1. Introduction
Obesity is a global health problem [
1]. Studies in various populations have shown the importance of the genetic component in obesity. Studies in twins have revealed that 80% of variations in the body mass index (BMI) are related to a genetic component [
2]; other studies have reported that adopted children have more BMI alterations compared to those shown by their biological parents, indicating that 63% of these alterations resulted from a hereditary component and 31% from environmental factors. Furthermore, studies based on single nucleotide polymorphisms (SNP) have only been able to attribute 3% of BMI variation to a genetic effect [
3,
4]. Available data suggest a susceptibility of some populations to have higher figures of obesity, as in the case of the Latin American population, where obesity statistics have increased alarmingly and Mexico is considered the country with the highest rate of obesity. Both adult and child populations [
5,
6] are susceptible to being diagnosed as obese in the same proportion. Several independent studies have shown an association between
FTO SNPs and fat mass and obesity [
7,
8,
9].
FTO has been studied for several years and is known to encode for an enzyme nucleic acid methylase, dependent on α-ketoglutarate and iron (Fe II), which is ubiquitous in human tissues. Understanding the exact mechanism by which it is associated with obesity has been difficult [
10,
11]. However, a loss of function in homozygous
FTO carriers has been observed to cause growth retardation and central nervous system disorders. Likewise, there are thin and obese heterozygous individuals, which indicates that the loss or gain of the
FTO function is not a condition for the development of obesity but rather specific modifications in their activity. Such modifications can be due to subtle changes in the gene sequence, such as SNPs [
11].
In a study investigating adipocytes derived from human adipose tissue, the researchers observed that the presence of the risk allele of SNP rs1421085 promoted a greater darkening of fat cells [
12]. On the other hand, in studies looking directly at humans, the association of various SNPs has been observed in different populations in recent decades. Such is the case for SNPs rs9939609, rs6499640, rs8050136, and rs1558902 in the Chinese population [
13]. A positive association was also observed with high BMI in the Korean population for SNPs rs1421085 and rs17817449 [
13]. Furthermore, rs1421085, rs17817449, and rs9939609 have been associated with obesity in European populations, while these relationships differed in Melanesian, Micronesian, and Polynesian populations [
14].
In the Mexican population, some associations of
FTO SNPs with obesity of the SNPs rs1121980, rs17817449, rs3751812, and rs9930506 have been observed in the mestizo population [
7], and rs9939609 and rs1421085 were associated with obesity in the Mayan population [
15].
As these previous studies have not been able to analyze a greater number of genetic variants associated with phenotypic obesity markers, the present work focuses on the evaluation of 175 FTO SNPs filtered from a microarray to investigate their potential associations with common indicators of obesity phenotypes.
2. Materials and Methods
2.1. Subjects and Genetic Sampling
A total of 638 subjects were included in this study from the SUSALUD-UAQ, an initiative that seeks to determine the risk factors of the main non-communicable diseases in the young population. Participants who met the following criteria were included: men and women with an age range of 18 to 22 years, who agreed to sign the informed consent letter and who had a complete evaluation. Likewise, those with previously diagnosed chronic diseases such as cancer, diabetes, cardiovascular disease, women with polycystic ovarian syndrome, pregnant or lactating women, and those who had thyroid problems were excluded from the study; those who did not have complete evaluation information were eliminated.
From this evaluation, the anthropometric parameters of height (m) and weight (Kg) were selected for the calculation of the BMI (kg/m2) and waist circumference (cm) in the same way as the percentage of body fat, determined by 4-pole multifrequency bioelectrical impedance, using the mBCA Mod. 514 equipment (SECA, Hamburg, Germany). Likewise, biochemical parameters of glucose, TG, cholesterol, and HDL were determined from a blood sample extracted by venipuncture, enzymatic methods (SPINREACT, Girona, Spain), and using the Chemistry Analyzer Mod. BS 120 automated equipment (Mindray, Shenzhen, China).
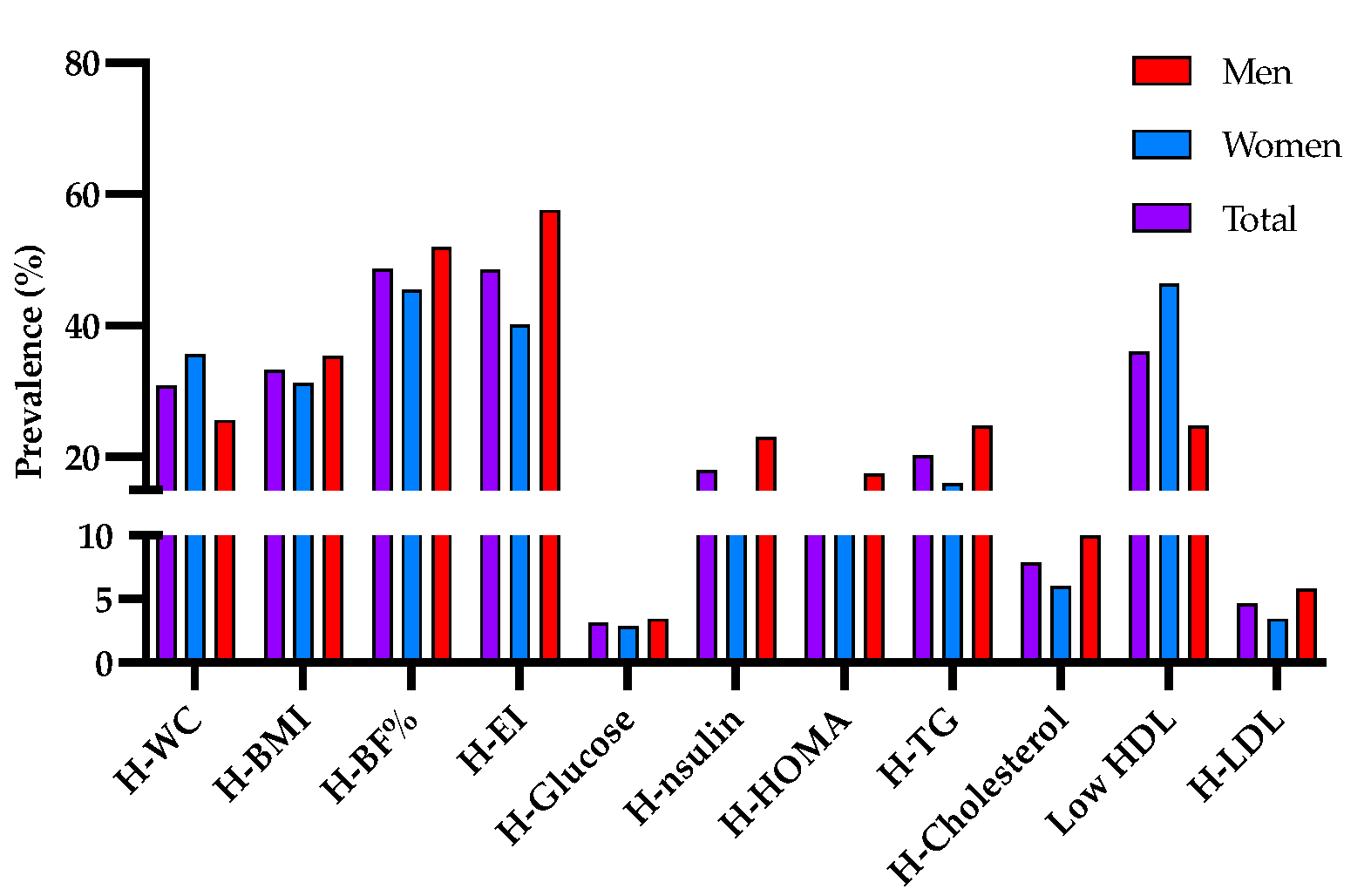
Since there is no accurate diagnosis of obesity, this study took as markers of obesity those that have been found to be the best predictors of obesity and its comorbidities: body mass index (BMI), waist circumference (WC), and body fat percentage (BF%) [
16], as well as elevated triglyceride levels [
17] and high energy intake [
18]. The following values were used as obesity parameters: body mass index > 25.0 kg/m
2; WC in women > 80 cm and in men > 90 cm; percentage of body fat in women > 35% and in men > 20%; TG > 150 mg/dL; and energy intake > population median (>2400 Kcal). Fasting glucose < 100 mg/dL was used to rule out diabetes mellitus.
2.2. Analysis of Genetic Material
Subjects’ DNA samples were obtained from whole blood, using the QIAamp 96 DNA blood kit (QIAGEN, Illumina, CA, USA) and following the supplier’s specifications. The Illumina Infinium HTS Automated protocol, along with the Beadchip Global Screening Array microarray (GSA-24 v1.0), were used for human genotyping [
19,
20] in the Código 46 Genetics Laboratories. Data from 216 genetic variants on the
FTO gene were initially recovered from the whole 669,672 variants on the Illumina microarray. We applied two data filters using PLINK, the percentage of missing variants per sample below 0.05, and the quality per individual with a call rate above 0.95 [
21], which resulted in 175 variants on
FTO fulfilling these filters. Genotypic and allelic frequencies were determined with GenAlEx 6.51 [
22]. Null alleles were excluded from the dataset prior to further analyses; all markers were analyzed for the Hardy–Weinberg equilibrium (HWE) (
Table S1).
2.3. Statistical Analysis
Statistical and descriptive analyses were performed to determine the general characteristics of the population. For the present study, the genotypes were grouped according to the additive model. For the recessive model, the alternative homozygous (xx) and reference homozygous plus heterozygous (XX + Xx) models were used, while for the dominant model, the reference homozygote (XX) and the set of heterozygote and alternative homozygotes were used. Binary logistic regressions were performed to determine significant associations (
p ≤ 0.05) between genetic variants and indicators of obesity. Student’s
t-tests (
p ≤ 0.05) were performed to compare the means of the indicators of obesity for each of the models. One-way ANOVAs were performed to describe the mean differences between the homozygous reference, heterozygous, and homozygous risk populations, followed by the Bonferroni adjustment (
p ≤ 0.05). All statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Macintosh, Version 23.0., Armonk, NY, USA: IBM Corp) [
23].
4. Discussion
Recent studies have shown the importance of the
FTO gene in the development of the organism. Studies in experimental mice showed that suppression of
FTO leads to reduced body weight and body mass, while overexpression promotes an increase in body mass, fat mass, and food consumption [
24]. Therefore,
FTO and downstream genes regulated from non-coding regions, mainly IRX3 and IRX5, which are genes related to neural development in areas associated with food consumption and may be valuable therapeutic targets for obesity [
25,
26] The effects of SNPs have been observed to be differential between populations; such is the case of rs9930506, which was observed to have risk associations with BMI in the European population but not in the Asian population [
27].
The present work analyzed 175 genetic variants of FTO, of which only 34 were associated with any of the indicators of overweight and obesity, while only 16 of these variants showed differences in means according to the recessive model of the minor allele and 12 differences in the average of the indicators of overweight and obesity according to the genotype present, whereas only 4 passed the Bonferroni adjustment. From these last variants, rs12232391 showed differences between the population means in WC, BMI, and BF%; however, it has not been reported in association with any condition.
The variant rs17817449 has been extensively studied, and its effects have been observed in different populations, such as in the case of a study in an Iranian population with type 2 diabetes mellitus [
28] and obesity [
29]. This has also been replicated in Chinese women [
30]. In the current study, the association of this marker with BMI >30 Kg/m
2 and with higher energy consumption was observed, while differences were observed in the means of WC, BMI, and percentage of body fat. The genetic variant rs7191566 was observed in a population study in Mexico but not included in further analyses because it was not in Hardy-Weinberg equilibrium [
7]. Interestingly, in the current work, this marker showed a different genotype when compared with the mean percentage of fat in the population.
In our results, variant rs1421085 was found to be associated with high consumption of Kcal, and mean differences were observed in the percentage of body fat. This marker has been extensively studied, and recent studies have found higher allelic frequencies in people with obesity as well as its associations with higher triglyceride and cholesterol levels in Turkish children [
31]. Likewise, rs1421085 was previously reported with higher allelic frequencies in the Iranian population, showing its association with obesity markers [
32]. In the adult Mexican obese population, rs1421085 has also been considered a genetic marker of risk [
15]. On the other hand, rs3751812 has been associated with obesity in the Taiwanese population, as well as the reduction of its effects by increasing the physical activity for this population [
33], while in a population of Greek adults, when analyzing the same SNP, it was not found in Hardy–Weinberg equilibrium, explaining why it had to be discarded from the study [
34]. Similarly, in a study in the Polish population, it was observed that people carrying this polymorphism tended to have higher levels in the blood lipid profile [
35].
Our findings show a positive association between energy consumption greater than 2400 Kcal and the said marker, in addition to differences in the means of body fat, both in the additive model and in the complete genotype. Similarly, rs17817964 in this study was associated with WC and energy consumption greater than the population median. It should be noted that this genetic marker was also associated with obesity in African-American women over 18 years of age with low birth weight [
36], and it was generally observed as associated with obesity in people with African-American ancestry [
37]. The variant rs2111650 was associated with the percentage of body fat and showed differences in the means of %BF related to its polymorphism; however, it has not been identified as a risk or protective variant in any other population. Furthermore, rs2111650 has been associated in various genome-wide association studies, mainly with obesity markers [
38,
39].
The rs9936385, rs7202116, and rs11075990 did not pass the Bonferroni adjustment and associations with obesity markers have not been observed in other studies. Interestingly, rs9939609 is one of the variants of the
FTO gene that has been most researched for its relationship with clinical obesity markers in various populations, including the Mexican child and adult populations [
40,
41]. It was also associated with hyperglycemia in women from southern Mexico with metabolic syndrome [
42]. In the current study, rs9939609 showed mean differences in the percentage of body fat according to the recessive model and with a higher energy intake, without exceeding the Bonferroni adjustment.
Finally, although FTO is a possible genetic marker for obesity as we have discussed throughout the previous lines when comparing the results of various studies in different populations, further population studies are required to corroborate it as a genetic marker for obesity risk.


 ,
, 



{kind=link}