
Analytical Performance of Next-Generation Sequencing and RT-PCR on Formalin-Fixed Paraffin-Embedded Tumor Tissues for PIK3CA Testing in HR+/HER2− Breast Cancer
 , , ,
, , ,  ,
,  ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
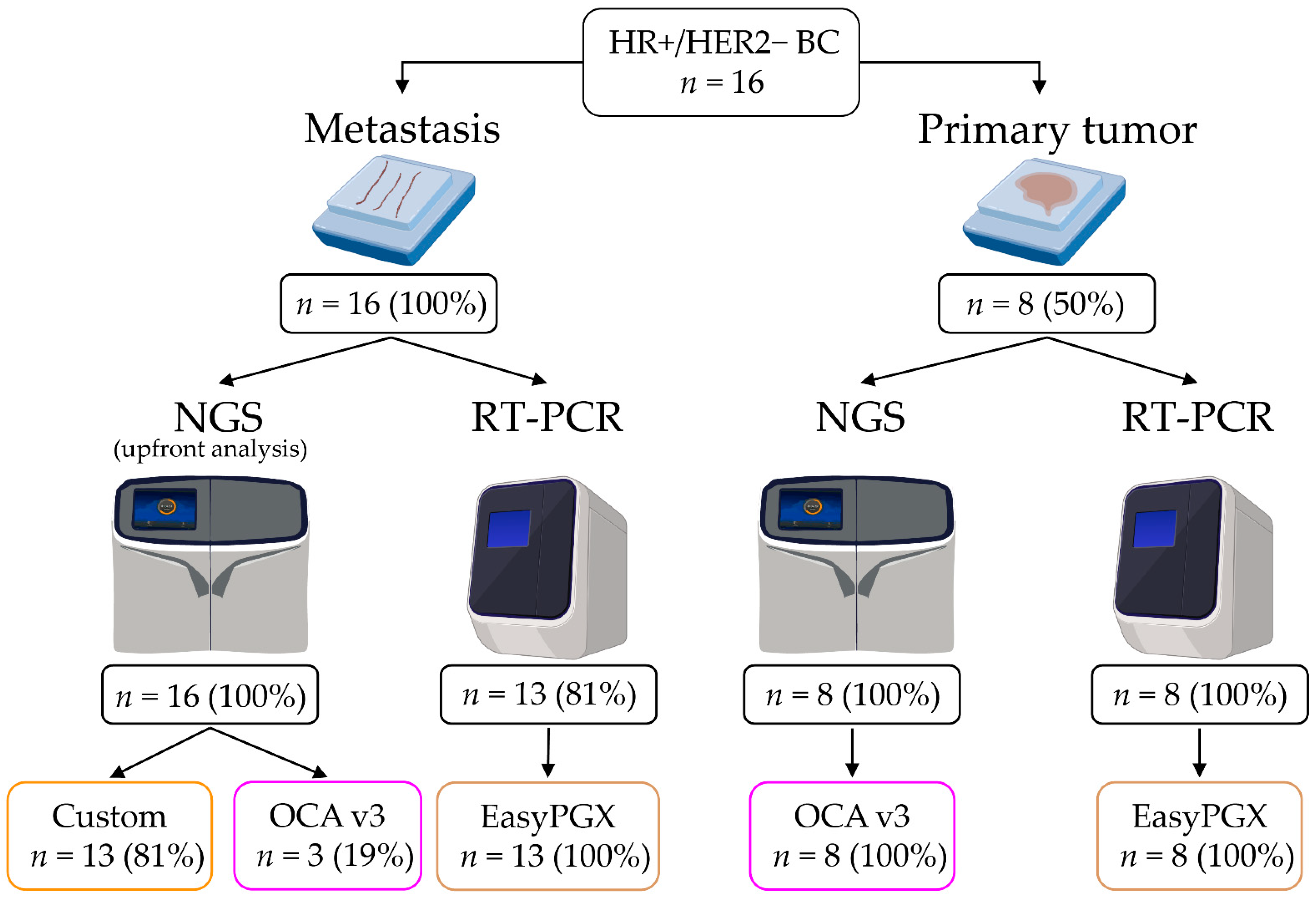
2.1. Study Design
2.2. Patients and Tissue Specimens
2.3. Nucleic Acids Purification
2.4. Next-Generation Sequencing (NGS) Analysis
2.5. RT-PCR Analysis
2.6. Statistical Analyses
3. Results
3.1. Clinicopathological Features
3.2. Concordance between Primary Tumor and Metastasis Samples Using NGS
3.3. Concordance between Primary Tumor and Metastasis Samples Using RT-PCR
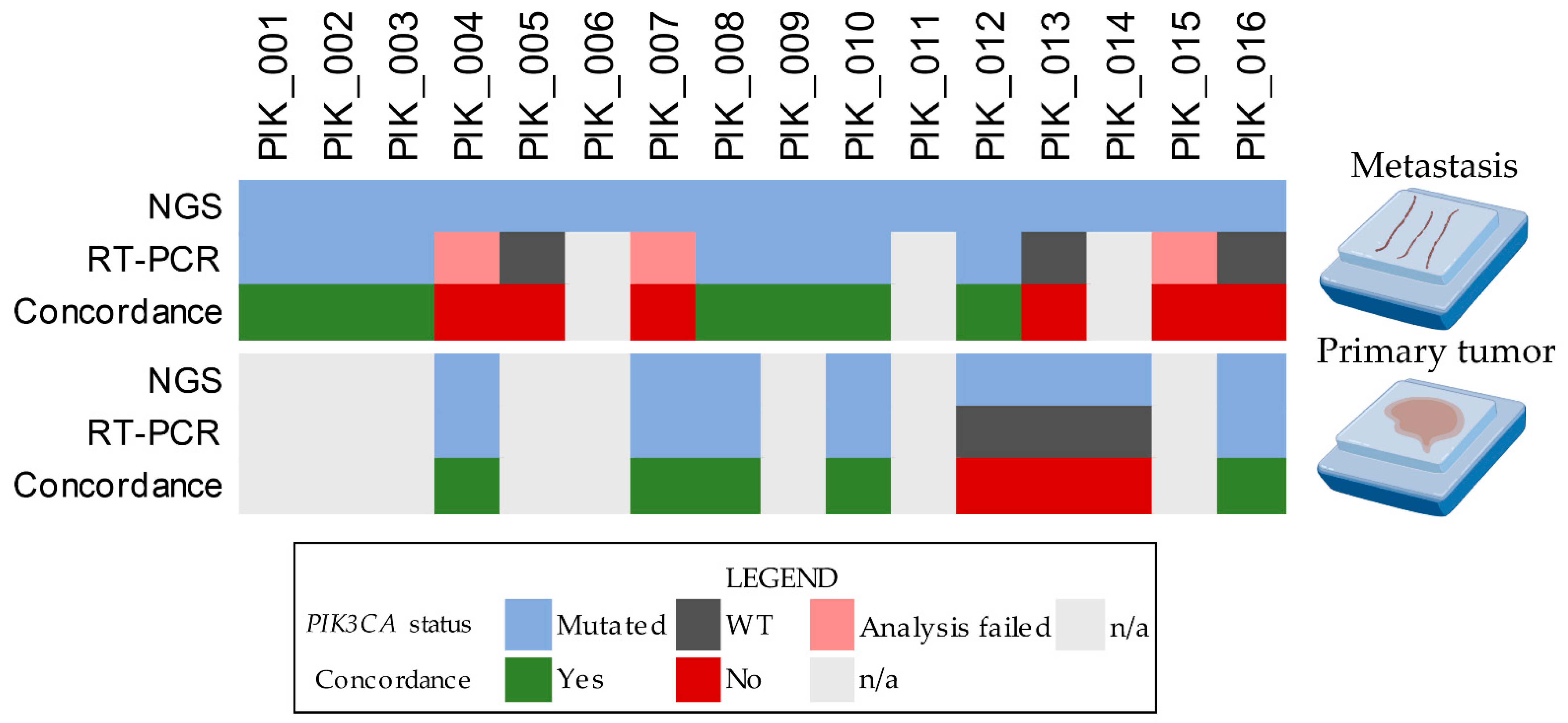
3.4. Comparison of NGS and RT-PCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Kaufman, B.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor-Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Lopez, G.; Costanza, J.; Colleoni, M.; Fontana, L.; Ferrero, S.; Miozzo, M.; Fusco, N. Molecular Insights into the Classification of Luminal Breast Cancers: The Genomic Heterogeneity of Progesterone-Negative Tumors. Int. J. Mol. Sci. 2019, 20, 510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Hui, R.; de Boer, R.; Lim, E.; Yeo, B.; Lynch, J. CDK4/6 inhibitor plus endocrine therapy for hormone receptor-positive, HER2-negative metastatic breast cancer: The new standard of care. Asia Pac. J. Clin. Oncol. 2021, 17 (Suppl. 1), 3–14. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.W.; Balko, J.M.; Arteaga, C.L. Phosphatidylinositol 3-kinase and antiestrogen resistance in breast cancer. J. Clin. Oncol. 2011, 29, 4452–4461. [Google Scholar] [CrossRef] [Green Version]
- Mosele, F.; Stefanovska, B.; Lusque, A.; Tran Dien, A.; Garberis, I.; Droin, N.; Le Tourneau, C.; Sablin, M.P.; Lacroix, L.; Enrico, D.; et al. Outcome and molecular landscape of patients with PIK3CA-mutated metastatic breast cancer. Ann. Oncol. 2020, 31, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Grizzi, G.; Ghidini, M.; Botticelli, A.; Tomasello, G.; Ghidini, A.; Grossi, F.; Fusco, N.; Cabiddu, M.; Savio, T.; Petrelli, F. Strategies for Increasing the Effectiveness of Aromatase Inhibitors in Locally Advanced Breast Cancer: An Evidence-Based Review on Current Options. Cancer Manag. Res. 2020, 12, 675–686. [Google Scholar] [CrossRef] [Green Version]
- Moynahan, M.E.; Chen, D.; He, W.; Sung, P.; Samoila, A.; You, D.; Bhatt, T.; Patel, P.; Ringeisen, F.; Hortobagyi, G.N.; et al. Correlation between PIK3CA mutations in cell-free DNA and everolimus efficacy in HR(+), HER2(-) advanced breast cancer: Results from BOLERO-2. Br. J. Cancer 2017, 116, 726–730. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Sáez, O.; Chic, N.; Pascual, T.; Adamo, B.; Vidal, M.; González-Farré, B.; Sanfeliu, E.; Schettini, F.; Conte, B.; Brasó-Maristany, F.; et al. Frequency and spectrum of PIK3CA somatic mutations in breast cancer. Breast Cancer Res. 2020, 22, 45. [Google Scholar] [CrossRef]
- Goncalves, M.D.; Hopkins, B.D.; Cantley, L.C. Phosphatidylinositol 3-Kinase, Growth Disorders, and Cancer. N. Engl. J. Med. 2018, 379, 2052–2062. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, C.; Huang, A.; Chatenay-Rivauday, C.; Schnell, C.; Reddy, A.; Liu, M.; Kauffmann, A.; Guthy, D.; Erdmann, D.; De Pover, A.; et al. Characterization of the novel and specific PI3Kα inhibitor NVP-BYL719 and development of the patient stratification strategy for clinical trials. Mol. Cancer Ther. 2014, 13, 1117–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritsch, C.; Pfister, E.; Ebel, N.; Guthy, D.; Schnell, C.; Hofmann, F. Abstract 3934: Determination of the PI3Kα selective inhibitor alpelisib mechanism of action and efficacy in ER+/PIK3CA mutant breast cancer preclinical models. Cancer Res. 2018, 78, 3934. [Google Scholar] [CrossRef]
- André, F.; Ciruelos, E.M.; Juric, D.; Loibl, S.; Campone, M.; Mayer, I.A.; Rubovszky, G.; Yamashita, T.; Kaufman, B.; Lu, Y.S.; et al. Alpelisib plus fulvestrant for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: Final overall survival results from SOLAR-1. Ann. Oncol. 2021, 32, 208–217. [Google Scholar] [CrossRef]
- Copur, M.S. Alpelisib to treat breast cancer. Drugs Today (Barc.) 2020, 56, 357–363. [Google Scholar] [CrossRef]
- Fusco, N.; Malapelle, U.; Fassan, M.; Marchiò, C.; Buglioni, S.; Zupo, S.; Criscitiello, C.; Vigneri, P.; Dei Tos, A.P.; Maiorano, E.; et al. PIK3CA Mutations as a Molecular Target for Hormone Receptor-Positive, HER2-Negative Metastatic Breast Cancer. Front. Oncol. 2021, 11, 644737. [Google Scholar] [CrossRef]
- Chan, A.C.; Weiss, L.M.; Bender, R. Abstract P4-09-15: A large study of PIK3CA mutations in the community setting identifies varying degree of mutation positivity rates across age groups in advanced HR+, HER2- breast cancer patients using an FDA RT-PCR cleared test. Cancer Res. 2020, 80, P4-09-15. [Google Scholar] [CrossRef]
- Rugo, H.S.; Lerebours, F.; Ciruelos, E.; Drullinsky, P.; Ruiz-Borrego, M.; Neven, P.; Park, Y.H.; Prat, A.; Bachelot, T.; Juric, D.; et al. Alpelisib plus fulvestrant in PIK3CA-mutated, hormone receptor-positive advanced breast cancer after a CDK4/6 inhibitor (BYLieve): One cohort of a phase 2, multicentre, open-label, non-comparative study. Lancet Oncol. 2021, 22, 489–498. [Google Scholar] [CrossRef]
- Angerilli, V.; Galuppini, F.; Pagni, F.; Fusco, N.; Malapelle, U.; Fassan, M. The Role of the Pathologist in the Next-Generation Era of Tumor Molecular Characterization. Diagnostics 2021, 11, 339. [Google Scholar] [CrossRef]
- Cappello, F.; Angerilli, V.; Munari, G.; Ceccon, C.; Sabbadin, M.; Pagni, F.; Fusco, N.; Malapelle, U.; Fassan, M. FFPE-Based NGS Approaches into Clinical Practice: The Limits of Glory from a Pathologist Viewpoint. J. Pers. Med. 2022, 12, 750. [Google Scholar] [CrossRef]
- Kalinsky, K.; Heguy, A.; Bhanot, U.K.; Patil, S.; Moynahan, M.E. PIK3CA mutations rarely demonstrate genotypic intratumoral heterogeneity and are selected for in breast cancer progression. Breast Cancer Res. Treat. 2011, 129, 635. [Google Scholar] [CrossRef] [PubMed]
- Zardavas, D.; te Marvelde, L.; Milne, R.L.; Fumagalli, D.; Fountzilas, G.; Kotoula, V.; Razis, E.; Papaxoinis, G.; Joensuu, H.; Moynahan, M.E.; et al. Tumor PIK3CA Genotype and Prognosis in Early-Stage Breast Cancer: A Pooled Analysis of Individual Patient Data. J. Clin. Oncol. 2018, 36, 981–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berrino, E.; Annaratone, L.; Miglio, U.; Maldi, E.; Piccinelli, C.; Peano, E.; Balmativola, D.; Cassoni, P.; Pisacane, A.; Sarotto, I.; et al. Cold Formalin Fixation Guarantees DNA Integrity in Formalin Fixed Paraffin Embedded Tissues: Premises for a Better Quality of Diagnostic and Experimental Pathology with a Specific Impact on Breast Cancer. Front. Oncol. 2020, 10, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- General Data Protection Regulation (GDPR). 2018. OJ L 119, 04.05.2016; cor. OJ L 127, 23.5.2018. Available online: https://www.epsu.org/sites/default/files/article/files/GDPR_FINAL_EPSU.pdf (accessed on 14 September 2022).
- WHO Classification of Tumours Editorial Board. WHO Classification of Breast Tumours: WHO Classification of Tumours; World Health Organization: Geneva, Switzerland, 2019; Volume 2. [Google Scholar]
- Rakha, E.A.; El-Sayed, M.E.; Lee, A.H.; Elston, C.W.; Grainge, M.J.; Hodi, Z.; Blamey, R.W.; Ellis, I.O. Prognostic significance of Nottingham histologic grade in invasive breast carcinoma. J. Clin. Oncol. 2008, 26, 3153–3158. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef]
- Fusco, N.; Ragazzi, M.; Sajjadi, E.; Venetis, K.; Piciotti, R.; Morganti, S.; Santandrea, G.; Fanelli, G.N.; Despini, L.; Invernizzi, M.; et al. Assessment of estrogen receptor low positive status in breast cancer: Implications for pathologists and oncologists. Histol. Histopathol 2021, 36, 18376. [Google Scholar] [CrossRef]
- Venetis, K.; Crimini, E.; Sajjadi, E.; Corti, C.; Guerini-Rocco, E.; Viale, G.; Curigliano, G.; Criscitiello, C.; Fusco, N. HER2 low, ultra-low, and novel complementary biomarkers: Expanding the spectrum of HER2 positivity in breast cancer. Front. Mol. Biosci. 2022, 9, 834651. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Cho, M.; Ahn, S.; Hong, M.; Bang, H.; Van Vrancken, M.; Kim, S.; Lee, J.; Park, S.H.; Park, J.O.; Park, Y.S.; et al. Tissue recommendations for precision cancer therapy using next generation sequencing: A comprehensive single cancer center’s experiences. Oncotarget 2017, 8, 42478–42486. [Google Scholar] [CrossRef] [Green Version]
- Groelz, D.; Viertler, C.; Pabst, D.; Dettmann, N.; Zatloukal, K. Impact of storage conditions on the quality of nucleic acids in paraffin embedded tissues. PLoS ONE 2018, 13, e0203608. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Cho, S.Y.; Chang, E.S.; Sung, M.; Song, J.Y.; Jung, K.; Kim, S.S.; Shin, Y.K.; Choi, Y.L. Analysis of PIK3CA Mutation Concordance and Frequency in Primary and Different Distant Metastatic Sites in Breast Cancer. Cancer Res. Treat 2022. [Google Scholar] [CrossRef]
- Zardavas, D.; Irrthum, A.; Swanton, C.; Piccart, M. Clinical management of breast cancer heterogeneity. Nat. Rev. Clin. Oncol. 2015, 12, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Suppan, C.; Graf, R.; Jahn, S.; Zhou, Q.; Klocker, E.V.; Bartsch, R.; Terbuch, A.; Kashofer, K.; Regitnig, P.; Lindenmann, J.; et al. Sensitive and robust liquid biopsy-based detection of PIK3CA mutations in hormone-receptor-positive metastatic breast cancer patients. Br. J. Cancer 2022, 126, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Aftimos, P.; Oliveira, M.; Irrthum, A.; Fumagalli, D.; Sotiriou, C.; Gal-Yam, E.N.; Robson, M.E.; Ndozeng, J.; Di Leo, A.; Ciruelos, E.M.; et al. Genomic and Transcriptomic Analyses of Breast Cancer Primaries and Matched Metastases in AURORA, the Breast International Group (BIG) Molecular Screening Initiative. Cancer Discov. 2021, 11, 2796–2811. [Google Scholar] [CrossRef]
- Markou, A.; Farkona, S.; Schiza, C.; Efstathiou, T.; Kounelis, S.; Malamos, N.; Georgoulias, V.; Lianidou, E. PIK3CA Mutational Status in Circulating Tumor Cells Can Change During Disease Recurrence or Progression in Patients with Breast Cancer. Clin. Cancer Res. 2014, 20, 5823–5834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, E.J.; Mollon, L.E.; Dean, J.L.; Warholak, T.L.; Aizer, A.; Platt, E.A.; Tang, D.H.; Davis, L.E. A Systematic Review of the Prevalence and Diagnostic Workup of PIK3CA Mutations in HR+/HER2- Metastatic Breast Cancer. Int. J. Breast. Cancer 2020, 2020, 3759179. [Google Scholar] [CrossRef]
- Kerr, K.M.; Bibeau, F.; Thunnissen, E.; Botling, J.; Ryška, A.; Wolf, J.; Öhrling, K.; Burdon, P.; Malapelle, U.; Büttner, R. The evolving landscape of biomarker testing for non-small cell lung cancer in Europe. Lung Cancer 2021, 154, 161–175. [Google Scholar] [CrossRef]
- Alvarez-Garcia, V.; Bartos, C.; Keraite, I.; Trivedi, U.; Brennan, P.M.; Kersaudy-Kerhoas, M.; Gharbi, K.; Oikonomidou, O.; Leslie, N.R. A simple and robust real-time qPCR method for the detection of PIK3CA mutations. Sci. Rep. 2018, 8, 4290. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients (n = 16) | |
|---|---|
| Age at diagnosis, range (median) | 32–73 (52.5) |
| Histology, n (%) | |
| NST | 15 (93.7) |
| Lobular | 1 (6.3) |
| ER, n (%) | |
| Positive | 16 (100) |
| Negative | 0 |
| PgR, n (%) | |
| Positive | 8 (50.0) |
| Negative | 8 (50.0) |
| HER2, n (%) | |
| Low | 7 (43.8) |
| Zero | 9 (56.2) |
| Metastatic site, n (%) | |
| Bone (iliac crest) | 2 (12.5) |
| Bone (pelvis) | 1 (6.3) |
| Lymph node | 2 (12.5) |
| Liver | 8 (50.0) |
| Pleura | 2 (12.5) |
| Thoracic wall | 1 (6.3) |
| Therapy with CDK4/6, n (%) | |
| Yes | 6 (37.5) |
| No | 10 (62.5) |
| #Case | Age at Original Diagnosis | Time between Primary Tumor and Metastasis (Months) | Sample Type | ER (%) | PgR (%) | HER2 (%) |
|---|---|---|---|---|---|---|
| PIK_004 | 26 | 69 | Primary | 95 | 95 | 1+ |
| Metastasis | 95 | 0 | 1+ | |||
| PIK_007 | 46 | 102 | Primary | 95 | 70 | 1+ |
| Metastasis | 90 | 2 | 2+ not amplified | |||
| PIK_008 | 45 | 54 | Primary | 95 | 0 | 1+ |
| Metastasis | 95 | 0 | 2+ not amplified | |||
| PIK_010 | 53 | 126 | Primary | 95 | 0 | 1+ |
| Metastasis | 95 | 0 | 2+ not amplified | |||
| PIK_012 | 43 | 38 | Primary | 95 | 20 | 2+ not amplified |
| Metastasis | 95 | 10 | 1+ | |||
| PIK_013 | 44 | 117 | Primary | 95 | 95 | 0 |
| Metastasis | 80 | 90 | 0 | |||
| PIK_014 | 41 | 116 | Primary | 95 | 95 | 1+ |
| Metastasis | 95 | 0 | 0 | |||
| PIK_016 | 40 | 127 | Primary | 95 | 95 | 0 |
| Metastasis | 60 | 0 | 0 |
| Metastases | Primary Tumors | |||||||
|---|---|---|---|---|---|---|---|---|
| #Case | [DNA] (ng/µL) | Tumor Cell Content (%) | Mutation | VAF (%) | [DNA] (ng/µL) | Tumor Cell Content (%) | Mutation | VAF (%) |
| PIK_001 | 0.26 | 20 | p.E545K/c.1633G>A | 3 | - | - | - | - |
| PIK_002 | 0.84 | 60 | p.H1047R/c.3140A>G | 29 | - | - | - | - |
| PIK_003 | 0.37 | 60 | p.H1047R/c.3140A>G | 67 | - | - | - | - |
| PIK_004 | 0.24 | 70 | p.H1047R/c.3140A>G | 38 | 2.99 | 60 | p.H1047R/c.3140A>G | 42 |
| PIK_005 | 0.44 | 80 | p.N1068Kfs*5/c.3203_3204insA | 20 | - | - | - | - |
| PIK_006 | 0.42 | 70 | p.E545K/c.1633G>A | 35 | - | - | - | - |
| PIK_007 | 0.36 | 30 | p.H1047R/c.3140A>G | 10 | 0.54 | 20 | p.H1047R/c.3140A>G | 41 |
| PIK_008 | 4.06 | 85 | p.H1047R/c.3140A>G | 56 | 0.41 | 35 | p.H1047R/c.3140A>G | 22 |
| PIK_009 | 0.43 | 70 | p.H1047L/c.3140A>T | 24 | - | - | - | - |
| PIK_010 | 0.24 | 70 | p.E545K/c.1633G>A | 25 | 0.66 | 60 | p.E545K/c.1633G>A | 49 |
| PIK_011 | 4.52 | 60 | p.H1047R/c.3140A>G | 44 | - | - | - | - |
| PIK_012 | 0.48 | 60 | p.E542K/c.1624G>A | 18 | 0.31 | 80 | p.E542K/c.1624G>A | 4 |
| PIK_013 | 113.00 | 80 | p.E453K/c.1357G>A | 13 | 3.06 | 75 | p.E453K/c.1357G>A | 37 |
| PIK_014 | 0.42 | 50 | p.N1044K/c.3132T>A | 54 | 1.83 | 75 | p.N1044K/c.3132T>A | 37 |
| PIK_015 | 0.12 | 90 | p.Q546K/c.1636C>A | 37 | - | - | - | - |
| PIK_016 | 0.07 | 80 | p.Q546R/c.1637A>G | 33 | 0.97 | 40 | p.Q546R/c.1637A>G | 45 |
| Metastases | Primary Tumors | |||||
|---|---|---|---|---|---|---|
| #Case | [DNA] (ng/µL) | Tumor Cell Content (%) | Mutation | [DNA] (ng/µL) | Tumor Cell Content (%) | Mutation |
| PIK_001 | 0.26 | 20 | E545x | - | - | - |
| PIK_002 | 0.84 | 60 | H1047x | - | - | - |
| PIK_003 | 0.37 | 60 | H1047x | - | - | - |
| PIK_004 | 0.26 | 35 | Failed * | 9.11 | 60 | H1047x |
| PIK_005 | 0.44 | 20 | WT # | - | - | - |
| PIK_006 | - | - | - | - | - | - |
| PIK_007 | 0.18 | 40 | Failed * | 0.54 | 20 | H1047x |
| PIK_008 | 4.06 | 85 | H1047x | 0.41 | 90 | H1047x |
| PIK_009 | 0.43 | 70 | H1047x | - | - | - |
| PIK_010 | 0.24 | 70 | E545x | 2.49 | 30 | E545x |
| PIK_011 | - | - | - | - | - | - |
| PIK_012 | 0.48 | 60 | E542x | 0.47 | 90 | WT |
| PIK_013 | 28.00 | 70 | WT # | 12.00 | 70 | WT # |
| PIK_014 | - | - | - | 7.31 | 35 | WT # |
| PIK_015 | 0.12 | 90 | Failed * | - | - | - |
| PIK_016 | 0.14 | 80 | WT | 0.97 | 40 | Q546x |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venetis, K.; Pepe, F.; Munzone, E.; Sajjadi, E.; Russo, G.; Pisapia, P.; Ivanova, M.; Bonizzi, G.; Vacirca, D.; Rappa, A.; et al. Analytical Performance of Next-Generation Sequencing and RT-PCR on Formalin-Fixed Paraffin-Embedded Tumor Tissues for PIK3CA Testing in HR+/HER2− Breast Cancer. Cells 2022, 11, 3545. https://doi.org/10.3390/cells11223545
Venetis K, Pepe F, Munzone E, Sajjadi E, Russo G, Pisapia P, Ivanova M, Bonizzi G, Vacirca D, Rappa A, et al. Analytical Performance of Next-Generation Sequencing and RT-PCR on Formalin-Fixed Paraffin-Embedded Tumor Tissues for PIK3CA Testing in HR+/HER2− Breast Cancer. Cells. 2022; 11(22):3545. https://doi.org/10.3390/cells11223545
Chicago/Turabian StyleVenetis, Konstantinos, Francesco Pepe, Elisabetta Munzone, Elham Sajjadi, Gianluca Russo, Pasquale Pisapia, Mariia Ivanova, Giuseppina Bonizzi, Davide Vacirca, Alessandra Rappa, and et al. 2022. "Analytical Performance of Next-Generation Sequencing and RT-PCR on Formalin-Fixed Paraffin-Embedded Tumor Tissues for PIK3CA Testing in HR+/HER2− Breast Cancer" Cells 11, no. 22: 3545. https://doi.org/10.3390/cells11223545