
Randomized Clinical Trial of Antioxidant Therapy Patients with Septic Shock and Organ Dysfunction in the ICU: SOFA Score Reduction by Improvement of the Enzymatic and Non-Enzymatic Antioxidant System


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Study
2.2. Sample Size
2.3. Ethical Aspects
2.4. Randomization
2.5. Data Collection
2.6. Description of the Intervention
2.7. Sample Collection and Storage
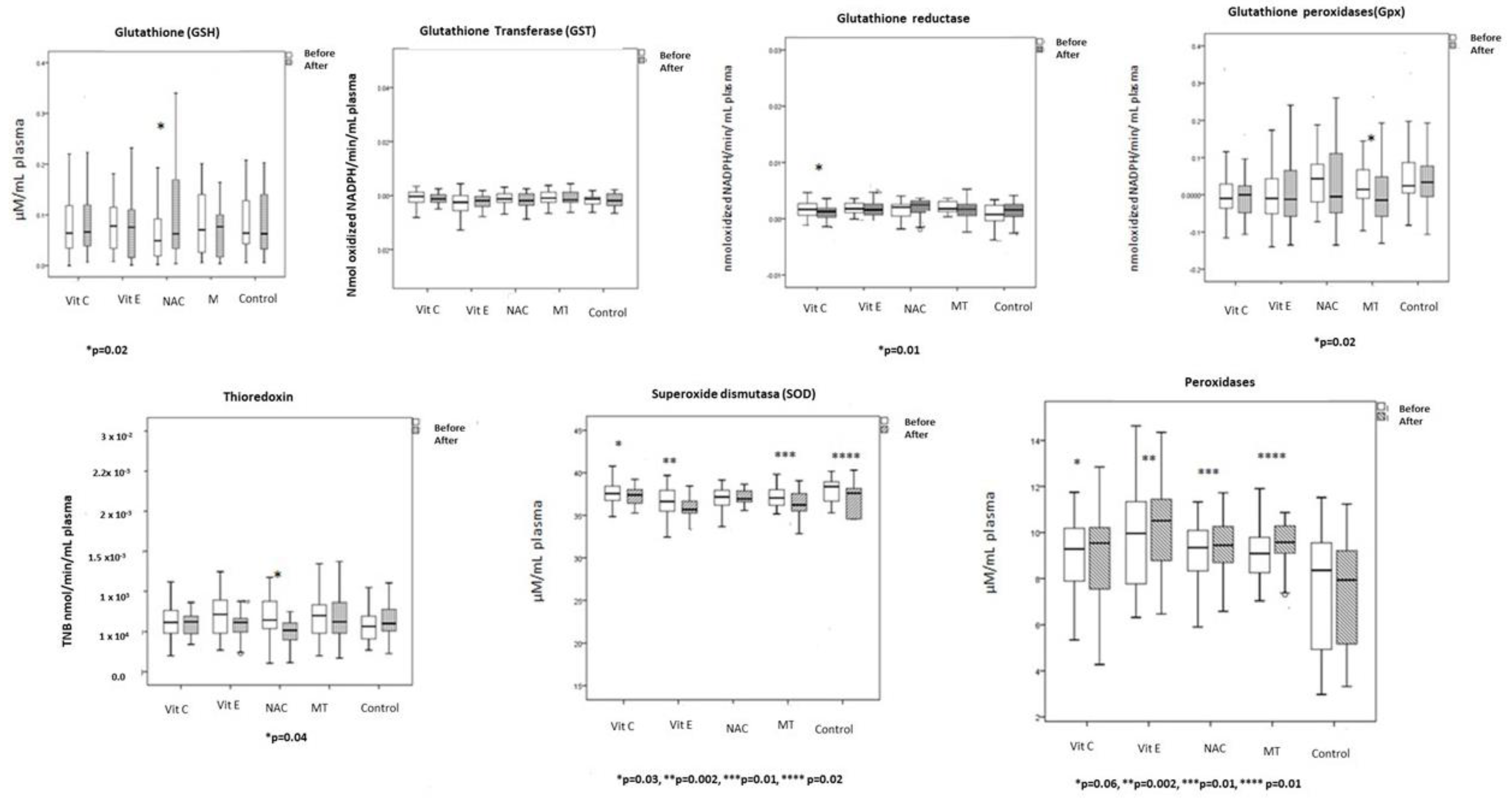
2.8. Evaluation of the Antioxidant Enzymes
2.8.1. GPx Activity
2.8.2. GST Activity
2.8.3. TrxR Activity
2.8.4. Extracellular Super Oxide Dismutase (ecSOD) Activity
2.8.5. Peroxidase Activity
2.8.6. GR Activity
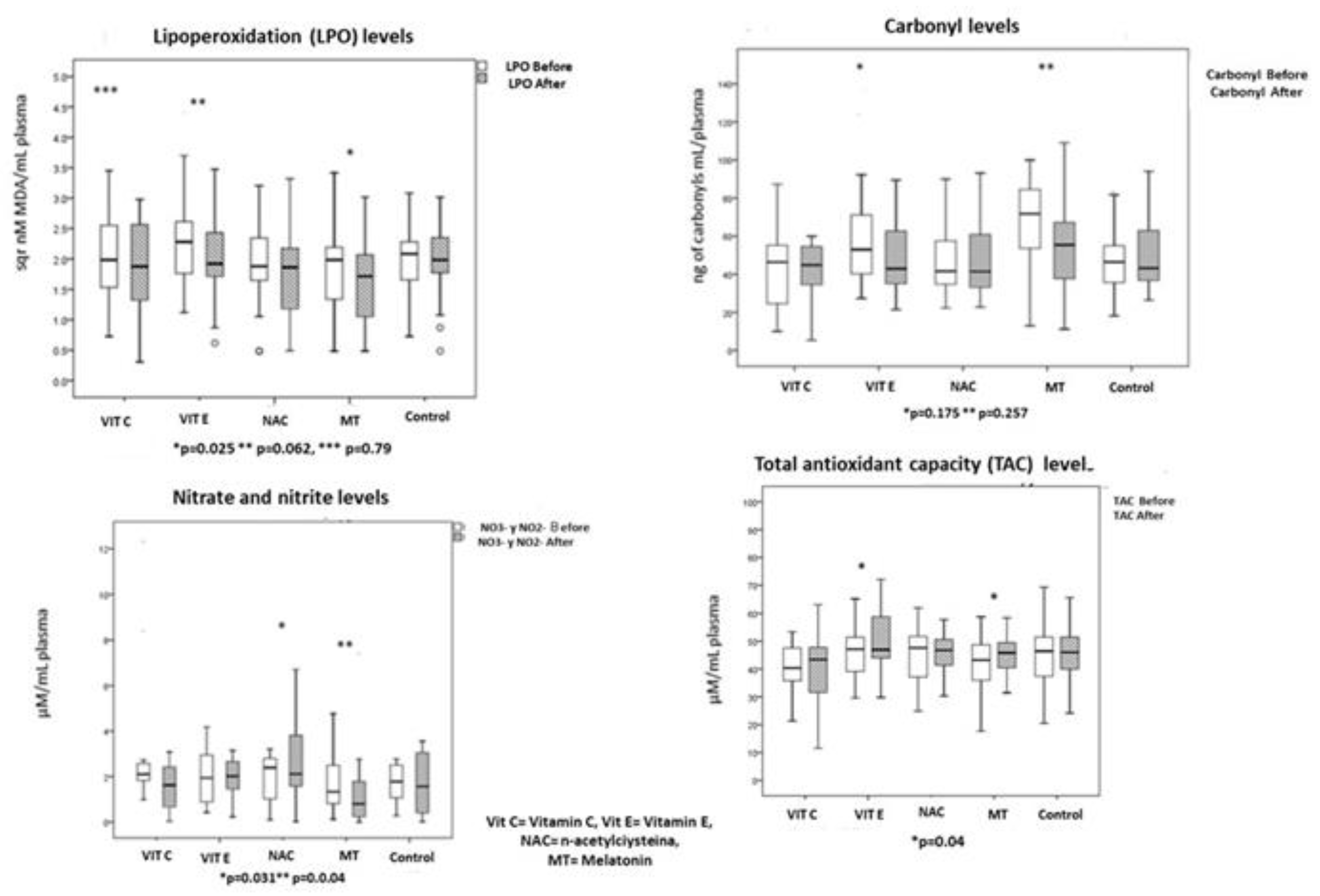
2.9. Oxidative Stress Markers
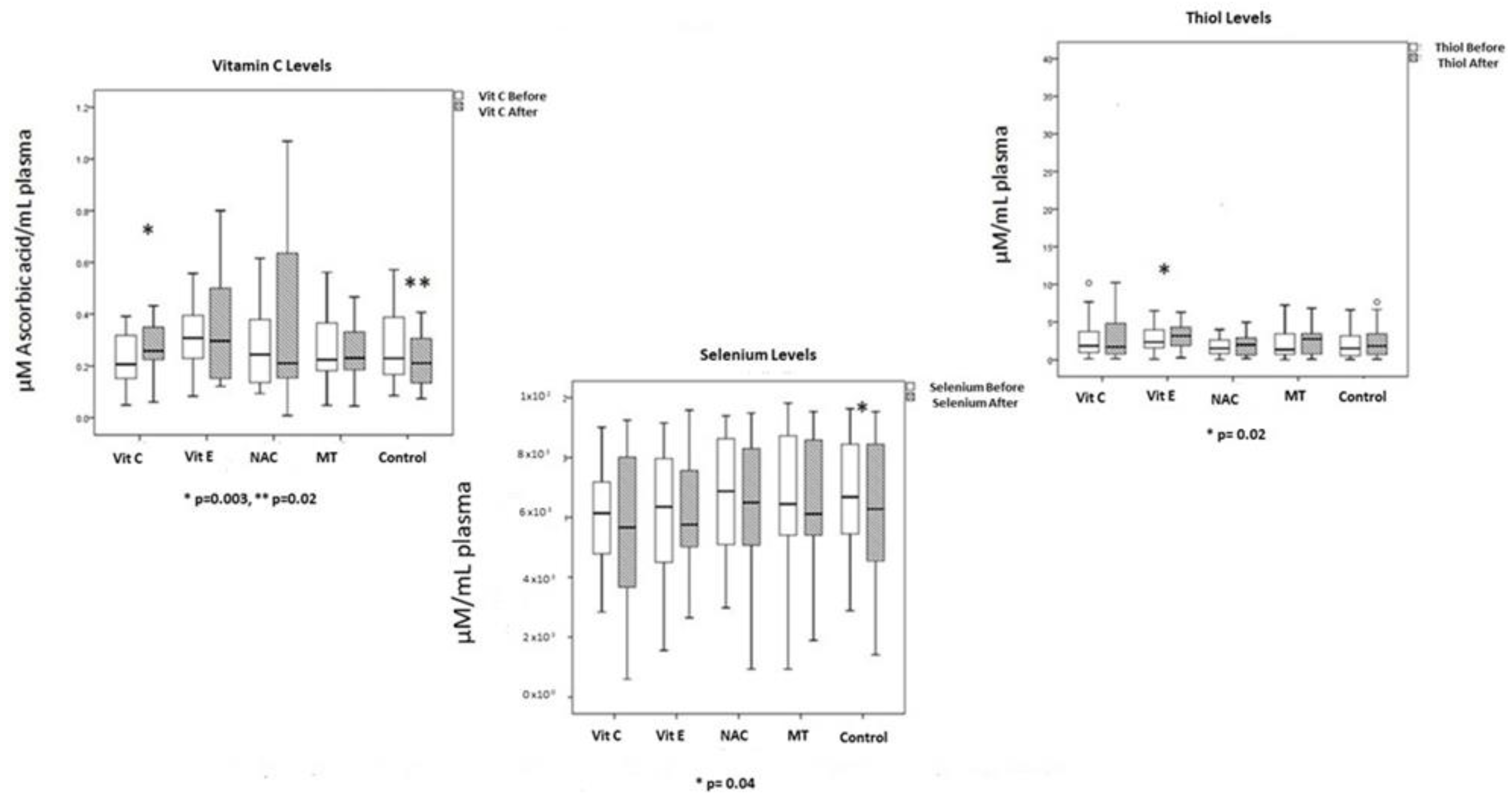
2.9.1. Determination of Selenium (Se)
2.9.2. Thiols
2.9.3. Total Antioxidant Capacity (TAC)
2.9.4. Lipid Peroxidation (LPO)
2.9.5. NO3−/NO2− Ratio
2.9.6. Carbonylation
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marshall, J.C.; Vincent, J.-L.; Guyatt, G.; Angus, D.C.; Abraham, E.; Bernard, G.; Bombardier, C.; Calandra, T.; Jørgensen, H.S.; Sylvester, R.; et al. Outcome Measures for Clinical Research in Sepsis: A Report of the 2nd Cambridge Colloquium of the International Sepsis Forum. Crit. Care Med. 2005, 33, 1708–1716. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of Severe Sepsis in the United States: Analysis of Incidence, Outcome, and Associated Costs of Care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef]
- Gorordo-Delsol, L.A.; Merinos-Sánchez, G.; Estrada-Escobar, R.A.; Medveczky-Ordoñez, N.I.; Amezcua-Gutiérrez, M.A.; Morales-Segura, M.A.; Uribe-Moya, S.E. Sepsis and Septic Shock in Emergency Departments of Mexico: A Multicenter Point Prevalence Study. Gac. Med. Méx. 2021, 156, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Ericson, O.; Hjelmgren, J.; Fredrik Sjövall, F.; Söderberg, J.; Persson, I. The Potential Cost and Cost-Effectiveness Impact of Using a Machine Learning Algorithm for Early Detection of Sepsis in Intensive Care Units in Sweden. J. Health Econ. Outcomes Res. 2022, 9, 101–110. [Google Scholar] [PubMed]
- Xiao, L.; Niu, L.; Xu, X.; Zhao, Y.; Yue, L.; Liu, X.; Li, G. Comparative Efficacy of Tonic Chinese Herbal Injections for Treating Sepsis or Septic Shock: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials. Front. Pharmacol. 2022, 13, 830030. [Google Scholar] [CrossRef]
- Xiao, H.; Wang, G.; Wang, Y.; Tan, Z.; Sun, X.; Zhou, J.; Duan, M.; Zhi, D.; Tang, Z.; Hang, C.; et al. Potential Value of Presepsin Guidance in Shortening Antibiotic Therapy in Septic Patients: A Multicenter, Prospective Cohort Trial. Shock 2022, 57, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.J.; Young, P.J.; Venkatesh, B.; Cohen, J.; Finfer, S.R.; Grattan, S.; Hammond, N.E.; Jan, S.; Li, Q.; di Tanna, G.L.; et al. Long-Term Costs and Cost-Effectiveness of Adjunctive Corticosteroids for Patients with Septic Shock in New Zealand. Aust. Crit. Care 2022, 35, 241–250. [Google Scholar] [CrossRef]
- Costa, N.A.; Pereira, A.G.; Sugizaki, C.S.A.; Vieira, N.M.; Garcia, L.R.; de Paiva, S.A.R.; Zornoff, L.A.M.; Azevedo, P.S.; Polegato, B.F.; Minicucci, M.F. Insights Into Thiamine Supplementation in Patients with Septic Shock. Front. Med. 2022, 8, 805199. [Google Scholar] [CrossRef]
- Doganyigit, Z.; Eroglu, E.; Akyuz, E. Inflammatory Mediators of Cytokines and Chemokines in Sepsis: From Bench to Bedside. Hum. Exp. Toxicol. 2022, 41, 096032712210788. [Google Scholar] [CrossRef] [PubMed]
- Cross, D.; Drury, R.; Hill, J.; Pollard, A.J. Epigenetics in Sepsis: Understanding Its Role in Endothelial Dysfunction, Immunosuppression, and Potential Therapeutics. Front. Immunol. 2019, 10, 1363. [Google Scholar] [CrossRef]
- Pacheco-Navarro, A.E.; Rogers, A.J. The Metabolomics of Critical Illness. Handb. Exp. Pharmacol. 2023, 277, 367–384. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Cheng, M.; Li, J.; Zhang, P.; Fan, H.; Hu, Q.; Han, M.; Su, L.; He, H.; Tong, Y.; et al. Classification of the Gut Microbiota of Patients in Intensive Care Units during Development of Sepsis and Septic Shock. Genom. Proteom. Bioinform. 2020, 18, 696–707. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, M.; Chen, W.; Ma, J.; Peng, Y.; Zhang, M.; Wang, C.; Yan, G.; Lu, G. Altered Gut Microbiota Taxonomic Compositions of Patients with Sepsis in a Pediatric Intensive Care Unit. Front. Pediatr. 2021, 9, 645060. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; He, C.; Liu, C.; Xu, X.; Chen, C.; Yang, H.; Shi, H.; Fei, Y.; Sun, Y.; Zhou, S.; et al. Mechanisms of JinHong Formula on Treating Sepsis Explored by Randomized Controlled Trial Combined with Network Pharmacology. J. Ethnopharmacol. 2023, 305, 116040. [Google Scholar] [CrossRef]
- Zhu, H.; Zhang, L.; Jia, H.; Xu, L.; Cao, Y.; Zhai, M.; Li, K.; Xia, L.; Jiang, L.; Li, X.; et al. Tetrahydrocurcumin Improves Lipopolysaccharide-Induced Myocardial Dysfunction by Inhibiting Oxidative Stress and Inflammation via JNK/ERK Signaling Pathway Regulation. Phytomedicine 2022, 104, 154283. [Google Scholar] [CrossRef]
- Zhu, X.; Sun, M.; Guo, H.; Lu, G.; Gu, J.; Zhang, L.; Shi, L.; Gao, J.; Zhang, D.; Wang, W.; et al. Verbascoside Protects from LPS-Induced Septic Cardiomyopathy via Alleviating Cardiac Inflammation, Oxidative Stress and Regulating Mitochondrial Dynamics. Ecotoxicol. Environ. Saf. 2022, 233, 113327. [Google Scholar] [CrossRef] [PubMed]
- Matzinger, P. The Danger Model: A Renewed Sense of Self. Science 2002, 296, 301–305. [Google Scholar] [CrossRef]
- Shati, A.A.; Zaki, M.S.A.; Alqahtani, Y.A.; Al-Qahtani, S.M.; Haidara, M.A.; Dawood, A.F.; AlMohanna, A.M.; El-Bidawy, M.H.; Alaa Eldeen, M.; Eid, R.A. Antioxidant Activity of Vitamin C against LPS-Induced Septic Cardiomyopathy by Down-Regulation of Oxidative Stress and Inflammation. Curr. Issues Mol. Biol. 2022, 44, 2387–2400. [Google Scholar] [CrossRef]
- Conway-Morris, A.; Wilson, J.; Shankar-Hari, M. Immune Activation in Sepsis. Crit. Care Clin. 2018, 34, 29–42. [Google Scholar] [CrossRef]
- Hawiger, J. Heartfelt Sepsis: Microvascular Injury Due to Genomic Storm. Kardiol. Pol. 2018, 76, 1203–1216. [Google Scholar] [CrossRef]
- Rosengart, M.R.; Nathens, A.B.; Arbabi, S.; Neff, M.J.; Garcia, I.; Martin, T.R.; Maier, R.v. Mitogen-Activated Protein Kinases in the Intensive Care Unit: Prognostic Potential. Ann. Surg. 2003, 237, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Kaminskyy, V.O.; Zhivotovsky, B. Free Radicals in Cross Talk Between Autophagy and Apoptosis. Antioxid. Redox Signal. 2014, 21, 86–102. [Google Scholar] [CrossRef]
- Cavaillon, J.; Singer, M.; Skirecki, T. Sepsis Therapies: Learning from 30 Years of Failure of Translational Research to Propose New Leads. EMBO Mol. Med. 2020, 12, e10128. [Google Scholar] [CrossRef] [PubMed]
- Venet, F.; Davin, F.; Guignant, C.; Larue, A.; Cazalis, M.-A.; Darbon, R.; Allombert, C.; Mougin, B.; Malcus, C.; Poitevin-Later, F.; et al. Early assessment of leukocyte alterations at diagnosis of septic shock. Shock 2010, 34, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.; O’Dea, K.; Gordon, A. Immune Therapy in Sepsis: Are We Ready to Try Again? J. Intensive Care Soc. 2018, 19, 326–344. [Google Scholar] [CrossRef]
- Ramesh, B.; Karuna, R.; Sreenivasa, R.S.; Haritha, K.; Sai, M.D.; Sasis, B.R.B.; Saralakumari, D. Effect of Commiphora Mukul Gum Resin on Hepatic Marker Enzymes, Lipid Peroxidation and Antioxidants Status in Pancreas and Heart of Streptozotocin Induced Diabetic Rats. Asian. Pac. J. Trop. Biomed. 2012, 2, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Sotoudeh, R.; Hadjzadeh, M.; Gholamnezhad, Z.; Aghaei, A. The anti-diabetic and antioxidant effects of a combination of Commiphora mukul, Commiphora myrrha and Terminalia chebula in diabetic rats. Avicenna J. Phytomed. 2019, 9, 454–464. [Google Scholar]
- Prauchner, C.A. Oxidative Stress in Sepsis: Pathophysiological Implications Justifying Antioxidant Co-Therapy. Burns 2017, 43, 471–485. [Google Scholar] [CrossRef]
- Lowes, D.A.; Webster, N.R.; Murphy, M.P.; Galley, H.F. Antioxidants That Protect Mitochondria Reduce Interleukin-6 and Oxidative Stress, Improve Mitochondrial Function, and Reduce Biochemical Markers of Organ Dysfunction in a Rat Model of Acute Sepsis. Br. J. Anaesth. 2013, 110, 472–480. [Google Scholar] [CrossRef]
- Park, J.E.; Shin, T.G.; Jeong, D.; Lee, G.T.; Ryoo, S.M.; Kim, W.Y.; Jo, Y.H.; Suh, G.J.; Hwang, S.Y. Association between Vitamin C Deficiency and Mortality in Patients with Septic Shock. Biomedicines 2022, 10, 2090. [Google Scholar] [CrossRef]
- Zhu, H.; Xu, X.; Zhang, K.; Ye, Q. The Effect of Intravenous Vitamin C on Clinical Outcomes in Patients with Sepsis or Septic Shock: A Meta-Analysis of Randomized Controlled Trials. Front. Nutr. 2022, 9, 964484. [Google Scholar] [CrossRef]
- Aisa-Alvarez, A.; Soto, M.E.; Guarner-Lans, V.; Camarena-Alejo, G.; Franco-Granillo, J.; Martínez-Rodríguez, E.A.; Gamboa Ávila, R.; Manzano Pech, L.; Pérez-Torres, I. Usefulness of Antioxidants as Adjuvant Therapy for Septic Shock: A Randomized Clinical Trial. Medicina 2020, 56, 619. [Google Scholar] [CrossRef] [PubMed]
- Chavarría, A.P.; Vázquez, R.R.V.; Cherit, J.G.D.; Bello, H.H.; Suastegui, H.C.; Moreno-Castañeda, L.; Alanís Estrada, G.; Hernández, F.; González-Marcos, O.; Saucedo-Orozco, H.; et al. Antioxidants and Pentoxifylline as Coadjuvant Measures to Standard Therapy to Improve Prognosis of Patients with Pneumonia by COVID-19. Comput. Struct. Biotechnol. J. 2021, 19, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef] [PubMed]
- Fowler, A.A.; Syed, A.A.; Knowlson, S.; Sculthorpe, R.; Farthing, D.; De Wilde, C.; Farthing, C.A.; Larus, T.L.; Martin, E.; Brophy, D.F.; et al. Phase I Safety Trial of Intravenous Ascorbic Acid in Patients with Severe Sepsis. J. Transl. Med. 2014, 12, 32. [Google Scholar] [CrossRef]
- Friedland, J.S.; Porter, J.C.; Daryanani, S.; Bland, J.M.; Screaton, N.J.; Vesely, M.J.J.; Griffin, G.E.; Bennett, E.D.; Remick, D.G. Plasma Proinflammatory Cytokine Concentrations, Acute Physiology and Chronic Health Evaluation (APACHE) III Scores and Survival in Patients in an Intensive Care Unit. Crit. Care Med. 1996, 24, 1775–1781. [Google Scholar] [CrossRef] [PubMed]
- Ghuysen, A.; Lambermont, B.; D’Orio, V. Application Du Simplified Acute Physiology Score II (SAPS II) Dans Une Unité de Soins Intensifs Médicaux. Ann. Fr. Anesth. Reanim. 2000, 19, 510–516. [Google Scholar] [CrossRef]
- Flohé, L.; Günzler, W.A. Assays of Glutathione Peroxidase. Methods. Enzymol. 1984, 105, 114–120. [Google Scholar] [PubMed]
- Soto, M.E.; Soria-Castro, E.; Guarner Lans, V.; Muruato Ontiveros, E.; Iván Hernández Mejía, B.; Jorge Martínez Hernandez, H.; Barragán García, R.; Herrera, V.; Pérez-Torres, I. Analysis of Oxidative Stress Enzymes and Structural and Functional Proteins on Human Aortic Tissue from Different Aortopathies. Oxid. Med. Cell. Longev. 2014, 2014, 760694. [Google Scholar] [CrossRef]
- Holmgren, A.; Bjornstedt, M. Thioredoxin and Thioredoxin Reductase. Methods Enzymol. 1995, 252, 199–208. [Google Scholar]
- Pérez-Torres, I.; Roque, P.; el Hafidi, M.; Diaz-Diaz, E.; Baños, G. Association of Renal Damage and Oxidative Stress in a Rat Model of Metabolic Syndrome. Influence of Gender. Free Radic. Res. 2009, 43, 761–771. [Google Scholar] [CrossRef]
- Zúñiga-Muñoz, A.M.; Pérez-Torres, I.; Guarner-Lans, V.; Núñez-Garrido, E.; Velázquez Espejel, R.; Huesca-Gómez, C.; Gamboa-Ávila, R.; Soto, M.E. Glutathione System Participation in Thoracic Aneurysms from Patients with Marfan Syndrome. Vasa 2017, 46, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Manzano-Pech, L.G.; Guarner-Lans, V.; Díaz-Galindo, J.A.; Vásquez, X.; Castrejón-Tellez, V.; Gamboa, R.; Huesca, C.; Fuentevilla-Alvárez, G.; Pérez-Torres, I. Oxidant/Antioxidant Profile in the Thoracic Aneurysm of Patients with the Loeys-Dietz Syndrome. Oxid. Med. Cell. Longev. 2020, 2020, 5392454. [Google Scholar] [CrossRef] [PubMed]
- Benzie, I.F.F.; Strain, J.J. The Ferric Reducing Ability of Plasma (FRAP) as a Measure of “Antioxidant Power”: The FRAP Assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torres, I.; Soto, M.E.; Manzano-Pech, L.; Díaz-Diaz, E.; Soria-Castro, E.; Rubio-Ruíz, M.E.; Guarner-Lans, V. Oxidative Stress in Plasma from Patients with Marfan Syndrome Is Modulated by Deodorized Garlic Preliminary Findings. Oxid. Med. Cell. Longev. 2022, 2022, 5492127. [Google Scholar] [CrossRef]
- Ruiz-Sanmartín, A.; Ribas, V.; Suñol, D.; Chiscano-Camón, L.; Palmada, C.; Bajaña, I.; Larrosa, N.; González, J.J.; Canela, N.; Ferrer, R.; et al. Characterization of a Proteomic Profile Associated with Organ Dysfunction and Mortality of Sepsis and Septic Shock. PLoS ONE 2022, 17, e0278708. [Google Scholar] [CrossRef]
- Zou, R.; Tao, J.; Qiu, J.; Lu, H.; Wu, J.; Zhu, H.; Li, R.; Mui, D.; Toan, S.; Chang, X.; et al. DNA-PKcs Promotes Sepsis-Induced Multiple Organ Failure by Triggering Mitochondrial Dysfunction. J. Adv. Res. 2022, 41, 39–48. [Google Scholar] [CrossRef]
- Escames, G.; Guerrero, J.M.; Reiter, R.J.; Garcia, J.J.; Munoz-Hoyos, A.; Ortiz, G.G.; Oh, C.S. Melatonin and Vitamin E Limit Nitric Oxide-Induced Lipid Peroxidation in Rat Brain Homogenates. Neurosci. Lett. 1997, 230, 147–150. [Google Scholar] [CrossRef]
- Vlasiuk, E.; Rosengrave, P.; Roberts, E.; Boden, J.M.; Shaw, G.; Carr, A.C. Critically Ill Septic Patients Have Elevated Oxidative Stress Biomarkers: Lack of Attenuation by Parenteral Vitamin C. Nutr. Res. 2022, 108, 53–59. [Google Scholar] [CrossRef]
- Ho, C.T.; Chan, A.C. Regeneration of Vitamin E in Rat Polymorphonuclear Leucocytes. FEBS Lett. 1992, 306, 269–272. [Google Scholar] [CrossRef]
- Martin, G.S.; Mannino, D.M.; Eaton, S.; Moss, M. The Epidemiology of Sepsis in the United States from 1979 through 2000. N. Eng. J. Med. 2003, 348, 1546–1554. [Google Scholar] [CrossRef] [PubMed]
- Galli, F. Vitamin C, Vitamin E and Immune Response. J. Nutr. Biochem. 2005, 16, 257. [Google Scholar] [CrossRef] [PubMed]
- Schorah, C.J.; Downing, C.; Piripitsi, A.; Gallivan, L.; Al-Hazaa, A.H.; Sanderson, M.J.; Bodenham, A. Total Vitamin C, Ascorbic Acid, and Dehydroascorbic Acid Concentrations in Plasma of Critically Ill Patients. Am. J. Clin. Nutr. 1996, 63, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Oudemans-van Straaten, H.M. Vitamin C Supplementation in the Critically Ill Patient. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 193–201. [Google Scholar] [CrossRef]
- Dalle-Donne, I.; Giustarini, D.; Colombo, R.; Rossi, R.; Milzani, A. Protein Carbonylation in Human Diseases. Trends Mol. Med. 2003, 9, 169–176. [Google Scholar] [CrossRef]
- Dilek, O. Current Probes for Imaging Carbonylation in Cellular Systems and Their Relevance to Progression of Diseases. Technol. Cancer Res. Treat. 2022, 21, 153303382211373. [Google Scholar] [CrossRef]
- Spencer, E.; Rosengrave, P.; Williman, J.; Shaw, G.; Carr, A.C. Circulating Protein Carbonyls Are Specifically Elevated in Critically Ill Patients with Pneumonia Relative to Other Sources of Sepsis. Free Radic. Biol. Med. 2022, 179, 208–212. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Chiu, C.-T.; Lee, H.-S.; Lai, C.-C. The Impact of Vitamin C-Containing Treatment on the Mortality of Patients with Sepsis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Infect. Public Health 2022, 15, 1514–1520. [Google Scholar] [CrossRef]
- Tariq, M.A.; Amin, H.; Ali, U. Meta-Analysis Assessing the Effectiveness of Intravenous Vitamin C in Patients with Sepsis and Septic Shock. Acute Crit. Care 2022, 37, 674–677. [Google Scholar] [CrossRef]
- Berger, M.M. Vitamin C Requirements in Parenteral Nutrition. Gastroenterology 2009, 137, S70–S78. [Google Scholar] [CrossRef]
- May, J.M.; Harrison, F.E. Role of Vitamin C in the Function of the Vascular Endothelium. Antioxid. Redox Signal. 2013, 19, 2068–2083. [Google Scholar] [CrossRef]
- Oliva, A.; Bianchi, A.; Russo, A.; Ceccarelli, G.; Cancelli, F.; Aloj, F.; Alunni Fegatelli, D.; Mastroianni, C.M.; Venditti, M. Effect of N-Acetylcysteine Administration on 30-Day Mortality in Critically Ill Patients with Septic Shock Caused by Carbapenem-Resistant Klebsiella Pneumoniae and Acinetobacter Baumannii: A Retrospective Case-Control Study. Antibiotics 2021, 10, 271. [Google Scholar] [CrossRef]
- Hsu, B.-G.; Lee, R.-P.; Yang, F.-L.; Harn, H.-J.; Chen, H.I. Post-Treatment with N-Acetylcysteine Ameliorates Endotoxin Shock-Induced Organ Damage in Conscious Rats. Life Sci. 2006, 79, 2010–2016. [Google Scholar] [CrossRef] [PubMed]
- Zafarullah, M.; Li, W.Q.; Sylvester, J.; Ahmad, M. Molecular Mechanisms of N -Acetylcysteine Actions. Cell. Mol. Life Sci. 2003, 60, 6–20. [Google Scholar] [CrossRef]
- Taher, A.; Shokoohmand, F.; Abdoli, E.; Mohammadi, Y.; Mehrpooya, M. A Pilot Study on the Melatonin Treatment in Patients with Early Septic Shock: Results of a Single-Center Randomized Controlled Trial. Irish. J. Med. Sci. 2022, 191, 1913–1924. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Luo, X.; Li, J.; Lei, Y.; Zeng, F.; Huang, X.; Lan, Y.; Yang, F. Melatonin: A Window into the Organ-Protective Effects of Sepsis. Biomed. Pharmacother. 2022, 154, 113556. [Google Scholar] [CrossRef]
- Aydogan, S.; Yerer, M.B.; Goktas, A. Melatonin and Nitric Oxide. J. Endocrinol. Investig. 2006, 29, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.-X.; Manchester, L.C.; Reiter, R.J.; Qi, W.-B.; Karbownik, M.; Calvo, J.R. Significance of Melatonin in Antioxidative Defense System: Reactions and Products. Neurosignals 2000, 9, 137–159. [Google Scholar] [CrossRef] [PubMed]
- Urata, Y.; Honma, S.; Goto, S.; Todoroki, S.; Iida, T.; Cho, S.; Honma, K.; Kondo, T. Melatonin Induces γ-Glutamylcysteine Synthetase Mediated by Activator Protein-1 in Human Vascular Endothelial Cells. Free Radic. Biol. Med. 1999, 27, 838–847. [Google Scholar] [CrossRef]
- Sewerynek, E.; Melchiorri, D.; Chen, L.; Reiter, R.J. Melatonin Reduces Both Basal and Bacterial Lipopolysaccharide-Induced Lipid Peroxidation in Vitro. Free Radic. Biol. Med. 1995, 19, 903–909. [Google Scholar] [CrossRef]
- Kiefer, P.; Vogt, J.; Radermacher, P. From Mucolytic to Antioxidant and Liver Protection: New Aspects in the Intensive Care Unit Career of N-Acetylcysteine. Crit. Care Med. 2000, 28, 3935–3936. [Google Scholar] [CrossRef]
- Forceville, X.; Mostert, V.; Pierantoni, A.; Vitoux, D.; le Toumelin, P.; Plouvier, E.; Dehoux, M.; Thuillier, F.; Combes, A. Selenoprotein P, Rather than Glutathione Peroxidase, as a Potential Marker of Septic Shock and Related Syndromes. Eur. Surg. Res. 2009, 43, 338–347. [Google Scholar] [CrossRef]
- Manzanares, W.; Langlois, P.L.; Heyland, D.K. Pharmaconutrition with Selenium in Critically Ill Patients. Nutrit. Clin. Pract. 2015, 30, 34–43. [Google Scholar] [CrossRef]
- Forceville, X.; Vitoux, D.; Gauzit, R.; Combes, A.; Lahilaire, P.; Chappuis, P. Selenium, Systemic Immune Response Syndrome, Sepsis, and Outcome in Critically Ill Patients. Crit. Care Med. 1998, 26, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Jacobi, J.; Sindi, A.; Hartog, C.; Reinhart, K.; Kokkoris, S.; Gerlach, H.; Andrews, P.; Drabek, T.; Manzanares, W.; et al. The Effect of Selenium Therapy on Mortality in Patients with Sepsis Syndrome. Crit. Care Med. 2013, 41, 1555–1564. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mateo, G.; Carrillo-Santisteve, P.; Elosua, R.; Guallar, E.; Marrugat, J.; Bleys, J.; Covas, M.-I. Antioxidant Enzyme Activity and Coronary Heart Disease: Meta-Analyses of Observational Studies. Am. J. Epidemiol. 2009, 170, 135–147. [Google Scholar] [CrossRef]
- Bleys, J.; Navas-Acien, A.; Stranges, S.; Menke, A.; Miller, E.R.; Guallar, E. Serum Selenium and Serum Lipids in US Adults. Am. J. Clin. Nutr. 2008, 88, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-S.; Shyu, Y.-C.; Chen, H.-Y.; Lin, L.-M.; Lo, C.-Y.; Yuan, S.-S.; Chen, P.-J. Effect of Parenteral Selenium Supplementation in Critically Ill Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e54431. [Google Scholar] [CrossRef]
- Kong, Z.; Wang, F.; Ji, S.; Deng, X.; Xia, Z. Selenium Supplementation for Sepsis: A Meta-Analysis of Randomized Controlled Trials. Am. J. Emerg. Med. 2013, 31, 1170–1175. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient. JPEN J. Parenter. Enteral. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Allingstrup, M.; Afshari, A. Selenium Supplementation for Critically Ill Adults. Cochrane Database Syst. Rev. 2015, 7, CD003703. [Google Scholar] [CrossRef] [PubMed]
- Landucci, F.; Mancinelli, P.; de Gaudio, A.R.; Virgili, G. Selenium Supplementation in Critically Ill Patients: A Systematic Review and Meta-Analysis. J. Crit. Care 2014, 29, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xie, L.; Song, A.; Zhang, C. Selenium Status and Its Antioxidant Role in Metabolic Diseases. Oxid. Med. Cell. Longev. 2022, 2022, 7009863. [Google Scholar] [CrossRef] [PubMed]
- Ilhan, I.; Asci, H.; Tepebasi, M.Y.; Imeci, O.B.; Sevuk, M.A.; Temel, E.N.; Ozmen, O. Selenium Exerts Protective Effects on Inflammatory Cardiovascular Damage: Molecular Aspects via SIRT1/P53 and Cyt-c/Cas-3 Pathways. Mol. Biol. Rep. 2022, 50, 1627–1637. [Google Scholar] [CrossRef] [PubMed]
- Börner, J.; Zimmermann, T.; Albrecht, S.; Roesner, D. Selensubstitution Bei Schweren Entzündlichen Chirurgischen Krankheitsbildern Sowie Verbrennungen Und Verbrühungen Im Kindesalter. Med. Klin. 1997, 92, 17–19. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Vit C n = 25 | Vit E n = 27 | NAC n = 24 | MT n = 26 | Without Tx n = 29 | p |
|---|---|---|---|---|---|---|
| Age, years Median (range) | 62 (58–78) | 70 (51–77) | 69 (59–78) | 62.5 (58–69) | 75 (65–81) | 0.10 |
| IMC Median (range) | 25 (23–30) | 25 (22.8–29) | 23 (21–26) | 25.(21–28) | 25 (23–28) | 0.41 |
| Men, n and (%) Women, n and (%) | 10 (40) 15 (60) | 17 (63) 10 (37) | 14 (58) 10(42) | 13 (50) 13 (50) | 16 (55) 13 (45) | 0.53 0.56 |
| SAPS II, Mean ± SD | 39.4 ± 14.1 | 45.7 ± 16.3 | 42.4 ± 19.84 | 40.8 ± 16.8 | 47.2 ± 7.1 | 0.60 |
| APACHE II Median (range) | 14 (12–19) | 20 (15–24) | 15.5 (11–21) | 16.5 (10–21) | 17 (15–25) | 0.15 |
| SOFA, Median (range) | 8 (6–9) | 9 (7–11) | 8 (4–10) | 8 (6–9) | 9 (7–11) | 0.42 |
| NUTRIC, Mean ± SD | 4.1 ± 2.2 | 4.8 ± 1.6 | 4.0 ± 1.8 | 3.8 ± 1.7 | 5.1 ± 1.5 | 0.41 |
| Diabetes Mellitus, n and (%) | 7 (28) | 5 (19) | 5 (21) | 6 (23) | 8 (28) | 0.90 |
| Arterial hypertension, n and (%) | 10 (40) | 11 (41) | 12 (50) | 8 (31) | 15 (52) | 0.53 |
| COPD, n and (%) | 1 (4) | 5 (19) | 4 (17) | 2 (8) | 0 (0) | 0.05 |
| Smoking, n and (%) | 17 (68) | 12 (44) | 9 (38) | 15 (58) | 14 (48) | 0.22 |
| Cancer, n and (%) | 6(24) | 11 (41) | 8 (33) | 8 (31) | 14 (48) | 0.39 |
| Cirrhosis, n and (%) | 2 (8) | 2 (7) | 1 (4) | 1 (4) | 4 (14) | 0.71 |
| Chronic kidney disease, n and (%) | 2 (8) | 3 (11) | 4 (17) | 3 (12) | 3 (10) | 0.92 |
| Hypothyroidism, n and (%) | 4 (16) | 4 (15) | 2 (8) | 6 (23) | 7 (24) | 0.56 |
| CVD, n and (%) | 3 (12) | 0 (0.00) | 1 (4) | 2 (8) | 3 (10) | 0.41 |
| AMI, n and (%) | 1 (4) | 0 (0) | 3 (13) | 2 (8) | 2 (7) | 0.43 |
| Atrial fibrillation, n and (%) | 3 (12) | 2 (7) | 3 (13) | 5 (19) | 4 (14) | 0.79 |
| Pulmonary and CNS | 0 (0) | 0 (0) | 1 (4) | 0 (0) | 0 (0) | 0.20 |
| Admission to the ICU | Vit C n = 25 | Vit E n = 27 | NAC n = 24 | MT n = 26 | Without Tx n = 29 | p |
|---|---|---|---|---|---|---|
| Reason for admission n (%) | ||||||
| Septic shock from surgery | 7 (28) | 6 (22) | 5 (21) | 4 (15 | 13 (14) | 0.14 |
| Septic shock from non-surgical | 18 (72) | 21 (78) | 19 (79) | 22 (84) | 16 (55) | |
| Infection site n (%) | ||||||
| Pulmonary | 7 (29) | 11 (41) | 9 (39) | 11 (42) | 10 (34) | 0.83 |
| Gastrointestinal | 10 (42) | 8 (30) | 5 (22) | 5 (19) | 11 (38) | |
| Nephro-Urinary | 3 (13) | 3 (11) | 6 (26) | 6 (23) | 3 (10) | |
| CNS | 0 (0) | 2 (7) | 0 (0) | 0 (0) | 1 (3) | |
| Skin and soft tissues | 2 (8) | 2 (7) | 2 (9) | 2 (8) | 2 (7) | |
| Endocarditis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (3) | |
| Gastrointestinal-Urinary | 0 (0) | 1 (4) | 0 (0) | 2 (8) | 1 (3) | |
| Pulmonary-CNS | 0 (0) | 0 (0) | 1 (4) | 0 (0) | 0 (0) | |
| Pulmonary-Gastrointestinal | 1 (4) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Variables median (min-max ranges) | ||||||
| Temperature | 36 (36–37) | 36 (36–37) | 36 (36–37) | 37 (36–37) | 36 (36–37) | 0.34 |
| Cardiac Frequency | 83 (68–94) | 85 (66–108) | 86 (66–97) | 86 (67–100) | 83 (74–104) | 0.98 |
| PVC, mmHg | 11.5 (6.5–14) | 9 (6–12) | 12 (7–13) | 9 (7–13) | 13 (9–17) | 0.15 |
| MAP, mmHg | 73 (63–83) | 77 (73–81) | 78 (68.5–85) | 73 (65–81) | 78 (65–82) | 0.52 |
| Minime MAP, mmHg | 63 (54–72) | 68 (61–75) | 63 (55–68) | 61 (55–72) | 61 (54–68) | 0.11 |
| PaO2/FiO2, mmHg | 196 (129–309) | 240 (120–266) | 239 (141–300) | 197 (115–242) | 190 (150–250 | 0.93 |
| Lactate, mmol/L | 1.3 (1.09–2.4) | 2.4 (1.4–3.7) | 2.0 (1.4–3.2) | 2.3 (1.49–4.6) | 2.6 (2.08–4.05) | 0.01 |
| Bilirubins mg/dL | 0.8 (0.42–1.1) | 1.2 (0.6–2.2) | 0.9 (0.46–1.9) | 1.02 (0.5–1.8) | 1.1 (0.7–2.3) | 0.27 |
| Hemoglobin g/dL | 12 (10–14) | 11 (10–15) | 11 (10–11) | 11 (10–13) | 12 (10–14) | 0.21 |
| Leucocytes 103/µL | 11 (8–19) | 10 (7–16) | 9 (8–14) | 13 (10–20) | 14 (7–21) | 0.35 |
| Procalcitonin ng/dI | 1.2 (0.5–30) | 4 (0.5–40) | 1.2 (0.3–10) | 2.8 (1.04–8.4) | 7.6 (1.4–32) | 0.33 |
| C Reactive protein mg/dI | 20 (11–31) | 25 (12–32) | 12 (8–23) | 22 (10–29() | 23 (11–33) | 0.38 |
| Platelets | 241 (186–295) | 166 (82–258) | 161 (110–215) | 245 (161–443) | 212 (131–297) | 0.01 |
| Inotropic type (n and %) | ||||||
| Steroid treatment | 6 (24.00) | 16 (59.26) | 9 (37.50) | 8 (30.77) | 14 (48.28) | 0.07 |
| Enteral, nutrition | 21 (87.50) | 23 (85.19) | 21 (87.50) | 24 (96.00) | 23 (79.31) | 0.50 |
| Parenteral nutrition | 4 (16.67) | 7 (25.93) | 7 (29.17) | 5 (20.00) | 9 (31.03) | 0.73 |
| Inotropic | 2 (8.33) | 7 (25.93) | 3 (12.50) | 5 (19.23) | 10 (34.48) | 0.14 |
| Dobutamine | 1 (4.17) | 1 (3.70) | 0 (0.00) | 0 (0.00) | 1 (3.45) | |
| Levosimendan | 0 (0.00) | 6 (22.22) | 2 (8.33) | 4 (15.38) | 8 (27.59) | 0.06 |
| Dopamine | 1 (4.17) | 0 (0.00) | 0 (0.00) | 1 (3.85) | 0 (0.00) | |
| Vasopressor type (n and %) | ||||||
| Norepinephrine Vasopressin, Norepinephrine + Vasopressin, | 16 (67) 0 (0) 8 (33) | 11 (41) 1 (4) 15 (56) | 16 (67) 0 (0) 16 (70) | 13 (50) 0 (0) 16 (62) | 17 (59) 0 (0) 23 (79) | 0.26 |
| Other treatments | ||||||
| Antifungal | 6 (25.00) | 6 (22.22) | 7 (29.17) | 6 (23.08) | 11 (37.93) | 0.70 |
| RTT | 1 (4.17) | 3 (11.11) | 2 (8.33) | 1 (3.85) | 3 (10.34) | 0.80 |
| Mechanic ventilation | 13 (54.17) | 15 (55.56) | 16 (69.57) | 16 (61.54) | 23 (79.31) | 0.26 |
| IMV | 12 (50) 1 (4) | 12 (44) 4 (15) | 11 (48) 5(22) | 10 (38) 5(19) | 19 (66) 2 (7) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aisa-Álvarez, A.; Pérez-Torres, I.; Guarner-Lans, V.; Manzano-Pech, L.; Cruz-Soto, R.; Márquez-Velasco, R.; Casarez-Alvarado, S.; Franco-Granillo, J.; Núñez-Martínez, M.E.; Soto, M.E. Randomized Clinical Trial of Antioxidant Therapy Patients with Septic Shock and Organ Dysfunction in the ICU: SOFA Score Reduction by Improvement of the Enzymatic and Non-Enzymatic Antioxidant System. Cells 2023, 12, 1330. https://doi.org/10.3390/cells12091330
Aisa-Álvarez A, Pérez-Torres I, Guarner-Lans V, Manzano-Pech L, Cruz-Soto R, Márquez-Velasco R, Casarez-Alvarado S, Franco-Granillo J, Núñez-Martínez ME, Soto ME. Randomized Clinical Trial of Antioxidant Therapy Patients with Septic Shock and Organ Dysfunction in the ICU: SOFA Score Reduction by Improvement of the Enzymatic and Non-Enzymatic Antioxidant System. Cells. 2023; 12(9):1330. https://doi.org/10.3390/cells12091330
Chicago/Turabian StyleAisa-Álvarez, Alfredo, Israel Pérez-Torres, Verónica Guarner-Lans, Linaloe Manzano-Pech, Randall Cruz-Soto, Ricardo Márquez-Velasco, Sergio Casarez-Alvarado, Juvenal Franco-Granillo, Marcela Elizabeth Núñez-Martínez, and María Elena Soto. 2023. "Randomized Clinical Trial of Antioxidant Therapy Patients with Septic Shock and Organ Dysfunction in the ICU: SOFA Score Reduction by Improvement of the Enzymatic and Non-Enzymatic Antioxidant System" Cells 12, no. 9: 1330. https://doi.org/10.3390/cells12091330