
Gathering the Stakeholder’s Perspective: Experiences and Opportunities in Rare Genetic Disease Research
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
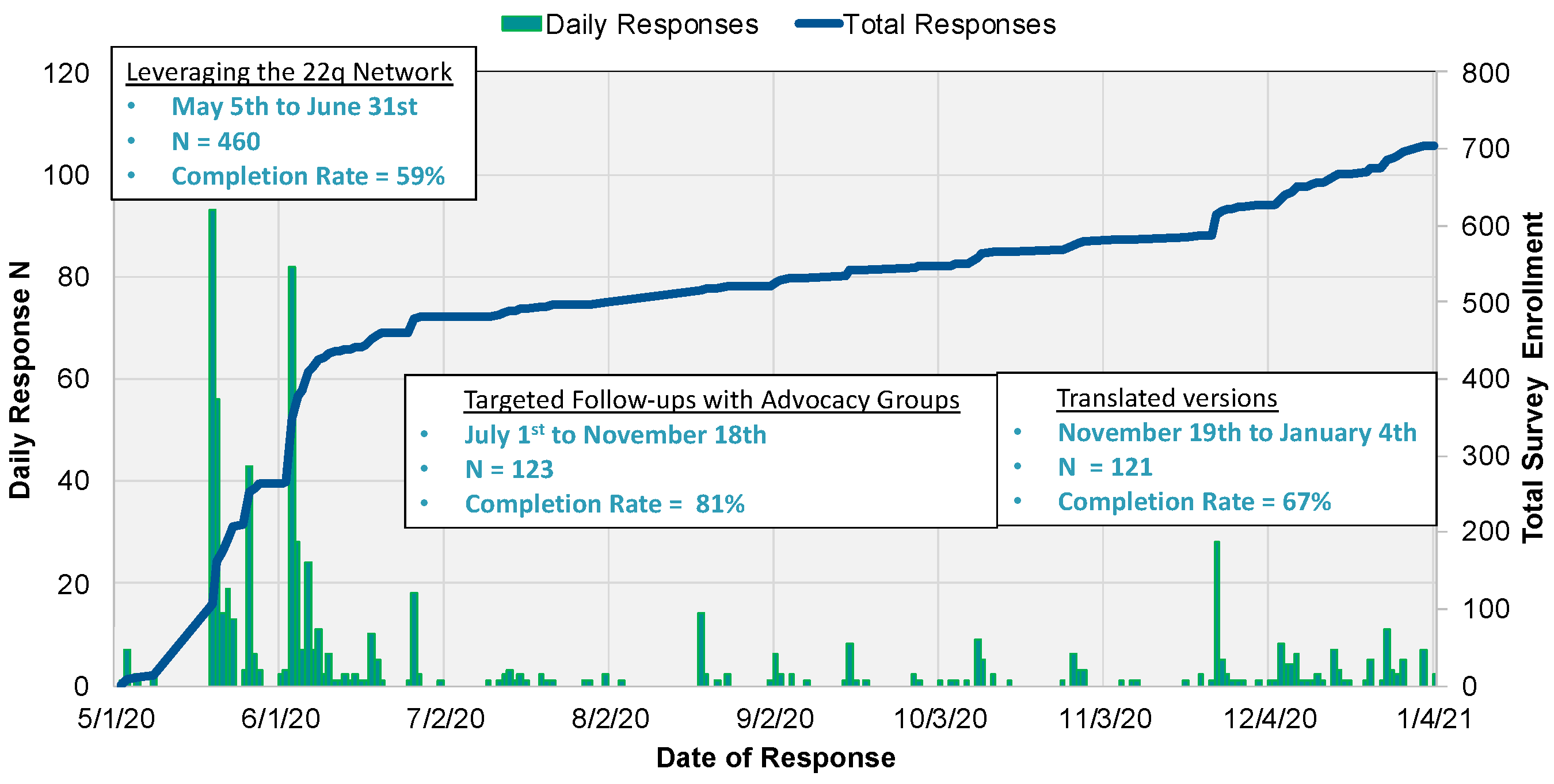
2.1. Procedures
2.2. Participants
2.3. Research Participation Survey
2.4. Data Analysis
3. Results
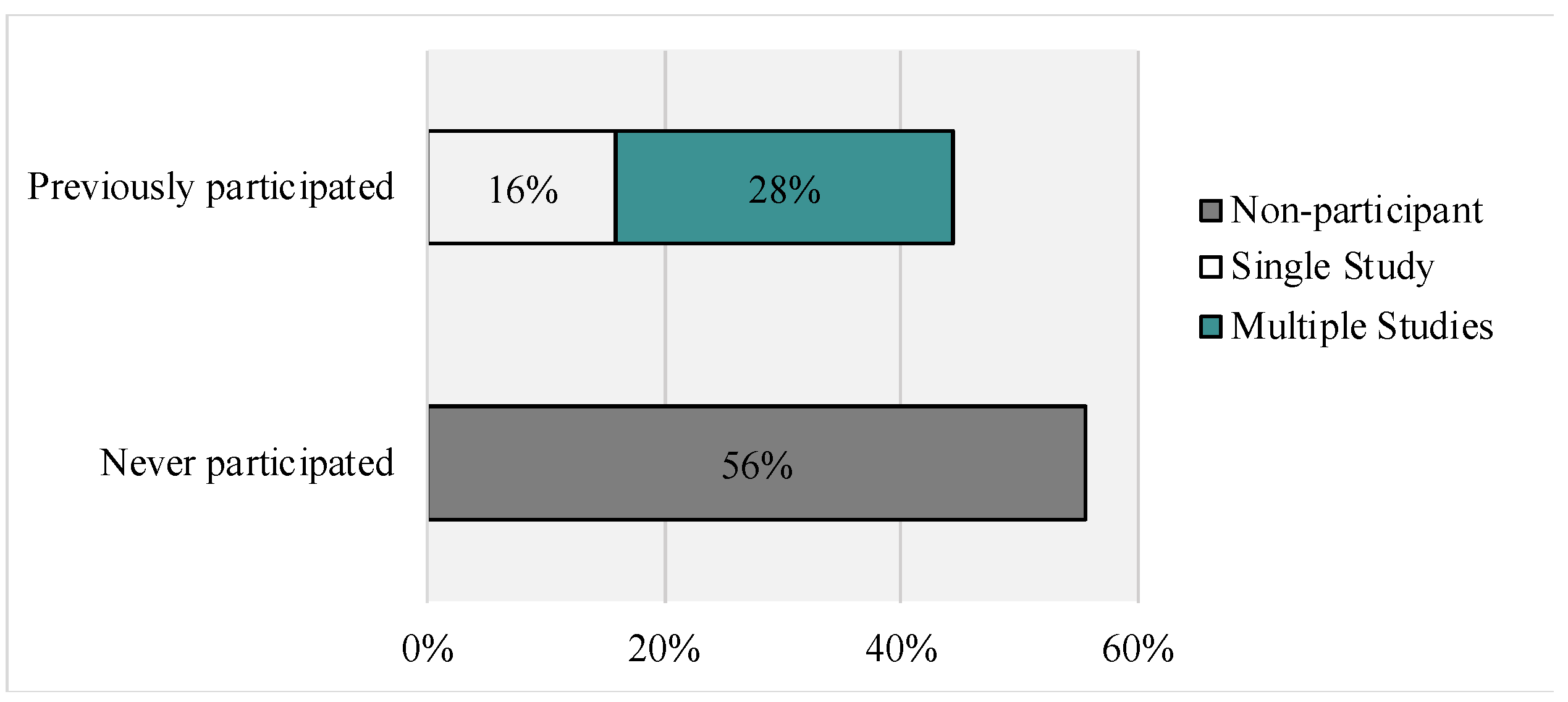
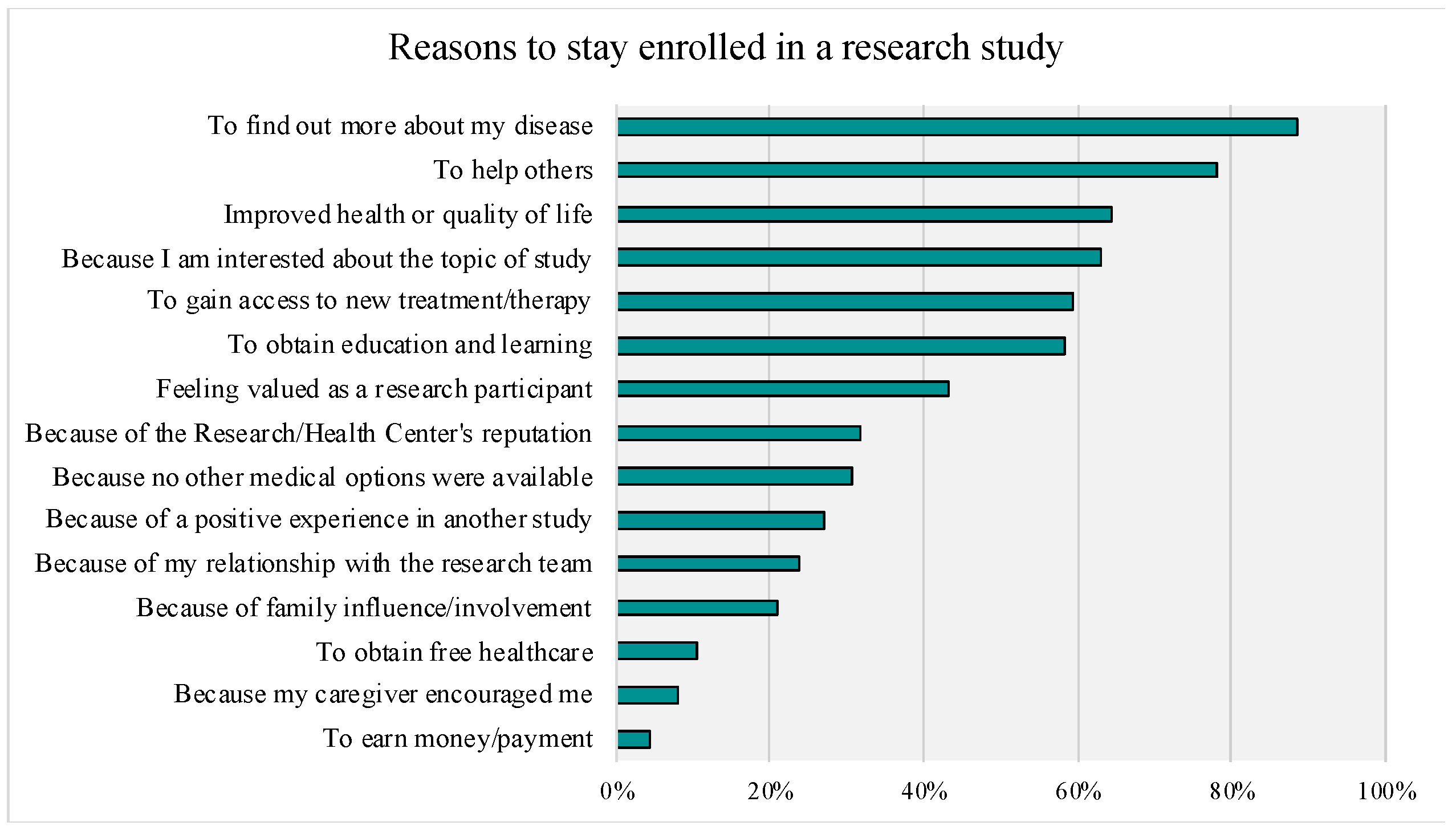
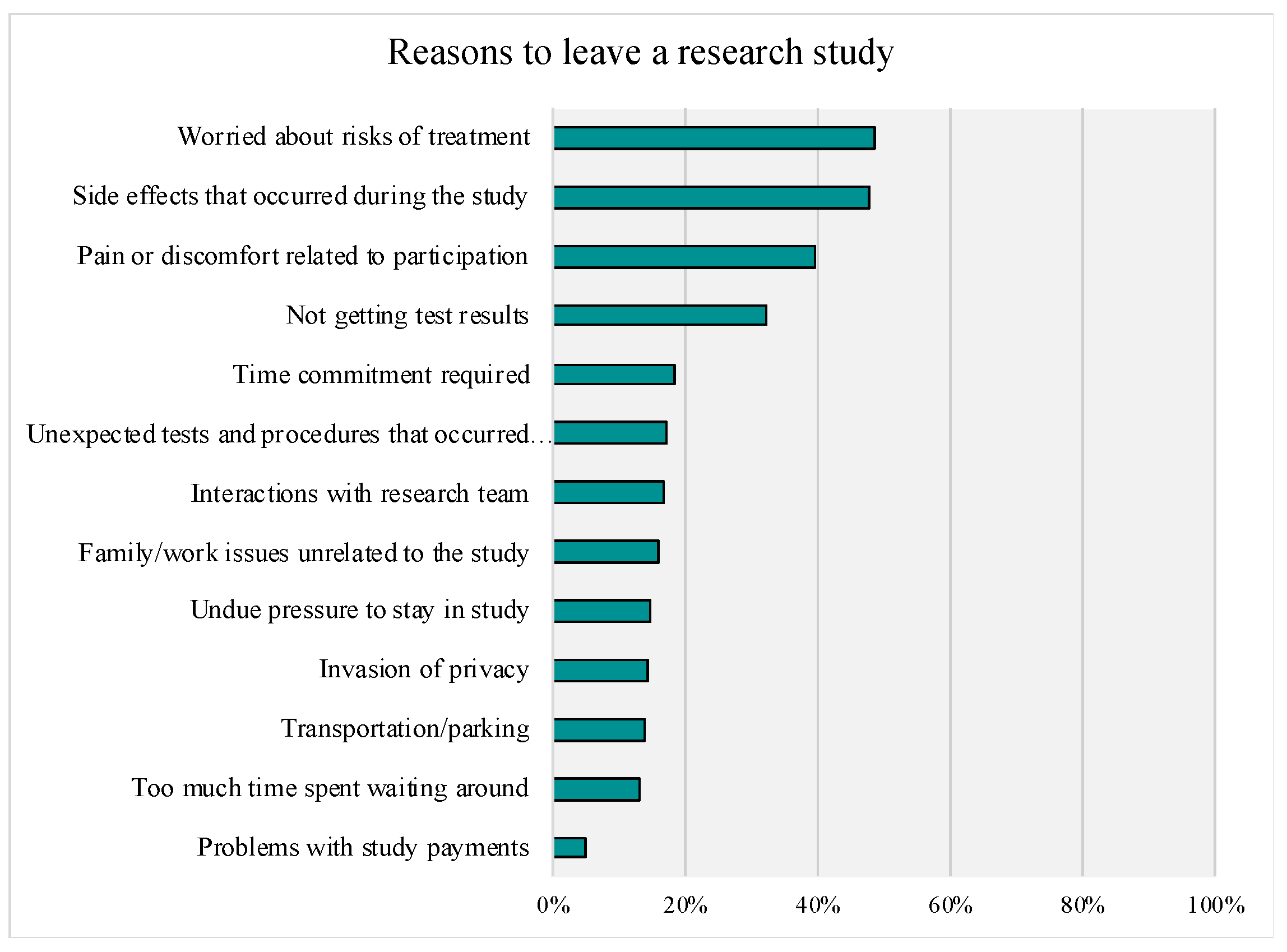
3.1. Research Study Enrollment, Retainment, Withdrawal, and Future Participation
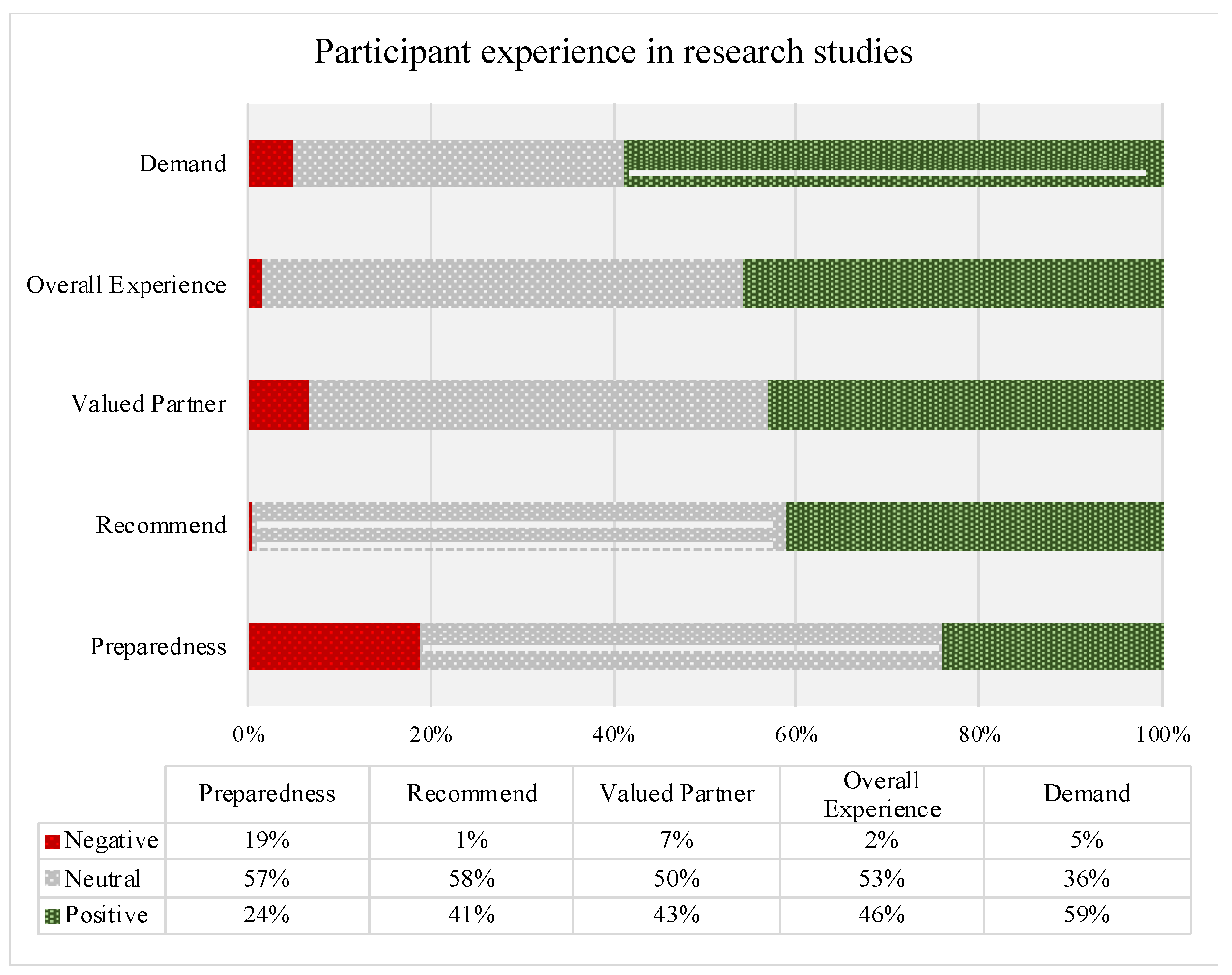
3.2. Overall Research Experience, Burden, and Preparedness
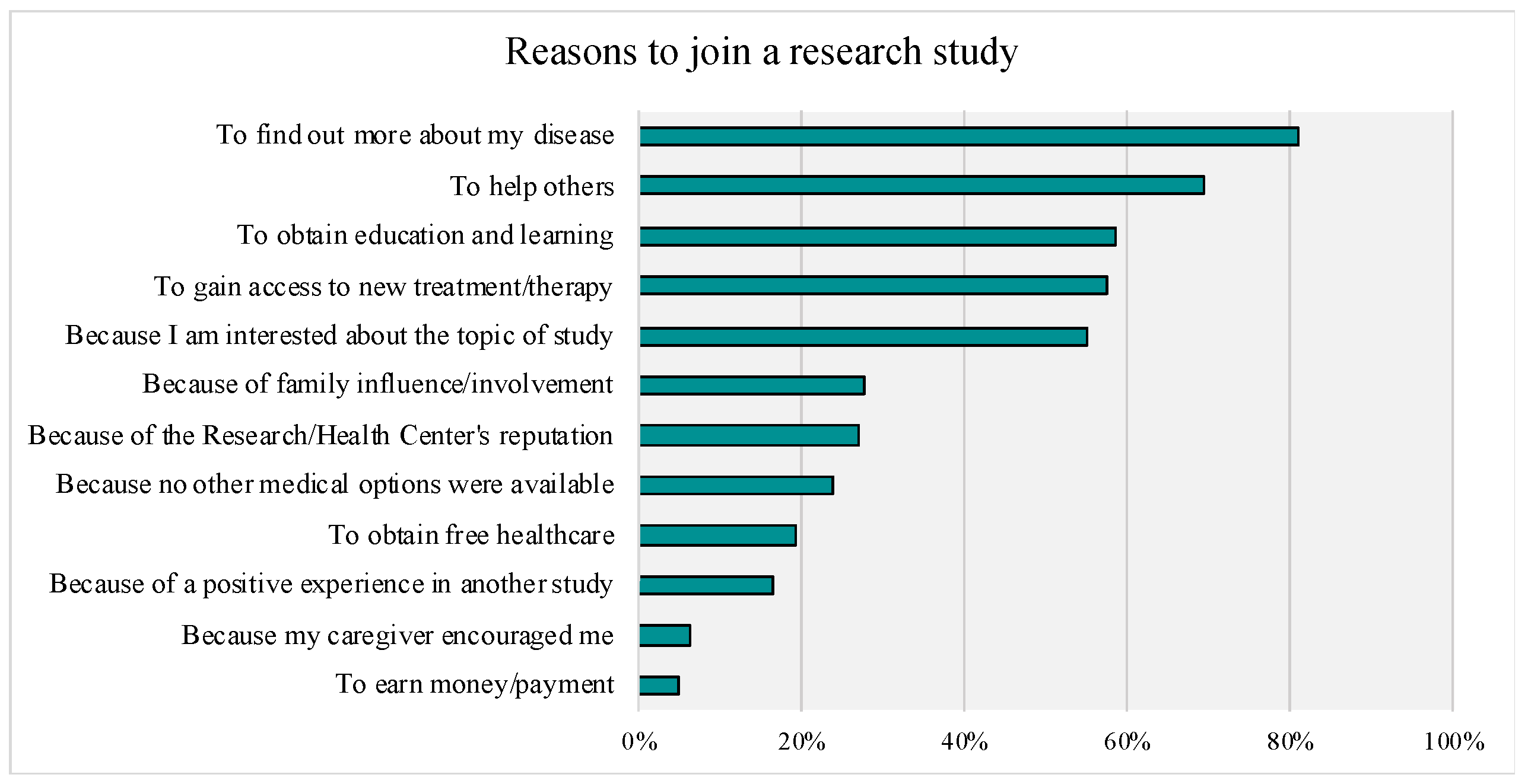
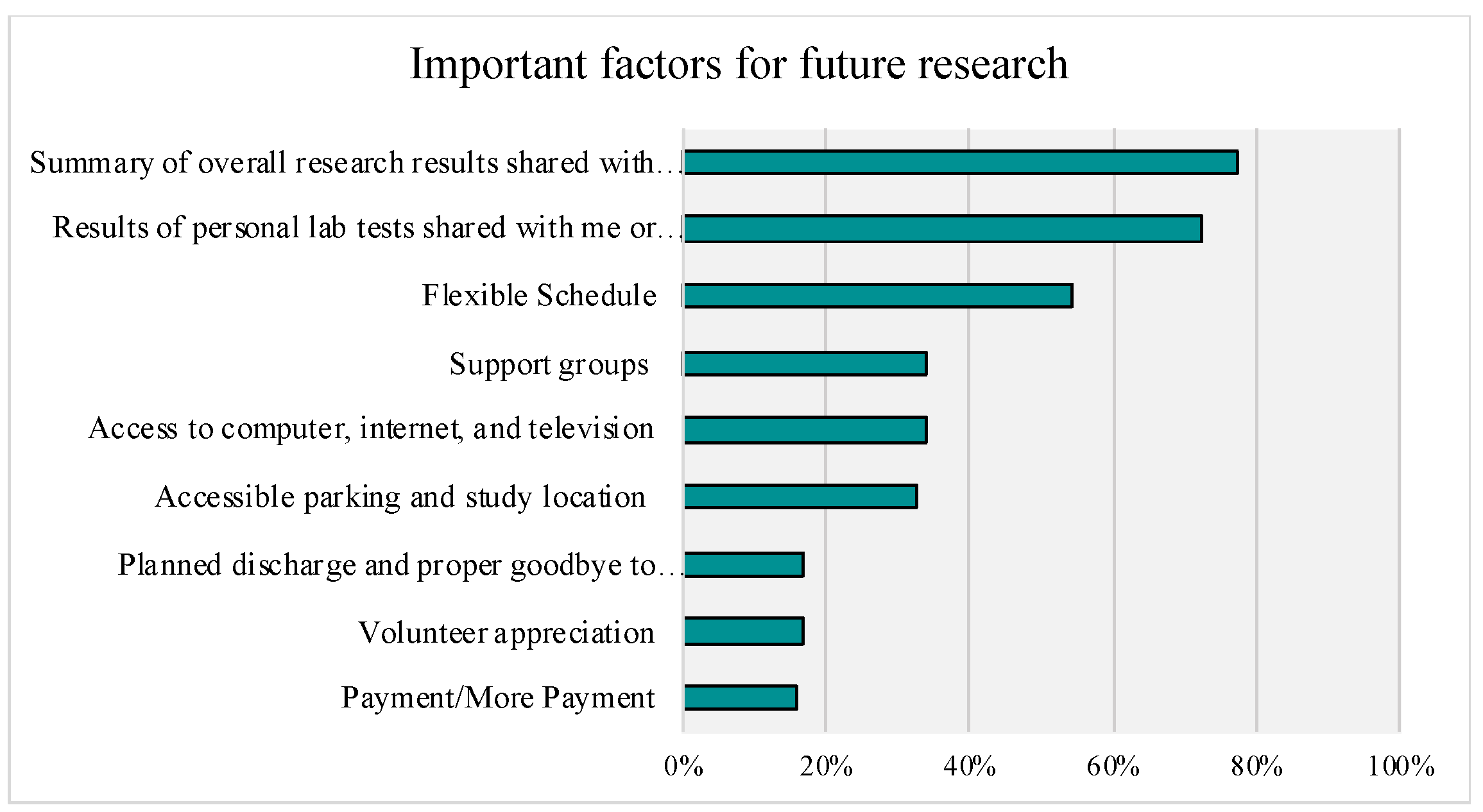
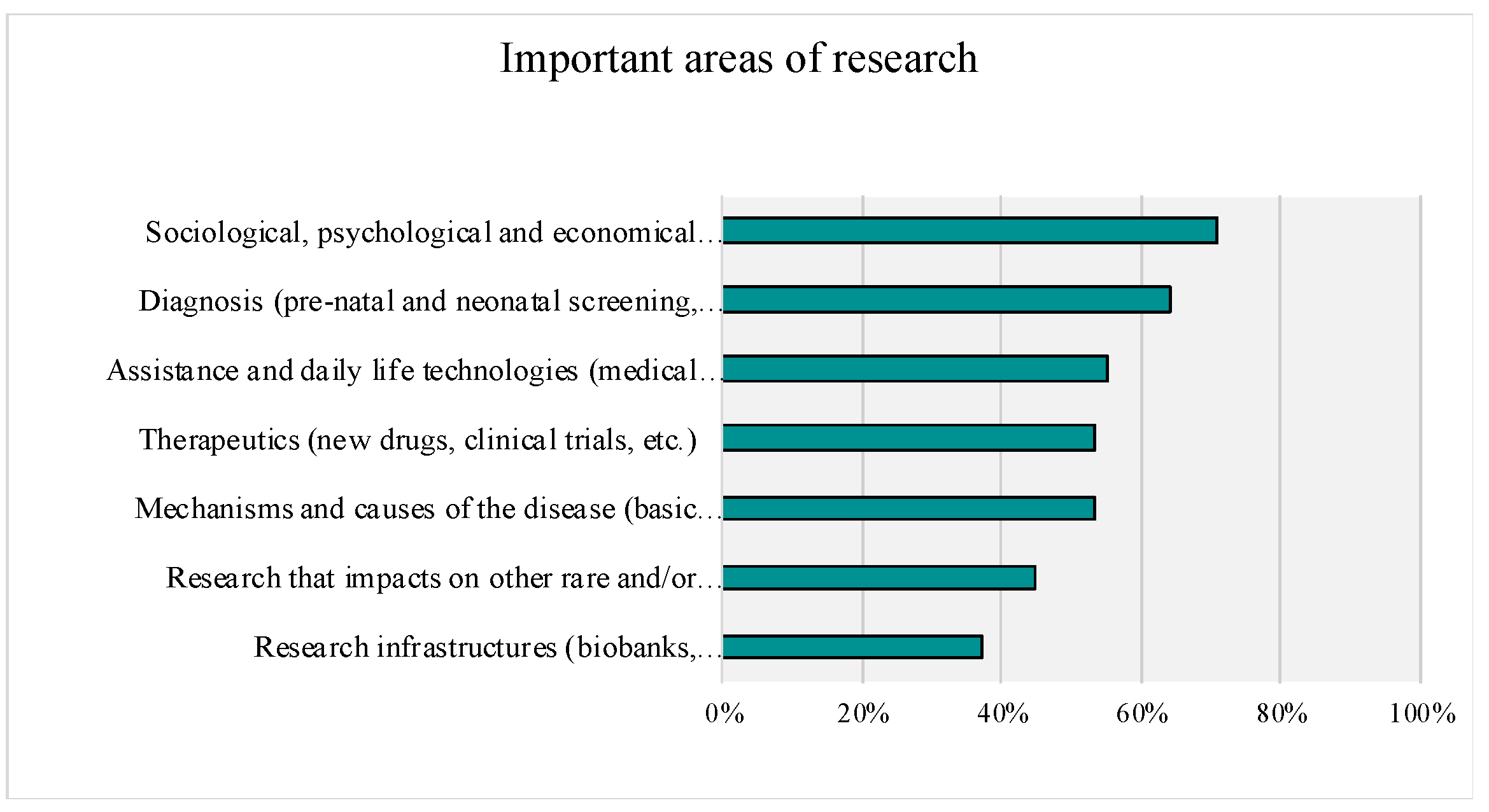
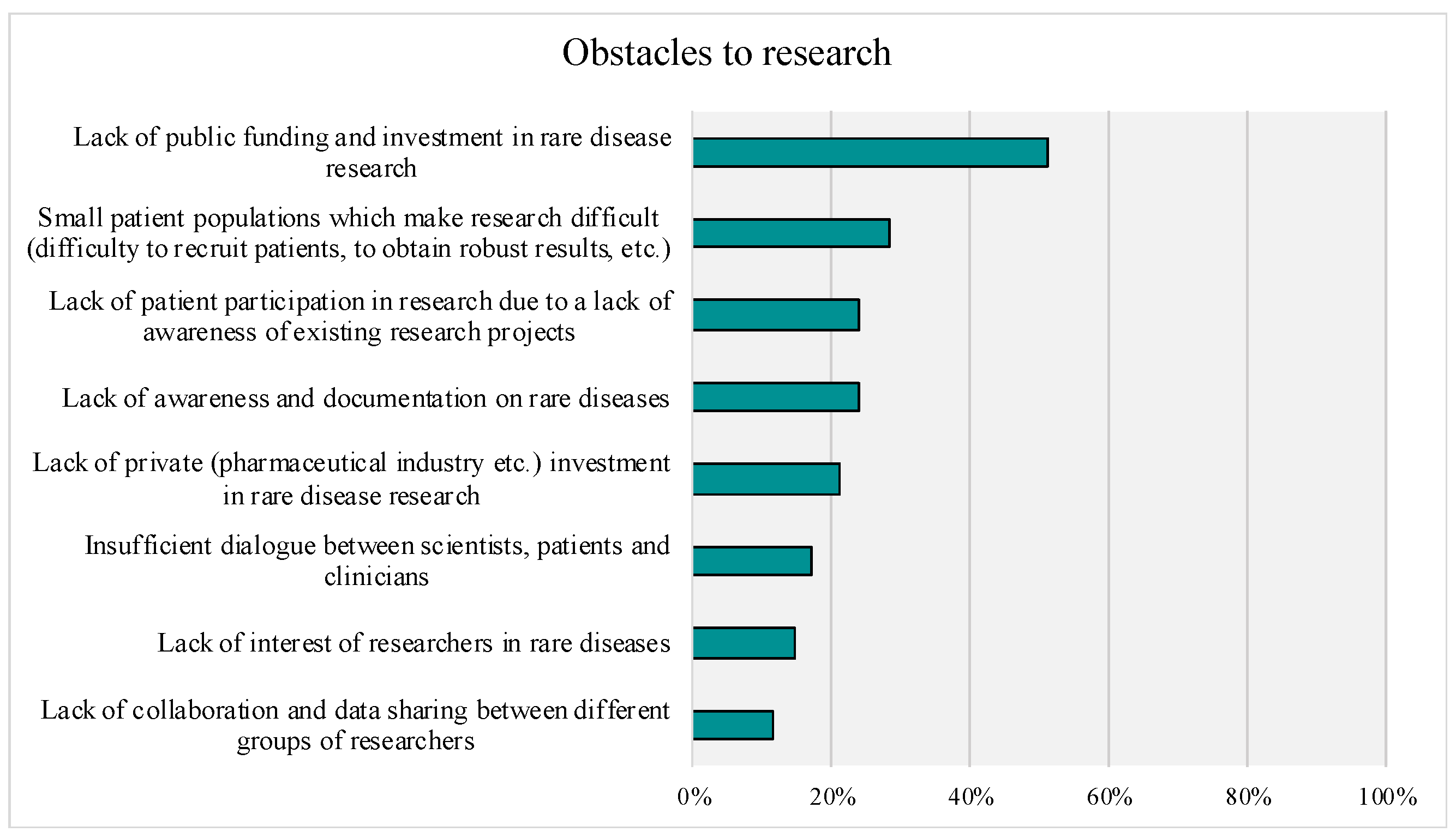
3.3. Research Priorities and Obstacles
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smailes, P.; Reider, C.; Hallarn, R.K.; Hafer, L.; Wallace, L.; Miser, W.F. Implementation of a Research Participant Satisfaction Survey at an Academic Medical Center. Clin. Res. Alex. Va 2016, 30, 42–47. [Google Scholar]
- Adler, P.; Otado, J.; Kwagyan, J. Satisfaction and perceptions of research participants in clinical and translational studies: An urban multi-institution with CTSA. J. Clin. Transl. Sci. 2020, 4, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verheggen, F.W.; Nieman, F.H.; Reerink, E.; Kok, G.J. Patient satisfaction with clinical trial participation. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 1998, 10, 319–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaac, T.; Zaslavsky, A.M.; Cleary, P.D.; Landon, B.E. The Relationship between Patients’ Perception of Care and Measures of Hospital Quality and Safety. Health Serv. Res. 2010, 45, 1024–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kost, R.G.; Lee, L.M.; Yessis, J.; Coller, B.S.; Henderson, D.K.; Research Participant Perception Survey Focus Group Subcommittee. Assessing research participants’ perceptions of their clinical research experiences. Clin. Transl. Sci. 2011, 4, 403–413. [Google Scholar] [CrossRef]
- Pflugeisen, B.M.; Rebar, S.; Reedy, A.; Pierce, R.; Amoroso, P.J. Assessment of clinical trial participant patient satisfaction: A call to action. Trials 2016, 17, 483. [Google Scholar] [CrossRef] [Green Version]
- Kirov, G. CNVs in neuropsychiatric disorders. Hum. Mol. Genet. 2015, 24, R45–R49. [Google Scholar] [CrossRef]
- Malhotra, D.; Sebat, J. CNVs: Harbingers of a Rare Variant Revolution in Psychiatric Genetics. Cell 2012, 148, 1223–1241. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.L.; Wain, K.E.; Oetjens, M.T.; Tolwinski, K.; Palen, E.; Hare-Harris, A.; Habegger, L.; Maxwell, E.K.; Reid, J.G.; Walsh, L.K.; et al. Identification of Neuropsychiatric Copy Number Variants in a Health Care System Population. JAMA Psychiatry 2020, 77, 1276–1285. [Google Scholar] [CrossRef]
- McDonald-McGinn, D.M.; Sullivan, K.E.; Marino, B.; Philip, N.; Swillen, A.; Vorstman, J.A.S.; Zackai, E.H.; Emanuel, B.S.; Vermeesch, J.R.; Morrow, B.E.; et al. 22q11.2 deletion syndrome. Nat. Rev. Dis. Primer 2015, 1, 15071. [Google Scholar] [CrossRef] [Green Version]
- Merikangas, A.K.; Corvin, A.P.; Gallagher, L. Copy-number variants in neurodevelopmental disorders: Promises and challenges. Trends Genet. 2009, 25, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Yessis, J.L.; Kost, R.G.; Lee, L.M.; Coller, B.S.; Henderson, D.K. Development of a Research Participants’ Perception Survey to Improve Clinical Research. Clin. Transl. Sci. 2012, 5, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Blagojevic, C.; Heung, T.; Theriault, M.; Tomita-Mitchell, A.; Chakraborty, P.; Kernohan, K.; Bulman, D.E.; Bassett, A.S. Estimate of the contemporary live-birth prevalence of recurrent 22q11.2 deletions: A cross-sectional analysis from population-based newborn screening. CMAJ Open 2021, 9, E802–E809. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, R.; Mahjani, B.; Loos, R.J.F.; Sharp, A.J. Clinical Characterization of Copy Number Variants Associated With Neurodevelopmental Disorders in a Large-scale Multiancestry Biobank. JAMA Psychiatry 2022, 79, 250–259. [Google Scholar] [CrossRef] [PubMed]
- McDonald-Mcginn, D.M.; Sullivan, K.E. Chromosome 22q11.2 deletion syndrome (DiGeorge syndrome/velocardiofacial syndrome). Medicine 2011, 90, 1–18. [Google Scholar] [CrossRef]
- Rees, E.; Kirov, G. Copy number variation and neuropsychiatric illness. Curr. Opin. Genet. Dev. 2021, 68, 57–63. [Google Scholar] [CrossRef]
- EURORDIS 2021 Results Report. 2021. Available online: https://download2.eurordis.org/rbv/HCARE/HCARE_FS_long.pdf (accessed on 28 May 2021).
- Kost, R.G.; Lee, L.M.; Yessis, J.; Wesley, R.A.; Henderson, D.K.; Coller, B.S. Assessing Participant-Centered Outcomes to Improve Clinical Research. N. Engl. J. Med. 2013, 369, 2179–2181. [Google Scholar] [CrossRef] [Green Version]
- Kost, R.G.; Lee, L.N.; Yessis, J.L.; Wesley, R.; Alfano, S.; Alexander, S.R.; Kassis, S.B.; Cola, P.; Dozier, A.; Ford, D.E.; et al. Research Participant-Centered Outcomes at NIH-Supported Clinical Research Centers. Clin. Transl. Sci. 2014, 7, 430–440. [Google Scholar] [CrossRef]
- Geppert, C.; Candilis, P.; Baker, S.; Lidz, C.; Appelbaum, P.; Fletcher, K. Motivations of Patients with Diabetes to Participate in Research. AJOB Empir. Bioeth. 2014, 5, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Mattson, M.E.; Curb, J.D.; McArdle, R. Participation in a clinical trial: The patients’ point of view. Control. Clin. Trials 1985, 6, 156–167. [Google Scholar] [CrossRef]
- Udrea, G.; Dumitrescu, B.; Purcarea, M.; Balan, I.; Rezus, E.; Deculescu, D. Patients’ perspectives and motivators to participate in clinical trials with novel therapies for rheumatoid arthritis. J. Med. Life 2009, 2, 227–231. [Google Scholar] [PubMed]
- Mezinska, S.; Gallagher, L.; Verbrugge, M.; Bunnik, E.M. Ethical issues in genomics research on neurodevelopmental disorders: A critical interpretive review. Hum. Genom. 2021, 15, 16. [Google Scholar] [CrossRef] [PubMed]
- Harmsen, S.; Pittens, C.A.C.M.; Vroonland, E.; van Rensen, A.J.M.L.; Broerse, J.E.W. Supporting health researchers to realize meaningful patient involvement in research: Exploring researchers’ experiences and needs. Sci. Public Policy 2022, 49, 751–764. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Status and Relationship | Percentage of Respondents Reporting | Mean Age in Years (SD) | |||||
|---|---|---|---|---|---|---|---|
| N | Female | United States | Urban or Suburban | Previous Participation | Respondent | Child | |
| Unaffected | |||||||
| Parent | 575 | 85% | 59% | 79% | 43% | 44 (10) | 13 (9) |
| Other Family Member | 37 | 94% | 73% | 88% | 10% | 49 (17) | - |
| Affected | |||||||
| Parent | 33 | 82% | 42% | 61% | 47% | 43 (11) | 11 (9) |
| Individual | 27 | 68% | 40% | 86% | 45% | 33 (14) | - |
| Declined to answer | |||||||
| 32 | 100% | 33% | 63% | 44% | 36 (14) | - | |
| Total | |||||||
| 704 | 85% | 51% | 78% | 41% | 44 (11) | 13 (9) | |
| Specific CNV Type | N | % |
|---|---|---|
| 22q11.2 deletion | 470 | 66.8 |
| 22q11.2 duplication | 72 | 10.2 |
| 16p11.2 deletion | 31 | 4.4 |
| 16p11.2 duplication | 11 | 1.6 |
| 15q11.2 duplication | 6 | 0.9 |
| 15q11.2 deletion | 2 | 0.3 |
| 1q21.1 duplication | 5 | 0.7 |
| 1q21.1 deletion | 3 | 0.4 |
| 2p16.3 deletion | 3 | .04 |
| 2p16.3 duplication | 1 | 0.1 |
| 17p11.2 deletion | 2 | 0.3 |
| 17p11.2 duplication | 1 | 0.1 |
| 15q13.3 duplication | 3 | 0.4 |
| 7q11.23 deletion | 3 | 0.4 |
| Other | 41 | 5.8 |
| Declined to answer | 50 | 7.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
White, L.K.; Crowley, T.B.; Finucane, B.; McClellan, E.J.; Donoghue, S.; Garcia-Minaur, S.; Repetto, G.M.; Fischer, M.; Jacquemont, S.; Gur, R.E.; et al. Gathering the Stakeholder’s Perspective: Experiences and Opportunities in Rare Genetic Disease Research. Genes 2023, 14, 169. https://doi.org/10.3390/genes14010169
White LK, Crowley TB, Finucane B, McClellan EJ, Donoghue S, Garcia-Minaur S, Repetto GM, Fischer M, Jacquemont S, Gur RE, et al. Gathering the Stakeholder’s Perspective: Experiences and Opportunities in Rare Genetic Disease Research. Genes. 2023; 14(1):169. https://doi.org/10.3390/genes14010169
Chicago/Turabian StyleWhite, Lauren K., T. Blaine Crowley, Brenda Finucane, Emily J. McClellan, Sarah Donoghue, Sixto Garcia-Minaur, Gabriela M. Repetto, Matthias Fischer, Sebastien Jacquemont, Raquel E. Gur, and et al. 2023. "Gathering the Stakeholder’s Perspective: Experiences and Opportunities in Rare Genetic Disease Research" Genes 14, no. 1: 169. https://doi.org/10.3390/genes14010169