
Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy

 , , , , , ,
, , , , , ,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Patients and Systemic Inflammation Indexes
- PLR = P/L
- PW/L = P × W/L
- SII = N × P/L
- NPW/L = N × P × W/L
- NPM/L = N × P × M/L
- NPMW/L = N × P × M × W/L
- NPM/LW = N × P × M/(L × W)
- NP/LM = N × P/(L × M)
- NP/(L + M) = N × P/(L + M)
- NPW/LM = N × P × W/(L × M)
- NP/WLM = N × P/(W × (L + M))
- NPW/(L + M) = N × P × W/(L + M)
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Mason, W.P.; Van Den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro-Oncology 2020, 22, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, S.G.M.; Alonso, M.M.; Pasqualetti, F. Basic and Translational Advances in Glioblastoma. BioMed Res. Int. 2018, 2018, 1820345. [Google Scholar] [CrossRef] [PubMed]
- Pasqualetti, F.; Orlandi, P.; Simeon, V.; Cantarella, M.; Giuliani, D.; Di Desidero, T.; Gonnelli, A.; Delishaj, D.; Lombardi, G.; Sechi, A.; et al. Melanocortin Receptor-4 Gene Polymorphisms in Glioblastoma Patients Treated with Concomitant Radio-Chemotherapy. Mol. Neurobiol. 2017, 55, 1396–1404. [Google Scholar] [CrossRef]
- Wesseling, P.; Capper, D.W.H.O. WHO 2016 Classification of gliomas. Neuropathol. Appl. Neurobiol. 2018, 44, 139–150. [Google Scholar] [CrossRef]
- Fanelli, G.; Grassini, D.; Ortenzi, V.; Pasqualetti, F.; Montemurro, N.; Perrini, P.; Naccarato, A.; Scatena, C. Decipher the Glioblastoma Microenvironment: The First Milestone for New Groundbreaking Therapeutic Strategies. Genes 2021, 12, 445. [Google Scholar] [CrossRef]
- Montemurro, N.; Fanelli, G.N.; Scatena, C.; Ortenzi, V.; Pasqualetti, F.; Mazzanti, C.M.; Morganti, R.; Paiar, F.; Naccarato, A.G.; Perrini, P. Surgical outcome and molecular pattern characterization of recurrent glioblastoma multiforme: A single-center retrospective series. Clin. Neurol. Neurosurg. 2021, 207, 106735. [Google Scholar] [CrossRef]
- Yan, Q.; Ertao, Z.; Zhimei, Z.; Weigang, D.; Jianjun, P.; Jianhui, C.; Chuangqi, C. Systemic immune-inflammation index (SII): A More Promising Inflammation-Based Prognostic Marker for Patients with synchronic colorectal peritoneal carcinomatosis. J. Cancer 2020, 11, 5264–5272. [Google Scholar] [CrossRef]
- Wang, D.; Kang, K.; Lin, Q.; Hai, J. Prognostic Significance of Preoperative Systemic Cellular Inflammatory Markers in Gliomas: A Systematic Review and Meta-Analysis. Clin. Transl. Sci. 2019, 13, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat. Cancer 2021, 21, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Liu, Y.; Li, Q.; Li, Z.; Hou, H.; Wu, A. Pre-treatment neutrophil-to-lymphocyte ratio is associated with neutrophil and T-cell infiltration and predicts clinical outcome in patients with glioblastoma. BMC Cancer 2015, 15, 617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavreul, A.; Lemée, J.-M.; Soulard, G.; Rousseau, A.; Menei, P. A Simple Preoperative Blood Count to Stratify Prognosis in Isocitrate Dehydrogenase-Wildtype Glioblastoma Patients Treated with Radiotherapy plus Concomitant and Adjuvant Temozolomide. Cancers 2021, 13, 5778. [Google Scholar] [CrossRef]
- Topkan, E.; Besen, A.A.; Ozdemir, Y.; Küçük, A.; Mertsoylu, H.; Pehlivan, B.; Selek, U. Prognostic Value of Pretreatment Systemic Immune-Inflammation Index in Glioblastoma Multiforme Patients Undergoing Postneurosurgical Radiotherapy Plus Concurrent and Adjuvant Temozolomide. Mediat. Inflamm. 2020, 2020, 4392189. [Google Scholar] [CrossRef]
- Wang, Q.; Tan, X.; Deng, G.; Fu, S.; Li, J.; Li, Z. Dynamic changes in the systemic immune-inflammation index predict the prognosis of EGFR-mutant lung adenocarcinoma patients receiving brain metastasis radiotherapy. BMC Pulm. Med. 2022, 22, 75. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Z.; Jin, F.; Guo, D.; Chen, Q.; Liu, Z.; Ji, S.; Gao, G. The Value of the Systemic Immune-Inflammation Index in Predicting Survival Outcomes in Patients with Brain Metastases of Non-Small-Cell Lung Cancer Treated with Stereotactic Radiotherapy. Mediat. Inflamm. 2021, 2021, 2910892. [Google Scholar] [CrossRef] [PubMed]
- Perrini, P.; Gambacciani, C.; Weiss, A.; Pasqualetti, F.; Delishaj, D.; Paiar, F.; Morganti, R.; Vannozzi, R.; Lutzemberger, L. Survival outcomes following repeat surgery for recurrent glioblastoma: A single-center retrospective analysis. J. Neuro-Oncol. 2016, 131, 585–591. [Google Scholar] [CrossRef]
- Pasqualetti, F.; Gonnelli, A.; Molinari, A.; Cantarella, M.; Montrone, S.; Cristaudo, A.; Baldaccini, D.; Mattioni, R.; Delishaj, D.; Mazzotti, V.; et al. Different Timing to Use Bevacizumab in Patients with Recurrent Glioblastoma: Early Versus Delayed Administration. Anticancer Res. 2018, 38, 5877–5881. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; DeGroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Afshar-Kharghan, V.; Schafer, A.I. Paraneoplastic thrombocytosis: The secrets of tumor self-promotion. Blood 2014, 124, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Karpatkin, S.; Pearlstein, E. Role of Platelets in Tumor Cell Metastases. Ann. Intern. Med. 1981, 95, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Nolte, I.; Przibylla, H.; Bostel, T.; Groden, C.; Brockmann, M.A. Tumor–platelet interactions: Glioblastoma growth is accompanied by increasing platelet counts. Clin. Neurol. Neurosurg. 2008, 110, 339–342. [Google Scholar] [CrossRef]
- Yu, D.; Liu, B.; Zhang, L.; Du, K. Platelet count predicts prognosis in operable non-small cell lung cancer. Exp. Ther. Med. 2013, 5, 1351–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Suh, K.W.; Oh, S.Y. Preoperative thrombocytosis predicts prognosis in stage II colorectal cancer patients. Ann. Surg. Treat. Res. 2016, 90, 322–327. [Google Scholar] [CrossRef] [Green Version]
- Marini, A.; Dobran, M.; Aiudi, D.; Pesaresi, A.; di Somma, L.G.M.; Iacoangeli, M. Pre-operative hematological markers as predictive factors for overall survival and progression free survival in glioblastomas. Clin. Neurol. Neurosurg. 2020, 197, 106162. [Google Scholar] [CrossRef]
- Uribe-Querol, E.; Rosales, C. Neutrophils in Cancer: Two Sides of the Same Coin. J. Immunol. Res. 2015, 2015, 983698. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.R.; Huttenlocher, A. Neutrophils in the Tumor Microenvironment. Trends Immunol. 2015, 37, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Liang, J.; Piao, Y.; Holmes, L.; Fuller, G.; Henry, V.; Tiao, N.; De Groot, J.F. Neutrophils Promote the Malignant Glioma Phenotype through S100A4. Clin. Cancer Res. 2013, 20, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, A.; Cederarv, M.; Wolmer-Solberg, N.; Tammik, C.; Stragliotto, G.; Peredo, I.; Fornara, O.; Xu, X.; Dzabic, M.; Taher, C.; et al. Enhanced neutrophil activity is associated with shorter time to tumor progression in glioblastoma patients. OncoImmunology 2015, 5, e1075693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Mittal, S.; McGee, K.; Alfaro-Munoz, K.D.; Majd, N.; Balasubramaniyan, V.; de Groot, J.F. Role of Neutrophils and Myeloid-Derived Suppressor Cells in Glioma Progression and Treatment Resistance. Int. J. Mol. Sci. 2020, 21, 1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolás-Ávila, J.Á.; Adrover, J.M.; Hidalgo, A. Neutrophils in Homeostasis, Immunity, and Cancer. Immunity 2017, 46, 15–28. [Google Scholar] [CrossRef] [Green Version]
- Sippel, T.R.; White, J.; Nag, K.; Tsvankin, V.; Klaassen, M.; Kleinschmidt-DeMasters, B.; Waziri, A. Neutrophil Degranulation and Immunosuppression in Patients with GBM: Restoration of Cellular Immune Function by Targeting Arginase I. Clin. Cancer Res. 2011, 17, 6992–7002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Song, H.-W.; Cai, H.-Q.; Kong, L.-W.; Yao, K.; Jiang, T.; Li, S.; Yan, C.-X. Preoperative inflammation markers and IDH mutation status predict glioblastoma patient survival. Oncotarget 2017, 8, 50117–50123. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Feature | Number |
|---|---|
| Gender M/F | 43/34 |
| Median age (years) | 64 (range 26–84) |
| Second surgery | 20 (24.3%) |
| Median KPS | 80 |
| Extent of Surgery: Gross Tumor Removal: 31 (40.2%) Partial Tumor Removal: 46 (59.8%) | |
| MGMT meth. | 23/34 (67.6%) |
| Blood cells | Mean Value |
| White blood cells | 9.26 (3.55) |
| Red blood cells | 4.70 (0.50) |
| Hemoglobin | 13.9 (1.6) |
| Platelets | 246 (87) |
| Neutrophils | 6.75 (3.29) |
| Lymphocytes | 1.96 (1.39) |
| Monocytes | 0.608 (0.393) |
| Eosinophils | 0.073 (0.082) |
| Basophils | 0.016 (0.013) |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Factor | HR (95% CI) | p-Value | RC | HR (95% CI) | p-Value |
| PLR (0) ≤ 250 (1) > 250 | 2.402 (1.242–4.644) | 0.009 | 0.477 | ||
| PLRW (0) < 2500 (1) ≥ 2500 | 2.175 (0.965–4.903) | 0.061 | 0.363 | ||
| SII (0) < 1200 (1) ≥ 1200 | 1.848 (1.056–3.234) | 0.032 | 0.924 | ||
| NPW/L (0) < 7500 (1) ≥ 7500 | 1.773 (1.045–3.007) | 0.034 | 0.894 | ||
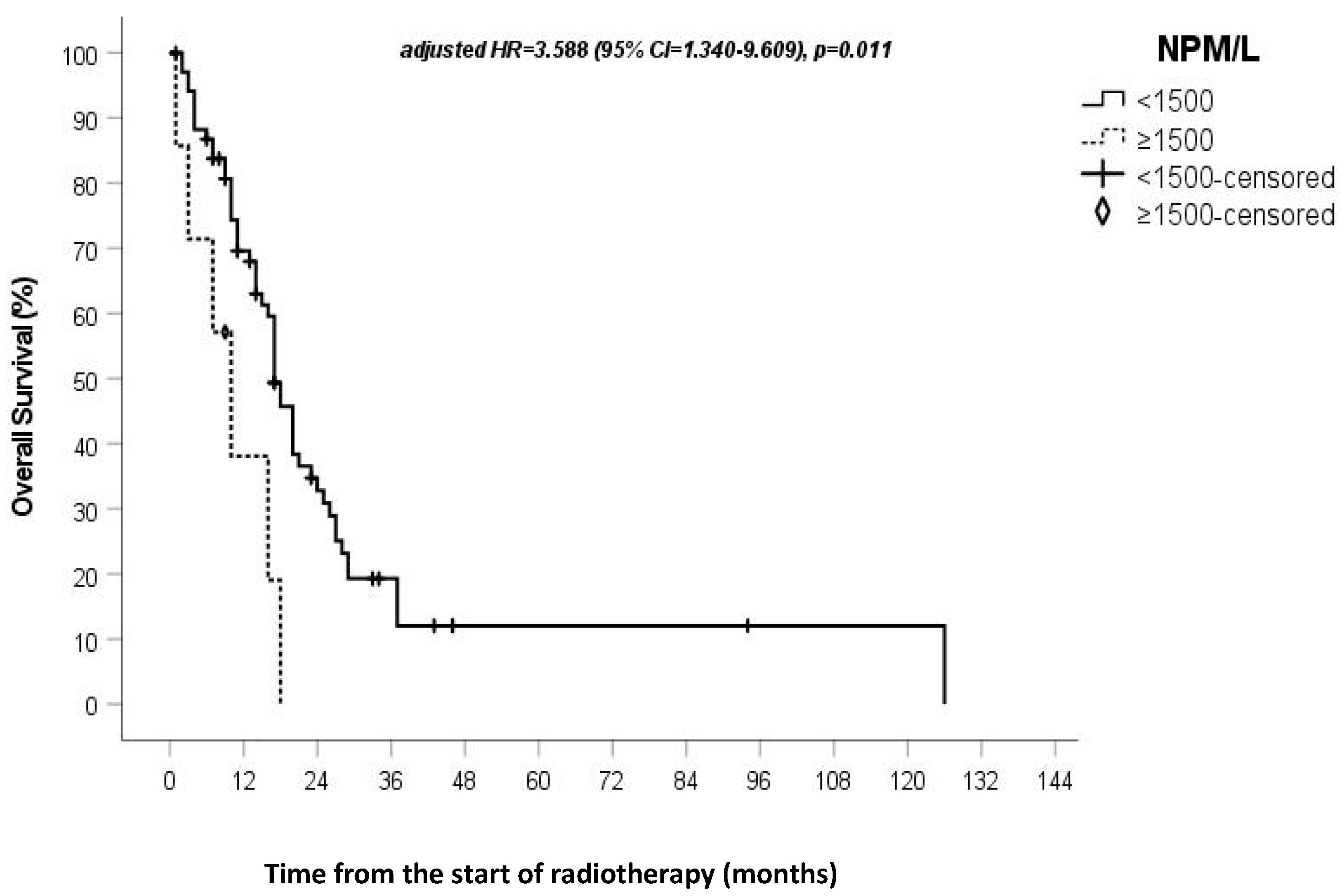
| NPM/L (0) < 1500 (1) ≥ 1500 | 2.983 (1.243–7.161) | 0.014 | 1.278 | 3.588 (1.340–9.609) | 0.011 |
| NPMW/L (0) < 8000 (1) ≥ 8000 | 3.271 (1.269–8.435) | 0.014 | 0.538 | ||
| NPM/LW (0) < 90 (1) ≥ 90 | 2.404 (1.148–5.033) | 0.020 | 0.941 | ||
| NP/LM (0) < 5000 (1) ≥ 5000 | 2.283 (1.179–4.420) | 0.014 | 0.748 | ||
| NP/(L + M) (0) < 1300 (1) ≥ 1300 | 2.263 (1.147–4.463) | 0.018 | 0.736 | ||
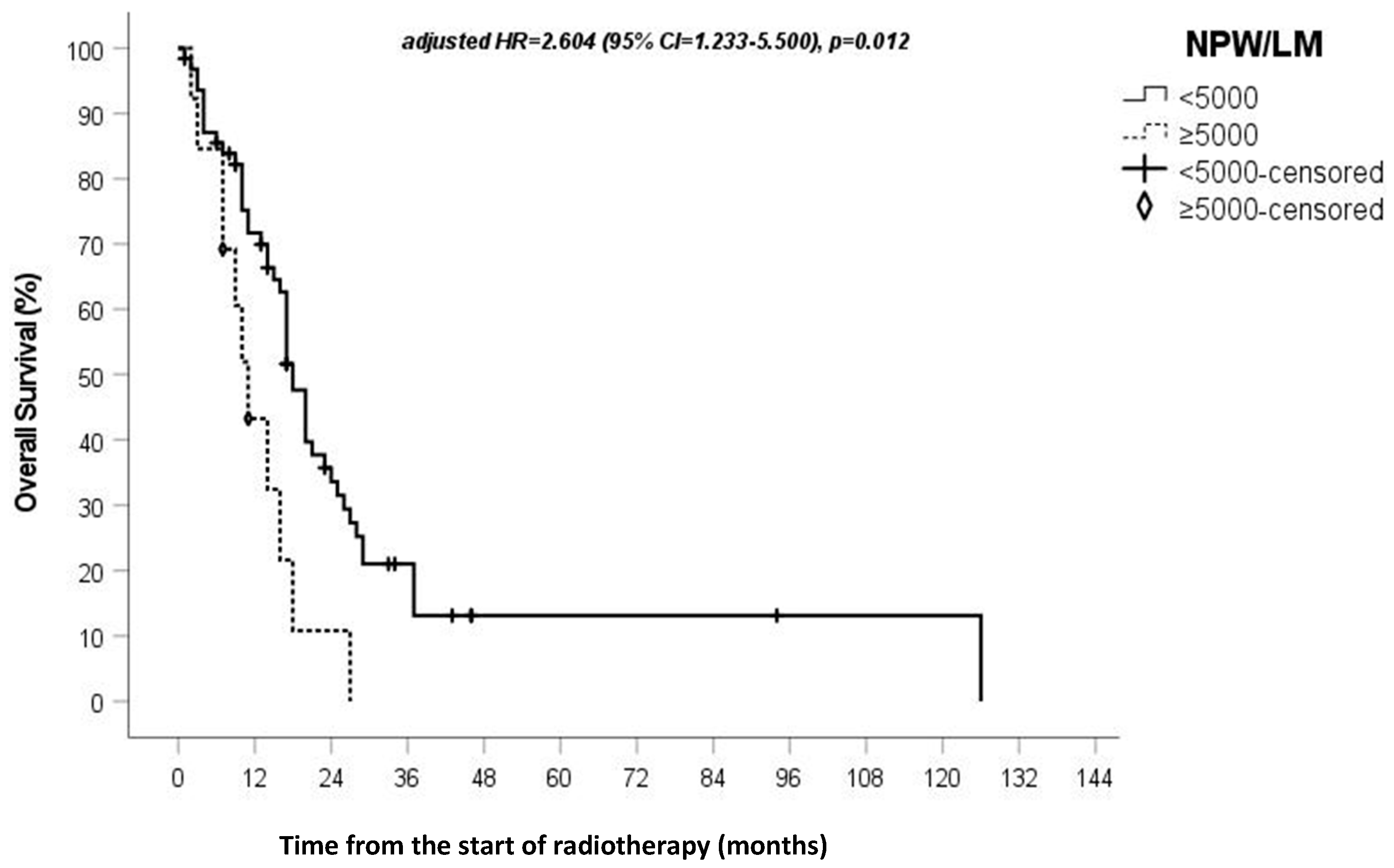
| NPW/LM (0) < 5000 (1) ≥ 5000 | 2.411 (1.218–4.771) | 0.012 | 0.957 | 2.604 (1.233–5.500) | 0.012 |
| NP/LMW (0) < 1000 (1) ≥ 1000 | 2.147 (1.036–4.450) | 0.040 | 0.996 | ||
| NPW/(L + M) (0) < 2500 (1) ≥ 2500 | 1.852 (0.930–3.689) | 0.080 | 0.860 | ||
| Surgery (0) GTR (1) STR | 2.235 (1.214–4.117) | 0.010 | 0.703 | 2.020 (1.081–3.775) | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasqualetti, F.; Giampietro, C.; Montemurro, N.; Giannini, N.; Gadducci, G.; Orlandi, P.; Natali, E.; Chiarugi, P.; Gonnelli, A.; Cantarella, M.; et al. Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy. Genes 2022, 13, 1054. https://doi.org/10.3390/genes13061054
Pasqualetti F, Giampietro C, Montemurro N, Giannini N, Gadducci G, Orlandi P, Natali E, Chiarugi P, Gonnelli A, Cantarella M, et al. Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy. Genes. 2022; 13(6):1054. https://doi.org/10.3390/genes13061054
Chicago/Turabian StylePasqualetti, Francesco, Celeste Giampietro, Nicola Montemurro, Noemi Giannini, Giovanni Gadducci, Paola Orlandi, Eleonora Natali, Paolo Chiarugi, Alessandra Gonnelli, Martina Cantarella, and et al. 2022. "Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy" Genes 13, no. 6: 1054. https://doi.org/10.3390/genes13061054