
Central Auditory Functions of Alzheimer’s Disease and Its Preclinical Stages: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
3. Results
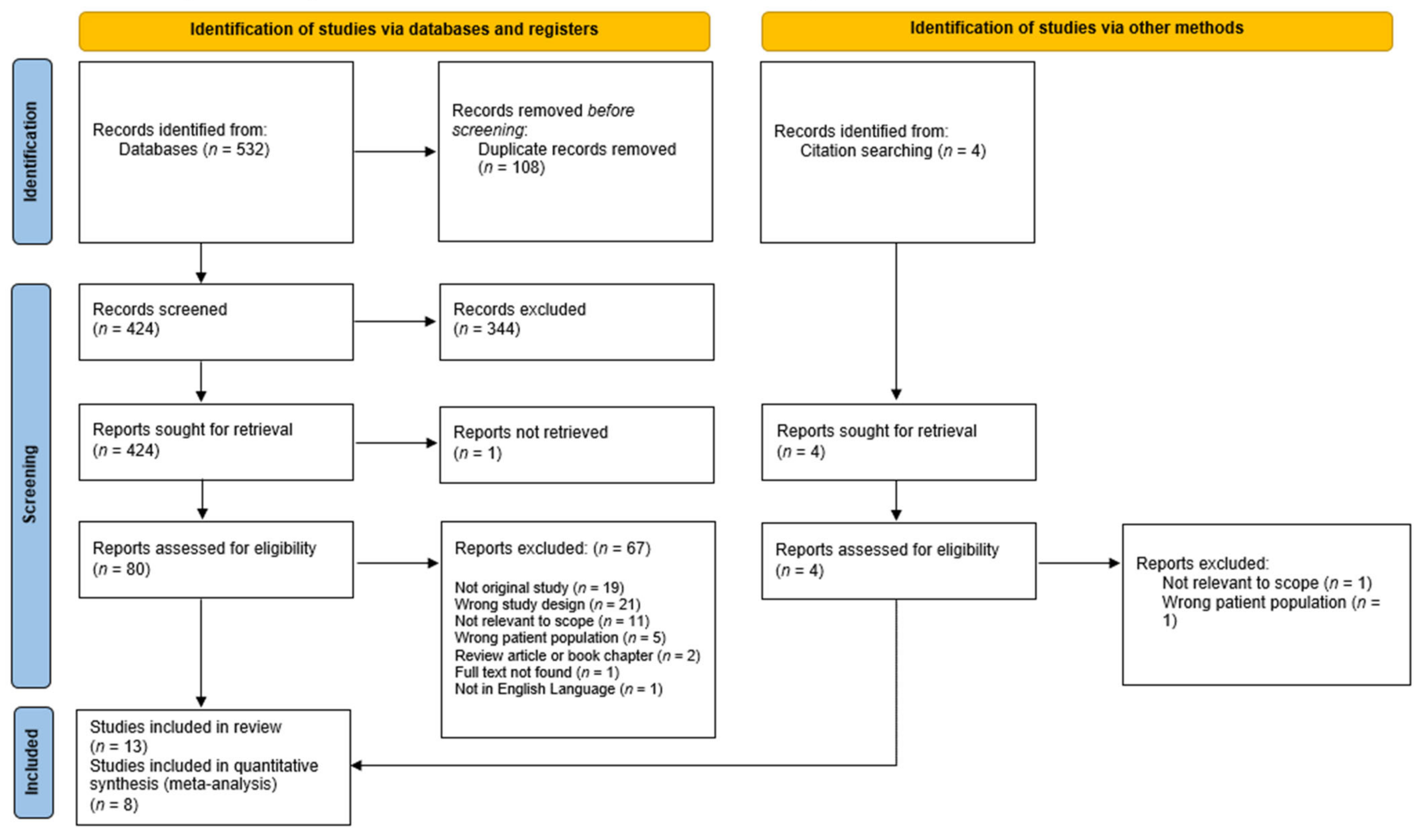
3.1. Search Results
3.2. Study Characteristics
3.3. Quantitative Analysis
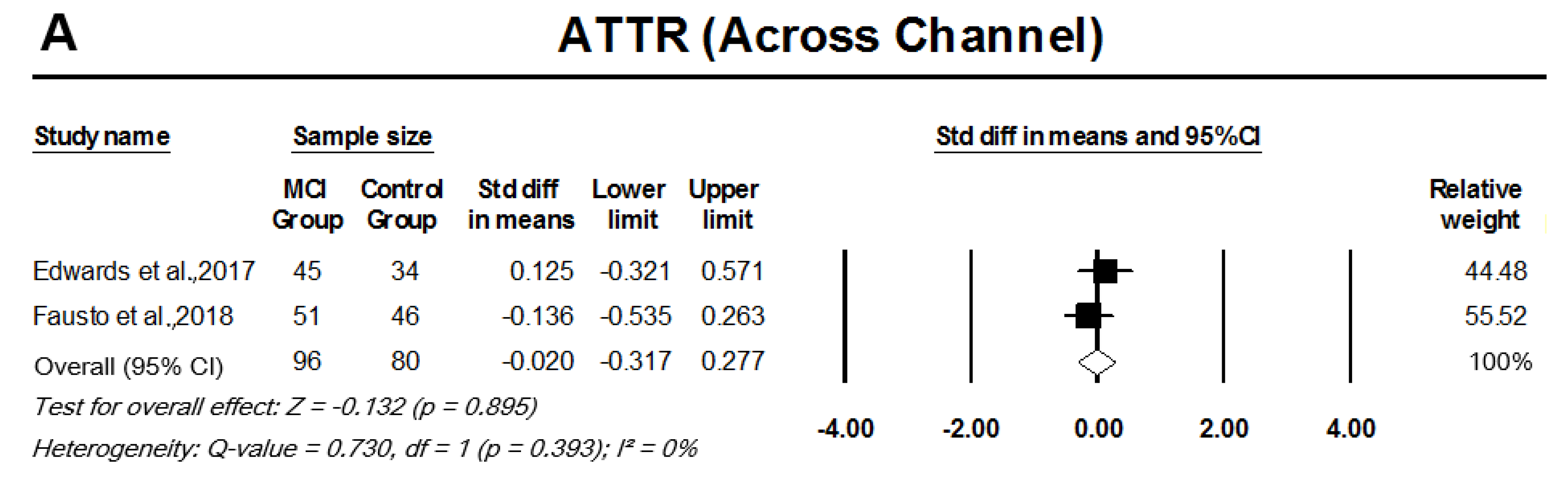
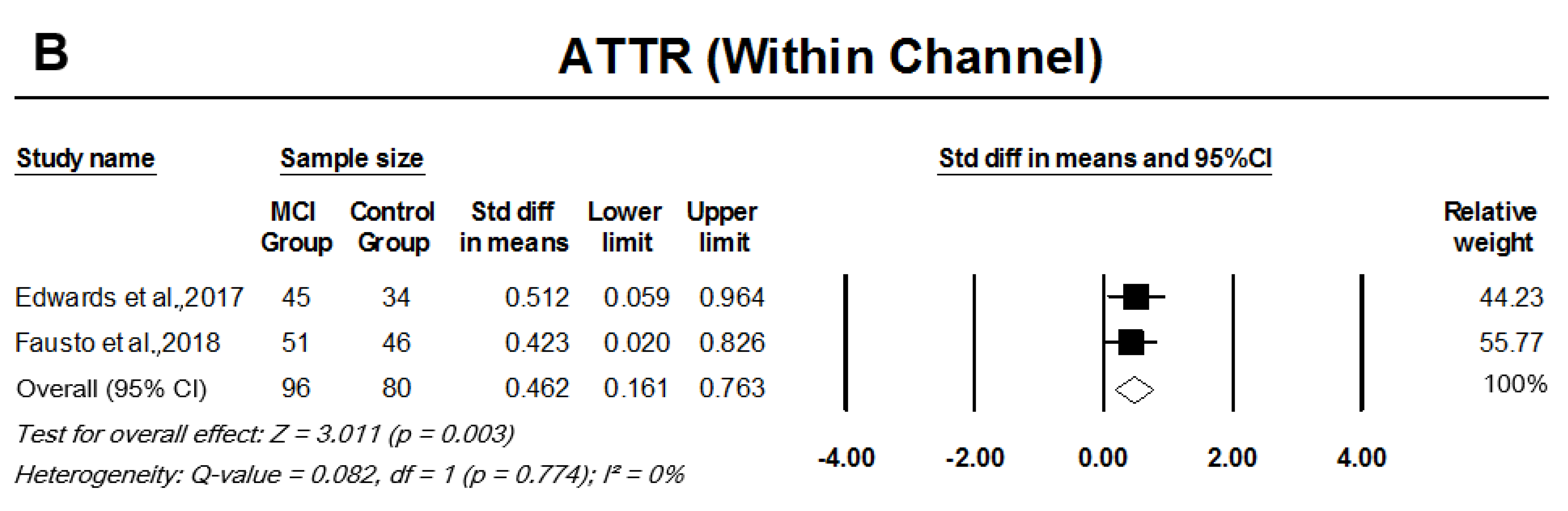
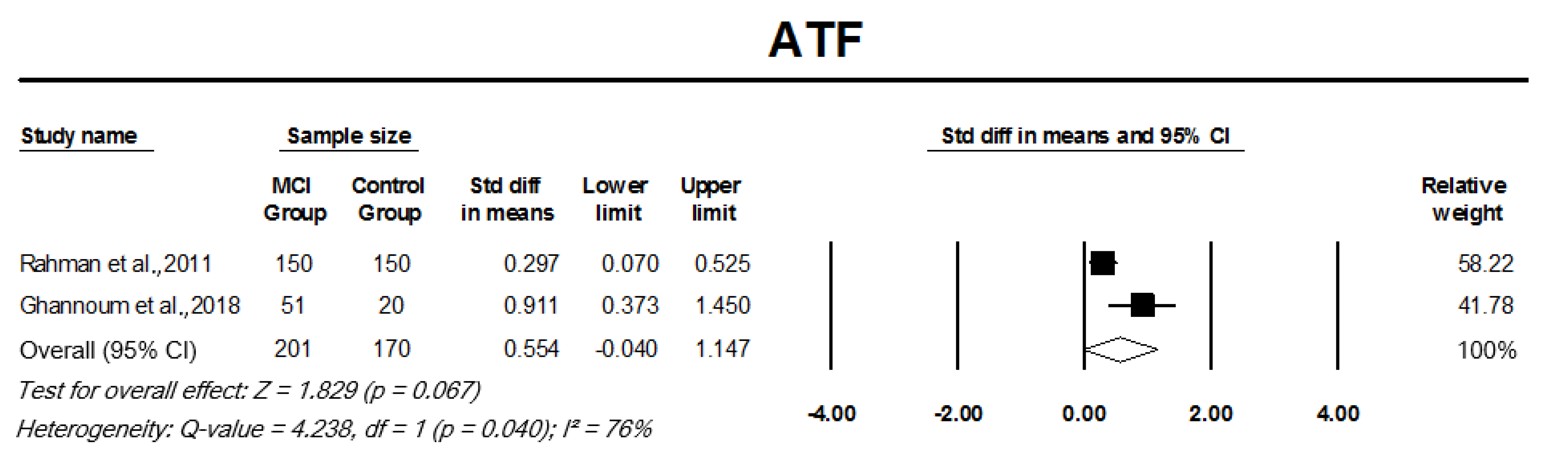
3.3.1. Auditory Temporal Processing Tests
3.3.2. Dichotic Tests/Binaural Interaction Tests
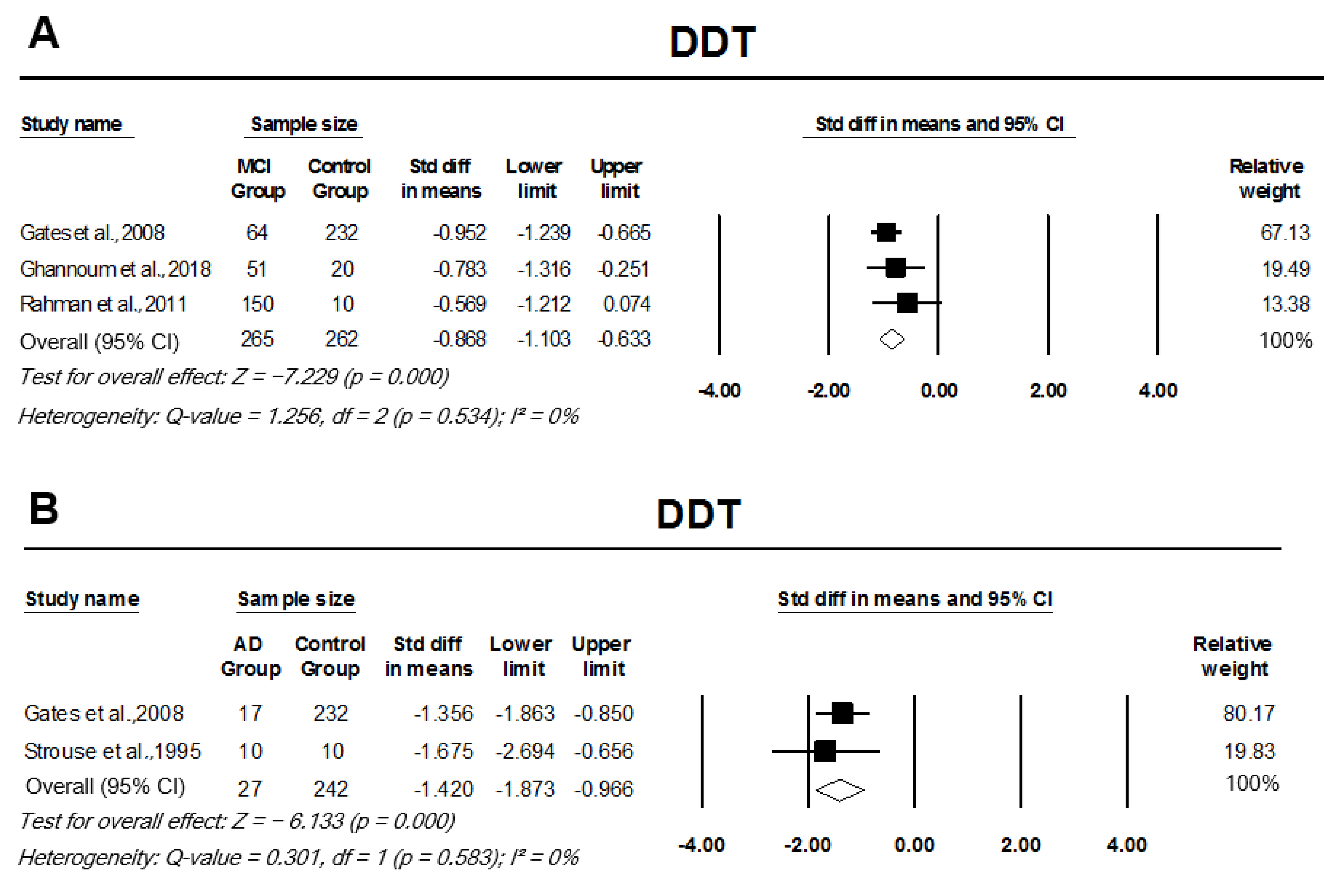
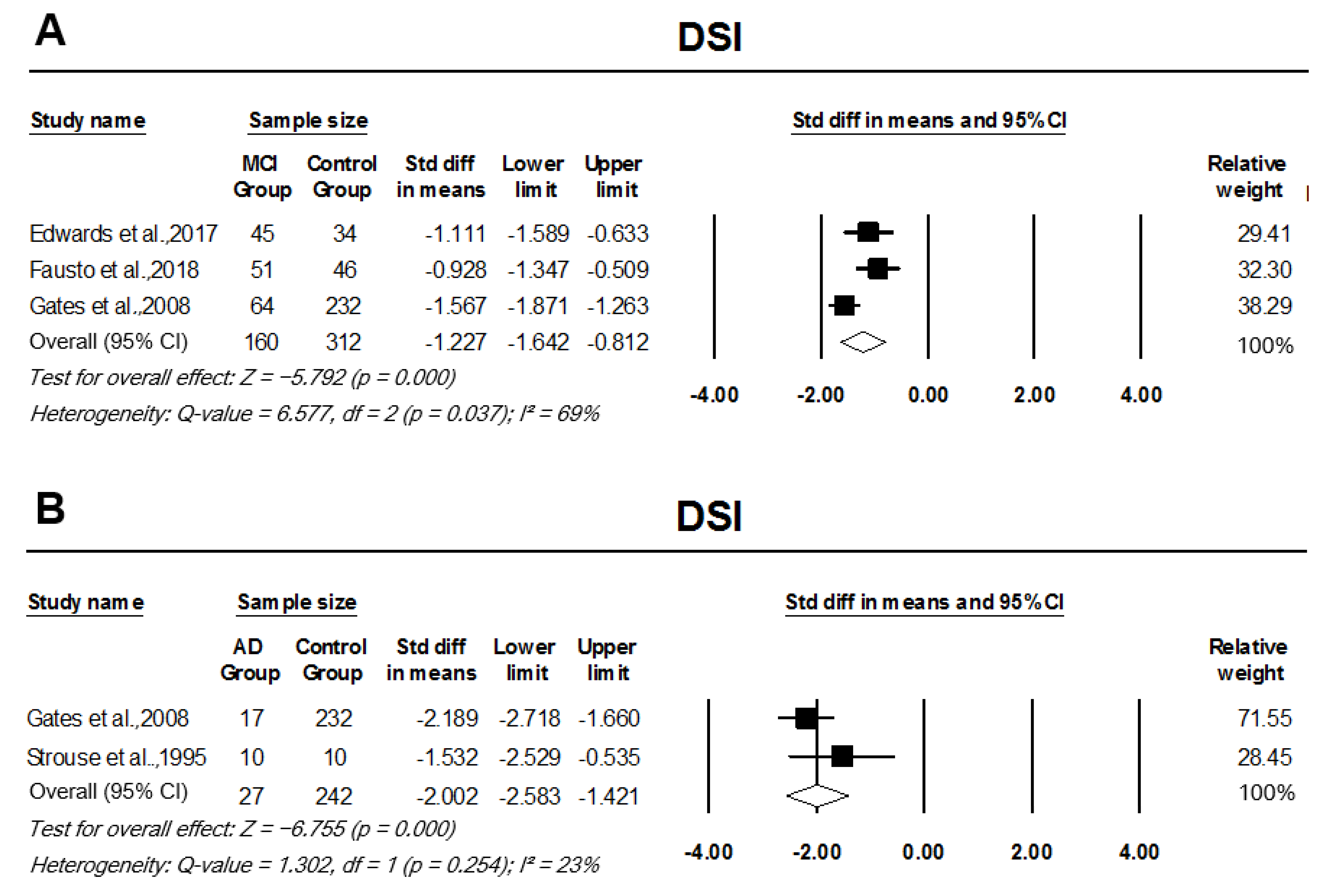
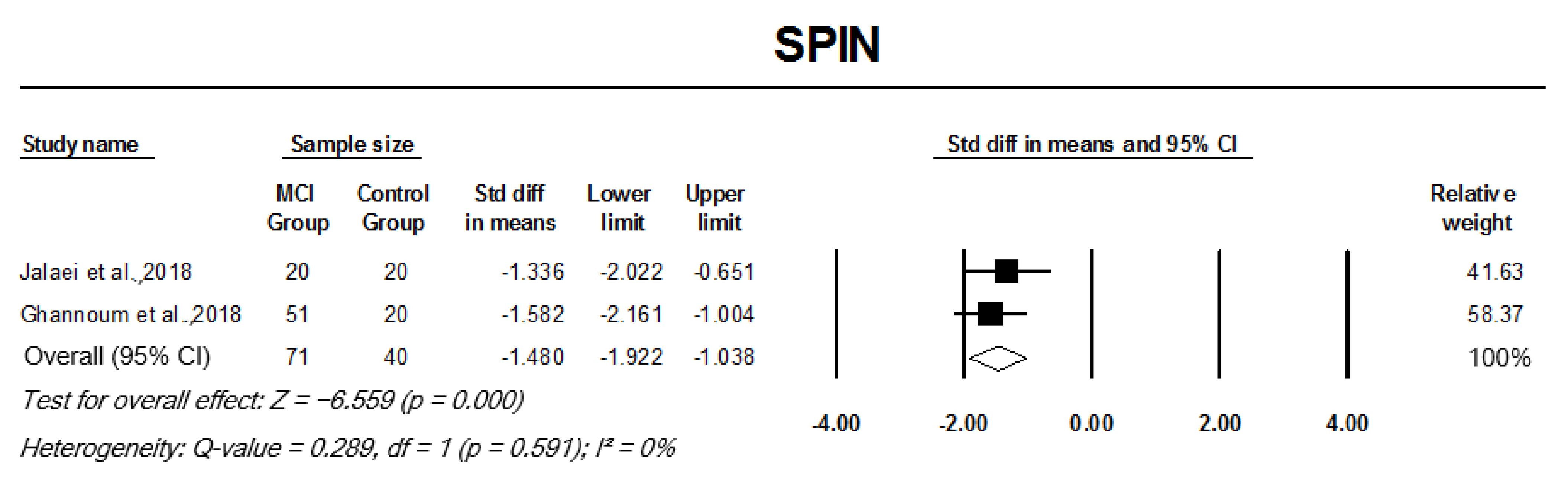
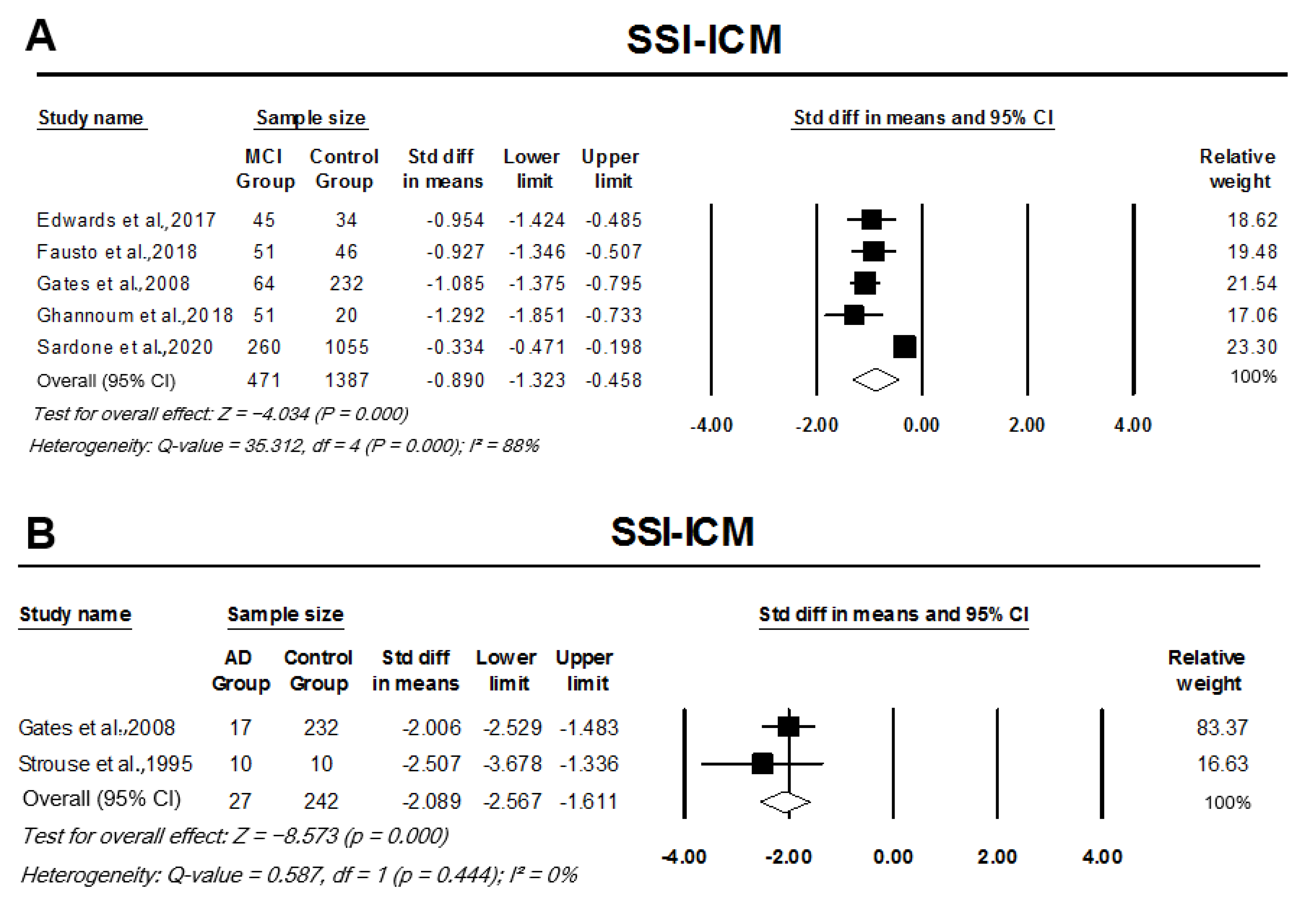
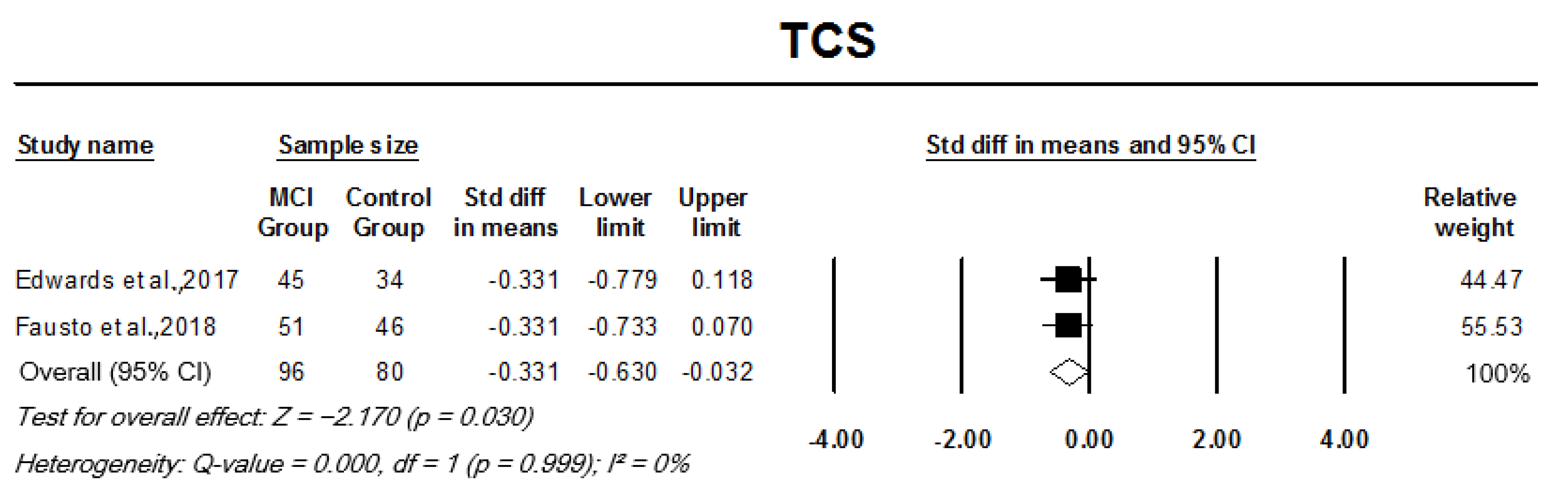
3.3.3. Monaural Low-Redundancy Speech Tests
3.4. Quality Assessment
4. Discussion
4.1. Auditory Temporal Processing in MCI and AD
4.2. Dichotic Tests/Binaural Interaction in MCI and AD
4.3. Monaural Low-Redundancy Speech in MCI and AD
4.4. Auditory Memory and Discrimination in MCI and AD
4.5. Clinical Limitations of the CAP Testing
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Alzheimer’s Association. Alzheimer’s disease facts and figures. Alzheimers Dement. 2020, 16, 391–460. [Google Scholar] [CrossRef]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. J. Alzheimers Assoc. 2013, 9, 63–75.e2. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Purves, D.; Augustine, G.; Fitzpatrick, D.; Hall, W.; LaMantia, A.S.; White, L. Neuroscience, 5th ed.; Mooney, R., Platt, M., Eds.; Sinauer Associates: Sunderland, MA, USA, 2012; p. 15. [Google Scholar]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Lin, F.R.; Metter, E.J.; O’Brien, R.J.; Resnick, S.M.; Zonderman, A.B.; Ferrucci, L. Hearing loss and incident dementia. Arch. Neurol. 2011, 68, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Jayakody, D.M.P.; Friedland, P.L.; Martins, R.N.; Sohrabi, H.R. Impact of Aging on the Auditory System and Related Cognitive Functions: A Narrative Review. Front. Neurosci. 2018, 12, 125. [Google Scholar] [CrossRef]
- Jayakody, D.M.P.; Menegola, H.K.; Yiannos, J.M.; Goodman-Simpson, J.; Friedland, P.L.; Taddei, K.; Laws, S.M.; Weinborn, M.; Martins, R.N.; Sohrabi, H.R. The Peripheral Hearing and Central Auditory Processing Skills of Individuals with Subjective Memory Complaints. Front. Neurosci. 2020, 14, 888. [Google Scholar] [CrossRef]
- Runge, C.L.; Friedland, D.R. 127—Neuroanatomy of the Auditory System. In Cummings Otolaryngology Head and Neck Surgery, 7th ed.; Flint, P.W., Francis, H.W., Haughey, B.H., Lesperance, M.M., Lund, V.J., Robbins, K.T., Thomas, J.R., Eds.; Elsevier, Inc.: Philadelphia, PA, USA, 2021; pp. 1938–1944. [Google Scholar]
- Eggermont, J.J.; Wang, X. Temporal Coding in Auditory Cortex. In The Auditory Cortex, 1st ed.; Winer, J.A., Schreiner, C.E., Eds.; Springer: New York, NY, USA, 2011. [Google Scholar]
- King, A.J.; Middlebrooks, J.C. Cortical Representation of Auditory Space. In The Auditory Cortex, 1st ed.; Winer, J.A., Schreiner, C.E., Eds.; Springer: New York, NY, USA, 2011. [Google Scholar]
- Bregman, A.S. Auditory Scene Analysis: The Perceptual Organization of Sound; MIT Press: Cambridge, MA, USA, 1990. [Google Scholar]
- Kraus, K.S.; Canlon, B. Neuronal connectivity and interactions between the auditory and limbic systems. Effects of noise and tinnitus. Hear. Res. 2012, 288, 34–46. [Google Scholar] [CrossRef]
- Kanwal, J.S.; Ehret, G. Communication Sounds and their Cortical Representation. In The Auditory Cortex, 1st ed.; Winer, J.A., Schreiner, C.E., Eds.; Springer: New York, NY, USA, 2011. [Google Scholar]
- Ardila, A.; Bernal, B.; Rosselli, M. The role of Wernicke’s area in language comprehension. Psychol. Neurosci. 2016, 9, 340–343. [Google Scholar] [CrossRef]
- Turkeltaub, P.E.; Coslett, H.B. Localization of sublexical speech perception components. Brain Lang. 2010, 114, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Musiek, F.E. Handbook of Central Auditory Processing Disorder Volume 1: Auditory Neuroscience and Diagnosis, 2nd ed.; Plural Publishing, Inc.: San Diego, CA, USA, 2013; Volume 1. [Google Scholar]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Dekosky, S.T.; Barberger-Gateau, P.; Cummings, J.; Delacourte, A.; Galasko, D.; Gauthier, S.; Jicha, G.; et al. Research criteria for the diagnosis of Alzheimer’s disease: Revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007, 6, 734–746. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Albert, M.S.; Knopman, D.S.; McKhann, G.M.; Sperling, R.A.; Carrillo, M.C.; Thies, B.; Phelps, C.H. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. J. Alzheimers Assoc. 2011, 7, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Silhan, D.; Bartos, A.; Mrzilkova, J.; Pashkovska, O.; Ibrahim, I.; Tintera, J. The Parietal Atrophy Score on Brain Magnetic Resonance Imaging is a Reliable Visual Scale. Curr. Alzheimer Res. 2020, 17, 534–539. [Google Scholar] [CrossRef]
- Du, A.T.; Schuff, N.; Kramer, J.H.; Ganzer, S.; Zhu, X.P.; Jagust, W.J.; Miller, B.L.; Reed, B.R.; Mungas, D.; Yaffe, K.; et al. Higher atrophy rate of entorhinal cortex than hippocampus in AD. Neurology 2004, 62, 422–427. [Google Scholar] [CrossRef]
- Pennanen, C.; Kivipelto, M.; Tuomainen, S.; Hartikainen, P.; Hänninen, T.; Laakso, M.P.; Hallikainen, M.; Vanhanen, M.; Nissinen, A.; Helkala, E.L.; et al. Hippocampus and entorhinal cortex in mild cognitive impairment and early AD. Neurobiol. Aging 2004, 25, 303–310. [Google Scholar] [CrossRef]
- Li, X.; Coyle, D.; Maguire, L.; Watson, D.R.; McGinnity, T.M. Gray matter concentration and effective connectivity changes in Alzheimer’s disease: A longitudinal structural MRI study. Neuroradiology 2011, 53, 733–748. [Google Scholar] [CrossRef]
- Ten Kate, M.; Barkhof, F.; Boccardi, M.; Visser, P.J.; Jack, C.R., Jr.; Lovblad, K.O.; Frisoni, G.B.; Scheltens, P. Clinical validity of medial temporal atrophy as a biomarker for Alzheimer’s disease in the context of a structured 5-phase development framework. Neurobiol. Aging 2017, 52, 167–182.e1. [Google Scholar] [CrossRef] [Green Version]
- Barber, R.; Gholkar, A.; Scheltens, P.; Ballard, C.; McKeith, I.G.; O’Brien, J.T. Medial temporal lobe atrophy on MRI in dementia with Lewy bodies. Neurology 1999, 52, 1153–1158. [Google Scholar] [CrossRef]
- Nesteruk, M.; Nesteruk, T.; Styczyńska, M.; Barczak, A.; Mandecka, M.; Walecki, J.; Barcikowska-Kotowicz, M. Predicting the conversion of mild cognitive impairment to Alzheimer’s disease based on the volumetric measurements of the selected brain structures in magnetic resonance imaging. Neurol. Neurochir. Pol. 2015, 49, 349–353. [Google Scholar] [CrossRef]
- Koedam, E.L.G.E.; Lehmann, M.; van der Flier, W.M.; Scheltens, P.; Pijnenburg, Y.A.L.; Fox, N.; Barkhof, F.; Wattjes, M.P. Visual assessment of posterior atrophy development of a MRI rating scale. Eur. Radiol. 2011, 21, 2618–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates, G.A.; Anderson, M.L.; McCurry, S.M.; Feeney, M.P.; Larson, E.B. Central auditory dysfunction as a harbinger of Alzheimer dementia. Arch. Otolaryngol.-Head Neck Surg. 2011, 137, 390–395. [Google Scholar] [CrossRef] [Green Version]
- Rönnberg, J.; Lunner, T.; Zekveld, A.; Sörqvist, P.; Danielsson, H.; Lyxell, B.; Dahlström, Ö.; Signoret, C.; Stenfelt, S.; Pichora-Fuller, K.; et al. The Ease of Language Understanding (ELU) model: Theoretical, empirical, and clinical advances. Front. Syst. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. World Report on Hearing; 978-92-4-002048-1; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Jayakody, D.M.P.; Friedland, P.L.; Eikelboom, R.H.; Martins, R.N.; Sohrabi, H.R. A novel study on association between untreated hearing loss and cognitive functions of older adults: Baseline non-verbal cognitive assessment results. Clin. Otolaryngol. 2017, 43, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Deal, J.A.; Betz, J.; Yaffe, K.; Harris, T.; Purchase-Helzner, E.; Satterfield, S.; Pratt, S.; Govil, N.; Simonsick, E.M.; Lin, F.R. Hearing Impairment and Incident Dementia and Cognitive Decline in Older Adults: The Health ABC Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 72, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Ferrucci, L.; Metter, E.J.; An, Y.; Zonderman, A.B.; Resnick, S.M. Hearing Loss and Cognition in the Baltimore Longitudinal Study of Aging. Neuropsychology 2011, 25, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates, G.A.; Anderson, M.L.; Feeney, M.P.; McCurry, S.M.; Larson, E.B. Central auditory dysfunction in older persons with memory impairment or alzheimer dementia. Arch. Otolaryngol.-Head Neck Surg. 2008, 134, 771–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates, G.A.; Beiser, A.; Rees, T.S.; D’ Agostino, R.B.; Wolf, P.A. Central Auditory Dysfunction May Precede the Onset of Clinical Dementia in People with Probable Alzheimer’s Disease. J. Am. Geriatr. Soc. 2002, 50, 482–488. [Google Scholar] [CrossRef]
- Panza, F.; Lozupone, M.; Sardone, R.; Battista, P.; Piccininni, M.; Dibello, V.; La Montagna, M.; Stallone, R.; Venezia, P.; Liguori, A.; et al. Sensorial frailty: Age-related hearing loss and the risk of cognitive impairment and dementia in later life. Ther. Adv. Chronic Dis. 2019, 10, 2040622318811000. [Google Scholar] [CrossRef]
- Yuan, J.; Sun, Y.; Sang, S.; Pham, J.H.; Kong, W.-J. The risk of cognitive impairment associated with hearing function in older adults: A pooled analysis of data from eleven studies. Sci. Rep. 2018, 8, 2137. [Google Scholar] [CrossRef] [Green Version]
- Panza, F.; Quaranta, N.; Logroscino, G. Sensory changes and the hearing loss–cognition link: The cognitive ear. JAMA Otolaryngol.-Head Neck Surg. 2018, 144, 127–128. [Google Scholar] [CrossRef]
- Sardone, R.; Battista, P.; Panza, F.; Lozupone, M.; Griseta, C.; Castellana, F.; Capozzo, R.; Ruccia, M.; Resta, E.; Seripa, D. The Age-Related Central Auditory Processing Disorder: Silent Impairment of the Cognitive Ear. Front. Neurosci. 2019, 13, 619. [Google Scholar] [CrossRef]
- Scahill, R.I.; Frost, C.; Jenkins, R.; Whitwell, J.L.; Rossor, M.N.; Fox, N.C. A longitudinal study of brain volume changes in normal aging using serial registered magnetic resonance imaging. Arch. Neurol. 2003, 60, 989. [Google Scholar] [CrossRef] [Green Version]
- Raz, N.; Rodrigue, K.M.; Head, D.; Kennedy, K.M.; Acker, J.D. Differential aging of the medial temporal lobe: A study of a five-year change. Neurology 2004, 62, 433–438. [Google Scholar] [CrossRef]
- Raz, N.; Gunning, F.M.; Head, D.; Dupuis, J.H.; McQuain, J.; Briggs, S.D.; Loken, W.J.; Thornton, A.E.; Acker, J.D. Selective aging of the human cerebral cortex observed in vivo: Differential vulnerability of the prefrontal gray matter. Cereb. Cortex 1997, 7, 268–282. [Google Scholar] [CrossRef] [Green Version]
- Hedman, A.M.; Van Haren, N.E.M.; Schnack, H.G.; Kahn, R.S.; Hulshoff Pol, H.E. Human brain changes across the life span: A review of 56 longitudinal magnetic resonance imaging studies. Hum. Brain Mapp. 2012, 33, 1987–2002. [Google Scholar] [CrossRef]
- Lin, F.R.; Ferrucci, L.; An, Y.; Goh, J.O.; Doshi, J.; Metter, E.J.; Davatzikos, C.; Kraut, M.A.; Resnick, S.M. Association of hearing impairment with brain volume changes in older adults. NeuroImage 2014, 90, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Husain, F.T.; Medina, R.E.; Davis, C.W.; Szymko-Bennett, Y.; Simonyan, K.; Pajor, N.M.; Horwitz, B. Neuroanatomical changes due to hearing loss and chronic tinnitus: A combined VBM and DTI study. Brain Res. 2011, 1369, 74–88. [Google Scholar] [CrossRef] [Green Version]
- Eckert, M.; Cute, S.; Vaden, K.; Kuchinsky, S.; Dubno, J. Auditory Cortex Signs of Age-Related Hearing Loss. J. Assoc. Res. Otolaryngol. 2012, 13, 703–713. [Google Scholar] [CrossRef] [Green Version]
- Peelle, J.E.; Troiani, V.; Grossman, M.; Wingfield, A. Hearing Loss in Older Adults Affects Neural Systems Supporting Speech Comprehension. J. Neurosci. 2011, 31, 12638–12643. [Google Scholar] [CrossRef]
- Jayakody, D.M.P.; Tarawneh, H.Y.; Menegola, H.K.; Yiannos, J.M.; Friedland, P.L.; Wilson, W.J.; Martins, R.N.; Sohrabi, H.R. Systematic review protocol for assessing central auditory functions of Alzheimer’s disease and its preclinical stages. BMJ Open 2020, 10, e033342. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 148–160. [Google Scholar] [CrossRef] [Green Version]
- Amaral, M.I.R.; Casali, R.L.; Boscariol, M.; Lunardi, L.L.; Guerreiro, M.M.; Colella-Santos, M.F. Temporal Auditory Processing and Phonological Awareness in Children with Benign Epilepsy with Centrotemporal Spikes. BioMed Res. Int. 2015, 2015, 256340–256349. [Google Scholar] [CrossRef] [PubMed]
- Schochat, E.; Rabelo, C.; Sanfins, M. Central auditory processing: Pitch and duration patterns in normal hearing subjects from 7 to 16 years old. Atualizaçao Cient. 2000, 12, 1–7. [Google Scholar]
- Bellis, T.J. Assessment and Management of Central Auditory Processing Disorders in the Educational Setting: From Science to Practice; Plural Publishing: San Diego, CA, USA, 2011. [Google Scholar]
- Humes, L.E.; Dubno, J.R. Factors affecting speech understanding in older adults. In The Aging Auditory System; Springer: New York, NY, USA, 2010; pp. 211–257. [Google Scholar]
- Gordon-Salant, S.; Fitzgibbons, P.J. Profile of Auditory Temporal Processing in Older Listeners. J. Speech Lang. Hear. Res. 1999, 42, 300–311. [Google Scholar] [CrossRef] [PubMed]
- Lister, J.J.; Maxfield, N.D.; Pitt, G.J.; Gonzalez, V.B. Auditory evoked response to gaps in noise: Older adults. Int. J. Audiol. 2011, 50, 211–225. [Google Scholar] [CrossRef] [Green Version]
- Gootjes, L.; Bouma, A.; Van Strien, J.W.; Scheltens, P.; Stam, C.J. Attention modulates hemispheric differences in functional connectivity: Evidence from MEG recordings. Neuroimage 2006, 30, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Lipschutz, B.; Kolinsky, R.; Damhaut, P.; Wikler, D.; Goldman, S. Attention-Dependent Changes of Activation and Connectivity in Dichotic Listening. Neuroimage 2002, 17, 643–656. [Google Scholar] [CrossRef]
- Thomsen, T.; Specht, K.; Hammar, Å.; Nyttingnes, J.; Ersland, L.; Hugdahl, K. Brain localization of attentional control in different age groups by combining functional and structural MRI. Neuroimage 2004, 22, 912–919. [Google Scholar] [CrossRef]
- Bouma, A.; Gootjes, L. Effects of attention on dichotic listening in elderly and patients with dementia of the Alzheimer type. Brain Cogn. 2011, 76, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Grady, C.L.; Grimes, A.M.; Patronas, N.; Sunderland, T.; Foster, N.L.; Rapoport, S.I. Divided attention, as measured by dichotic speech performance, in dementia of the Alzheimer type. Arch. Neurol. 1989, 46, 317–320. [Google Scholar] [CrossRef]
- Grimes, A.M.; Grady, C.L.; Foster, N.L.; Sunderland, T.; Patronas, N.J. Central auditory function in Alzheimer’s disease. Neurology 1985, 35, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Tuwaig, M.; Savard, M.; Jutras, B.; Poirier, J.; Collins, D.L.; Rosa-Neto, P.; Fontaine, D.; Breitner, J.C.S. Deficit in Central Auditory Processing as a Biomarker of Pre-Clinical Alzheimer’s Disease. J. Alzheimers Dis. 2017, 60, 1589–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickerson, B.C.; Feczko, E.; Augustinack, J.C.; Pacheco, J.; Morris, J.C.; Fischl, B.; Buckner, R.L. Differential effects of aging and Alzheimer’s disease on medial temporal lobe cortical thickness and surface area. Neurobiol. Aging 2007, 30, 432–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goll, J.C.; Kim, L.G.; Ridgway, G.R.; Hailstone, J.C.; Lehmann, M.; Buckley, A.H.; Crutch, S.J.; Warren, J.D. Impairments of auditory scene analysis in Alzheimer’s disease. Brain 2012, 135, 190–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brun, A.; Englund, E. Regional pattern of degeneration in Alzheimer’s disease: Neuronal loss and histopathological grading. A. Brun & E. Englund. Histopathology 1981; 5; 459–564; reprinted in. Histopathology 2002, 41, 37. [Google Scholar] [CrossRef]
- Ranganath, C.; Johnson, M.K.; D’Esposito, M. Prefrontal activity associated with working memory and episodic long-term memory. Neuropsychologia 2003, 41, 378–389. [Google Scholar] [CrossRef]
- Binetti, G.; Magni, E.; Padovani, A.; Cappa, S.F.; Bianchetti, A.; Trabucchi, M. Executive dysfunction in early Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 1996, 60, 91–93. [Google Scholar] [CrossRef] [Green Version]
- Gootjes, L.; Bouma, A.; Van Strien, J.W.; Schijndel, R.V.; Barkhof, F.; Scheltens, P. Corpus callosum size correlates with asymmetric performance on a dichotic listening task in healthy aging but not in Alzheimer’s disease. Neuropsychologia 2006, 44, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Duke, L.M.; Kaszniak, A.W. Executive Control Functions in Degenerative Dementias: A Comparative Review. Neuropsychol. Rev. 2000, 10, 75–99. [Google Scholar] [CrossRef]
- Rahman, T.T.A.; Mohamed, S.T.; Albanouby, M.H.; Bekhet, H.F. Central auditory processing in elderly with mild cognitive impairment. Geriatr. Gerontol. Int. 2011, 11, 304–308. [Google Scholar] [CrossRef]
- Strouse, A.L.; Hall, J.W.I.; Burger, M.C. Central Auditory Processing in Alzheimer’s Disease. Ear Hear. 1995, 16, 230–238. [Google Scholar] [CrossRef]
- Ghannoum, M.T.; Shalaby, A.A.; Farghaly, M.; Hamdy, M.; Hamdy, H.S. Central auditory processing findings in a group of cognitively impaired individuals. Hear. Balance Commun. 2018, 16, 145–154. [Google Scholar] [CrossRef]
- Jack, J.C.R.; Holtzman, D.M. Biomarker modeling of Alzheimer’s disease. Neuron 2013, 80, 1347–1358. [Google Scholar] [CrossRef] [Green Version]
- Greene, S.J.; Killiany, R.J.; Alzheimer’s Disease Neuroimaging Initiative. Subregions of the inferior parietal lobule are affected in the progression to Alzheimer’s disease. Neurobiol. Aging. 2010, 31, 1304–1311. [Google Scholar] [CrossRef] [Green Version]
- Zatorre, R.J.; Belin, P. Spectral and temporal processing in human auditory cortex. Cereb. Cortex 2001, 11, 946–953. [Google Scholar] [CrossRef]
- Anderson, S.; Skoe, E.; Chandrasekaran, B.; Kraus, N. Neural Timing Is Linked to Speech Perception in Noise. J. Neurosci. 2010, 30, 4922–4926. [Google Scholar] [CrossRef] [Green Version]
- Shinn-Cunningham, B.G.; Best, V. Selective Attention in Normal and Impaired Hearing. Trends Amplif. 2008, 12, 283–299. [Google Scholar] [CrossRef]
- Jane, H.; Erika, S.; Trent, N.; Steven, Z.; Nina, K.; Michael, M.M. Subcortical Differentiation of Stop Consonants Relates to Reading and Speech-in-Noise Perception. Proc. Natl. Acad. Sci. USA 2009, 106, 13022–13027. [Google Scholar] [CrossRef] [Green Version]
- Della Penna, S.; Brancucci, A.; Babiloni, C.; Franciotti, R.; Pizzella, V.; Rossi, D.; Torquati, K.; Rossini, P.M.; Romani, G.L. Lateralization of Dichotic Speech Stimuli is Based on Specific Auditory Pathway Interactions: Neuromagnetic Evidence. Cereb. Cortex 2007, 17, 2303–2311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Zomorrodi, R.; Ghazala, Z.; Goodman, M.S.; Blumberger, D.M.; Cheam, A.; Fischer, C.; Daskalakis, Z.J.; Mulsant, B.H.; Pollock, B.G.; et al. Extent of Dorsolateral Prefrontal Cortex Plasticity and Its Association with Working Memory in Patients with Alzheimer Disease. JAMA Psychiatry 2017, 74, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Goldman, R.; Fristoe, M. Assessment of various auditory perceptual and cognitive skills. J. Commun. Disord. 1975, 8, 171–180. [Google Scholar] [CrossRef]
- Hellström, A.; Almkvist, O. Tone duration discrimination in demented, memory-impaired, and healthy elderly. Dement. Geriatr. Cogn. Disord. 1997, 8, 49–54. [Google Scholar] [CrossRef]
- Phillips, S.L.; Gordon-Salant, S.; Fitzgibbons, P.J.; Yeni-Komshian, G.H. Auditory duration discrimination in young and elderly listeners with normal hearing. J. Am. Acad. Audiol. 1994, 5, 210–215. [Google Scholar]
- Willott, J.F. Anatomic and physiologic aging: A behavioral neuroscience perspective. J. Am. Acad. Audiol. 1996, 7, 141–151. [Google Scholar]
- Working Group on Speech Understanding and Aging. Speech understanding and aging. J. Acoust. Soc. Am. 1988, 83, 859–895. [Google Scholar] [CrossRef]
- Pichora-Fuller, M.K. Cognitive aging and auditory information processing. Int. J. Audiol. 2003, 42, 26–32. [Google Scholar] [CrossRef]
- Schneider, B.A.; Pichora-Fuller, M.K. Implications of perceptual deterioration for cognitive aging research. In The Handbook of Aging and Cognition, 2nd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2000; pp. 155–219. [Google Scholar]
- Ohlenforst, B.; Zekveld, A.; Jansma, E.P.; Wang, Y.; Naylor, G.; Lorens, A.; Lunner, T.; Kramer, S. Effects of Hearing Impairment and Hearing Aid Amplification on Listening Effort: A Systematic Review. Ear Hear. 2016, 38, 267–281. [Google Scholar] [CrossRef] [Green Version]
- Lindenberger, U.; Baltes, P.B. Sensory Functioning and Intelligence in Old Age: A Strong Connection. Psychol. Aging 1994, 9, 339–355. [Google Scholar] [CrossRef]
- Baltes, P.B.; Lindenberger, U. Emergence of a Powerful Connection Between Sensory and Cognitive Functions Across the Adult Life Span: A New Window to the Study of Cognitive Aging? Psychol. Aging 1997, 12, 12–21. [Google Scholar] [CrossRef]
- Humes, L.E.; Dubno, J.R.; Gordon-Salant, S.; Lister, J.J.; Cacace, A.T.; Cruickshanks, K.J.; Gates, G.A.; Wilson, R.H.; Wingfield, A. Central presbycusis: A review and evaluation of the evidence. J. Am. Acad. Audiol. 2012, 23, 635–666. [Google Scholar] [CrossRef]
- Weihing, J.; Chermak, G.D.; Musiek, F.E. Auditory Training for Central Auditory Processing Disorder. Semin. Hear. 2015, 36, 199–215. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Country) | Groups Mean Age (±SD) (n) M/F | Patient Diagnostic Tool | Study Aim(s) | Types of Tests Used | Outcomes Measured | Major Findings | Limitations and/or Difficulties Reported |
|---|---|---|---|---|---|---|---|
| Edwards et al., 2016 USA | MCI: 73.73 ± 6.82 (45) 30/15 | MoCA | To compare older adults with and without MCI in auditory performance in competing acoustics signals and temporal aspects of audition. | SSI-ICM | Percent of correct answers | MCI < HC (p < 0.001) | Thorough neuropsychological evaluations for all study participants could not be obtained. |
| DSI (Free recall) | Percent of correct answers | MCI < HC (p < 0.001) | |||||
| HC: 70.59 ± 5.77 (34) 11/23 | ATTR (Across channel and within channel) | Average of shortest gap detected by participants (ms) | Across channel: MCI = HC | The sample included community-dwelling, noninstitutionalised older adults who were required to commute to the location of testing and were likely less impaired than the population. | |||
| Within channel: MCI > HC (p < 0.05) | |||||||
| TCS (Presented at a compression rate of 45% and 65%) | Percent of correct answers: average of score at 45% and 65% compression | MCI = HC | |||||
| Fausto et al., 2017 USA | MCI: 74.53 ± 6.58 (55) 30/21 | MoCA | To compare the Cognitive Self-Report Questionnaire (CSRQ) Hearing and Cognitive subscale ratings among older adults with and without MCI | SSI-ICM | Percent of correct answers | MCI < HC (p < 0.05) | The study did not examine cognitive domains other than memory. |
| DSI (Free recall) | Percent of correct answers | MCI < HC (p < 0.05) | |||||
| ATTR (Across channel and within channel) | Average of shortest gap detected by participants (ms) | Across channel: MCI = HC | Only assessed speech understanding in single-talker competition and did not assess speech understanding in multi-talker or broadband noise. | ||||
| HC: 71.37 ± 6.09 (50) 18/26 | To examine whether self-report, as measured by the CSRQ, is associated with objective measures of hearing, auditory processing, and cognition. | Within channel: MCI > HC (p < 0.05) | |||||
| TCS (Presented at a compression rate of 45% and 65%) | Percent correct out of 100 | 45% compression: MCI = HC | Lack of a diverse sample population | ||||
| 65% compression: MCI = HC | |||||||
| Gates et al., 2008 USA | AD: 84.0 ± 5.1 (17) 10/7 | CASI, CDR, and NINCDS-ADRDA | To evaluate whether abnormal central auditory processing test results could also be observed in persons with memory loss but none of the other criteria for a diagnosis of AD (i.e., MCI). | SSI-ICM | Percent of correct answers | MCI < HC (p < 0.05) | Patients must have sufficient vision to read the number of sentences heard and sufficient peripheral auditory function to understand speech at a comfortable loudness level. Because of the need to ensure adequate peripheral auditory function, CAP testing would not be suitable for those with severe hearing losses. |
| AD < HC (p < 0.05) | |||||||
| MCI: 82.3 ± 6.1 (64) 23/41 | DSI (Free recall) | Percent of correct answers | MCI < HC (p < 0.05) | ||||
| AD < HC (p < 0.05) | |||||||
| HC: 78.8 ± 4.7 (232) 86/146 | DDT (Free recall) | Percent of correct answers | MCI < HC (p < 0.05) | ||||
| AD < HC (p < 0.05) | |||||||
| Ghannoum et al., 2018 Egypt | MCI: 59.35 ± 4.8 (51) 34/17 | DSM-V | To clarify if the cognitive decline is associated with central auditory dysfunction. | SSI-ICM | Percent of correct answers | MCI < HC (p < 0.001) | None reported |
| To assess which tests of central auditory dysfunction or function of central auditory processing should be included in the early diagnostic procedure of memory complaints. | SSI-CCM | Percent of correct answers | MCI < HC (p < 0.001) | ||||
| DDT (Free recall) | Percent of correct answers | MCI < HC (p < 0.002) | |||||
| HC: 58.15 ± 4.18 (20) 13/7 | To identify which type of CAP impairment is present in patients with cognitive impairment. | AFT | ms | MCI > HC (p < 0.001) | |||
| To correlate objective auditory evoked potentials in speech auditory brainstem response with cognitive and central auditory dysfunction. | GFW | Correct number of words recalled | MCI < HC (p < 0.001) | ||||
| SPIN | Percent of correct answers (word recall) | MCI < HC (p < 0.001) | |||||
| Gootjes et al., 2018 The Netherlands | AD: 69.3 ± 8.7 (25) 18/7 | NINCDS-ADRDA | The study aimed to see whether asymmetrical performance on a dichotic listening task (DLT) in Alzheimer’s disease and aging is related to white matter pathology as reflected by corpus callosum atrophy. | DDT (DLT) (Directed attention) | Number of correct responses out of 60 | AD < SCD (p < 0.001) | Several patients had profound difficulties attending to the LE, and the attentional deficits of this subgroup might contaminate possible associations. |
| SCD (SMC): 66.1 ± 9.3 (20) 13/7 | AD< HC (p < 0.05) | ||||||
| HC: 68.6 ± 9.1 (20) 9/11 | SCD = HC | ||||||
| Hellstrom et al., 1996 Sweden | AD: 72.5 ± 6.5 (29) 6/23 | NINCDS-ADRDA and DSM-III-R | To investigate to what extent groups of AD, Ml, and healthy elderly can be differentiated by a TDD test. | TDD | C% Total percent correct responses | AD < HC (p < 0.05) | None reported. |
| MI (MCI): 73.6 ± 7.9 (10) 4/6 | MI < HC (p < 0.05) | ||||||
| HC: 80.6 ± 3 (21) 9/12 | |||||||
| Lliadou et al., 2016 Greece | MCI: 51-82 (18) 6/12 | DSM-V | To evaluate auditory perception in a group of older adults diagnosed with mild cognitive impairment (MCI). | SinB | SNR of 50% correct speech identification | MCI < HC (p < 0.05) | None reported. |
| RGDT | Threshold of gap detection at each frequency (shortest time interval participants reports perception of two tones) | MCI < HC (p < 0.005) | |||||
| HC: 50-73 (11) 5/6 | GIN | Gap detection threshold (shortest gap duration detected on at least four out of six presentations) | MCI < HC (p < 0.01) | ||||
| Jayakody et al., 2020 Australia | SCD (SMC) 71.5 ± 7.2 (61) 20/41 HC 68.8 ± 7.7 (34) 10/24 | MAC-Q and MoCA | To examine the central auditory processing (CAP) assessment results of adults between 45 and 85 years of age with subjective memory complaints (SMCs) as compared to those who were not reporting significant levels of memory complaints (non-SMCs). | DDT (Free recall) | Percent of correct answers | SCD = HC | None reported. |
| DPT | Percent of correct answers | SCD = HC | |||||
| QuickSIN | Signal-to-noise ratio loss | SCD = HC | |||||
| DSI (Directed attention) | Percent of correct answers | SCD = HC | |||||
| SSI-ICM | Percent of correct answers | SCD < HC (p < 0.05) | |||||
| Jalaei et al., 2019 Iran | MCI: 70.75 ± 5.09 (20) 13/7 | MMSE score | The purpose of this study was to examine the utility of central auditory processing tests as early diagnostic tools for identifying the elderly with MCI. | SPIN | Percent of correct answers (word recall) | MCI < HC (p < 0.001) | The use of simple clinical measures to investigate sensory processing is not enough to detect the sensory impairment associated with cognitive impairment. Moreover, frequency discrimination and temporal processing are needed for better speech perception. |
| HC: 71.3 ± 4.41 (20) 12/8 | GIN | Gap detection threshold (the smallest gap that the subject detects correctly in at least four out of the six presentations) | MCI > HC (p < 0.001) | ||||
| Lee et al., 2018 Korea | MCI: 68.56 ± 6.34 (30) 6/24 | Petersen’s criteria and MMSE score | The purpose of this study was (1) to compare speech perception performance among MCI subgroups and (2) to identify the cognitive domains specifically related to speech-in-noise perception. | SPIN | Percent of correct answers (word recall) | MCI < HC (p < 0.05) | None reported. |
| HC: 63.92 ± 4.48 (39) 14/25 | |||||||
| Rahman et al., 2011 Egypt | MCI: 66.5 ± 5.4 (150) 70/80 | CAMCOG | To assess if central auditory processing skills are affected in patients with MCI or not and assess sensitivity and specificity of central auditory processing tests in the detection of MCI. | SAAT | Percent of correct answers | MCI < HC (p = 0.001) | CAP tests require patients to be attentive and have sufficient peripheral auditory function to understand speech at a comfortable loudness level. |
| DDT (Free recall) | Percent of correct answers | MCI < HC Left ear only (p = 0.005) | |||||
| HC: 66.4 ± 5.6 (150) 70/80 | AFT | ms | MCI = HC | ||||
| PPS | Percent of correct answers | MCI < HC (p = 0.002) | |||||
| GFW | Correct number of words recalled | MCI < HC (p = 0.001) | |||||
| Sardone et al., 2020 Italy | MCI: 74 ± 5.62 (260) 148/112 | DSM-V | To explore the associations of age-related central auditory processing disorder (CAPD) with mild cognitive impairment (MCI) and dementia in an older population-based cohort. | SSI-ICM | Percent of correct answers | MCI < HC (p < 0.05) | None reported. |
| HC: 73.1 ± 5.74 (1055) 535/520 | |||||||
| Strouse et al., 1995 USA | AD: 72.3 ± 11.6 (10) 2/8 | DSM-III-R | To determine whether people in the early to middle phases of AD show impaired central auditory processing than those without dementia. | SSI-ICM | Percent of correct answers | AD < HC @ 0dB, −10 dB, −20 dB (p = 0.0001) | One subject within each experimental group was below the age of 65, and thus comparisons with existing studies evaluating elderly populations would not be applicable for these subjects. |
| DSI (Free recall) | Percent of correct answers | AD < HC (p < 0.004) | |||||
| HC: 70.1 ± 7.9 (10) 2/8 | DDT (Free recall) | Percent of correct answers | AD < HC (p < 0.001) | ||||
| PPS | Percent of correct answers | AD = HC | |||||
| DPT | Percent of correct answers | AD < HC (p = 0.0001) |
| Core Item | Tool Question (EPHPP, 1998) | Studies with Positive Assessment |
|---|---|---|
| Selection Bias | Are the individuals selected to participate in the study likely to be representative of the target population? | 11 (very likely) |
| What percentage of selected individuals agreed to participate? | 2 (80–100%) 11 (not described) | |
| Study Design | Was the study described as randomised? If NO, go to CONFOUNDERS. If Yes, was the method of randomisation described? If Yes, was the method appropriate? | 0 (Yes) |
| Confounders | Were there important differences between groups before the intervention? | 9 (No) |
| Indicate the percentage of relevant confounders that were controlled either in the design (e.g., stratification, matching) or analysis. | 13 (80–100%) | |
| Blinding | Was (were) the outcome assessor(s) aware of the intervention or exposure status of participants? | 0 (No) |
| Were the study participants aware of the research question? | 0 (No) | |
| Data Collection Methods | Were data collection tools shown to be valid? | 13 (Yes) |
| Were data collection tools shown to be reliable? | 13 (Yes) | |
| Withdraws and Dropout | Were withdrawals and dropouts reported in terms of numbers and/or reasons per group? | Not applicable (all studies were retrospective case–control) |
| Indicate the percentage of participants completing the study. (If the percentage differs by group, record the lowest.) | Not applicable (all studies were retrospective case–control) | |
| Intervention Integrity | What percentage of participants received the allocated intervention or exposure of interest? | 13 (80–100%) |
| Was the consistency of the intervention measured? | 13 (Yes) | |
| Is it likely that subjects received an unintended intervention (contamination or cointervention) that may influence the results? | 13 (No) | |
| Analysis | Indicate the unit of allocation. | 13 (Individual) |
| Indicate the unit of analysis. | 13 (Individual) | |
| Are the statistical methods appropriate for the study design? | 13 (Yes) | |
| Was the analysis performed by intervention allocation status (i.e., intention to treat) rather than the actual intervention received? | 13 (No) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarawneh, H.Y.; Menegola, H.K.; Peou, A.; Tarawneh, H.; Jayakody, D.M.P. Central Auditory Functions of Alzheimer’s Disease and Its Preclinical Stages: A Systematic Review and Meta-Analysis. Cells 2022, 11, 1007. https://doi.org/10.3390/cells11061007
Tarawneh HY, Menegola HK, Peou A, Tarawneh H, Jayakody DMP. Central Auditory Functions of Alzheimer’s Disease and Its Preclinical Stages: A Systematic Review and Meta-Analysis. Cells. 2022; 11(6):1007. https://doi.org/10.3390/cells11061007
Chicago/Turabian StyleTarawneh, Hadeel Y., Holly K. Menegola, Andrew Peou, Hanadi Tarawneh, and Dona M. P. Jayakody. 2022. "Central Auditory Functions of Alzheimer’s Disease and Its Preclinical Stages: A Systematic Review and Meta-Analysis" Cells 11, no. 6: 1007. https://doi.org/10.3390/cells11061007