

Detecting COVID-19 from Chest X-rays Using Convolutional Neural Network Ensembles



Abstract
:1. Introduction
2. Literature Review
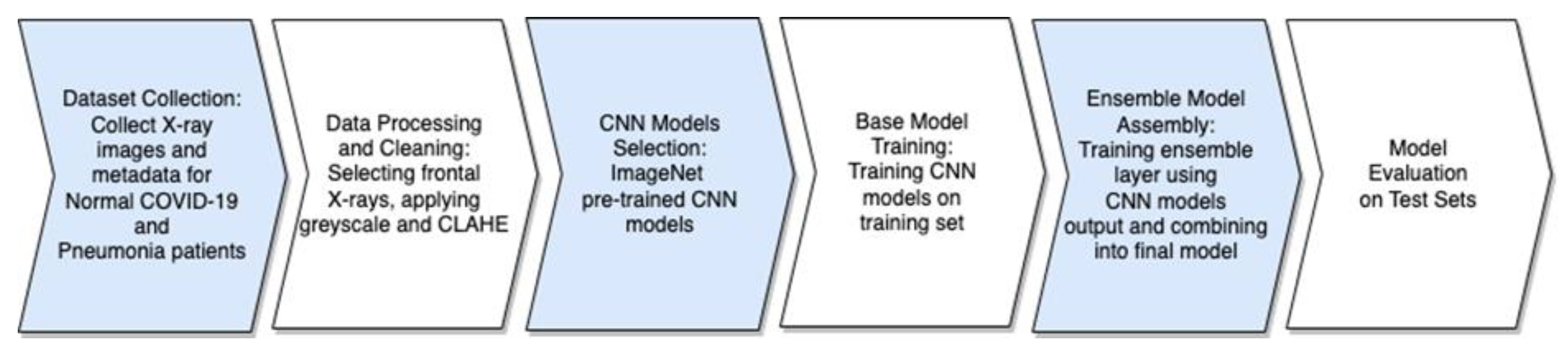
3. Methodology
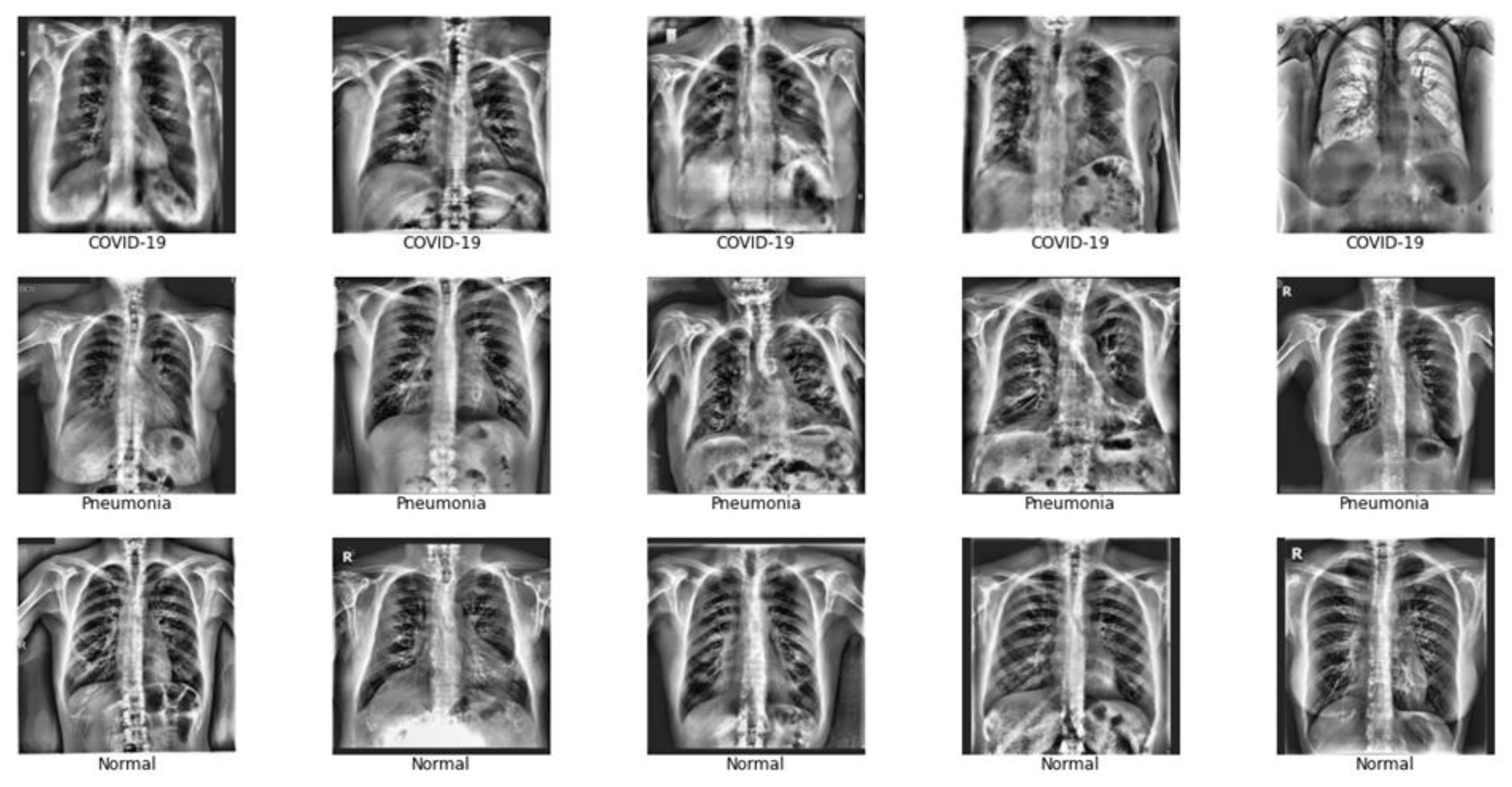
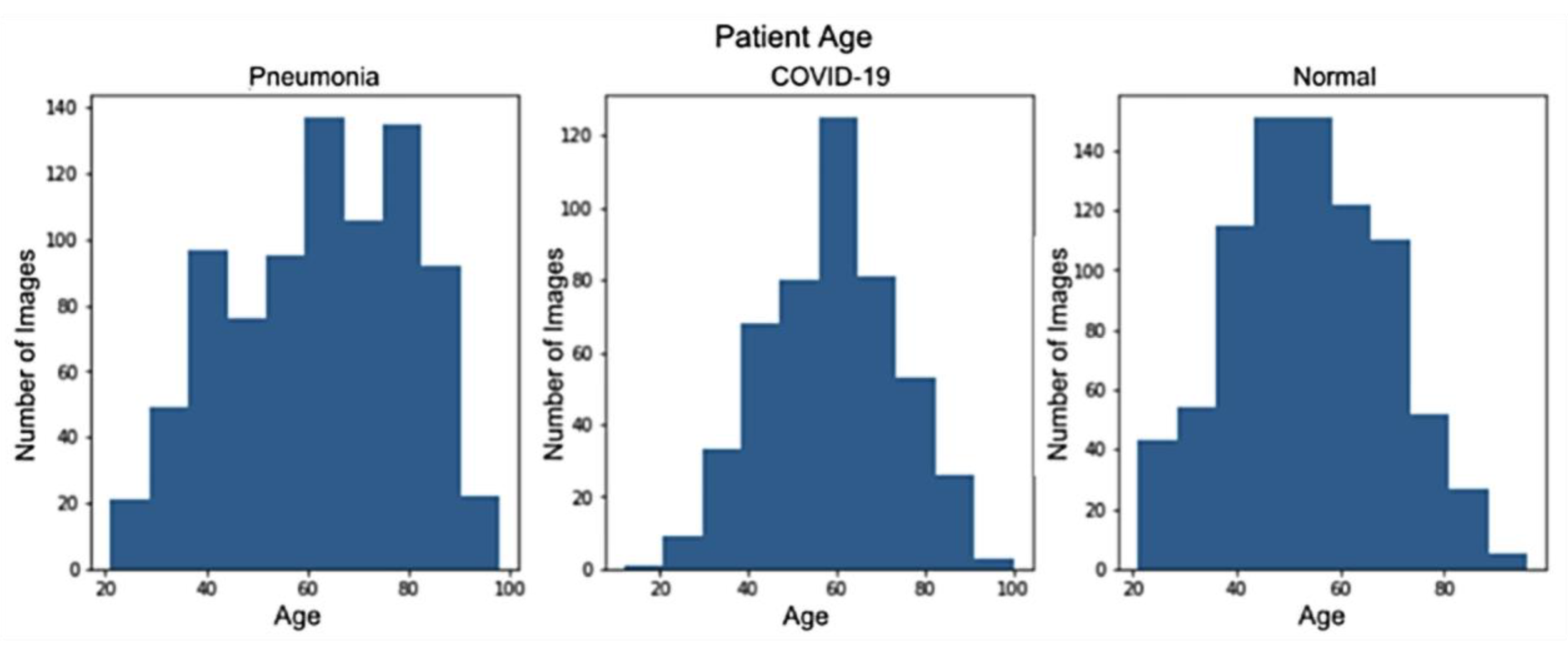
3.1. Data Description
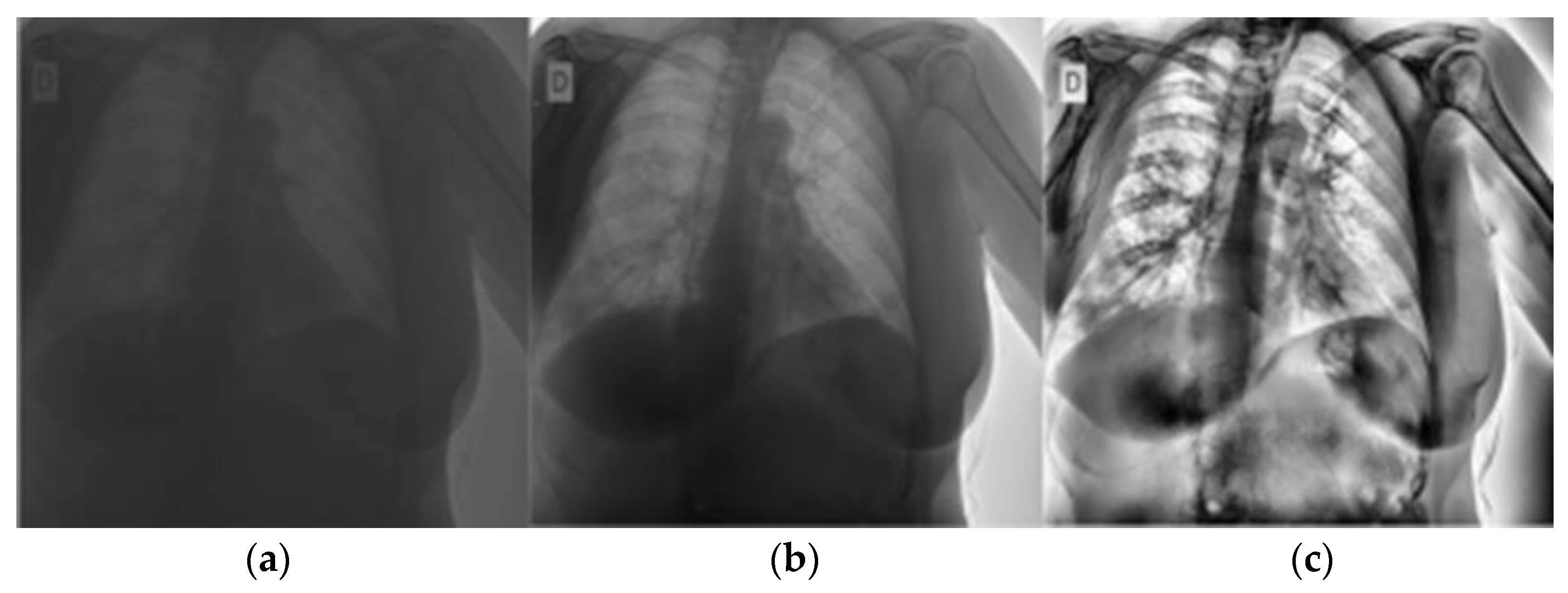
3.2. Pre-Processing
3.3. CNN and CNN Ensemble Models
4. Results and Discussion
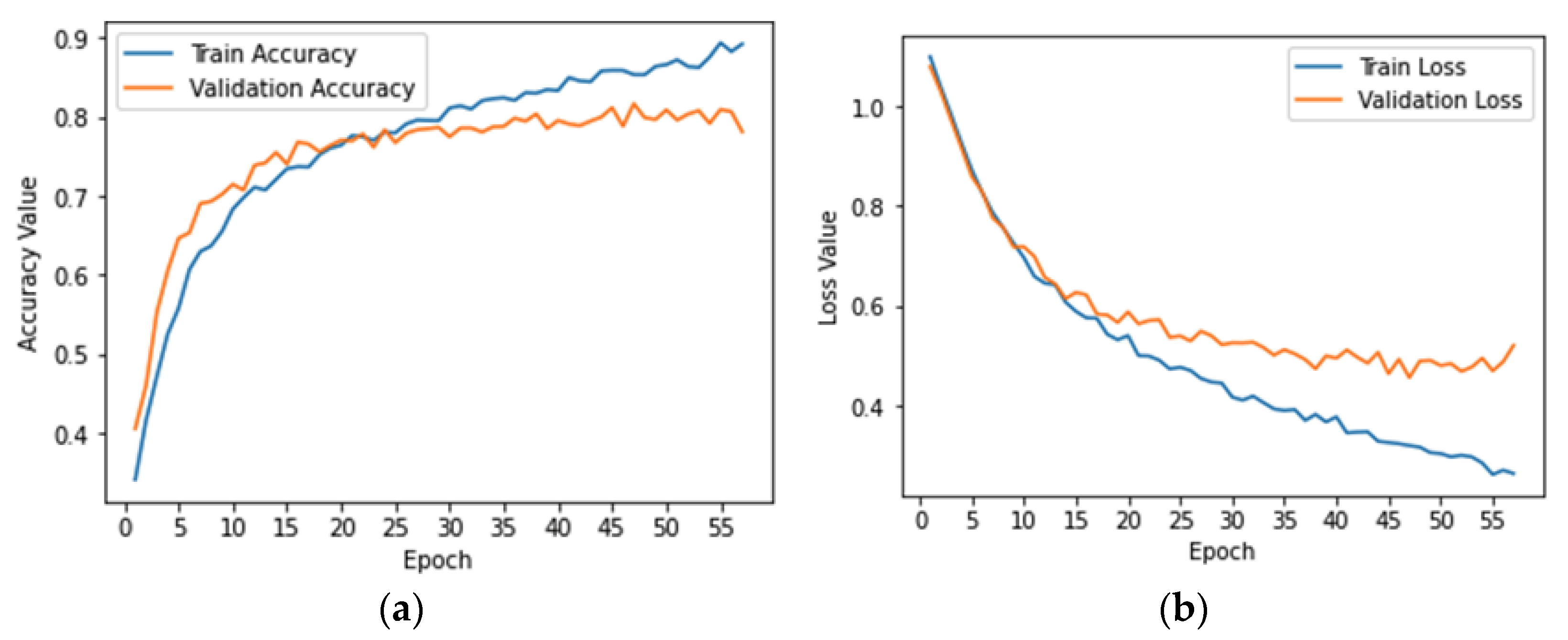
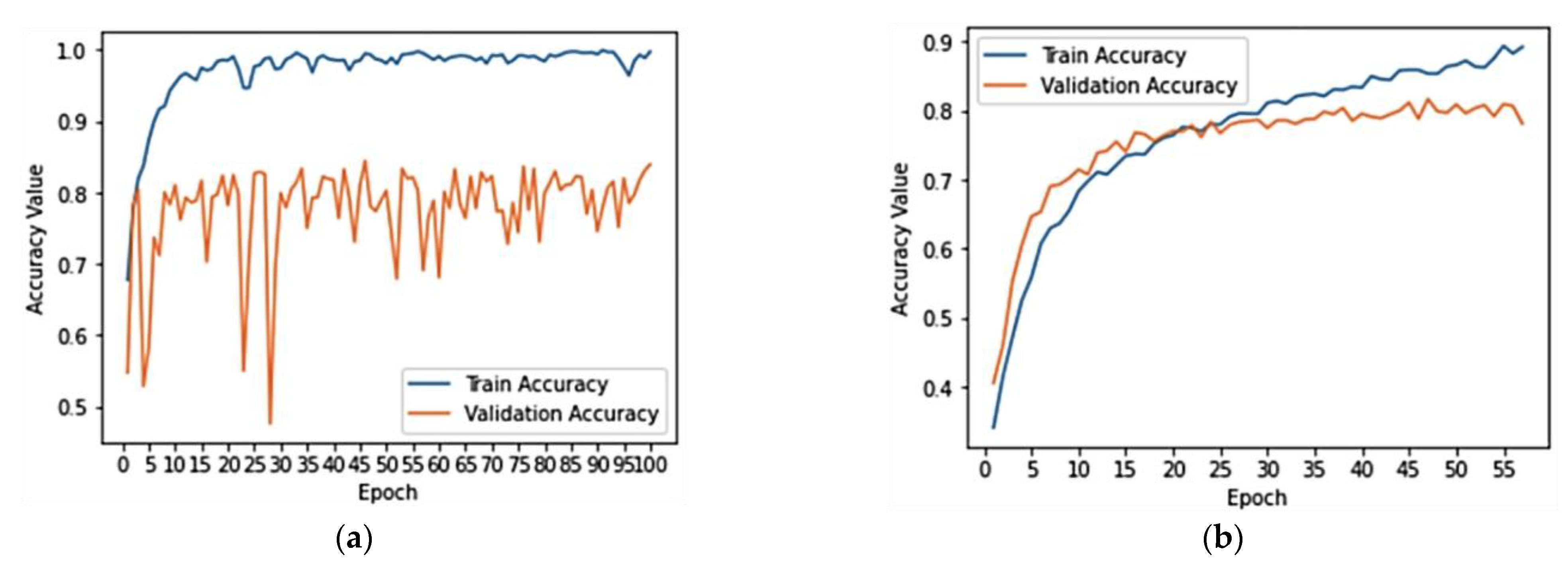
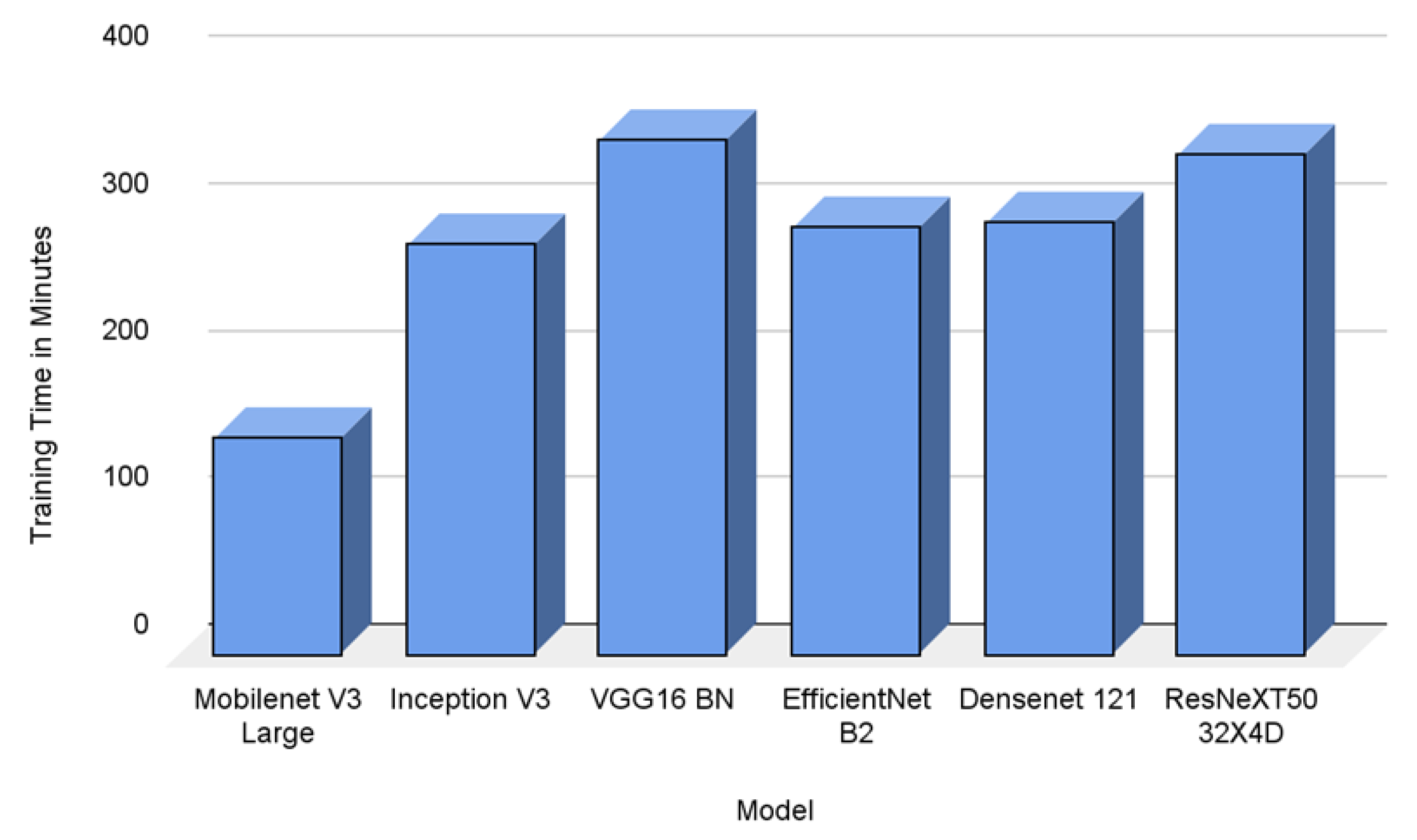
4.1. CNN Model Training and Results
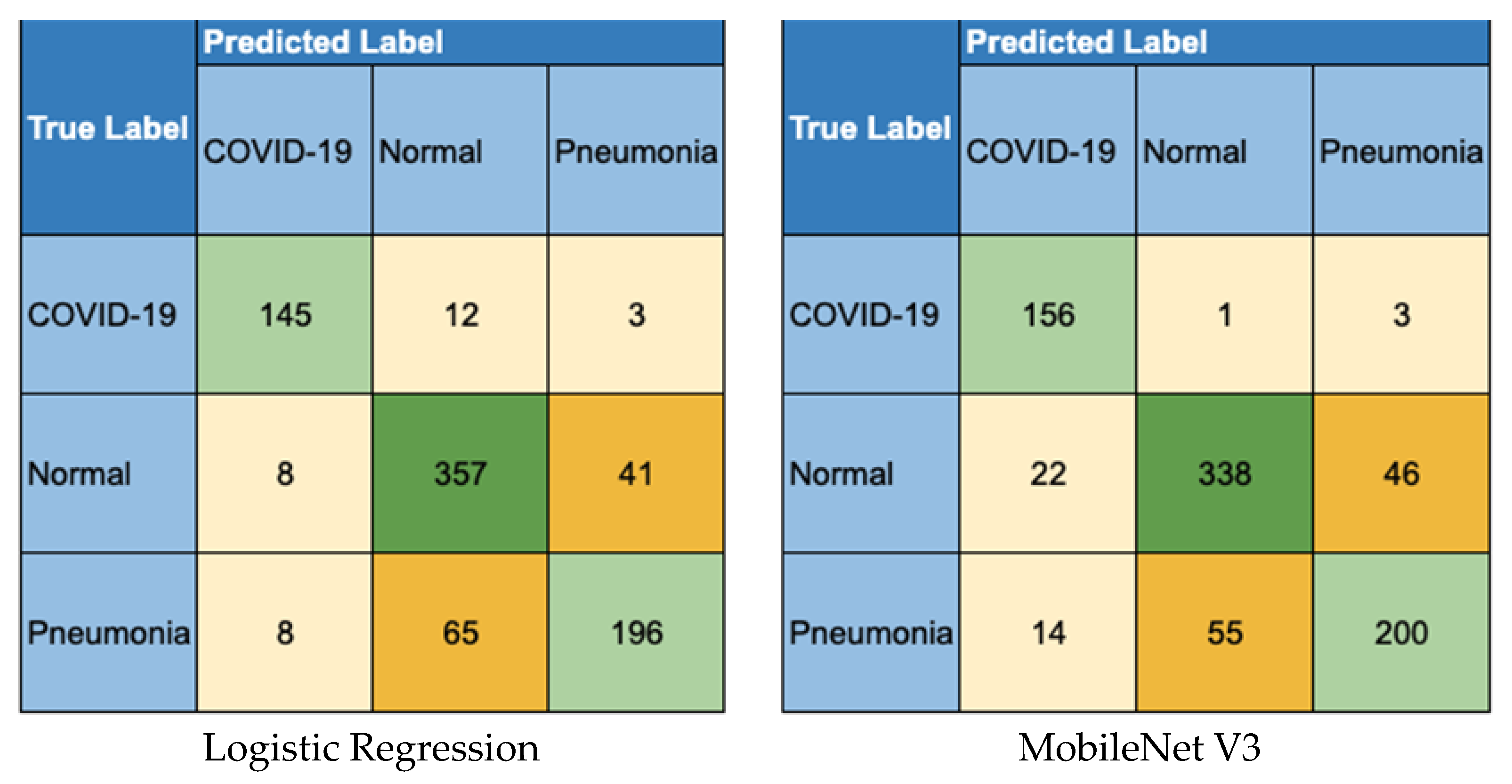
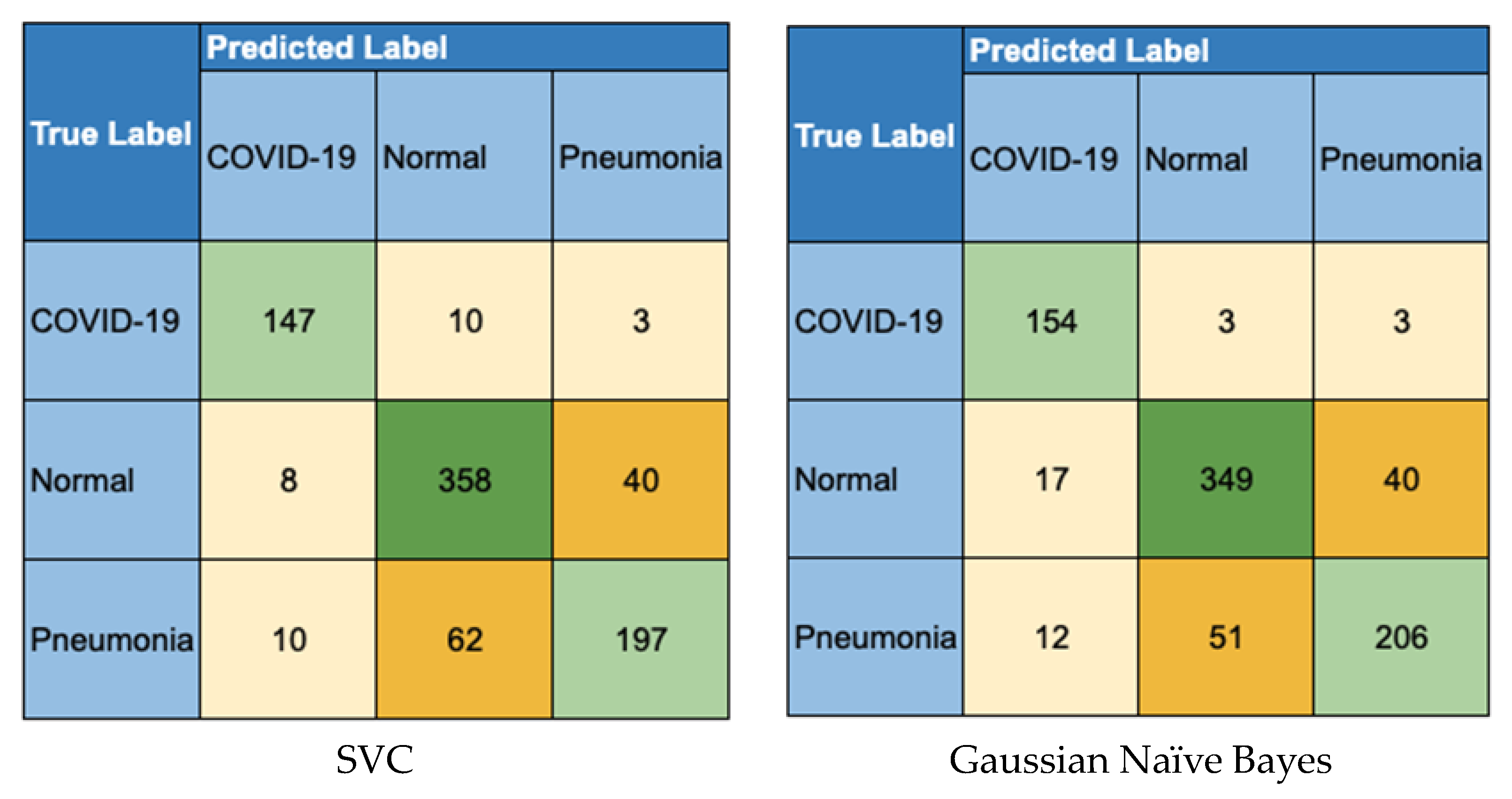
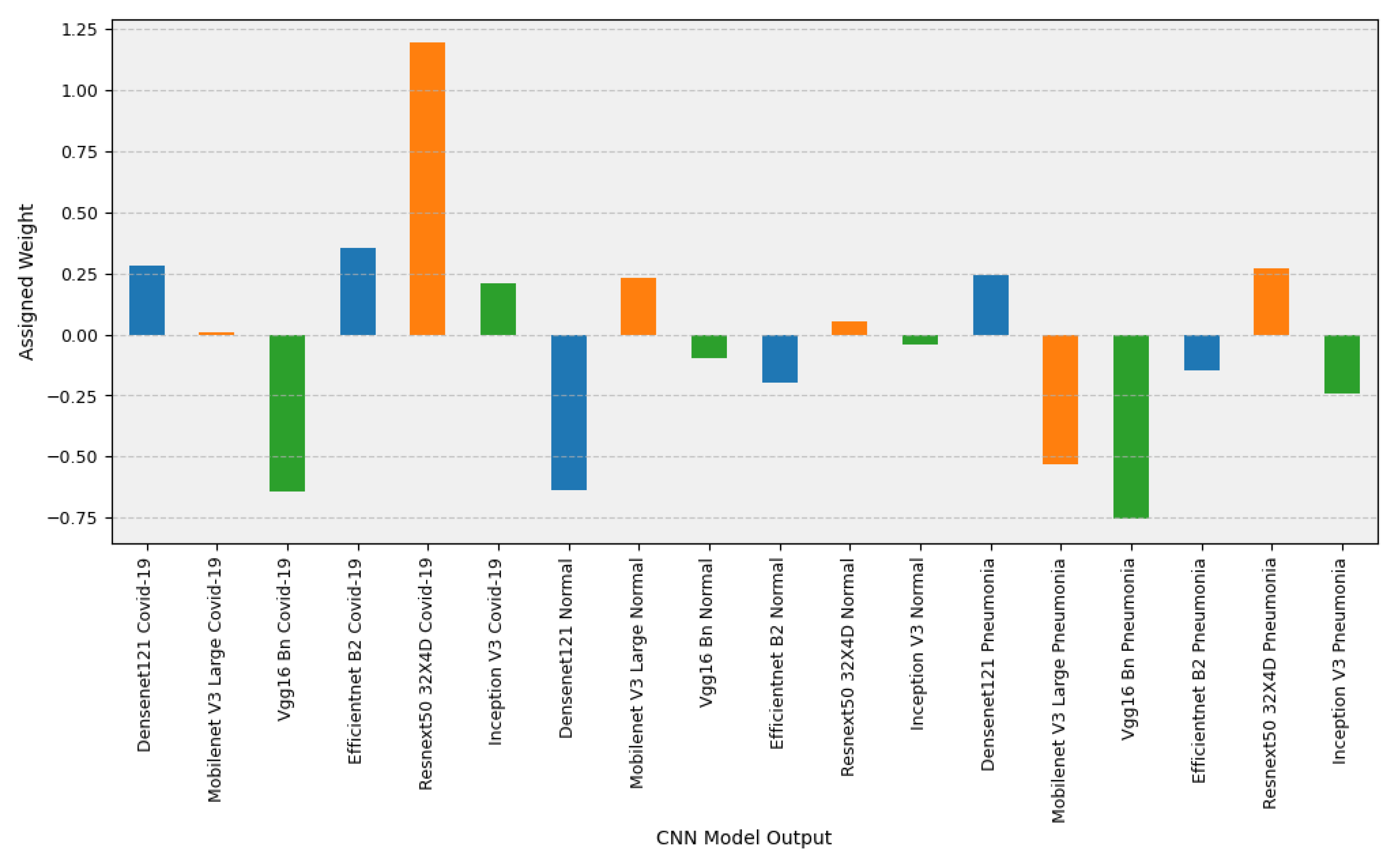
4.2. Ensemble Model Results
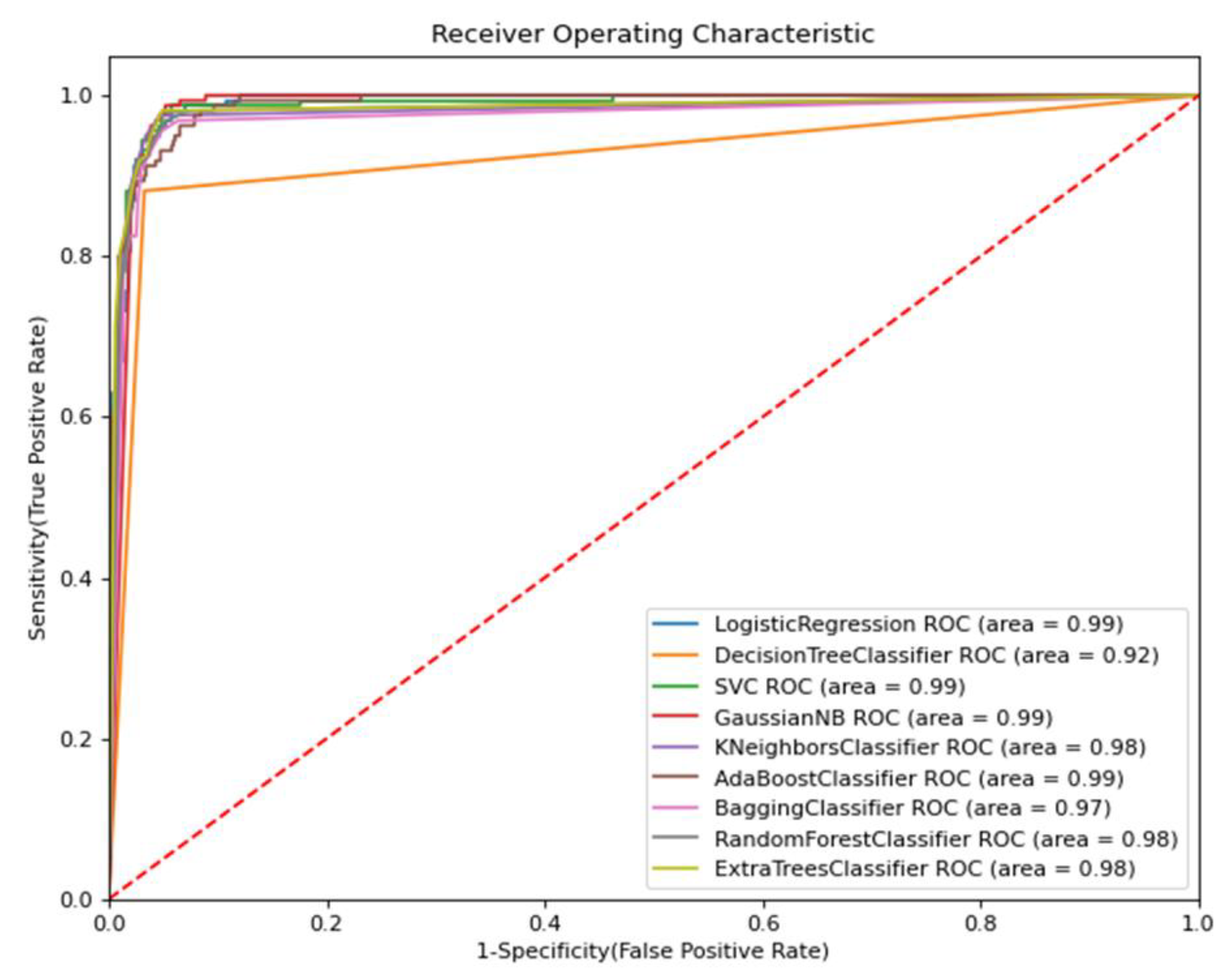
4.3. Performance Comparison Analysis
4.4. Performance Comparison with Previous Works
4.5. Strengths
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, R.; Agarwal, M.; Gupta, M.; Somendra, S.; Saxena, S.K. Clinical Characteristics and Differential Clinical Diagnosis of Novel Coronavirus Disease 2019 (COVID-19). Coronavirus Dis. 2019 COVID-19 2020, 2020, 55–70. [Google Scholar]
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatungea, J. Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy. Environ. Ress. 2020, 188, 109819. [Google Scholar] [CrossRef] [PubMed]
- Vilella, A. The COVID-19 Pandemic-an Epidemiological Perspective. Curr. Allergy Asthma Rep. 2021, 21, 29. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Du, Z.; Zhu, F.; Cao, Z.; An, Y.; Gao, Y.; Jiang, B. Comorbidities and multi-organ injuries in the treatment of COVID-19. Lancet 2020, 395, e52. [Google Scholar] [CrossRef] [PubMed]
- Merkur, S.; Maresso, A.; Cylus, J.; Ginneken, E.; Lessof, S. Lessons from the First Wave: The COVID-19 Health System Response Monitor an Evidence Resource and a Source of Analysis. Eurohealth 2020, 26, 5–9. [Google Scholar]
- Burki, T. Global COVID-19 Vaccine Inequity. Lancet Infect. Dis. 2021, 21, 922–923. [Google Scholar] [CrossRef]
- Kwon, R.; Rahmati, M. Global, regional, and national COVID-19 vaccination rate in 237 countries and territories, March 2022: A systematic analysis for World Health Organization COVID-19 Dashboard, Release 2. Life Cycle 2022, 2, e15. [Google Scholar] [CrossRef]
- Qjidaa, M.; Ben-Fares, A.; Mechbal, Y.; Amakdouf, H.; Maaroufi, M.; Alami, B.; Qjidaa, H. Development of a clinical decision support system for the early detection of COVID-19 using deep learning based on chest radiographic images. In Proceedings of the 2020 International Conference on Intelligent Systems and Computer Vision (ISCV), Fez, Morocco, 9–11 June 2020; pp. 1–6. [Google Scholar]
- Mayer, F.J.; Ratzinger, F.; Schmidt, R.L.J.; Greiner, G.; Landt, O.; Ende, A.A.; Corman, V.M.; Perkmann-Nagele, N.; Watkins-Riedel, T.; Petermann, D.; et al. Development of a fully automated high throughput PCR for the detection of SARS-CoV-2: The need for speed. Virulence 2020, 11, 964–967. [Google Scholar] [CrossRef]
- Mayer, F.J.; Ratzinger, F.; Schmidt, R.L.J.; Greiner, G.; Landt, O.; Ende, A.A.; Corman, V.M.; Perkmann-Nagele, N.; Watkins-Riedel, T.; Petermann, D.; et al. False-negative results of initial RT-PCR assays for COVID-19: A systematic review. PLoS ONE 2020, 15, e0242958. [Google Scholar]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef]
- Pratt, H.; Coenen, F.; Broadbent, D.M.; Harding, S.P.; Zheng, Y. Convolutional neural networks for diabetic retinopathy. Procedia. Comput. Sci. 2016, 90, 200–205. [Google Scholar] [CrossRef]
- Pereira, S.; Pinto, A.; Alves, V.; Silva, C.A. Brain tumor segmentation using convolutional neural networks in MRI images. IEEE Trans. Med. Imag. 2016, 35, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Ghazal, M.; Asl, E.H.; Mahmoud, A.; Aslantas, A.; Shalaby, A.; Casanova, M.; Barnes, G.; Gimel’farb, G.; Keynton, R.; El Baz, A. Alzheimer’s disease diagnostics by a 3D deeply supervised adaptable convolutional network. Front Biosci. 2018, 23, 584–596. [Google Scholar] [CrossRef] [PubMed]
- Klang, E. Deep Learning and Medical Imaging. J. Thorac. Dis. 2018, 10, 657–668. [Google Scholar] [CrossRef]
- Cha, D.; Pae, C.; Seong, S.-B.; Choi, J.Y.; Park, H.J. Automated diagnosis of ear disease using ensemble deep learning with a with a big otoendoscopy image database. EBioMedicine 2019, 45, 606–614. [Google Scholar] [CrossRef]
- Pham, H.H.; Le, T.T.; Tran, D.Q.; Ngo, D.T.; Nguyen, H.Q. Interpreting Chest X-rays Via CNNS That Exploit Hierarchical Disease Dependencies and Uncertainty Labels. Neurocomputing 2021, 437, 186–194. [Google Scholar] [CrossRef]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest X-ray images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef]
- Afifi, A.E.; Hafsa, N.; Ali, M.A.S.; Alhumam, A.; Alsalman, S. An Ensemble of Global and Local-Attention Based Convolutional Neural Networks for COVID-19 Diagnosis on Chest X-ray Images. Symmetry 2021, 13, 113. [Google Scholar] [CrossRef]
- Apostolopoulos, I.; Pesiana, T. COVID-19: Automatic detection from X-ray images utilizing transfer learning with convolutional neural networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef]
- Sethy, P.; Behera, S. Detection of Coronavirus Disease (COVID-19) Based on Deep Features. 2020. Available online: https://www.preprints.org/manuscript/202003.0300/v1 (accessed on 20 May 2022).
- Hemdan, E.; Shouman, M.A.; Karar, M.E. COVIDX-Net: A Framework of Deep Learning Classifiers to Diagnose COVID-19 in X-ray Images. 2020. Available online: https://arxiv.org/pdf/2003.11055.pdf (accessed on 25 April 2022).
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Haralabopoulos, G.; Anagnostopoulos, I.; McAuley, D. Ensemble Deep Learning for Multilabel Binary Classification of User-Generated Content. Algorithms 2020, 13, 83. [Google Scholar] [CrossRef]
- Ahmad, F.; Farooq, A.; Ghani, M.U. Deep Ensemble Model for Classification of Novel Coronavirus in Chest X-ray Images. Comput. Intell. Neurosci. 2021, 2021, 8890226. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Li, F.-F. ImageNet: A large-scale hierarchical image database. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; IEEE: New York, NY, USA; pp. 248–255. [Google Scholar]
- Vayá, M.D.L.I.; Saborit, J.M.; Montell, J.A.; Pertusa, A.; Bustos, A.; Cazorla, M.; Galant, J.; Barber, X.; Orozco-Beltrán, D.; García-García, F.; et al. BIMCV COVID-19+: A Large Annotated Dataset of RX and CT Images from COVID-19 Patients. Available online: https://arxiv.org/abs/2006.01174 (accessed on 21 July 2022).
- Zhao, W.; Jiang, W.; Qiu, X. Deep learning for COVID-19 detection based on CT images. Sci. Rep. 2021, 11, 14353. [Google Scholar] [CrossRef] [PubMed]
- Pathak, Y.; Shukla, P.K.; Arya, K.V. Deep Bidirectional Classification Model for COVID-19 Disease Infected Patients. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 18, 1234–1241. [Google Scholar] [CrossRef]
- Sahoo, P.; Saha, S.; Mondal, S.; Chowdhury, S.; Gowda, S. Computer-Aided COVID-19 Screening from Chest CT-Scan using a Fuzzy Ensemble-based Technique. In Proceedings of the 2022 International Joint Conference on Neural Networks (IJCNN), Shenzhen, China, 18–23 June 2022; pp. 1–8. [Google Scholar]
- Dialameh, M.; Hamzeh, A.; Rahmani, H.; Radmard, A.R.; Dialameh, S. Proposing a novel deep network for detecting COVID-19 based on chest images. Sci. Rep. 2022, 12, 3116. [Google Scholar] [CrossRef]
- Zhao, C.; Xu, Y.; He, Z.; Tang, J.; Zhang, Y.; Han, J.; Shi, Y.; Zhou, W. Lung segmentation and automatic detection of COVID-19 using radiomic features from chest CT images. Pattern Recognit. 2021, 119, 108071. [Google Scholar] [CrossRef]
- Basu, A.; Sheikh, K.H.; Cuevas, E.; Sarkar, R. COVID-19 detection from CT scans using a two-stage framework. Expert Syst. Appl. 2022, 193, 116377. [Google Scholar] [CrossRef]
- Brito, V.C.; Santos, P.R.S.; Sales Carvalho, N.R.; Carvalho Filho, A.O. COVID-index: A texture-based approach to classifying lung lesions based on CT images. Pattern Recognit. 2021, 119, 108083. [Google Scholar] [CrossRef]
- Gupta, P.K.; Siddiqui, M.K.; Huang, X.; Morales-Menendez, R.; Pawar, H.; Terashima-Marin, H.; Wajid, M.S. COVID-WideNet-A capsule network for COVID-19 detection. Appl. Soft Comput. 2022, 122, 108780. [Google Scholar] [CrossRef]
- Karthik, R.; Menaka, R.M.H. Learning distinctive filters for COVID-19 detection from chest X-ray using shuffled residual CNN. Appl. Soft Comput. J. 2021, 99, 106744. [Google Scholar] [CrossRef] [PubMed]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic Detection of Coronavirus Disease (COVID-19) Using X-ray Images and Deep Convolutional Neural Networks. Pattern Anal. Appl. 2021, 24, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Hira, S.; Bai, A.; Hira, S. An automatic approach based on CNN architecture to detect Covid-19 disease from chest X-ray images. Appl. Intell. 2021, 51, 2864–2889. [Google Scholar] [CrossRef] [PubMed]
- Heidari, M.; Mirniaharikandehei, S.; Khuzani, A.Z.; Danala, G.; Qiu, Y.; Zheng, B. Improving the performance of CNN to predict the likelihood of COVID-19 using chest X-ray images with preprocessing algorithms. Int. J. Med. Inform. 2020, 144, 104284. [Google Scholar] [CrossRef]
- Jain, R.; Gupta, M.; Taneja, S.; Thakur, P.; Sharma, R.; Pachori, R.B. Deep learning-based detection and analysis of COVID-19 on chest X-ray images. Appl. Intell. 2001, 51, 1690–1700. [Google Scholar] [CrossRef]
- Gouda, W.; Almurafeh, M.; Humayun, M.; Jhanjhi, N.Z. Detection of COVID-19 Based on Chest X-rays Using Deep Learning. Healthcare 2022, 10, 343. [Google Scholar] [CrossRef] [PubMed]
- Elhanashi, A.; Lowe, D.; Saponara, S.; Moshfeghi, Y. Deep learning techniques to identify and classify COVID-19 abnormalities on chest x-ray images. In Proceedings of the Real-Time Image Processing and Deep Learning 2022, Orlando, FL, USA, 27 May 2022; Volume 12102. [Google Scholar] [CrossRef]
- Bhattacharyya, A.; Bhaik, D.; Kumar, S.; Thakur, P.; Sharma, R.; Pachori, R.B. A deep learning based approach for automatic detection of COVID-19 cases using chest X-ray images. Biomed. Signal Process Control. 2022, 71, 103182. [Google Scholar] [CrossRef]
- Loey, M.; El-Sappagh, S.; Mirjalili, S. Bayesian-based optimized deep learning model to detect COVID-19 patients using chest X-ray image data. Comput. Biol. Med. 2022, 142, 105213. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Versaci, M.; Varone, G.; Ali, A.R.; Armentano, A.; Calabrese, G.; Ferrarelli, A.; Turano, L.; Tebala, C.; et al. A fuzzy-enhanced deep learning approach for early detection of Covid-19 pneumonia from portable chest X-ray images. Neurocomputing 2022, 481, 202–215. [Google Scholar] [CrossRef]
- Barshooi, A.; Amirkhani, A. A novel data augmentation based on Gabor filter and convolutional deep learning for improving the classification of COVID-19 chest X-ray images. Biomed. Signal Process Control. 2022, 72, 103326. [Google Scholar] [CrossRef]
- Ullah Khan, I.; Aslam, N.; Anwar, T.; Alsaif, H.S.; Chrouf, S.M.B.; Alzahrani, N.A.; Alamoudi, F.A.; Kamaleldin, M.M.A.; Awary, K.B. Using a Deep Learning Model to Explore the Impact of Clinical Data on COVID-19 Diagnosis Using Chest X-ray. Sensors 2022, 22, 669. [Google Scholar] [CrossRef] [PubMed]
- Chhikara, P.; Gupta, P.; Singh, P.; Bhatia, T. A deep transfer learning based model for automatic detection of COVID-19 from chest X-rays. Turk. J. Electr. Eng. Comput. Sci. 2021, 29, 2663–2679. [Google Scholar] [CrossRef]
- Khan, E.; Rehman, M.Z.U.; Ahmed, F.; Alfouzan, F.A.; Alzahrani, N.M.; Ahmad, J. Chest X-ray Classification for the Detection of COVID-19 Using Deep Learning Techniques. Sensors 2022, 22, 1211. [Google Scholar] [CrossRef] [PubMed]
- Muralidharan, N.; Gupta, S.; Prusty, M.R.; Tripathy, R.K. Detection of COVID19 from X-ray images using multiscale Deep Convolutional Neural Network. Appl. Soft Comput. Appl. Soft Comput. 2022, 119, 108610. [Google Scholar] [CrossRef]
- Muralidharan, N.; Gupta, S.; Prusty, M.R.; Tripathy, R.K. COVID-CXNet: Detecting COVID-19 in frontal chest X-ray images using deep learning. Multimed. Tools Appl. 2022, 81, 30615–30645. [Google Scholar]
- Breve, F. COVID-19 detection on Chest X-ray images: A comparison of CNN architectures and ensembles. Expert Syst. Appl. 2022, 204, 117549. [Google Scholar] [CrossRef]
- Zhou, T. The Ensemble Deep Learning Model for Novel COVID-19 on CT Images. Appiedl. Soft Comput. 2021, 98, 106885. [Google Scholar] [CrossRef]
- Jin, W.; Dong, S.; Dong, C.; Ye, X. Hybrid ensemble model for differential diagnosis between COVID-19 and common viral pneumonia by chest X-ray radiograph. Comput. Biol. Med. 2021, 131, 104252. [Google Scholar] [CrossRef]
- Dey, S.; Bhattacharya, R.; Malakar, S.; Schwenker, F.; Sarkar, R. CovidConvLSTM: A fuzzy ensemble model for COVID-19 detection from chest X-rays. Expert Syst. Appl. 2022, 206, 117812. [Google Scholar] [CrossRef]
- Nasiri, H.; Nasiri, S. Automated detection of COVID-19 cases from chest X-ray images using deep neural network and XGBoost. Radiography 2022, 28, 732–738. [Google Scholar] [CrossRef]
- Hryniewska, W.; Bombiński, P.; Szatkowski, P.; Tomaszewska, P.; Przelaskowski, A.; Biecek, P. Checklist for responsible deep learning modeling of medical images based on COVID-19 detection studies. Pattern Recognit. 2021, 118, 108035. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.; Driggs, D.; Thorpe, M.; Gilbey, J.; Yeung, M.; Ursprung, S.; Aviles-Rivero, A.I.; Etmann, C.; McCague, C.; Beer, L.; et al. Common pitfalls and recommendations for using machine learning to detect and prognosticate for COVID-19 using chest radiographs and CT scans. Nat. Mach. Intell. 2021, 3, 197–217. [Google Scholar] [CrossRef]
- Bui, H.M.; Lech, M.; Cheng, E.; Neville, K.; Burnett, I.S. Using grayscale images for object recognition with convolutional-recursive neural network. In Proceedings of the IEEE Sixth International Conference on Communications and Electronics (ICCE), Ha-Long, Vietnam, 27–29 July 2016; pp. 311–325. [Google Scholar]
- Duran-Lopez, L.; Dominguez-Morales, J. COVID-XNet: A Custom Deep Learning System to Diagnose and Locate COVID-19 in Chest X-ray Images. Appl. Sci. 2020, 10, 5683. [Google Scholar] [CrossRef]
- Nahiduzzaman; Goni, O.F.; Anower, S.; Islam, R.; Ahsan, M.; Haider, J.; Gurusamy, S.; Hassan, R.; Islam, R. A Novel Method for Multivariant Pneumonia Classification Based on Hybrid CNN-PCA Based Feature Extraction Using Extreme Learning Machine with CXR Images. IEEE Access 2021, 9, 147512–147526. [Google Scholar] [CrossRef]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. MobileNets: Efficient Convolutional Neural Networks for Mobile Vision Applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A.; Liu, W.; et al. Going Deeper with Convolutions. arXiv 2014, arXiv:1409.4842. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 29 May 2019. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity Mappings in Deep Residual networks. In Proceedings of the European Conference on Computer Vision, Online. 17 September 2016. [Google Scholar]
- Sousa, P.M.; Carneiro, P.C.; Oliveira, M.M.; Pereira, G.M.; Junior, C.A.C.; Moura, L.V.; Mattjie, C.; Silva, A.M.M.; Patrocinio, A.C. COVID-19 classification in X-ray chest images using a new convolutional neural network: CNN-COVID. Res. Biomed. Eng. 2022, 38, 87–97. [Google Scholar] [CrossRef]
- Arias-Garzón, D.; Alzate-Grisales, J.A.; Orozco-Arias, S.; Arteaga-Arteaga, H.B.; Bravo-Ortiz, M.A.; Mora-Rubio, A.; Saborit-Torres, J.M.; Serrano, J.M.; Tabares-Soto, R.; Vayá, M.D.L.I. COVID-19 detection in X-ray images using convolutional neural networks. Mach. Learn. Appl. 2021, 6, 100138. [Google Scholar] [CrossRef]
- Nishio, M.; Kobayashi, D.; Nishioka, E.; Matsuo, H.; Urase, Y.; Onoue, K.; Ishikura, K.; Kitamura, Y.; Sakai, E.; Tomita, E.; et al. Deep learning model for the automatic classification of COVID-19 pneumonia, non-COVID-19 pneumonia, and the healthy: A multi-center retrospective study. Sci. Rep. 2022, 12, 8214. [Google Scholar] [CrossRef]
- Panwar, H.; Gupta, P.; Siddiqui, M.K.; Morales-Menendez, R.; Singh, V. Application of deep learning for fast detection of COVID-19 in X-rays using nCOVnet. Chaos Solitons Fractals 2020, 138, 109944. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, T. CovXNet: A multidilation convolutional neural network for automatic COVID-19 and other pneumonia detection from chest X-ray images with transferable multi-receptive feature optimization. Comput. Biol. Med. 2020, 122, 103869. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.E.H.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Mahbub, Z.B. Can AI help in screening Viral and COVID-19 pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | No. of X-ray Images |
|---|---|
| COVID-19 | 632 |
| Normal | 1592 |
| Pneumonia | 1106 |
| Total | 3330 |
| Model | Trainable Parameters | References |
|---|---|---|
| MobileNet V3 Large | 5.5 M | [60] |
| Inception V3 | 27.2 M | [61] |
| VGG16 BN | 138.4 M | [62] |
| EfficientNet B2 | 9.1 M | [63] |
| Densenet 121 | 8.0 M | [64] |
| ResNeXT50 32X4D | 25.0 M | [65] |
| Model | 3-Class Accuracy | COVID-19 Accuracy | COVID-19 F1-Score | Normal Accuracy | Normal F1-Score | Pneumonia Accuracy | Pneumonia F1-Score |
|---|---|---|---|---|---|---|---|
| MobileNet V3 Large | 83.11% | 95.21% | 88.64% | 85.15% | 84.50% | 85.87% | 77.22% |
| Inception V3 | 82.16% | 95.21% | 88.51% | 84.79% | 84.14% | 84.31% | 74.86% |
| VGG16 BN | 80.84% | 94.85% | 87.32% | 83.11% | 82.83% | 83.71% | 73.33% |
| EfficientNet B2 | 82.04% | 94.49% | 87.15% | 84.43% | 83.20% | 85.15% | 76.95% |
| DenseNet 121 | 82.04% | 94.73% | 86.67% | 84.67% | 83.51% | 84.67% | 77.31% |
| ResNeXT50 32X4D | 80.60% | 94.37% | 85.17% | 83.11% | 83.27% | 83.71% | 73.33% |
| Ensemble Model | 3-Class Accuracy | COVID-19 Accuracy | COVID-19 F1-Score | Normal Accuracy | Normal F1-Score | Pneumonia Accuracy | Pneumonia F1-Score |
|---|---|---|---|---|---|---|---|
| SVC | 84.07% | 96.29% | 90.46% | 85.63% | 85.65% | 86.23% | 77.41% |
| Random Forest Classifier | 84.07% | 96.29% | 90.46% | 85.63% | 85.54% | 86.23% | 77.67% |
| Logistic Regression | 83.59% | 96.29% | 90.34% | 84.91% | 85.00% | 85.99% | 77.01% |
| K-Neighbors Classifier | 84.07% | 96.17% | 90.30% | 85.51% | 85.37% | 86.47% | 77.97% |
| Extra Trees Classifier | 83.47% | 96.29% | 90.28% | 85.27% | 85.34% | 85.39% | 76.17% |
| Gaussian Naive Bayes | 84.91% | 95.81% | 89.80% | 86.71% | 86.28% | 87.31% | 79.54% |
| Majority Voting | 84.43% | 95.33% | 88.83% | 86.59% | 86.37% | 86.95% | 78.16% |
| AdaBoost Classifier | 79.16% | 95.81% | 88.82% | 81.20% | 80.83% | 81.32% | 71.00% |
| Unweighted Average Predictions | 84.91% | 95.33% | 88.70% | 86.83% | 86.49% | 87.66% | 79.84% |
| Bagging Classifier | 82.63% | 95.45% | 88.13% | 84.43% | 84.60% | 85.39% | 75.89% |
| Decision Tree Classifier | 80.72% | 94.85% | 86.52% | 82.75% | 82.65% | 83.83% | 74.09% |
| Metric | Top Ensemble Model | Ensemble Model Performance | Top CNN Model | CNN Model Performance | Ensemble Improvement over CNN Model |
|---|---|---|---|---|---|
| 3-Class Accuracy | Gaussian Naive Bayes | 84.91% | MobileNet V3 Large | 83.07% | 2.16% |
| COVID-19 Accuracy | Logistic Regression | 96.29% | MobileNet V3 Large | 95.20% | 1.13% |
| COVID-19 Precision | AdaBoost Classifier | 90.85% | ResNeXT50 32X4D | 85.71% | 5.65% |
| COVID-19 Recall | - | - | MobileNet V3 Large | 97.50% | 0.00% |
| COVID-19 F1-Score | SVC | 90.46% | MobileNet V3 Large | 88.60% | 2.06% |
| Normal Accuracy | Unweighted Average Predictor | 86.83% | MobileNet V3 Large | 85.12% | 1.97% |
| Normal Precision | - | - | Densenet 121 | 87.57% | 0.00% |
| Normal Recall | SVC | 88.18% | ResNeXT50 32X4D | 86.42% | 1.99% |
| Normal F1-Score | Unweighted Average Predictor | 86.49% | MobileNet V3 Large | 84.45% | 2.35% |
| Pneumonia Accuracy | Unweighted Average Predictor | 87.66% | MobileNet V3 Large | 85.83% | 2.09% |
| Pneumonia Precision | Majority Voting Predictor | 84.78% | MobileNet V3 Large | 80.07% | 5.55% |
| Pneumonia Recall | DenseNet 121 | 81.04% | Densenet 121 | 81.04% | 0.00% |
| Pneumonia F1-Score | Unweighted Average Predictor | 79.84% | Densenet 121 | 77.22% | 3.28% |
| Number of CNN Models | Top Ensemble | COVID-19 Accuracy | F1-Score |
|---|---|---|---|
| Top CNN Model | - | 95.20% | 88.60% |
| Top 2 CNN Models | K Neighbors Classifier | 96.53% | 91.19% |
| Top 3 CNN Models | Random Forest Classifier | 96.41% | 90.80% |
| Top 4 CNN Models | Support Vector Classifier | 96.53% | 91.34% |
| Top 5 CNN Models | Logistic Regression | 96.53% | 91.24% |
| Top 6 Models | Support Vector Classifier | 96.29% | 90.46% |
| References | Architecture | COVID-19 Accuracy |
|---|---|---|
| Hira et al. [39] | Se-ResNeXt | 99.23% |
| Jin et al. [55] | AlexNet | 98.64% |
| S. Dey et al. [56] | CovidConvLSTM | 98.63% |
| A. Barshooi & A. Amirkhani [47] | DenseNet | 98.50% |
| Ozturk [24] | DarkNet | 98.08% |
| Narin et al. [38] | ResNet-50 | 98.00% |
| Chhikara et al. [49] | InceptionV3 | 97.70% |
| Khan et al. [48] | EfficientNet | 97.00% |
| Bhattacharyya [44] | VGG-19 | 96.60% |
| Proposed Model | Support Vector Classifier | 96.53% |
| Khan et al. [50] | EfficientNet | 96.13% |
| P. Sethy & E. Behara [22] | ResNet-50 | 95.38% |
| Haidari et al. [40] | VGG16 | 94.50% |
| Wang et al. [12] | COVID-Net | 92.40% |
| E. Hemdan et al. [23] | VGG19 | 90.00% |
| H. Nasiri & E. Nasiri [57] | DenseNet + XGBoost | 89.70% |
| I.D. Apostolopoulos et al. [21] | Xception | 85.57% |
| References | Architecture | COVID-19 Accuracy |
|---|---|---|
| P. de Sousa et al. [69] | Custom CNN | 98.84% |
| Proposed Model | Support Vector Classifier | 96.53% |
| Arias-Garzon [70] | VGG-19 | 96.30% |
| Mizuho et al. [71] | EfficientNet | 94.60% |
| Duran-Lopez et al. [61] | COVID-XNet | 94.43% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Lel, T.; Ahsan, M.; Haider, J. Detecting COVID-19 from Chest X-rays Using Convolutional Neural Network Ensembles. Computers 2023, 12, 105. https://doi.org/10.3390/computers12050105
El Lel T, Ahsan M, Haider J. Detecting COVID-19 from Chest X-rays Using Convolutional Neural Network Ensembles. Computers. 2023; 12(5):105. https://doi.org/10.3390/computers12050105
Chicago/Turabian StyleEl Lel, Tarik, Mominul Ahsan, and Julfikar Haider. 2023. "Detecting COVID-19 from Chest X-rays Using Convolutional Neural Network Ensembles" Computers 12, no. 5: 105. https://doi.org/10.3390/computers12050105