
Morbidity and Mortality of Neutropenic Patients in Visceral Surgery: A Narrative Review
 , , and
, , and
Abstract
:1. Introduction
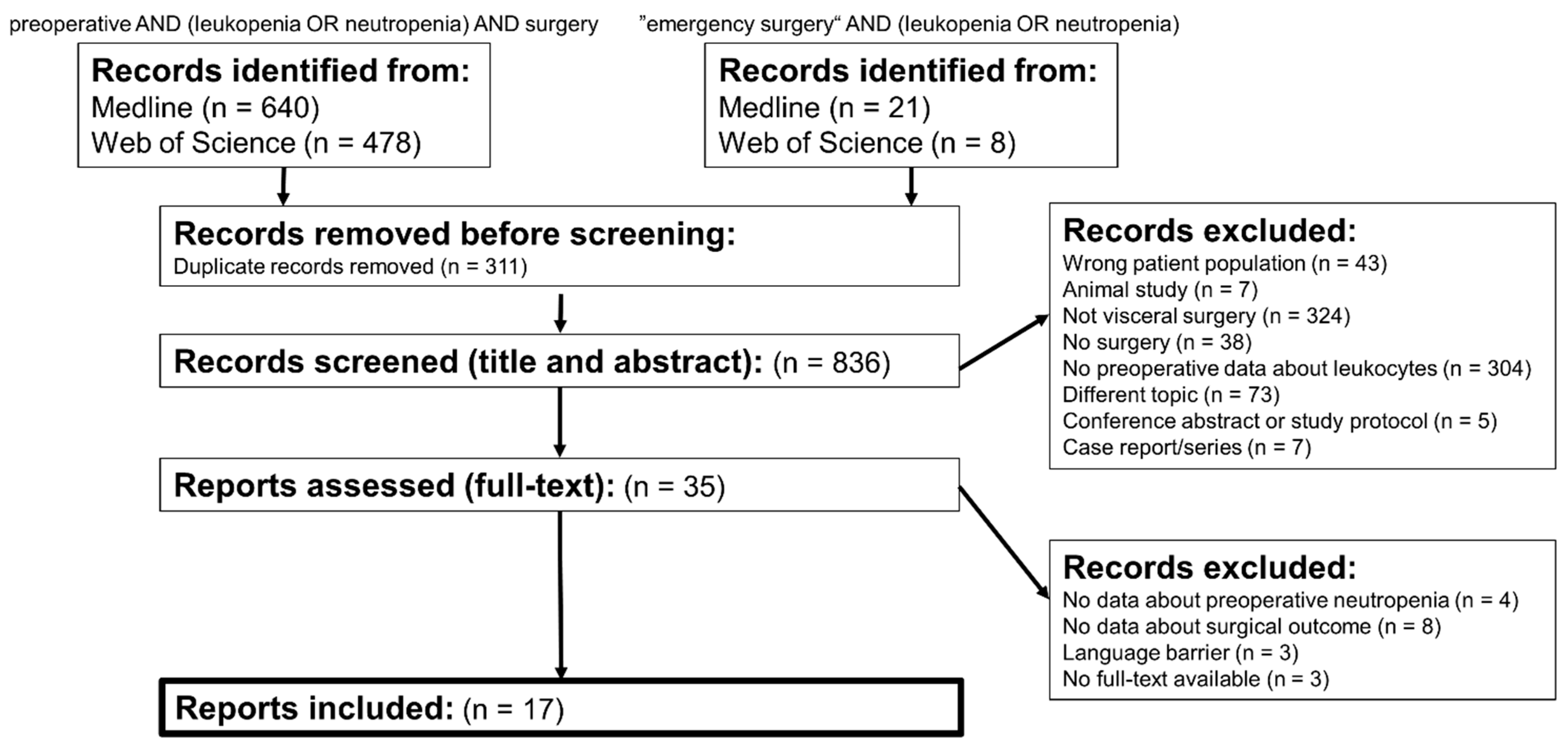
2. Materials and Methods
Research Questions
- (1)
- Does preoperative neutropenia affect the morbidity and mortality of patients undergoing emergency visceral surgery?
- (2)
- Does preoperative neutropenia affect the morbidity and mortality of patients undergoing elective visceral surgery?
3. Results
3.1. Research Question 1: Morbidity and Mortality in Emergency Surgery
Short Digression: Improving the Postoperative Outcome by an Application of G-CSF
3.2. Research Question 2: Morbidity and Mortality in Elective Surgery
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| G-CSF | granulocyte colony-stimulating factor |
| NOMI | non-occlusive mesenteric ischemia |
| SSI | surgical site infection |
References
- Sattler, S. The Role of the Immune System Beyond the Fight Against Infection. Adv. Exp. Med. Biol. 2017, 1003, 314. [Google Scholar] [CrossRef]
- Rosales, C. Neutrophils at the crossroads of innate and adaptive immunity. J. Leukoc. Biol. 2020, 108, 377–396. [Google Scholar] [CrossRef] [PubMed]
- Silvestre-Roig, C.; Fridlender, Z.G.; Glogauer, M.; Scapini, P. Neutrophil Diversity in Health and Disease. Trends Immunol. 2019, 40, 565–583. [Google Scholar] [CrossRef]
- Huse, M. Mechanical forces in the immune system. Nat. Rev. Immunol. 2017, 17, 679–690. [Google Scholar] [CrossRef]
- Foucar, K.; Duncan, M.H.; Smith, K.J. Practical Approach to the Investigation of Neutropenia. Clin. Lab. Med. 1993, 13, 879–894. [Google Scholar] [CrossRef]
- Hidalgo, A.; Chilvers, E.R.; Summers, C.; Koenderman, L. The Neutrophil Life Cycle. Trends Immunol. 2019, 40, 584–597. [Google Scholar] [CrossRef]
- Greenlee-Wacker, M.C. Clearance of apoptotic neutrophils and resolution of inflammation. Immunol. Rev. 2016, 273, 357–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natoli, G.; Ostuni, R. Adaptation and memory in immune responses. Nat. Immunol. 2019, 20, 783–792. [Google Scholar] [CrossRef]
- Ballesteros, I.; Rubio-Ponce, A.; Genua, M.; Lusito, E.; Kwok, I.; Fernández-Calvo, G.; Khoyratty, T.E.; van Grinsven, E.; González-Hernández, S.; Nicolás-Ávila, J.Á.; et al. Co-option of Neutrophil Fates by Tissue Environments. Cell 2020, 183, 1282–1297.e18. [Google Scholar] [CrossRef]
- Gibson, C.; Berliner, N. How we evaluate and treat neutropenia in adults. Blood 2014, 124, 1251–1258. [Google Scholar] [CrossRef]
- Schatzman, A.; Vandenheuvel, J.; Villalobos, T.; Rooney, K. Transient leukopenia, thrombocytopenia, and severe neutropenia associated with acute SARS-CoV-2 infection. Pediatr. Blood Cancer 2021, 68, 10. [Google Scholar] [CrossRef] [PubMed]
- Christen, D.; Brümmendorf, T.; Panse, J. Leukopenie-ein diagnostischer Leitfaden für die Praxis. DMW-Dtsch. Med. Wochenschr. 2017, 142, 1744–1749. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, V.; Saleem, A. Review: Drug-induced neutropenia--pathophysiology, clinical features, and management. Ann. Clin. Lab. Sci. 2004, 34, 131–137. [Google Scholar]
- Palmblad, J.; Dufour, C.; Papadaki, H.A. How we diagnose neutropenia in the adult and elderly patient. Haematologica 2014, 99, 1130–1133. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Hieber, M.; Teschner, D.; Maschmeyer, G.; Schalk, E. Management of febrile neutropenia in the perspective of antimicrobial de-escalation and discontinuation. Expert Rev. Anti. Infect. Ther. 2019, 17, 983–995. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.; Dale, D.C.; Lyman, G.H. Chemotherapy-induced neutropenia. Cancer 2004, 100, 228–237. [Google Scholar] [CrossRef]
- Penack, O.; Becker, C.; Buchheidt, D.; Christopeit, M.; Kiehl, M.; von Lilienfeld-Toal, M.; Hentrich, M.; Reinwald, M.; Salwender, H.; Schalk, E.; et al. Management of sepsis in neutropenic patients: 2014 updated guidelines from the Infectious Diseases Working Party of the German Society of Hematology and Medical Oncology (AGIHO). Ann. Hematol. 2014, 93, 1083–1095. [Google Scholar] [CrossRef] [Green Version]
- Common Terminology Criteria for Adverse Events (CTCAE). National Cancer Institute, Cancer Therapy Evaluation Program, Bethesda, MD, USA, 2017.
- White, M.G.; Morgan, R.B.; Drazer, M.W.; Eng, O.S. Gastrointestinal Surgical Emergencies in the Neutropenic Immunocompromised Patient. J. Gastrointest. Surg. 2021, 25, 3258–3264. [Google Scholar] [CrossRef]
- Wade, D.S. Abdominal Pain in Neutropenic Patients. Arch. Surg. 1990, 125, 1119. [Google Scholar] [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, R. Writing narrative style literature reviews. Med. Writ. 2015, 24, 230–235. [Google Scholar] [CrossRef]
- Nishida, T.; Hasegawa, J.; Nakao, K.; Fujita, N. Granulocyte colony-stimulating factor for gastrointestinal perforation in patients with leukopenia. J. Trauma 1996, 40, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Hansen, O.; Graupe, F.; Stock, W. Prognostic factors in perforating diverticulitis of the large intestine. Chirurg. 1998, 69, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.C.; Roman, S.A.; Sosa, J.A. Does Chemotherapy Prior to Emergency Surgery Affect Patient Outcomes? Examination of 1912 Patients. Ann. Surg. Oncol. 2012, 19, 11–18. [Google Scholar] [CrossRef]
- Sudarshan, M.; Feldman, L.S.; St. Louis, E.; Al-Habboubi, M.; Elhusseini Hassan, M.M.; Fata, P.; Deckelbaum, D.L.; Razek, T.S.; Khwaja, K.A. Predictors of mortality and morbidity for acute care surgery patients. J. Surg. Res. 2015, 193, 868–873. [Google Scholar] [CrossRef]
- Gulack, B.C.; Englum, B.R.; Lo, D.D.; Nussbaum, D.P.; Keenan, J.E.; Scarborough, J.E.; Shapiro, M.L. Leukopenia is associated with worse but not prohibitive outcomes following emergent abdominal surgery. J. Trauma Acute Care Surg. 2015, 79, 437–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokart, D.; Penalver, M.; Chow-Chine, L.; Ewald, J.; Sannini, A.; Brun, J.P.; Bisbal, M.; Lelong, B.; Delpero, J.R.; Faucher, M.; et al. Surgical treatment of acute abdominal complications in hematology patients: Outcomes and prognostic factors. Leuk. Lymphoma 2017, 58, 2395–2402. [Google Scholar] [CrossRef]
- Joo, Y.; Lee, Y.; Yoo, T.; Kim, J.; Park, I.; Gwak, G.; Cho, H.; Yang, K.; Kim, K.; Bae, B.-N. Prognostic Factors and Management for Left Colonic Perforation: Can Hartmann’s Procedure Be Preventable? Ann. Coloproctol. 2020, 36, 178–185. [Google Scholar] [CrossRef]
- Fokstuen, T.; Holm, T.; Glimelius, B. Postoperative morbidity and mortality in relation to leukocyte counts and time to surgery after short-course preoperative radiotherapy for rectal cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2009, 93, 293–297. [Google Scholar] [CrossRef]
- Reim, D.; Hüser, N.; Humberg, D.; Novotny, A.; Assfalg, V.; Matevossian, E.; Friess, H.; Schuhmacher, C. Preoperative clinically inapparent leucopenia in patients undergoing neoadjuvant chemotherapy for locally advanced gastric cancer is not a risk factor for surgical or general postoperative complications. J. Surg. Oncol. 2010, 102, 321–324. [Google Scholar] [CrossRef]
- Bamba, R.; Lorenz, J.M.; Lale, A.J.; Funaki, B.S.; Zangan, S.M. Clinical predictors of port infections within the first 30 days of placement. J. Vasc. Interv. Radiol. 2014, 25, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Ohira, M.; Kubo, N.; Yamashita, Y.; Sakurai, K.; Toyokawa, T.; Tanaka, H.; Muguruma, K.; Hirakawa, K. Impact of Chemoradiation-induced Myelosuppression on Prognosis of Patients with Locally Advanced Esophageal Cancer After Chemoradiotherapy Followed by Esophagectomy. Anticancer Res. 2015, 35, 4889–4895. [Google Scholar] [PubMed]
- Pluta, M.; Krzych, Ł. Can the leukocyte’s parameters in peripheral blood smear predict risk of in-hospital death of patients undergoing high-risk gastrointestinal surgery? Pol. Przegl. Chir. 2018, 91, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Wu, C.; Zhao, H.; Wu, J.; Zhao, J.; Bi, X.; Li, Z.; Huang, Z.; Zhang, Y.; Zhou, J.; et al. Neo-adjuvant Chemotherapy-Induced Neutropenia Is Associated with Histological Responses and Outcomes after the Resection of Colorectal Liver Metastases. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract. 2020, 24, 659–670. [Google Scholar] [CrossRef]
- Grant, H.M.; Davis, L.L.; Garb, J.; Arenas, R.B.; Stefan, M.S. Preoperative leukopenia does not affect outcomes in cancer patients undergoing elective and emergent abdominal surgery: A brief report. Am. J. Surg. 2020, 220, 132–134. [Google Scholar] [CrossRef]
- Hara, H.; Mizusawa, J.; Hironaka, S.; Kato, K.; Daiko, H.; Abe, T.; Nakamura, K.; Ando, N.; Kitagawa, Y. Influence of preoperative chemotherapy-induced leukopenia on survival in patients with esophageal squamous cell carcinoma: Exploratory analysis of JCOG9907. Esophagus 2021, 18, 41–48. [Google Scholar] [CrossRef]
- Zarain-Obrador, L.; Alonso-García, M.; Gil-Yonte, P.; Hijas-Gómez, A.I.; Rodríguez-Villar, D.; Martínez-Amores, B.; Gil-de-Miguel, Á.; Ruiz-Tovar, J.; Rodríguez-Caravaca, G.; Durán-Poveda, M. Effect of a Surgical Care Bundle on the Incidence of Surgical Site Infection in Colorectal Surgery: A Quasi-Experimental Intervention. Rev Invest Clin 2021, 73. [Google Scholar] [CrossRef]
- Zajicek, G. Cancer as a systemic disease. Med. Hypotheses 1978, 4, 193–207. [Google Scholar] [CrossRef]
- Alečković, M.; McAllister, S.S.; Polyak, K. Metastasis as a systemic disease: Molecular insights and clinical implications. Biochim. Biophys. Acta–Rev. Cancer 2019, 1872, 89–102. [Google Scholar] [CrossRef]
- Hendifar, A.E.; Chang, J.I.; Huang, B.Z.; Tuli, R.; Wu, B.U. Cachexia, and not obesity, prior to pancreatic cancer diagnosis worsens survival and is negated by chemotherapy. J. Gastrointest. Oncol. 2018, 9, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Tan, D.J.H.; Yaow, C.Y.L.; Mok, H.T.; Ng, C.H.; Tai, C.H.; Tham, H.Y.; Foo, F.J.; Chong, C.S. The influence of diabetes on postoperative complications following colorectal surgery. Tech. Coloproctol. 2021, 25, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Tønnesen, H. Alcohol abuse and postoperative morbidity. Dan. Med. Bull. 2003, 50, 139–160. [Google Scholar] [PubMed]
- Subramanian, V.; Saxena, S.; Kang, J.-Y.; Pollok, R.C.G. Preoperative Steroid Use and Risk of Postoperative Complications in Patients With Inflammatory Bowel Disease Undergoing Abdominal Surgery. Am. J. Gastroenterol. 2008, 103, 2373–2381. [Google Scholar] [CrossRef] [PubMed]
- Waeckel, L.; Venet, F.; Gossez, M.; Monard, C.; Rimmelé, T.; Monneret, G. Study of monocytic myeloid-derived suppressor cells and CD4 lymphopenia in septic shock-induced immunosuppression. Ann. Biol. Clin. 2021, 79, 17–27. [Google Scholar] [CrossRef]
- Szalewski, D.A.; Hinrichs, V.S.; Zinniel, D.K.; Barletta, R.G. The pathogenicity of Aspergillus fumigatus, drug resistance, and nanoparticle delivery. Can. J. Microbiol. 2018, 64, 439–453. [Google Scholar] [CrossRef] [Green Version]
- Davila, M.L. Neutropenic enterocolitis. Curr. Opin. Intern. Med. 2006, 5, 194–197. [Google Scholar] [CrossRef]
- Saillard, C.; Zafrani, L.; Darmon, M.; Bisbal, M.; Chow-Chine, L.; Sannini, A.; Brun, J.-P.; Ewald, J.; Turrini, O.; Faucher, M.; et al. The prognostic impact of abdominal surgery in cancer patients with neutropenic enterocolitis: A systematic review and meta-analysis, on behalf the Groupe de Recherche en Réanimation Respiratoire du patient d’Onco-Hématologie (GRRR-OH). Ann. Intensive Care 2018, 8, 47. [Google Scholar] [CrossRef] [Green Version]
- Wade, D.S.; Nava, H.R.; Douglass, H.O. Neutropenic enterocolitis. Clinical diagnosis and treatment. Cancer 1992, 69, 17–23. [Google Scholar] [CrossRef]
- Sloas, M.M.; Flynn, P.M.; Kaste, S.C.; Patrick, C.C. Typhlitis in Children with Cancer: A 30-Year Experience. Clin. Infect. Dis. 1993, 17, 484–490. [Google Scholar] [CrossRef]
- Gorschluter, M.; Mey, U.; Strehl, J.; Ziske, C.; Schepke, M.; Schmidt-Wolf, I.G.H.; Sauerbruch, T.; Glasmacher, A. Neutropenic enterocolitis in adults: Systematic analysis of evidence quality. Eur. J. Haematol. 2005, 75, 1–13. [Google Scholar] [CrossRef]
- Katz, J.A.; Wagner, M.L.; Gresik, M.V.; Mahoney, D.H.; Fernbach, D.J. Typhlitis. An 18-year experience and postmortem review. Cancer 1990, 65, 1041–1047. [Google Scholar] [CrossRef]
- Portugal, R.; Nucci, M. Typhlitis (neutropenic enterocolitis) in patients with acute leukemia: A review. Expert Rev. Hematol. 2017, 10, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Bourcier, S.; Oudjit, A.; Goudard, G.; Charpentier, J.; Leblanc, S.; Coriat, R.; Gouya, H.; Dousset, B.; Mira, J.-P.; Pène, F. Diagnosis of non-occlusive acute mesenteric ischemia in the intensive care unit. Ann. Intensive Care 2016, 6, 112. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Tsukahara, K.; Okamoto, I.; Kojima, R.; Hirasawa, K.; Sato, H. A Case of Septicemia due to Nonocclusive Mesenteric Ischemia Occurring in Induction Chemotherapy. Case Rep. Otolaryngol. 2018, 2018, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trompeter, M.; Brazda, T.; Remy, C.T.; Vestring, T.; Reimer, P. Non-occlusive mesenteric ischemia: Etiology, diagnosis, and interventional therapy. Eur. Radiol. 2002, 12, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Bala, M.; Kashuk, J.; Moore, E.E.; Kluger, Y.; Biffl, W.; Gomes, C.A.; Ben-Ishay, O.; Rubinstein, C.; Balogh, Z.J.; Civil, I.; et al. Acute mesenteric ischemia: Guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. 2017, 12, 38. [Google Scholar] [CrossRef] [Green Version]
- Schneider, C.; von Aulock, S.; Zedler, S.; Schinkel, C.; Hartung, T.; Faist, E. Perioperative recombinant human granulocyte colony-stimulating factor (Filgrastim) treatment prevents immunoinflammatory dysfunction associated with major surgery. Ann. Surg. 2004, 239, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, H.; Engert, A.; Grass, G.; Mansmann, G.; Wassmer, G.; Hubel, K.; Loehlein, D.; Ulrich, B.C.; Lippert, H.; Knoefel, W.T.; et al. Perioperative Granulocyte Colony-Stimulating Factor Does Not Preent Severe Infections in Patients Undergoing Esophagectomy for Esophageal Cancer. Ann. Surg. 2004, 240, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Nakano, Y.; Okutani, R. Perioperative management for a patient with chronic pancytopenia: A case of aplastic anemia with persistent neutropenia following preoperative administration of G-CSF. J. Anesth. 2010, 24, 268–271. [Google Scholar] [CrossRef]
- Pedroso-Fernandez, Y.; Aguirre-Jaime, A.; Ramos, M.J.; Hernández, M.; Cuervo, M.; Bravo, A.; Carrillo, A. Prediction of surgical site infection after colorectal surgery. Am. J. Infect. Control 2016, 44, 450–454. [Google Scholar] [CrossRef]
- Boev, C.; Kiss, E. Hospital-Acquired Infections. Crit. Care Nurs. Clin. N. Am. 2017, 29, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Owens, C.D.; Stoessel, K. Surgical site infections: Epidemiology, microbiology and prevention. J. Hosp. Infect. 2008, 70, 3–10. [Google Scholar] [CrossRef]
- Horan, T.C.; Gaynes, R.P.; Martone, W.J.; Jarvis, W.R.; Emori, T.G. CDC definitions of nosocomial surgical site infections, 1992: A modification of CDC definitions of surgical wound infections. Infect. Control Hosp. Epidemiol. 1992, 13, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Lederer, A.-K.; Chikhladze, S.; Kohnert, E.; Huber, R.; Müller, A. Current Insights: The Impact of Gut Microbiota on Postoperative Complications in Visceral Surgery—A Narrative Review. Diagnostics 2021, 11, 2099. [Google Scholar] [CrossRef] [PubMed]
- Mueck, K.M.; Kao, L.S. Patients at High-Risk for Surgical Site Infection. Surg. Infect. 2017, 18, 440–446. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Type | Cells Per µL Blood | Chemotherapy-Induced * |
|---|---|---|
| >1500 | Grade I | |
| Mild | 1000–1500 | Grade II |
| Moderate | 500–1000 | Grade III |
| Severe | <500 | Grade IV |
| Author | Ref. | Year | Study Type | N * | Type of Surgery | Disease | Results ° |
|---|---|---|---|---|---|---|---|
| Wade et al. | [20] | 1990 | Retrospective | 17 | Emergency | Hematologic | Mortality 41% |
| Nishida et al. | [23] | 1996 | Pilot trial | 8/23 | Emergency | Perforation | Mortality 13% vs. 65% + |
| Hansen et al. | [24] | 1998 | Retrospective | 105 | Emergency | Diverticulitis | Predictor for death |
| Sullivan et al. | [25] | 2012 | Retrospective | 956/956 | Emergency | Diverse | Predictor for death |
| Sudarshan et al. | [26] | 2015 | Retrospective | 527 | Emergency | Diverse | Predictor for death and complications |
| Gulack et al. | [27] | 2015 | Retrospective | 2057/18386 | Emergency | Diverse | Predictor for death |
| Mokart et al. | [28] | 2017 | Retrospective | 17/58 | Emergency | Hematologic | No association |
| Joo et al. | [29] | 2020 | Retrospective | 12/79 | Emergency | Colonic perforation | Predictor for death |
| Fokstuen et al. | [30] | 2009 | Retrospective | 274 | Elective | Rectal cancer | No association |
| Reim et al. | [31] | 2010 | Retrospective | 58/156 | Elective | Gastric cancer | No association |
| Bamba et al. | [32] | 2014 | Retrospective | 33/66 | Elective | Diverse | Association to an early port infection |
| Ohira et al. | [33] | 2015 | Retrospective | 44 | Elective | Esophageal cancer | No association |
| Pluta et al. | [34] | 2018 | Retrospective | 101 | Elective | Diverse | No association |
| Chen et al. | [35] | 2019 | Retrospective | 141 | Elective | Liver metastases | Predictor for major complications |
| Grant et al. | [36] | 2020 | Retrospective | 891/3493 | Elective | Malignant disease | No association |
| Hara et al. | [37] | 2021 | Retrospective | 52/100 | Elective | Esophageal cancer | No association |
| Zarain-Obrador et al. | [38] | 2021 | Retrospective | 1727 | Elective | Colorectalsurgery | Risk factor for surgical site infection |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lederer, A.-K.; Bartsch, F.; Moehler, M.; Gaßmann, P.; Lang, H. Morbidity and Mortality of Neutropenic Patients in Visceral Surgery: A Narrative Review. Cells 2022, 11, 3314. https://doi.org/10.3390/cells11203314
Lederer A-K, Bartsch F, Moehler M, Gaßmann P, Lang H. Morbidity and Mortality of Neutropenic Patients in Visceral Surgery: A Narrative Review. Cells. 2022; 11(20):3314. https://doi.org/10.3390/cells11203314
Chicago/Turabian StyleLederer, Ann-Kathrin, Fabian Bartsch, Markus Moehler, Peter Gaßmann, and Hauke Lang. 2022. "Morbidity and Mortality of Neutropenic Patients in Visceral Surgery: A Narrative Review" Cells 11, no. 20: 3314. https://doi.org/10.3390/cells11203314