19, 71. [Google Scholar] [CrossRef] [Green Version]
- Meng, W.; Shah, K.P.; Pollack, S.; Toppila, I.; Hebert, H.L.; McCarthy, M.I.; Groop, L.; Ahlqvist, E.; Lyssenko, V.; Agardh, E.; et al. A genome-wide association study suggests new evidence for an association of the NADPH Oxidase 4 (NOX4) gene with severe diabetic retinopathy in type 2 diabetes. Acta Ophthalmol. 2018, 96, e811–e819. [Google Scholar] [CrossRef] [Green Version]
- Pollack, S.; Igo, R.P., Jr.; Jensen, R.A.; Christiansen, M.; Li, X.; Cheng, C.Y.; Ng, M.C.Y.; Smith, A.V.; Rossin, E.J.; Segrè, A.V.; et al. Multiethnic Genome-Wide Association Study of Diabetic Retinopathy Using Liability Threshold Modeling of Duration of Diabetes and Glycemic Control. Diabetes 2019, 68, 441–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, W.; Chan, B.W.; Ezeonwumelu, C.; Hébert, H.L.; Campbell, A.; Soler, V.; Palmer, C.N. A genome-wide association study implicates that the TTC39C gene is associated with diabetic maculopathy with decreased visual acuity. Ophthalmic Genet. 2019, 40, 252–258. [Google Scholar] [CrossRef]
- Liu, C.; Chen, G.; Bentley, A.R.; Doumatey, A.; Zhou, J.; Adeyemo, A.; Yang, J.; Rotimi, C. Genome-wide association study for proliferative diabetic retinopathy in Africans. NPJ Genom. Med. 2019, 4, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Valle, M.L.; Beveridge, C.; Liu, Y.; Sharma, S. Unraveling the role of genetics in the pathogenesis of diabetic retinopathy. Eye 2019, 33, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Buniello, A.; MacArthur, J.A.L.; Cerezo, M.; Harris, L.W.; Hayhurst, J.; Malangone, C.; McMahon, A.; Morales, J.; Mountjoy, E.; Sollis, E.; et al. The NHGRI-EBI GWAS Catalog of published genome-wide association studies, targeted arrays and summary statistics 2019. Nucleic Acids Res. 2019, 47, D1005–D1012. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Li, Z.; Liu, K.; Rong, S.S.; Brelen, M.E.; Young, A.L.; Kumaramanickavel, G.; Pang, C.P.; Chen, H.; Chen, L.J. Association of Genetic Variants with Polypoidal Choroidal Vasculopathy: A Systematic Review and Updated Meta-analysis. Ophthalmology 2015, 122, 1854–1865. [Google Scholar] [CrossRef]
- Rong, S.S.; Ma, S.T.U.; Yu, X.T.; Ma, L.; Chu, W.K.; Chan, T.C.Y.; Wang, Y.M.; Young, A.L.; Pang, C.P.; Jhanji, V.; et al. Genetic associations for keratoconus: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 4620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rong, S.S.; Tang, F.Y.; Chu, W.K.; Ma, L.; Yam, J.C.; Tang, S.M.; Li, J.; Gu, H.; Young, A.L.; Tham, C.C.; et al. Genetic Associations of Primary Angle-Closure Disease: A Systematic Review and Meta-analysis. Ophthalmology 2016, 123, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.M.; Rong, S.S.; Young, A.L.; Tam, P.O.; Pang, C.P.; Chen, L.J. PAX6 gene associated with high myopia: A meta-analysis. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2014, 91, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.H.; Rong, S.S.; Chong, K.K.; Young, A.L.; Pang, C.P.; Chen, L.J. Genetic Associations of Interleukin-related Genes with Graves’ Ophthalmopathy: A Systematic Review and Meta-analysis. Sci. Rep. 2015, 5, 16672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkwood, B.; Sterne, J. Essentials of Medical Statistics, 2nd ed.; Blackwell Science: Hoboken, NJ, USA, 2003; p. 501. [Google Scholar]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, Alta, 2004; p. 22. [Google Scholar]
- Khan, K.S.; Riet, G.t.; Popay, J.; Nixon, J.; Kleijnen, J. Conducting the review: Phase 5 study quality assessment. In Undertaking Systematic Reviews of Research Effectiveness CDC’s Guidance for Those Carrying Out or Commissioning Reviews; Centre of Reviews and Dissemination: York, UK, 2001; Volume 20. [Google Scholar]
- Squires, J.E.; Estabrooks, C.A.; Gustavsson, P.; Wallin, L. Individual determinants of research utilization by nurses: A systematic review update. Implement. Sci. 2011, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- McPheeters, M.L.; Kripalani, S.; Peterson, N.B.; Idowu, R.T.; Jerome, R.N.; Potter, S.A.; Andrews, J.C. Closing the quality gap: Revisiting the state of the science (vol. 3: Quality improvement interventions to address health disparities). Evid. Rep. Technol. Assess. 2012, 208.3, 1–475. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: www.cochrane-handbook.org (accessed on 20 January 2023).
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Rong, S.S.; Peng, Y.; Liang, Y.B.; Cao, D.; Jhanji, V. Does cigarette smoking alter the risk of pterygium? A systematic review and meta-analysis. Investig. Ophthalmol. Vis. Sci. 2014, 55, 6235–6243. [Google Scholar] [CrossRef] [Green Version]
- Vaser, R.; Adusumalli, S.; Leng, S.N.; Sikic, M.; Ng, P.C. SIFT missense predictions for genomes. Nat. Protoc. 2016, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kircher, M.; Witten, D.M.; Jain, P.; O’Roak, B.J.; Cooper, G.M.; Shendure, J. A general framework for estimating the relative pathogenicity of human genetic variants. Nat. Genet. 2014, 46, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Boyle, A.P.; Hong, E.L.; Hariharan, M.; Cheng, Y.; Schaub, M.A.; Kasowski, M.; Karczewski, K.J.; Park, J.; Hitz, B.C.; Weng, S.; et al. Annotation of functional variation in personal genomes using RegulomeDB. Genome Res. 2012, 22, 1790–1797. [Google Scholar] [CrossRef] [Green Version]
- Genomes Project, C.; Auton, A.; Brooks, L.D.; Durbin, R.M.; Garrison, E.P.; Kang, H.M.; Korbel, J.O.; Marchini, J.L.; McCarthy, S.; McVean, G.A.; et al. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Consortium, G.T. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar] [CrossRef]
- Sobrin, L.; Susarla, G.; Stanwyck, L.; Rouhana, J.M.; Li, A.; Pollack, S.; Igo, R.P., Jr.; Jensen, R.A.; Li, X.; Ng, M.C.Y.; et al. Gene Set Enrichment Analsyes Identify Pathways Involved in Genetic Risk for Diabetic Retinopathy. Am. J. Ophthalmol. 2022, 233, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Sobrin, L.; Chong, Y.H.; Fan, Q.; Gan, A.; Stanwyck, L.K.; Kaidonis, G.; Craig, J.E.; Kim, J.; Liao, W.L.; Huang, Y.C.; et al. Genetically Determined Plasma Lipid Levels and Risk of Diabetic Retinopathy: A Mendelian Randomization Study. Diabetes 2017, 66, 3130–3141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.C.; Chang, Y.W.; Cheng, C.W.; Wu, C.M.; Liao, W.L.; Tsai, F.J. Causal Relationship between Adiponectin and Diabetic Retinopathy: A Mendelian Randomization Study in an Asian Population. Genes 2020, 12, 17. [Google Scholar] [CrossRef]
- Liu, K.; Zou, J.; Fan, H.; Hu, H.; You, Z. Causal effects of gut microbiota on diabetic retinopathy: A Mendelian randomization study. Front. Immunol. 2022, 13, 930318. [Google Scholar] [CrossRef] [PubMed]
- Forrest, I.S.; Chaudhary, K.; Paranjpe, I.; Vy, H.M.T.; Marquez-Luna, C.; Rocheleau, G.; Saha, A.; Chan, L.; Van Vleck, T.; Loos, R.J.F.; et al. Genome-wide polygenic risk score for retinopathy of type 2 diabetes. Hum. Mol. Genet. 2021, 30, 952–960. [Google Scholar] [CrossRef]
- Gurung, R.L.; FitzGerald, L.M.; Liu, E.; McComish, B.J.; Kaidonis, G.; Ridge, B.; Hewitt, A.W.; Vote, B.J.; Verma, N.; Craig, J.E.; et al. Identifying Genetic Biomarkers Predicting Response to Anti-Vascular Endothelial Growth Factor Injections in Diabetic Macular Edema. Int. J. Mol. Sci. 2022, 23, 4042. [Google Scholar] [CrossRef]
- Azzam, S.K.; Osman, W.M.; Lee, S.; Khalaf, K.; Khandoker, A.H.; Almahmeed, W.; Jelinek, H.F.; Al Safar, H.S. Genetic Associations With Diabetic Retinopathy and Coronary Artery Disease in Emirati Patients With Type-2 Diabetes Mellitus. Front. Endocrinol. 2019, 10, 283. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.Y.; Hui, E.Y.; Lee, C.H.; Kwok, K.H.; Gangwani, R.A.; Li, K.K.; Chan, J.C.; Woo, Y.C.; Chow, W.S.; Yuen, M.M.; et al. Impact of Genetic Loci Identified in Genome-Wide Association Studies on Diabetic Retinopathy in Chinese Patients With Type 2 Diabetes. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5518–5524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAuley, A.K.; Wang, J.J.; Dirani, M.; Connell, P.P.; Lamoureux, E.; Hewitt, A.W. Replication of genetic loci implicated in diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1666–1671. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, S.M.; Boright, A.P.; Sun, L.; Canty, A.J.; Bull, S.B.; Klein, B.E.; Klein, R.; Paterson, A.D. The association of previously reported polymorphisms for microvascular complications in a meta-analysis of diabetic retinopathy. Hum. Genet. 2015, 134, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciccacci, C.; Di Fusco, D.; Cacciotti, L.; Morganti, R.; D’Amato, C.; Novelli, G.; Sangiuolo, F.; Spallone, V.; Borgiani, P. TCF7L2 gene polymorphisms and type 2 diabetes: Association with diabetic retinopathy and cardiovascular autonomic neuropathy. Acta Diabetol. 2013, 50, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Zhao, L.; Chen, A.Y.; Zhang, X.; Zhu, J.; Zhao, J.; Ouyang, H.; Luo, H.; Song, Y.; Lee, J.; et al. TCF7L2 variation and proliferative diabetic retinopathy. Diabetes 2013, 62, 2613–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magazova, A.; Ashirbekov, Y.; Abaildayev, A.; Satken, K.; Balmukhanova, A.; Akanov, Z.; Jainakbayev, N.; Balmukhanova, A.; Sharipov, K. ITGA2 Gene Polymorphism Is Associated with Type 2 Diabetes Mellitus in the Kazakhstan Population. Medicina 2022, 58, 1416. [Google Scholar] [CrossRef]
- Shawki, H.A.M.; Abo-Hashem, E.; Youssef, M.M.; Shahin, M.; Elzehery, R. Association of transcription factor 7-like 2 (rs7903146) gene polymorphism with diabetic retinopathy. Ophthalmic Genet. 2020, 41, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Buraczynska, M.; Swatowski, A.; Markowska-Gosik, D.; Kuczmaszewska, A.; Ksiazek, A. Transcription factor 7-like 2 (TCF7L2) gene polymorphism and complication/comorbidity profile in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2011, 93, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Peterson, R.E.; Kuchenbaecker, K.; Walters, R.K.; Chen, C.Y.; Popejoy, A.B.; Periyasamy, S.; Lam, M.; Iyegbe, C.; Strawbridge, R.J.; Brick, L.; et al. Genome-wide Association Studies in Ancestrally Diverse Populations: Opportunities, Methods, Pitfalls, and Recommendations. Cell 2019, 179, 589–603. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Goldberg, M.F. ETDRS Grading of Diabetic Retinopathy: Still the Gold Standard? Ophthalmic Res. 2019, 62, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—An extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology 1991, 98, 786–806. [Google Scholar] [CrossRef]
- Kowluru, R.A. Cross Talks between Oxidative Stress, Inflammation and Epigenetics in Diabetic Retinopathy. Cells 2023, 12, 300. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Kaur, V.; Chamarthi, B.; Littleton, K.R.; Chen, L.; Manning, A.K.; Merino, J.; Thomas, M.K.; Hudson, M.; Goldfine, A.; et al. TCF7L2 Genetic Variation Augments Incretin Resistance and Influences Response to a Sulfonylurea and Metformin: The Study to Understand the Genetics of the Acute Response to Metformin and Glipizide in Humans (SUGAR-MGH). Diabetes Care 2018, 41, 554–561. [Google Scholar] [CrossRef] [Green Version]
- The Action to Control Cardiovascular Risk in Diabetes Follow-On (ACCORDION) Eye Study Group; the Action to Control Cardiovascular Risk in Diabetes Follow-On (ACCORDION) Study Group. Persistent Effects of Intensive Glycemic Control on Retinopathy in Type 2 Diabetes in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Follow-On Study. Diabetes Care 2016, 39, 1089–1100. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhao, J.; Zhao, T.; Liu, H. Effects of intensive glycemic control in ocular complications in patients with type 2 diabetes: A meta-analysis of randomized clinical trials. Endocrine 2015, 49, 78–89. [Google Scholar] [CrossRef]
- Del Bosque-Plata, L.; Hernandez-Cortes, E.P.; Gragnoli, C. The broad pathogenetic role of TCF7L2 in human diseases beyond type 2 diabetes. J. Cell. Physiol. 2022, 237, 301–312. [Google Scholar] [CrossRef]
- Del Bosque-Plata, L.; Martinez-Martinez, E.; Espinoza-Camacho, M.A.; Gragnoli, C. The Role of TCF7L2 in Type 2 Diabetes. Diabetes 2021, 70, 1220–1228. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Year | Studied Trait | Background Disease | Discovery Population | Replication Population | Discovery Sample Size (N) | Significant SNP | Reference | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Total | |||||||||
| 1 | Fu, Y.P. | 2010 | DR | T2D | Hispanic | None | 103 | 183 | 286 | 0 | [12] |
| 2 | Huang, Y.C. | 2011 | DR | T2D | Chinese | None | 174 | 575 | 749 * | 8 | [13] |
| 3 | Grassi, M.A. | 2011 | DR (DME + PDR) | T1D | European | None | 973 | 1856 | 2829 | 19 | [21] |
| 4 | Sheu, W.H. | 2013 | PDR | T2D | Chinese | Hispanic or Latin American | 437 | 570 | 1007 | 1 ** | [22] |
| 5 | Awata, T. | 2014 | DR | T2D | Japanese | Asian | 205 | 241 | 446 | 1 | [14] |
| 6 | Burdon, K.P. | 2015 | DR (severe NPDR + PDR + DME) | T2D | Australians (European) | European, Indian | 336 | 508 | 844 | 1 | [23] |
| 7 | Shtir, C. | 2016 | DR | DM | Saudi Arabian | None | 43 | 64 | 107 | 3 | [15] |
| 8 | Graham, P.S. | 2018 | DME and PDR | T2D | Australians (European) | None | 270 and 176 | 435 | 881 | 2 and 2 | [24] |
| 9 | Meng, W. | 2018 | Severe DR | T2D | Scottish (European) | Independent meta-analysis | 560 | 4106 | 4666 | 2 | [25] |
| 10 | Pollack, S. | 2018 | DR and PDR | T2D | African American, Afro-Caribbean, European | Asian, European, Hispanic | MDP | MDP | 5857 | 19 and 20 | [26] |
| 11 | Meng, W. | 2019 | Diabetic maculopathy | T2D | European | None | 469 | 1374 | 1843 | 8 | [27] |
| 12 | Liu, C. | 2019 | PDR | T2D | African | African American or Afro-Caribbean | 64 | 227 | 291 | 4 | [28] |
| 13 | Hsieh, A.R. | 2020 | DR | T2D | Chinese | None | 206 | 206 | 412 | 3 | [16] |
| 14 | Imamura, M. | 2021 | DR | T2D | Japanese | Japanese | 4839 | 4041 | 8880 | 6 | [17] |
| SNP | Position | Location | Gene | SIFT | PolyPhen | CADD | RegulomeDB * | eQTL (p) | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | rs4462262 | Chr10:59189178 | Intergenic | None | na | na | 7.10 | 5 | na |
| 2 | rs7903146 ** | Chr10:114758349 | Intronic | TCF7L2 | na | na | 3.27 | 5 | 2.9 × 10−7 |
| 3 | rs7074440 | Chr10:114785424 | Intronic | TCF7L2 | na | na | 10.10 | 2b | 2.1 × 10−6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, X.; Rong, S. Genome-Wide Associations and Confirmatory Meta-Analyses in Diabetic Retinopathy. Genes 2023, 14, 653. https://doi.org/10.3390/genes14030653
Yu X, Rong S. Genome-Wide Associations and Confirmatory Meta-Analyses in Diabetic Retinopathy. Genes. 2023; 14(3):653. https://doi.org/10.3390/genes14030653
Chicago/Turabian StyleYu, Xinting, and Shisong Rong. 2023. "Genome-Wide Associations and Confirmatory Meta-Analyses in Diabetic Retinopathy" Genes 14, no. 3: 653. https://doi.org/10.3390/genes14030653