
Current State of the Art and Next Generation of Materials for a Customized IntraOcular Lens according to a Patient-Specific Eye Power
 ,
,  , , ,
, , , 
Abstract
:
1. Introduction
2. IOLs Material Market
2.1. Silicone
2.2. Acrylic Materials for IOLs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Refractive Index | Water Content | Flexibility |
|---|---|---|---|
| MMA | 1.49 | <1% | rigid |
| PEA/PEMA | 1.55 | <1% | foldable |
| EA/EMA/TFEMA | 1.47 | <1% | foldable |
| HEMA/MMA | 1.47 | 20% | foldable |
| HEXMA/HEMA | 1.47 | 18% | foldable |
| HEMA | 1.44 | 38% | foldable |
2.2.1. Hydrophobic Acrylic Materials
2.2.2. Hydrophilic Acrylic Materials
2.2.3. Innovative Hybrid and Flexible Polymeric Materials
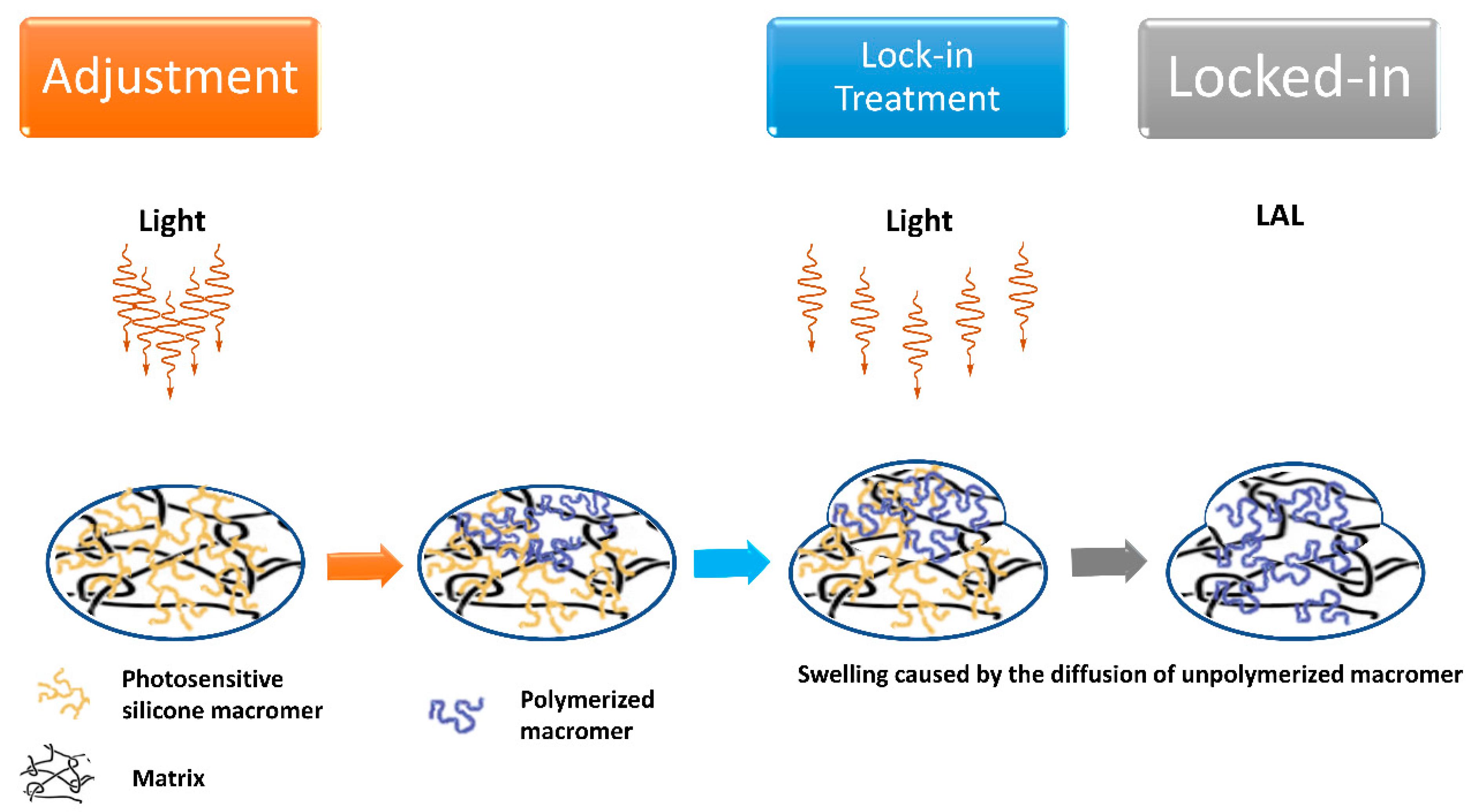
2.3. Advanced Materials for Injectable, Shape Memory, and Adjustable IOL
2.4. Variable Refractive Index Materials for IOLs
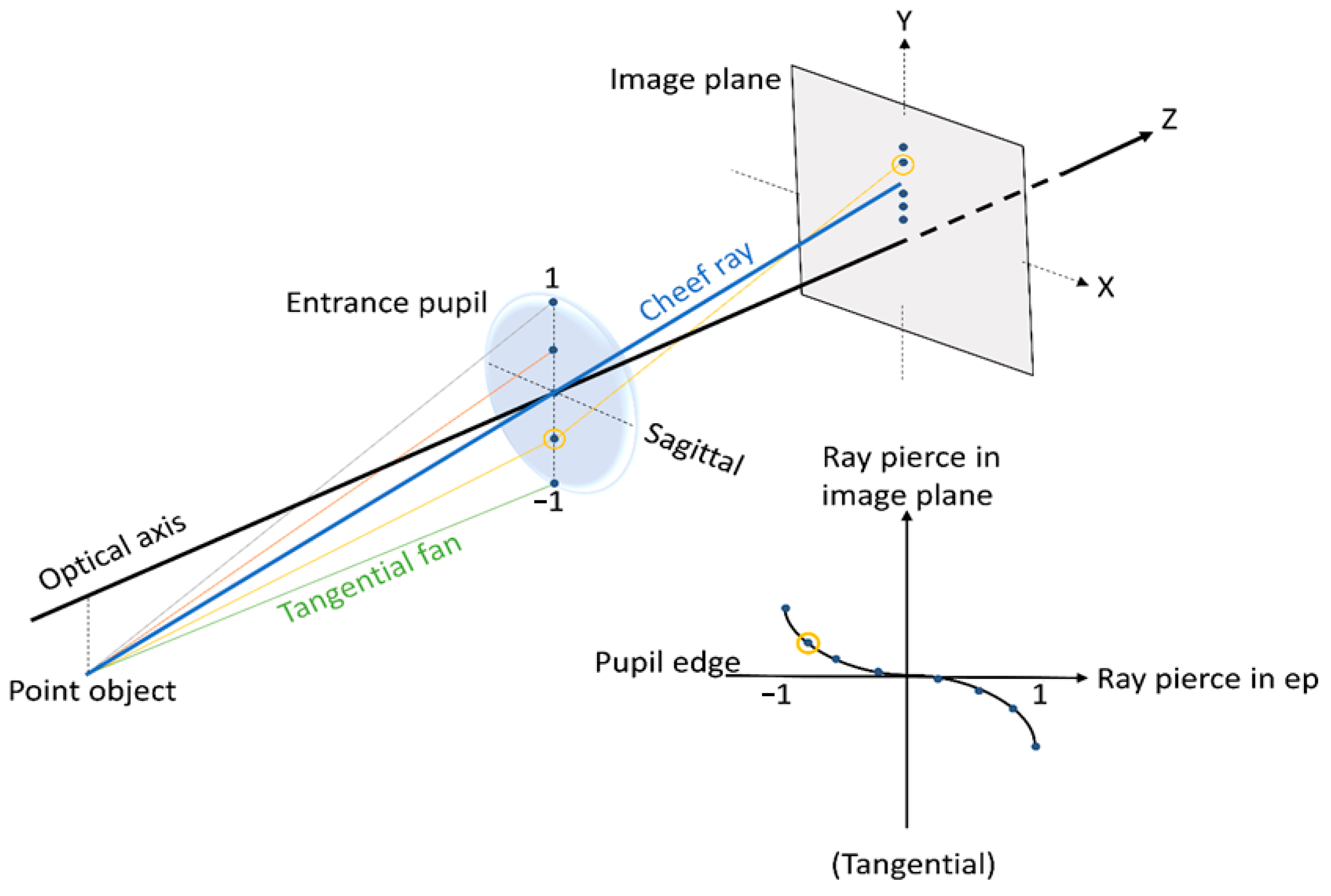
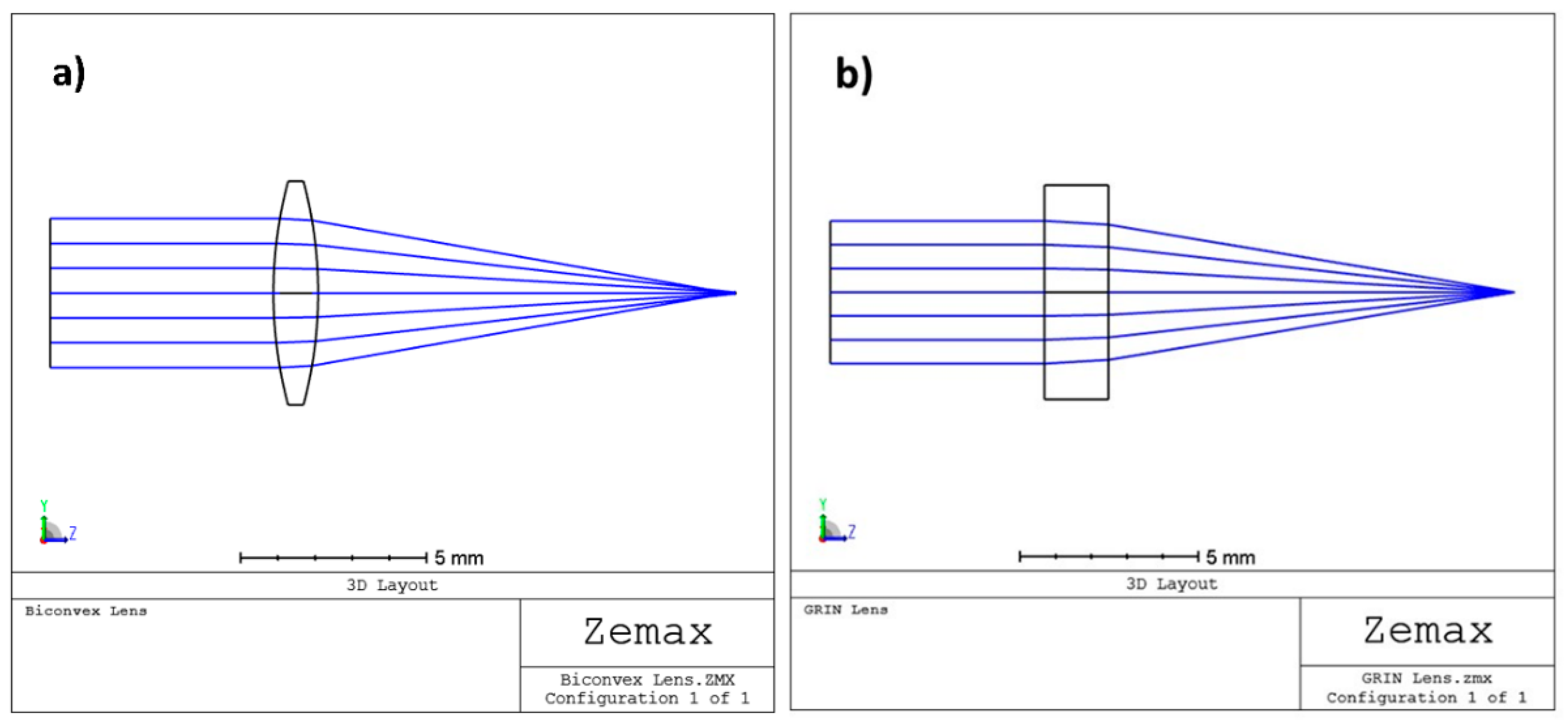
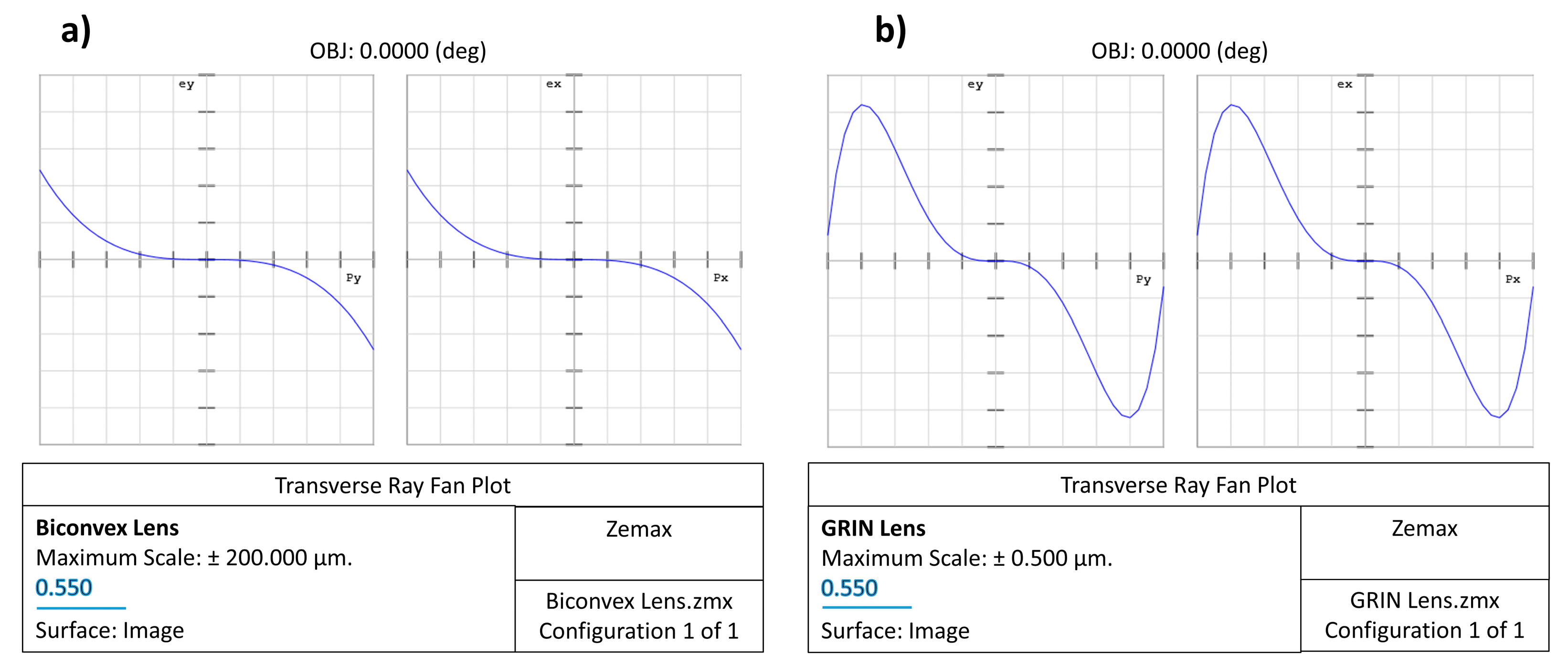
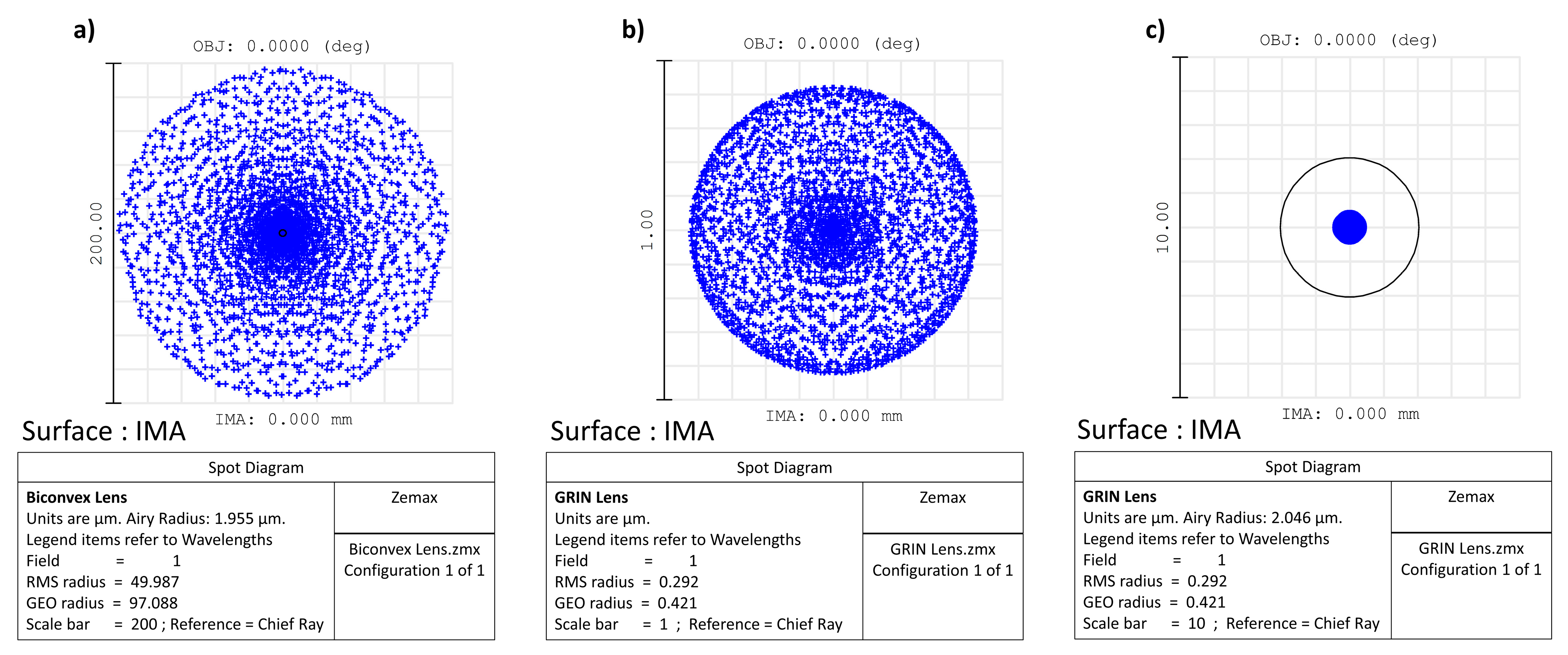
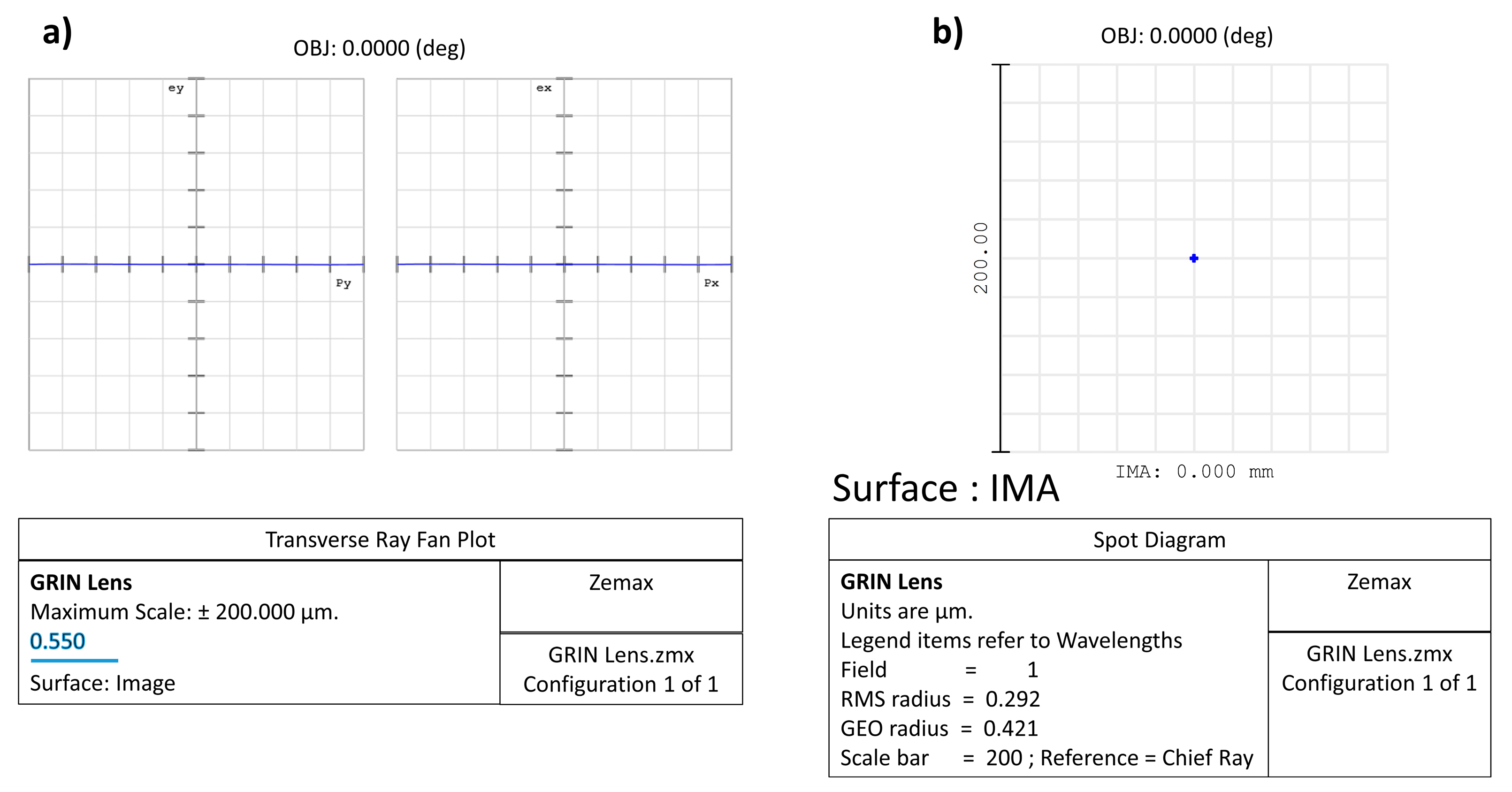
2.5. Zemax Simulation Data: Comparison between Two Lenses (One Biconvex and One GRIN)
3. IOL-Based Materials Characterization and Tests of Entire IOLs
3.1. Physico-Chemical Characterization
3.1.1. Contact Angle Analyses
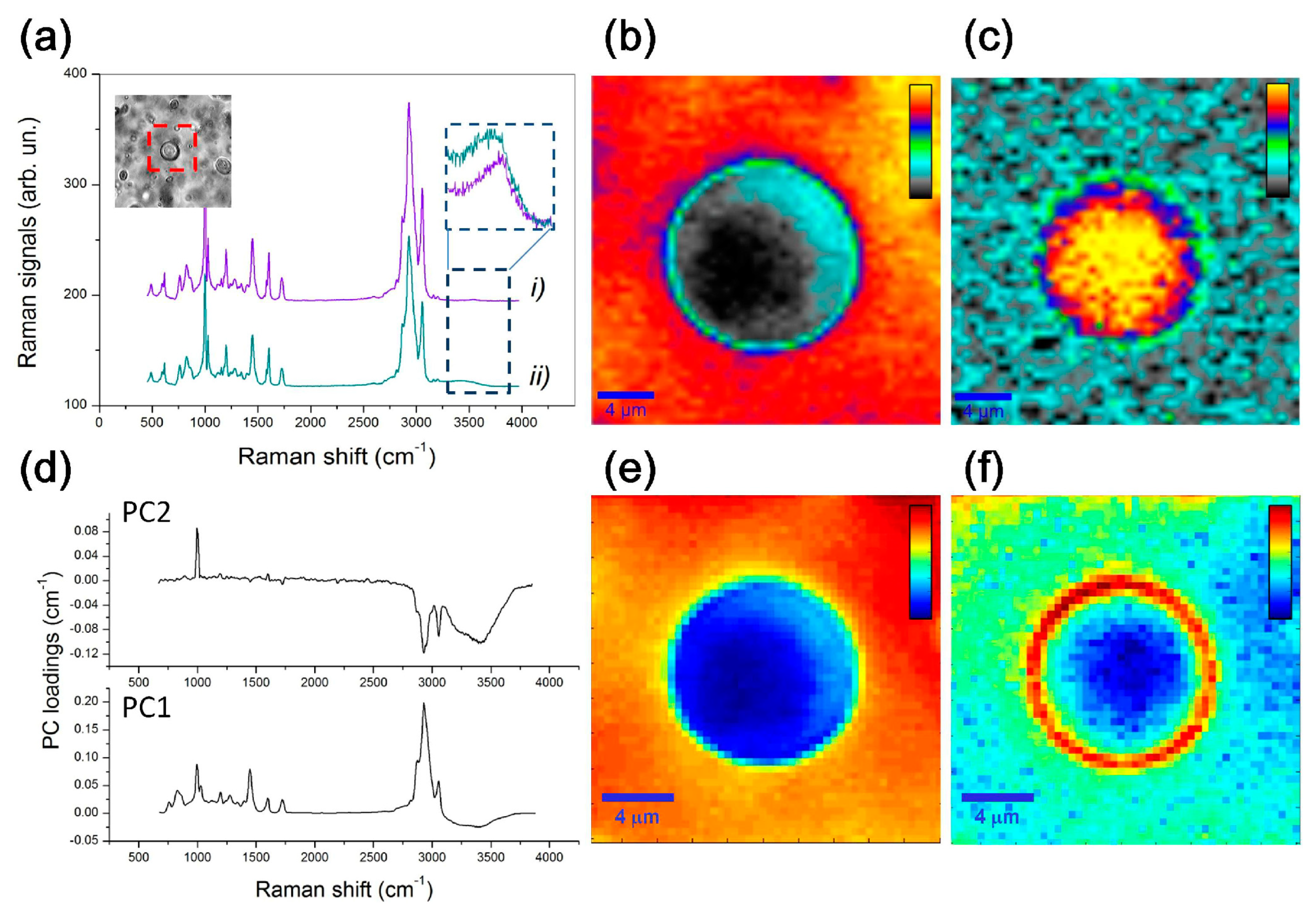
3.1.2. Vibrational Spectroscopic and Morphological Characterizations
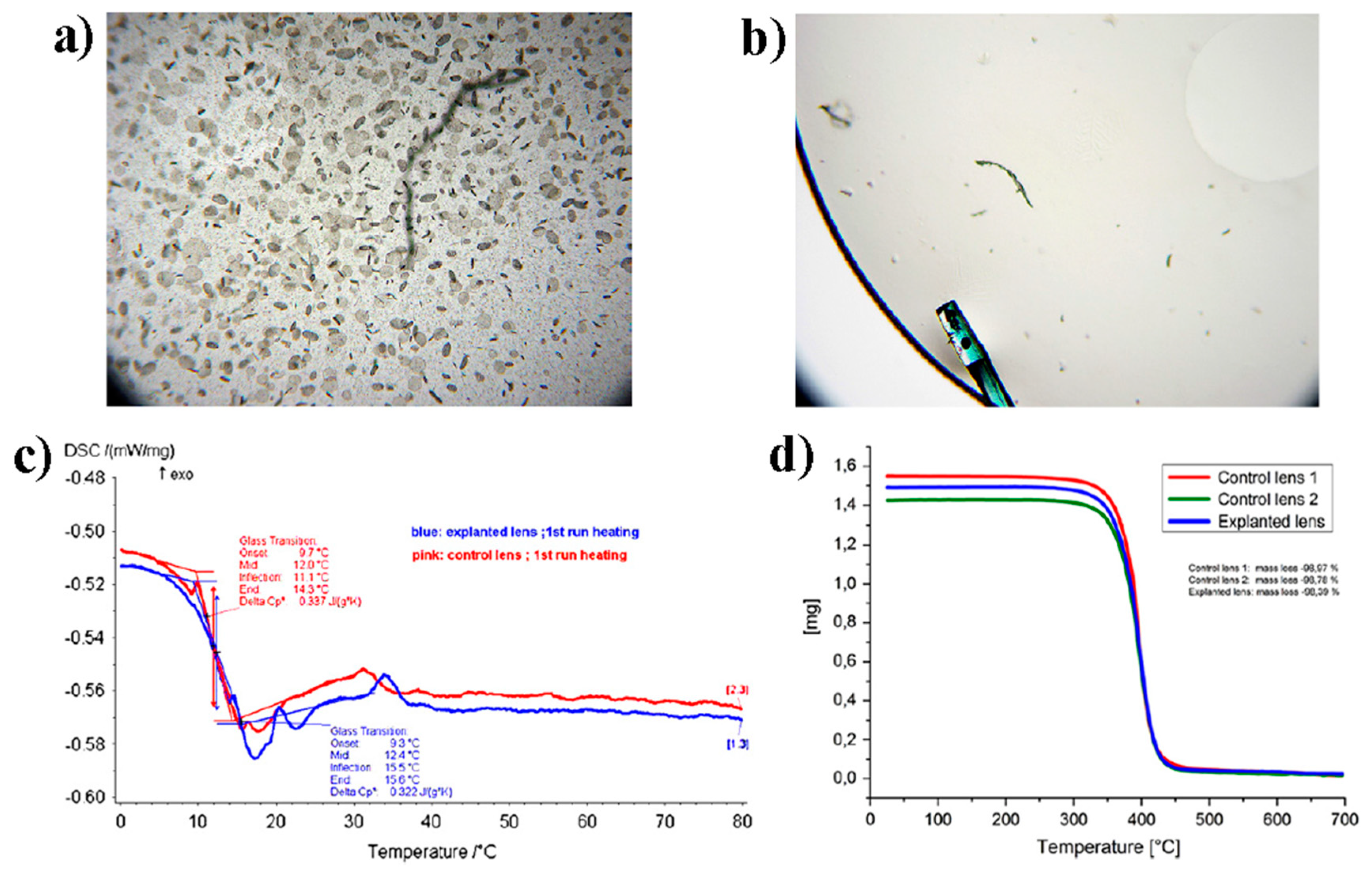
3.1.3. Mechanical and Thermomechanical Tests
3.2. Biocompatibility
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- National Eye Institute. Cataracts. Available online: https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/cataracts (accessed on 2 February 2023).
- Luo, C.; Wang, H.; Chen, X.; Xu, J.; Yin, H.; Yao, K. Recent Advances of Intraocular Lens Materials and Surface Modification in Cataract Surgery. Front. Bioeng. Biotechnol. 2022, 10, 913383. [Google Scholar] [CrossRef]
- de Groot, J.H.; van Beijma, F.J.; Haitjema, H.J.; Dillingham, K.A.; Hodd, K.A.; Koopmans, S.A.; Norrby, S. Injectable Intraocular Lens Materials Based upon Hydrogels. Biomacromolecules 2001, 2, 628–634. [Google Scholar] [CrossRef]
- Assia, E.I.; Blumenthal, M.; Apple, D.J. Effect of Expandable Full-Size Intraocular Lenses on Lens Centration and Capsule Opacification in Rabbits. J. Cataract Refract. Surg. 1999, 25, 347–356. [Google Scholar] [CrossRef]
- Song, L.; Hu, W.; Wang, G.; Zhang, H.; Niu, G.; Cao, H.; Yang, H.; Zhu, S. Synthesis and Characterization of Shape Memory (Meth)Acrylate Co-Polymers and Their Cytocompatibility In Vitro. J. Biomater. Sci. Polym. Ed. 2011, 22, 1–17. [Google Scholar] [CrossRef]
- Ford, J.; Werner, L.; Mamalis, N. Adjustable Intraocular Lens Power Technology. J. Cataract Refract. Surg. 2014, 40, 1205–1223. [Google Scholar] [CrossRef]
- Werner, L.; Chang, W.; Haymore, J.; Haugen, B.; Romaniv, N.; Sandstedt, C.; Chang, S.; Mamalis, N. Retinal Safety of the Irradiation Delivered to Light-Adjustable Intraocular Lenses Evaluated in a Rabbit Model. J. Cataract Refract. Surg. 2010, 36, 1392–1397. [Google Scholar] [CrossRef]
- Bille, J.F.; Engelhardt, J.; Volpp, H.-R.; Laghouissa, A.; Motzkus, M.; Jiang, Z.; Sahler, R. Chemical Basis for Alteration of an Intraocular Lens Using a Femtosecond Laser. Biomed. Opt. Express 2017, 8, 1390–1404. [Google Scholar] [CrossRef] [Green Version]
- Zhong, X.; Long, E.; Chen, W.; Xiang, W.; Liu, Z.; Chen, H.; Chen, J.; Lin, Z.; Lin, H.; Chen, W. Comparisons of the In-the-Bag Stabilities of Single-Piece and Three-Piece Intraocular Lenses for Age-Related Cataract Patients: A Randomized Controlled Trial. BMC Ophthalmol. 2016, 16, 100. [Google Scholar] [CrossRef] [Green Version]
- Zvorničanin, J.; Zvorničanin, E. Premium Intraocular Lenses: The Past, Present and Future. J. Curr. Ophthalmol. 2018, 30, 287–296. [Google Scholar] [CrossRef]
- Roach, L.; Pepose, J.S.; Santhiago, M.R.; Waring, G.O. Centration of IOLs: Challenges, Variables, and Advice for Optimal Outcomes. Available online: https://www.aao.org/eyenet/article/centration-of-iols-challenges-variables-advice-opt (accessed on 2 February 2023).
- Wang, L.; Houser, K.; Koch, D.D. Intraocular Lens Power Calculations. In Ophthalmology; Yanoff, M., Duker, J.S., Eds.; Elsevier: Edinburgh, UK, 2019; ISBN 9780323528214. [Google Scholar]
- Werner, L. Intraocular Lenses. Ophthalmology 2021, 128, e74–e93. [Google Scholar] [CrossRef]
- Megiddo-Barnir, E.; Alió, J.L. Latest Development in Extended Depth-of-Focus Intraocular Lenses: An Update. Asia-Pac. J. Ophthalmol. 2023, 12, 58–79. [Google Scholar] [CrossRef]
- Sánchez-González, J.-M.; Sánchez-González, M.C.; De-Hita-Cantalejo, C.; Ballesteros-Sánchez, A. Small Aperture IC-8 Extended-Depth-of-Focus Intraocular Lens in Cataract Surgery: A Systematic Review. J. Clin. Med. 2022, 11, 4654. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Vives, C. Biomaterial Influence on Intraocular Lens Performance: An Overview. J. Ophthalmol. 2018, 2018, 2687385. [Google Scholar] [CrossRef] [Green Version]
- Thomes, B.E.; Callaghan, T.A. Evaluation of in Vitro Glistening Formation in Hydrophobic Acrylic Intraocular Lenses. Clin. Ophthalmol. 2013, 7, 1529–1534. [Google Scholar] [CrossRef] [Green Version]
- Dhital, A.; Spalton, D.J.; Goyal, S.; Werner, L. Calcification in Hydrophilic Intraocular Lenses Associated with Injection of Intraocular Gas. Am. J. Ophthalmol. 2012, 153, 1154–1160. [Google Scholar] [CrossRef]
- Oshika, T. Influence of Glistenings on the Optical Quality of Acrylic Foldable Intraocular Lens. Br. J. Ophthalmol. 2001, 85, 1034–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.; Mainster, M.A. The Effect of Chromatic Dispersion on Pseudophakic Optical Performance. Br. J. Ophthalmol. 2007, 91, 1225–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinchuk, L. The Use of Polyisobutylene-Based Polymers in Ophthalmology. Bioact. Mater. 2022, 10, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Werner, L. Glistenings and Surface Light Scattering in Intraocular Lenses. J. Cataract Refract. Surg. 2010, 36, 1398–1420. [Google Scholar] [CrossRef] [PubMed]
- Tetz, M.; Jorgensen, M.R. New Hydrophobic IOL Materials and Understanding the Science of Glistenings. Curr. Eye Res. 2015, 40, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Liu, H.; Long Gu, F.; Wu, M.-X.; Wang, Y. The Molecular Design of Performance-Enhanced Intraocular Lens Composites. Biomater. Sci. 2022, 10, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Nagata, T.; Kubota, S.; Watanabe, I.; Aoshima, S. Chromatic Aberration in Pseudophakic Eyes. Nippon Ganka Gakkai Zasshi 1999, 103, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.; Atchison, D.A. The Eye and Visual Optical Instruments; Cambridge University Press: Cambridge, UK, 1996; ISBN 9780521472524. [Google Scholar]
- Jellali, R.; Alexandre, M.; Jérôme, C. Photosensitive Polydimethylsiloxane Networks for Adjustable-Patterned Films. Polym. Chem. 2017, 8, 2499–2508. [Google Scholar] [CrossRef]
- Teshigawara, T.; Meguro, A.; Mizuki, N. Relationship between Postoperative Intraocular Lens Shift and Postoperative Refraction Change in Cataract Surgery Using Three Different Types of Intraocular Lenses. Ophthalmol. Ther. 2021, 10, 989–1002. [Google Scholar] [CrossRef]
- Shimizu, K.; Kobayashi, K.; Takayama, S.; Zhaobin, G. Preloaded Injector for Intraocular Lens Implantation without the Use of Ophthalmic Viscosurgical Devices. J. Cataract Refract. Surg. 2008, 34, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, M.; Dick, H.B.; Wolters, B.; Pakula, T.; Wolf, E. Material Properties of Various Intraocular Lenses in an Experimental Study. Ophthalmologica 2004, 218, 57–63. [Google Scholar] [CrossRef]
- Li, N.; Chen, X.; Zhang, J.; Zhou, Y.; Yao, X.; Du, L.; Wei, M.; Liu, Y. Effect of AcrySof versus Silicone or Polymethyl Methacrylate Intraocular Lens on Posterior Capsule Opacification. Ophthalmology 2008, 115, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Bozukova, D.; Pagnoulle, C.; Jérôme, R.; Jérôme, C. Polymers in Modern Ophthalmic Implants—Historical Background and Recent Advances. Mater. Sci. Eng. R Rep. 2010, 69, 63–83. [Google Scholar] [CrossRef]
- Wei, Y.; Chen, Y.; Liu, P.; Gao, Q.; Sun, Y.; Huang, C. Surface Modification of Hydrophobic PMMA Intraocular Lens by the Immobilization of Hydroxyethyl Methacrylate for Improving Application in Ophthalmology. Plasma Chem. Plasma Process. 2011, 31, 811–825. [Google Scholar] [CrossRef]
- Kohnen, T. The Variety of Foldable Intraocular Lens Materials. J. Cataract Refract. Surg. 1996, 22, 1255–1258. [Google Scholar] [CrossRef]
- Bellucci, R. An Introduction to Intraocular Lenses: Material, Optics, Haptics, Design and Aberration. In Cataract. ESASO Course Series; Güell, J.L., Ed.; Karger: Basel, Switzerland, 2013; Volume 3, pp. 38–55. [Google Scholar]
- Lee, H.; Tae, G.; Kim, Y.H. A Study on the Copolymerization Kinetics of Phenylethyl Acrylate and Phenylethyl Methacrylate. Macromol. Res. 2008, 16, 614–619. [Google Scholar] [CrossRef]
- Parra Ruiz, F.J.; Vazquez Lasa, B.; San Roman Del Barrio, J. Hydrophilic Acrylic Systems with a High Refractive Index for Producing Intraocular Lenses. WO/2010/109043, 30 September 2010. [Google Scholar]
- Murthy, K.S.; Ravi, N. Hydrogels as Potential Probes for Investigating the Mechanism of Lenticular Presbyopia. Curr. Eye Res. 2001, 22, 384–393. [Google Scholar] [CrossRef]
- Hoffman, A.S. Hydrogels for Biomedical Applications. Ann. N. Y. Acad. Sci. 2001, 944, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Tripti, D.; Haldar, R.S.; Geetha, S.; Niyogi, U.K.; Khandal, R.K. Materials for Intraocular Lenses (IOLs): Review of Developments to Achieve Biocompatibility. e-Polymers 2009, 9, 1466. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, P.; González-Méijome, J.M.; Madrid-Costa, D.; Ferrer-Blasco, T.; Jorge, J.; Montés-Micó, R. Implantable Collamer Posterior Chamber Intraocular Lenses: A Review of Potential Complications. J. Refract. Surg. 2011, 27, 765–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seward, H.C. Folding Intraocular Lenses: Materials and Methods. Br. J. Ophthalmol. 1997, 81, 340–341. [Google Scholar] [CrossRef] [Green Version]
- Bellone, A. Mini Well Ready Iol. Available online: https://albertobellone.it/en/mini-well-ready-iol-sifi-medtech/ (accessed on 3 February 2023).
- Rusciano, G.; Capaccio, A.; Pesce, G.; Sasso, A. Experimental Study of the Mechanisms Leading to the Formation of Glistenings in Intraocular Lenses by Raman Spectroscopy. Biomed. Opt. Express 2019, 10, 1870–1881. [Google Scholar] [CrossRef]
- Werner, L.; Legeais, J.-M.; Nagel, M.-D.; Renard, G. Evaluation of Teflon-Coated Intraocular Lenses in an Organ Culture Method. J. Biomed. Mater. Res. 1999, 46, 347–354. [Google Scholar] [CrossRef]
- Ratner, B.D.; Mateo, N.B. Polymeric Intraocular Lens Material Having Improved Surface Properties 1987. EP0238508A1, 30 September 1987. [Google Scholar]
- Lee, H.I.; Kim, M.K.; Ko, J.H.; Lee, H.J.; Wee, W.R.; Lee, J.H. The Efficacy of an Acrylic Intraocular Lens Surface Modified with Polyethylene Glycol in Posterior Capsular Opacification. J. Korean Med. Sci. 2007, 22, 502–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, A.S.; Patel, A.S.; Llanos, G. Polyethylene Oxide Coated Intraocular Lens. U.S. Patent US5618316A, 8 April 1997. [Google Scholar]
- Bozukova, D.; Pagnoulle, C.; De Pauw-Gillet, M.-C.; Desbief, S.; Lazzaroni, R.; Ruth, N.; Jérôme, R.; Jérôme, C. Improved Performances of Intraocular Lenses by Poly(ethylene glycol) Chemical Coatings. Biomacromolecules 2007, 8, 2379–2387. [Google Scholar] [CrossRef] [PubMed]
- Bozukova, D.; Pagnoulle, C.; De Pauw-Gillet, M.-C.; Ruth, N.; Jérôme, R.; Jérôme, C. Imparting Antifouling Properties of Poly(2-hydroxyethyl methacrylate) Hydrogels by Grafting Poly(oligoethylene glycol methyl ether acrylate). Langmuir 2008, 24, 6649–6658. [Google Scholar] [CrossRef]
- Tognetto, D.; Toto, L.; Minutola, D.; Ballone, E.; di Nicola, M.; Di Mascio, R.; Ravalico, G. Hydrophobic Acrylic versus Heparin Surface-Modified Polymethylmethacrylate Intraocular Lens: A Biocompatibility Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2003, 241, 625–630. [Google Scholar] [CrossRef]
- Larsson, R.; Selen, G.; Bjorklund, H.; Fagerholm, P. Intraocular PMMA Lenses Modified with Surface-Immobilized Heparin: Evaluation of Biocompatibility In Vitro and In Vivo. Biomaterials 1989, 10, 511–516. [Google Scholar] [CrossRef] [PubMed]
- González-Chomón, C.; Concheiro, A.; Alvarez-Lorenzo, C. Drug-Eluting Intraocular Lenses. Materials 2011, 4, 1927–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Schickhardt, S.; Fang, H.; Auerbach, F.; Cagampang, P.; Merz, P.R.; Auffarth, G.U. Comparison of a New IOL Injector System against 3 Standard IOL Injector Systems with Different Incision Sizes: Miyake-Apple View Experimental Laboratory Study. J. Cataract Refract. Surg. 2022, 48, 230–237. [Google Scholar] [CrossRef]
- Cabeza-Gil, I.; Ríos-Ruiz, I.; Calvo, B. Experimental Evaluation of the Injection Force Exerted in Intraocular Lens Delivery with Syringe-Type Injectors. J. Mech. Behav. Biomed. Mater 2021, 124, 104793. [Google Scholar] [CrossRef] [PubMed]
- Lendlein, A.; Kelch, S. Shape-Memory Polymers. Angew. Chem. Int. Ed. 2002, 41, 2034–2057. [Google Scholar] [CrossRef]
- Oh, W.T.; Lee, J.B.; Choi, W.; Bae, H.W.; Kim, C.S.; Kim, C.Y.; Sung, H.-J. Shape Memory Tube Plug for Fine-Control of Intraocular Pressure by Glaucoma Devices. ACS Biomater Sci. Eng. 2020, 6, 3784–3790. [Google Scholar] [CrossRef]
- El Feninat, F.; Laroche, G.; Fiset, M.; Mantovani, D. Shape Memory Materials for Biomedical Applications. Adv. Eng. Mater. 2002, 4, 91–104. [Google Scholar] [CrossRef]
- Kimura, W.; Kimura, T.; Sawada, T.; Kikuchi, T.; Toda, H.; Yamada, Y.; Nagai, H. Comparison of Shape Recovery Ratios in Various IOL Haptics. Nippon Ganka Gakkai Zasshi 1991, 95, 548–555. [Google Scholar]
- Scholl, J.; Smiley, T.; Smith, D.J.; Burns, D.H.; Cheskin, B. Accommodating Intraocular Lens System Having Circumferential Haptic Support and Method. U.S. Patent US20070203578A1, 29 January 2013. [Google Scholar]
- Kahook, M.Y.; Mandava, N.; Shandas, R.; Rech, B.; Lowery, M.D.; Urbaniak, D. Shape Memory Polymer Intraocular Lenses. U.S. Patent US20140172094A1, 19 June 2014. [Google Scholar]
- Patadiya, J.; Gawande, A.; Joshi, G.; Kandasubramanian, B. Additive Manufacturing of Shape Memory Polymer Composites for Futuristic Technology. Ind. Eng. Chem. Res. 2021, 60, 15885–15912. [Google Scholar] [CrossRef]
- Lichtinger, A. The Light Adjustable Lens—A Review. Eur. Ophthalmic Rev. 2012, 6, 108–111. [Google Scholar] [CrossRef] [Green Version]
- Light-Adjustable IOLs & Cataracts with Unusual Corneas. Available online: https://ophthalmologybreakingnews.com/ophthalmologynews-light-adjustable-iols-cataractsunusualcorneas (accessed on 2 February 2023).
- RxSight Inc. Summary of Safety and Effectiveness Data (SSED). Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160055B.pdf (accessed on 2 February 2023).
- Chang, D.F. Disruptive Innovation and Refractive IOLs: How the Game Will Change with Adjustable IOLs. Asia-Pac. J. Ophthalmol. 2019, 8, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Schojai, M.; Schultz, T.; Schulze, K.; Hengerer, F.H.; Dick, H.B. Long-Term follow-up and Clinical Evaluation of the Light-Adjustable Intraocular Lens Implanted after Cataract Removal: 7-Year Results. J. Cataract Refract. Surg. 2020, 46, 8–13. [Google Scholar] [PubMed]
- Fernandez, E.J.; Artal, P. Achromatic Doublet Intraocular Lens for Full Aberration Correction. Biomed. Opt. Express 2017, 8, 2396–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malyugin, B.; Morozova, T.; Cherednik, V. Gradient Refractive Index Optics IOL: Theoretical Background and Clinical Results. MEAJO Middle East Afr. J. Ophthalmol. 2014, 21. [Google Scholar] [CrossRef] [PubMed]
- Pierscionek, B.K.; Regini, J.W. The Gradient Index Lens of the Eye: An Opto-Biological Synchrony. Prog. Retin. Eye Res. 2012, 31, 332–349. [Google Scholar] [CrossRef]
- Ruan, X.; Liu, Z.; Luo, L.; Liu, Y. The Structure of the Lens and Its Associations with the Visual Quality. BMJ Open Ophthalmol. 2020, 5, e000459. [Google Scholar] [CrossRef]
- Liu, Y.-J.; Wang, Z.-Q.; Song, L.-P.; Mu, G.-G. An Anatomically Accurate Eye Model with a Shell-Structure Lens. Optik 2005, 116, 241–246. [Google Scholar] [CrossRef]
- Navarro, R. The Optical Design of the Human Eye: A Critical Review. J. Optom. 2009, 2, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.-C.; Mesquita, G.M.; Williams, S.; Gregori, G.; Cabot, F.; Ho, A.; Ruggeri, M.; Yoo, S.H.; Parel, J.-M.; Manns, F. In Vivo Measurement of the Human Crystalline Lens Equivalent Refractive Index Using Extended-Depth OCT. Biomed. Opt. Express 2019, 10. [Google Scholar] [CrossRef]
- Feng, Y.; Lin, Y.; Xiong, S.; Xu, X. Electromagnetic Wave Lenses and Reflectors Designed with Transformation Electromagnetics. In Proceedings of the 2014 XXXIth URSI General Assembly and Scientific Symposium (URSI GASS), Beijing, China, 16–23 August 2014; pp. 1–4. [Google Scholar]
- Ohmi, S.; Sakai, H.; Asahara, Y.; Nakayama, S.; Yoneda, Y.; Izumitani, T. Gradient-Index Rod Lens Made by a Double Ion-Exchange Process. Appl. Opt. 1988, 27. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J.D.; Brooks, D.R.; Wozniak, K.T.; Gandara-Montano, G.A.; Fox, E.G.; Tinkham, K.J.; Butler, S.C.; Zheleznyak, L.A.; Buckley, M.R.; Funkenbusch, P.D.; et al. Manufacturing of Gradient Index Lenses for Ophthalmic Applications. In Proceedings of the Optical Design and Fabrication 2017 (Freeform, IODC, OFT), Denver, CO, USA, 9–13 July 2017; p. OW1B.3. [Google Scholar]
- Pickering, M.A.; Taylor, R.L.; Moore, D.T. Gradient Infrared Optical Material Prepared by a Chemical Vapor Deposition Process. Appl. Opt. 1986, 25. [Google Scholar] [CrossRef]
- Sinai, P. Correction of Optical Aberrations by Neutron Irradiation. Appl. Opt. 1971, 10. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Yin, K.; Mackey, M.; Brister, A.; Ponting, M.; Baer, E. Polymeric Nanolayered Gradient Refractive Index Lenses: Technology Review and Introduction of Spherical Gradient Refractive Index Ball Lenses. Opt. Eng. 2013, 52, 112105. [Google Scholar] [CrossRef]
- Sola, D.; Cases, R. High-Repetition-Rate Femtosecond Laser Processing of Acrylic Intra-Ocular Lenses. Polymers 2020, 12, 242. [Google Scholar] [CrossRef] [Green Version]
- Sahler, R.; Bille, J.F. Refractive Index Shaping: In Vivo Optimization of an Implanted Intraocular Lens (IOL). In High Resolution Imaging in Microscopy and Ophthalmology; Bille, J., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 319–336. [Google Scholar]
- Sahler, R.; Bille, J.F.; Enright, S.; Chhoeung, S.; Chan, K. Creation of a Refractive Lens within an Existing Intraocular Lens Using a Femtosecond Laser. J. Cataract Refract. Surg. 2016, 42, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.S.d.; Carvalho, L.A. Different Schematic Eyes and Their Accuracy to the in Vivo Eye: A Quantitative Comparison Study. Braz. J. Phys. 2007, 37, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Baillif, S.; Baziard-Mouysset, G.; Roques, C.; Baziard, Y.; Kodjikian, L. Calculation of Intraocular Lens Surface Free Energy and Its Components from Contact Angle Measurements. Ophthalmic Res. 2013, 50, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Cunanan, C.M.; Ghazizadeh, M.; Buchen, S.Y.; Knight, P.M. Contact-Angle Analysis of Intraocular Lenses. J. Cataract Refract. Surg. 1998, 24, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Dick, H.B.; Frohn, A.; Augustin, A.J.; Wolters, B.; Pakula, T.; Pfeiffer, N. Physicochemical Surface Properties of Various Intraocular Lenses. Ophthalmic Res. 2001, 33, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Lydon, M.J.; Minett, T.W.; Tighe, B.J. Cellular Interactions with Synthetic Polymer Surfaces in Culture. Biomaterials 1985, 6, 396–402. [Google Scholar] [CrossRef]
- Andrade, J.D.; Hlady, V. Protein Adsorption and Materials Biocompatibility: A Tutorial Review and Suggested Hypotheses; Springer: Berlin/Heidelberg, Germany, 1986; pp. 1–63. [Google Scholar]
- Tanaka, T.; Shigeta, M.; Yamakawa, N.; Usui, M. Cell Adhesion to Acrylic Intraocular Lens Associated with Lens Surface Properties. J. Cataract Refract. Surg. 2005, 31, 1648–1651. [Google Scholar] [CrossRef] [PubMed]
- De Giacinto, C.; Porrelli, D.; Turco, G.; Pastore, M.R.; D’Aloisio, R.; Tognetto, D. Surface Properties of Commercially Available Hydrophobic Acrylic Intraocular Lenses: Comparative Study. J. Cataract Refract. Surg. 2019, 45, 1330–1334. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, H.; Iwamoto, H.; Mukai, K.; Obara, Y. Active Oxygen Processing for Acrylic Intraocular Lenses to Prevent Posterior Capsule Opacification. J. Cataract Refract. Surg. 2006, 32, 1035–1040. [Google Scholar] [CrossRef]
- Owens, D.K.; Wendt, R.C. Estimation of the Surface Free Energy of Polymers. J. Appl. Polym. Sci. 1969, 13, 1741–1747. [Google Scholar] [CrossRef]
- Altay, B.N.; Ma, R.; Fleming, P.D.; Joyce, M.J.; Anand, A.; Chen, T.; Keskin, B.; Maddipatla, D.; Turkani, V.S.; Kotkar, P.R.; et al. Surface Free Energy Estimation: A New Methodology for Solid Surfaces. Adv. Mater. Interfaces 2020, 7, 1901570. [Google Scholar] [CrossRef]
- Zuppolini, S.; Borriello, A.; Pellegrino, M.; Venditto, V.; Ambrosio, L.; Nicolais, L. Potential Contact and Intraocular Lenses Based on Hydrophilic/Hydrophobic Sulfonated Syndiotactic Polystyrene Membranes. J. King Saud Univ. Sci. 2017, 29, 487–493. [Google Scholar] [CrossRef]
- Tarnawska, D.; Balin, K.; Jastrzębska, M.; Talik, A.; Wrzalik, R. Physicochemical Analysis of Sediments Formed on the Surface of Hydrophilic Intraocular Lens after Descemet’s Stripping Endothelial Keratoplasty. Materials 2020, 13, 4145. [Google Scholar] [CrossRef]
- Krajňák, T.; Černá, E.; Šuráňová, M.; Šamořil, T.; Zicha, D.; Vojtová, L.; Čechal, J. Replica-Mold Nanopatterned PHEMA Hydrogel Surfaces for Ophthalmic Applications. Sci. Rep. 2022, 12, 14497. [Google Scholar] [CrossRef]
- Smith, B.T.; Belani, S.; Ho, A.C. Ultraviolet and Near-Blue Light Effects on the Eye. Int. Ophthalmol. Clin. 2005, 45, 107–115. [Google Scholar]
- Mainster, M.A. Spectral Transmittance of Intraocular Lenses and Retinal Damage from Intense Light Sources. Am. J. Ophthalmol. 1978, 85, 167–170. [Google Scholar] [CrossRef]
- Henderson, B.A.; Grimes, K.J. Blue-Blocking IOLs: A Complete Review of the Literature. Surv. Ophthalmol. 2010, 55, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Artigas, J.M.; Felipe, A.; Navea, A.; Artigas, C.; García-Domene, M.C. Spectral Transmittance of Intraocular Lenses under Natural and Artificial Illumination. Ophthalmology 2011, 118, 3–8. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization, G.S. ISO 11979-3:2012; Ophthalmic Implants—Intraocular Lenses—Part 3: Mechanical Properties and Test Methods. Available online: https://www.iso.org/standard/55681.html (accessed on 3 February 2023).
- Remón, L.; Siedlecki, D.; Cabeza-Gil, I.; Calvo, B. Influence of Material and Haptic Design on the Mechanical Stability of Intraocular Lenses by Means of Finite-Element Modeling. J. Biomed. Opt. 2018, 23, 035003. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.; Collins, S.; Das, K.K.; Maass, S.; Thatthamla, I.; Schatz, H.; Van Noy, S.; Jain, R. Evaluation of Intraocular Lens Mechanical Stability. J. Cataract Refract. Surg. 2019, 45, 501–506. [Google Scholar] [CrossRef]
- Gu, X.; Chen, X.; Yang, G.; Wang, W.; Xiao, W.; Jin, G.; Wang, L.; Dai, Y.; Ruan, X.; Liu, Z.; et al. Determinants of Intraocular Lens Tilt and Decentration after Cataract Surgery. Ann. Transl. Med. 2020, 8, 921. [Google Scholar] [CrossRef]
- Bozukova, D.; Pagnoulle, C.; Jérôme, C. Biomechanical and Optical Properties of 2 New Hydrophobic Platforms for Intraocular Lenses. J. Cataract Refract. Surg. 2013, 39, 1404–1414. [Google Scholar] [CrossRef]
- Tortolano, L.; Mrad, O.; Manerlax, K.; Khalfoun, C.; Yousfi, R.; Saunier, J.; Secretan, P.; Yagoubi, N. Comparative Stability of Intraocular Lenses during 2–20 Years of Artificial Aging, Potential Effects in Terms of Biocompatibility. J. Appl. Polym. Sci. 2022, 139, e52752. [Google Scholar] [CrossRef]
- Werner, L.; Storsberg, J.; Mauger, O.; Brasse, K.; Gerl, R.; Müller, M.; Tetz, M. Unusual Pattern of Glistening Formation on a 3-Piece Hydrophobic Acrylic Intraocular Lens. J. Cataract Refract. Surg. 2008, 34, 1604–1609. [Google Scholar] [CrossRef]
- International Organization for Standardization: Geneva, S. ISO 11979-5:2020; Ophthalmic Implants—Intraocular Lenses—Part 5: Biocompatibility. Available online: https://www.iso.org/standard/72602.html (accessed on 3 February 2023).
- Carraway, J.W.; Daniel, E.M. Study Design and Methodologies for Study of Ocular Medical Devices. In Ocular Pharmacology and Toxicology; Gilger, B., Ed.; Humana Press: Totowa, NJ, USA, 2013; pp. 243–265. ISBN 978-1-62703-744-0. [Google Scholar]
- Chehade, M.; Elder, M.J. Intraocular Lens Materials and Styles: A Review. Aust. N. Z. J. Ophthalmol. 1997, 25, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Werner, L. Biocompatibility of Intraocular Lens Materials. Curr. Opin. Ophthalmol. 2008, 19, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Werner, L.; Legeais, J.-M.; Nagel, M.-D.; Renard, G. Neutral Red Assay of the Cytotoxicity of Fluorocarbon-Coated Polymethylmethacrylate Intraocular Lenses In Vitro. J. Biomed. Mater. Res. 1999, 48, 814–819. [Google Scholar] [CrossRef]
- Kao, E.C.Y.; Seo, J.; McCanna, D.J.; Subbaraman, L.N.; Jones, L.W. In Vitro Assessment of the Biocompatibility of Chemically Treated Silicone Materials with Human Lens Epithelial Cells. Sci. Rep. 2022, 12, 4649. [Google Scholar] [CrossRef]
- Tortolano, L.; Serrano, C.; Jubeli, E.; Saunier, J.; Yagoubi, N. Interaction of Intraocular Lenses with Fibronectin and Human Lens Epithelial Cells: Effect of Chemical Composition and Aging. J. Biomed. Mater Res. A 2015, 103, 3843–3851. [Google Scholar] [CrossRef] [PubMed]
- Özyol, P.; Özyol, E.; Karel, F. Biocompatibility of Intraocular Lenses. Turk. Oftalmol. Derg. 2017, 47, 221–225. [Google Scholar] [CrossRef]












| Silicone | PMMA | Hydrophobic Acrylic | Hydrophilic Acrylic | |
|---|---|---|---|---|
| Rigidity | flexible | rigid | flexible | flexible |
| Affinity to water | hydrophobic | hydrophobic | hydrophobic | hydrophilic |
| Refractive index | 1.41–1.46 | 1.49 | up to 1.55 | 1.43 |
| Abbe number | 42 | 58 | 37–55 | 58 |
| Material | WCA (° +/− SD) |
|---|---|
| Collamer | 77.7 +/− 0.79 |
| Hydrophilic acrylic | 68.4 +/− 1.11 |
| Hydrophobic acrylic | 88.7 +/− 1.24 |
| Silicone | 114.1 +/− 2.54 |
| PMMA | 77.1 +/− 2.34 |
| Heparinized PMMA | 79.9 +/− 2.21 |
| Model | Drop Profiling | WCA (°) | RMS Roughness (nm) |
|---|---|---|---|
| iSert 251 |  | 84.24 +/− 2.15 | 1.78 +/− 0.40 |
| CT Lucia 601P |  | 48.76 +/− 4.91 | 2.05 +/− 0.36 |
| enVista MX60 |  | 75.22 +/− 3.45 | 2.13 +/− 0.26 |
| Clareon SY60WF |  | 72.84 +/− 1.80 | 1.01 +/− 0.41 |
| Vivinex iSert XY1 |  | 78.94 +/− 6.66 | 0.63 +/− 0.57 |
| Tecnis PCB00 |  | 74.45 +/− 5.11 | 2.27 +/− 2.54 |
| Material | Water Content (%) | WCA (°) | Tensile Stress (MPa) | n | Tg (°C) |
|---|---|---|---|---|---|
| PMMA | 0.4–0.8 | 65–71 | 47–70 | 1.49 | 105–113 |
| Silicone | 0.38 | 97–120 | 5.9–8.2 | 1.43 | −120–−90 |
| Hydrophilic acrylics | 18–38 | 20–70 | 0.4.06 | 1.40–1.43 | 10–20 |
| Hydrophobic acrylics | 0.1–0.5 | 72–88 | No data | 1.47–1.56 | 5–16 |
| PHS | 4–5 | 69–79 | 4–6 | 1.54 | 27–29 |
| Materials | Advantage | Disadvantage |
|---|---|---|
| Hydrophilic acrylic | Higher tissue compatibility due to high water content; Low aqueous flare; Low rate of inflammatory cell accumulation on the lens surface. | Insufficient posterior sharp-edged design due to the high water content; High rate of posterior capsule opacification; High rate of anterior capsule opacification; Greater lens epithelial cell on growth on the lens surface. |
| Hydrophobic acrylic | Material compatible with a posterior sharp-edged design; Low rate of posterior capsule opacification; Low rate of anterior capsule opacification; Low rate of lens epithelial cell on growth on the lens surface. | High aqueous flare * Inflammatory cell accumulation on the lens surface *. * Not at a clinically significant level |
| PMMA | Good tissue compatibility; Low aqueous flare; Low rate of inflammatory cell accumulation on the lens surface. | Foldable High rate of posterior capsule opacification |
| Silicone | Low rate of inflammatory cell accumulation on the lens surface; Low rate of posterior capsule opacification. | Increased fibrotic reaction due to lens epithelial cell stimulation; Lens surface opacification due to contact with intravitreal air; Difficulty visualizing the retina due to interface formed with silicone oil used in vitreoretinal surgery. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vacalebre, M.; Frison, R.; Corsaro, C.; Neri, F.; Santoro, A.; Conoci, S.; Anastasi, E.; Curatolo, M.C.; Fazio, E. Current State of the Art and Next Generation of Materials for a Customized IntraOcular Lens according to a Patient-Specific Eye Power. Polymers 2023, 15, 1590. https://doi.org/10.3390/polym15061590
Vacalebre M, Frison R, Corsaro C, Neri F, Santoro A, Conoci S, Anastasi E, Curatolo MC, Fazio E. Current State of the Art and Next Generation of Materials for a Customized IntraOcular Lens according to a Patient-Specific Eye Power. Polymers. 2023; 15(6):1590. https://doi.org/10.3390/polym15061590
Chicago/Turabian StyleVacalebre, Martina, Renato Frison, Carmelo Corsaro, Fortunato Neri, Antonio Santoro, Sabrina Conoci, Elena Anastasi, Maria Cristina Curatolo, and Enza Fazio. 2023. "Current State of the Art and Next Generation of Materials for a Customized IntraOcular Lens according to a Patient-Specific Eye Power" Polymers 15, no. 6: 1590. https://doi.org/10.3390/polym15061590