
Female Sex but Not Oestrogen Receptor Expression Predicts Survival in Advanced Gastroesophageal Adenocarcinoma—A Post-hoc Analysis of the GO2 Trial
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
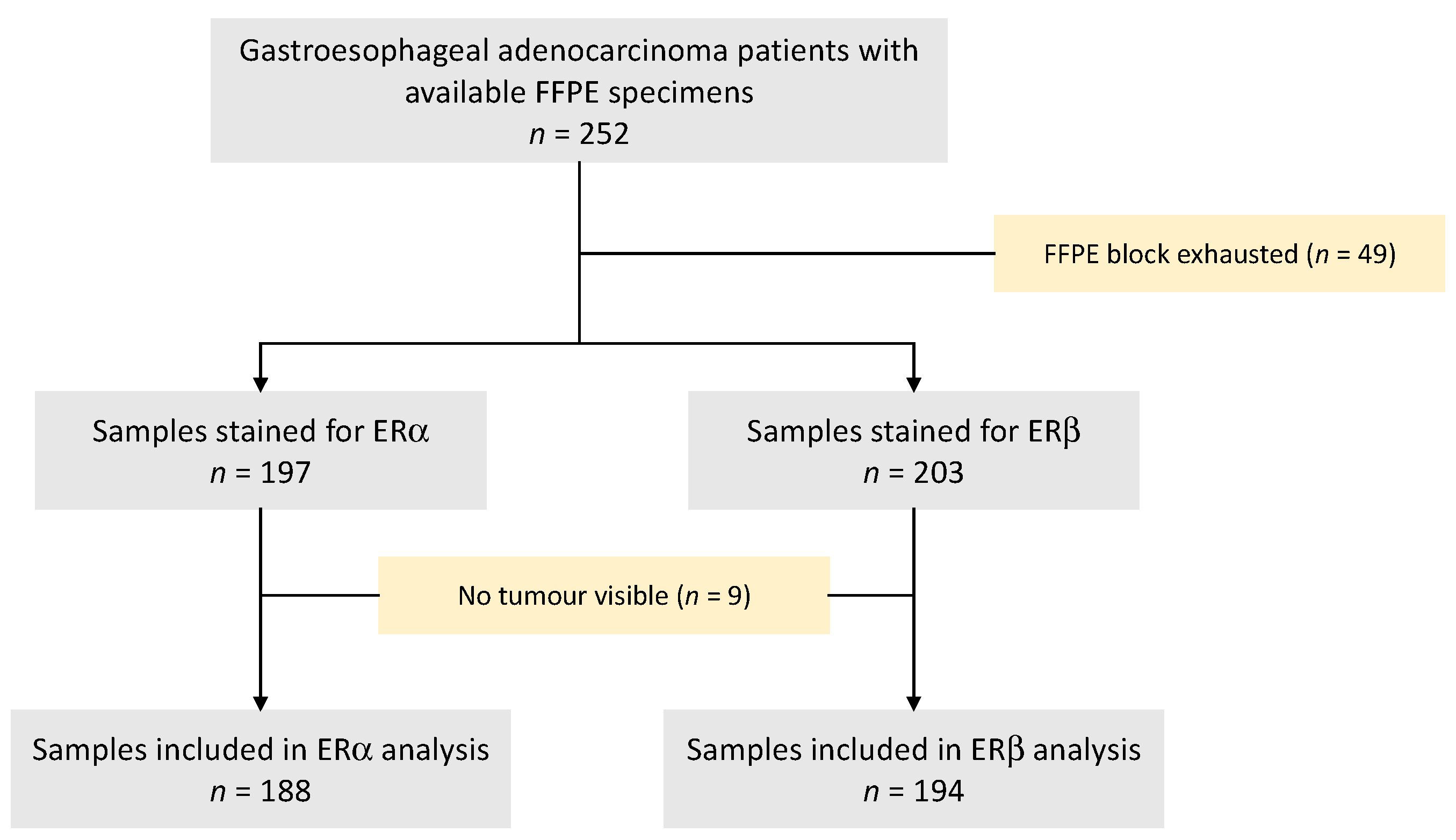
2.1. Study Cohort
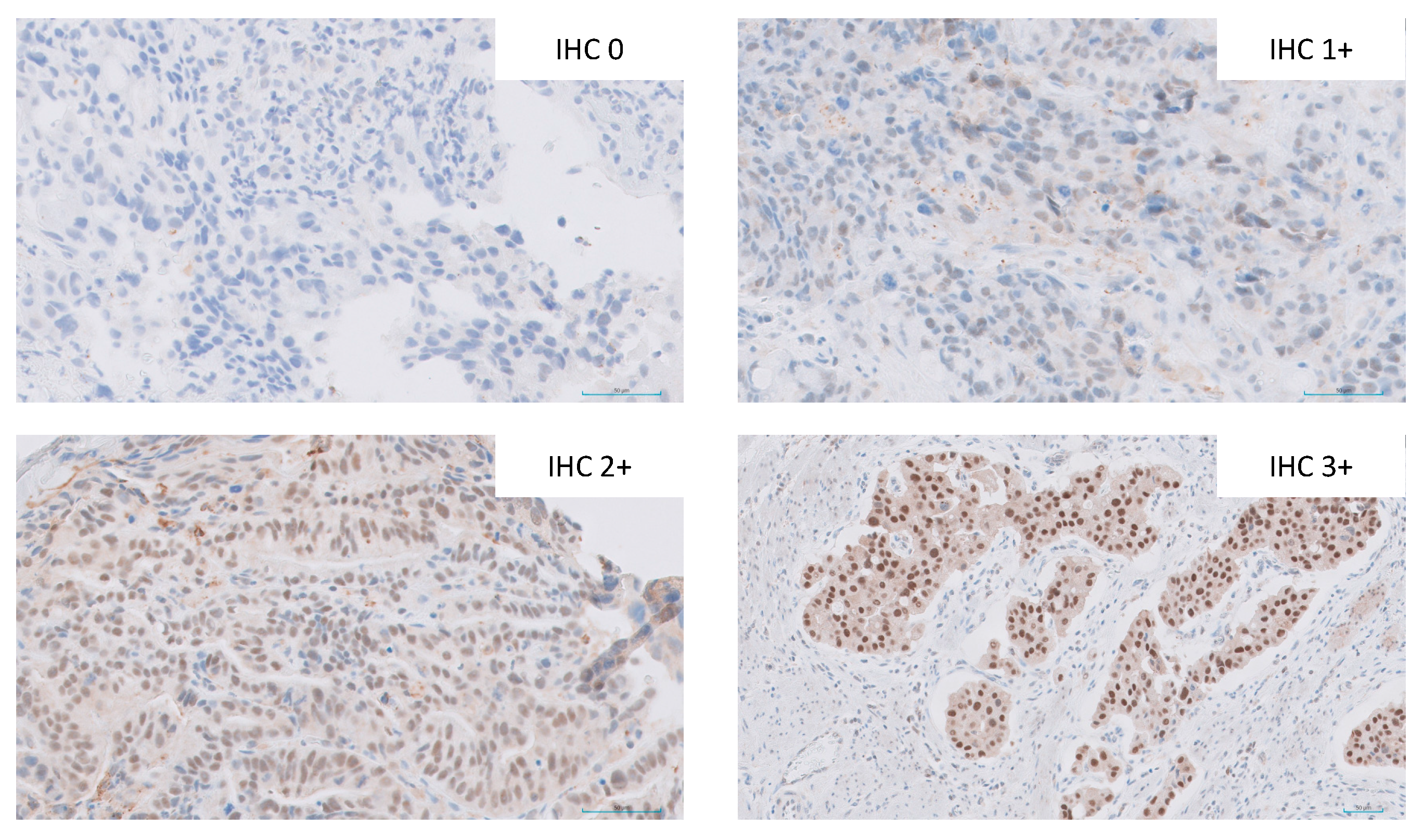
2.2. Immunohistochemistry
3. Results
3.1. Patient Cohort
3.1.1. ERα and ERβ Expression
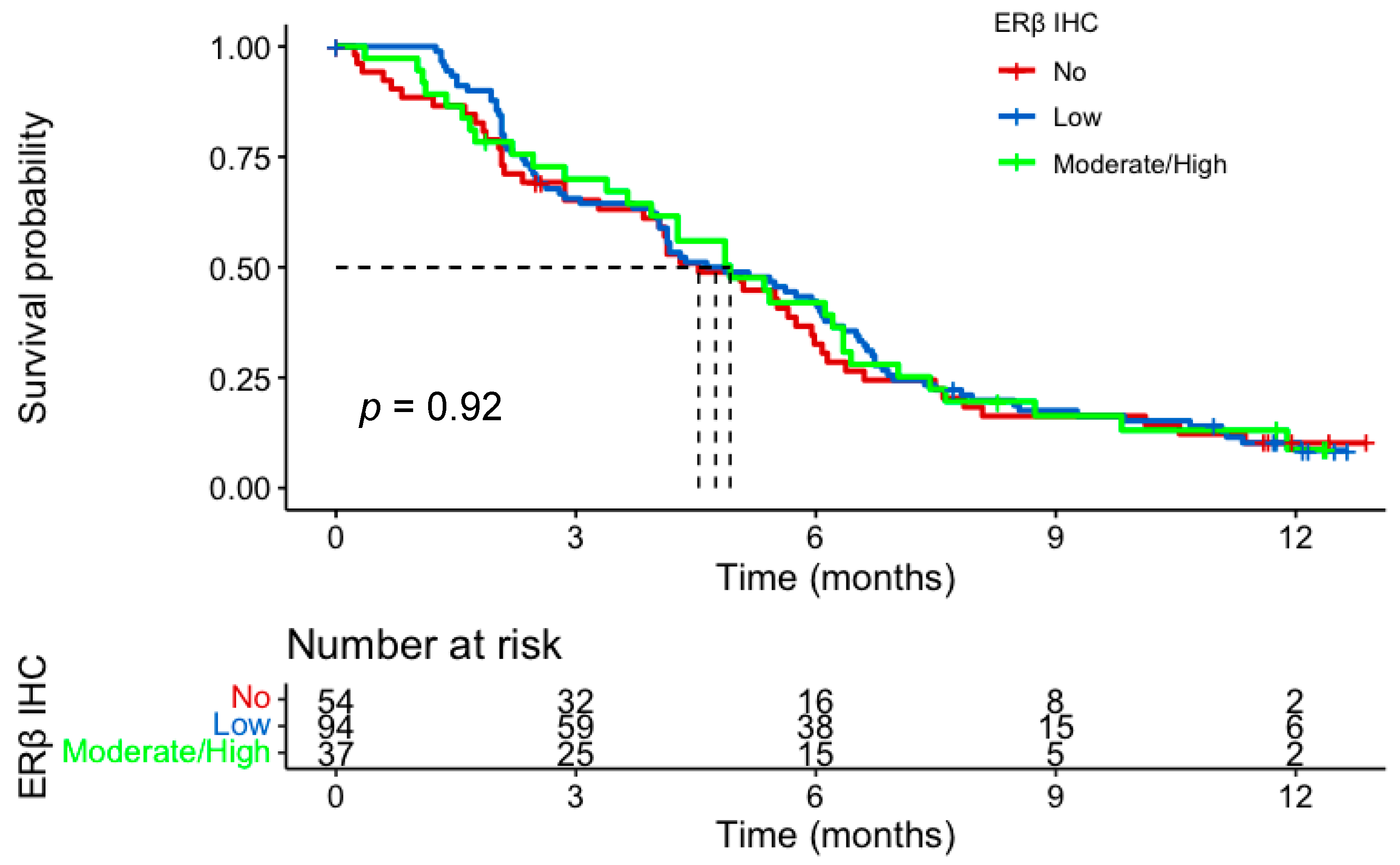
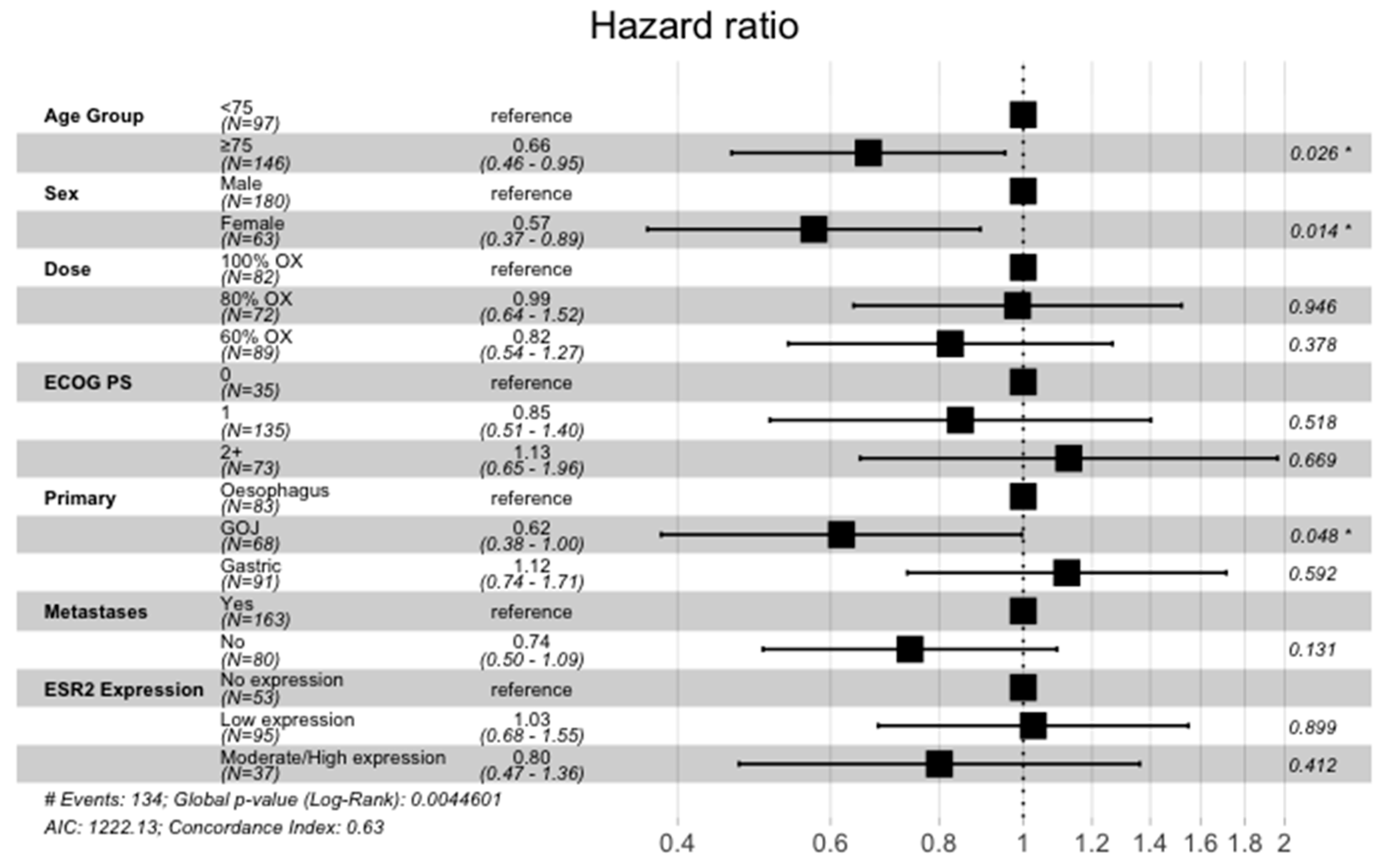
3.1.2. ERβ Expression and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smyth, E.C.; Lagergren, J.; Fitzgerald, R.C.; Lordick, F.; Shah, M.A.; Lagergren, P.; Cunningham, D. Oesophageal cancer. Nat. Rev. Dis. Prim. 2017, 3, 17048. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.; Lordick, F. Gastric cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Starling, N.; Rao, S.; Iveson, T.; Nicolson, M.; Coxon, F.; Middleton, G.; Daniel, F.; Oates, J.; Norman, A.R.; et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N. Engl. J. Med. 2008, 358, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Hall, P.S.; Swinson, D.; Cairns, D.A.; Waters, J.S.; Petty, R.; Allmark, C.; Ruddock, S.; Falk, S.; Wadsley, J.; Roy, R.; et al. Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Quality of Life and Cancer Control Among Older and Frail Patients With Advanced Gastroesophageal Cancer: The GO2 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 869–877. [Google Scholar] [CrossRef]
- Mathieu, L.N.; Kanarek, N.F.; Tsai, H.L.; Rudin, C.M.; Brock, M.V. Age and sex differences in the incidence of esophageal adenocarcinoma: Results from the Surveillance, Epidemiology, and End Results (SEER) Registry (1973–2008). Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2014, 27, 757–763. [Google Scholar] [CrossRef]
- Sipponen, P.; Correa, P. Delayed rise in incidence of gastric cancer in females results in unique sex ratio (M/F) pattern: Etiologic hypothesis. Gastric Cancer 2002, 5, 213–219. [Google Scholar] [CrossRef]
- Persson, C.; Inoue, M.; Sasazuki, S.; Kurahashi, N.; Iwasaki, M.; Ye, W.; Tsugane, S. Female reproductive factors and the risk of gastric cancer in a large-scale population-based cohort study in Japan (JPHC study). Eur. J. Cancer Prev. 2008, 17, 345–353. [Google Scholar] [CrossRef]
- Löfdahl, H.E.; Lu, Y.; Lagergren, J. Sex-specific risk factor profile in oesophageal adenocarcinoma. Br. J. Cancer 2008, 99, 1506–1510. [Google Scholar] [CrossRef]
- Brusselaers, N.; Maret-Ouda, J.; Konings, P.; El-Serag, H.B.; Lagergren, J. Menopausal hormone therapy and the risk of esophageal and gastric cancer. Int. J. Cancer 2017, 140, 1693–1699. [Google Scholar] [CrossRef]
- Lindblad, M.; Rodríguez, L.A.G.; Chandanos, E.; Lagergren, J. Hormone replacement therapy and risks of oesophageal and gastric adenocarcinomas. Br. J. Cancer 2005, 94, 136–141. [Google Scholar] [CrossRef]
- Chandanos, E.; Lindblad, M.; Jia, C.; Rubio, C.A.; Ye, W.; Lagergren, J. Tamoxifen exposure and risk of oesophageal and gastric adenocarcinoma: A population-based cohort study of breast cancer patients in Sweden. Br. J. Cancer 2006, 95, 118–122. [Google Scholar] [CrossRef]
- Wang, B.J.; Zhang, B.; Yan, S.S.; Li, Z.C.; Jiang, T.; Hua, C.J.; Lu, L.; Liu, X.Z.; Zhang, D.H.; Zhang, R.S.; et al. Hormonal and reproductive factors and risk of esophageal cancer in women: A meta-analysis. Dis. Esophagus 2015, 29, 448–454. [Google Scholar] [CrossRef]
- Petrick, J.L.; Hyland, P.L.; Caron, P.; Falk, R.T.; Pfeiffer, R.M.; Dawsey, S.M.; Abnet, C.; Taylor, P.R.; Weinstein, S.J.; Albanes, D.; et al. Associations Between Prediagnostic Concentrations of Circulating Sex Steroid Hormones and Esophageal/Gastric Cardia Adenocarcinoma Among Men. Gynecol. Oncol. 2018, 111, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Morgan, E.; Bardot, A.; Rutherford, M.J.; Ferlay, J.; Little, A.; Møller, B.; Bucher, O.; De, P.; Woods, R.R.; et al. International variation in oesophageal and gastric cancer survival 2012–2014: Differences by histological subtype and stage at diagnosis (an ICBP SURVMARK-2 population-based study). Gut 2021, 71, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- Sugimachi, K.; Matsuoka, H.; Matsufuji, H.; Maekawa, S.; Kai, H.; Okudaira, Y. Survival rates of women with carcinoma of the esophagus exceed those of men. Surg. Gynecol. Obstet. 1987, 164, 541–544. [Google Scholar]
- Morita, M.; Otsu, H.; Kawano, H.; Kasagi, Y.; Kimura, Y.; Saeki, H.; Ando, K.; Ida, S.; Oki, E.; Tokunaga, E.; et al. Gender differences in prognosis after esophagectomy for esophageal cancer. Surg. Today 2013, 44, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, G.G.; Enmark, E.; Pelto-Huikko, M.; Nilsson, S.; Gustafsson, J.A. Cloning of a novel receptor expressed in rat prostate and ovary. Proc. Natl. Acad. Sci. USA 1996, 93, 5925–5930. [Google Scholar] [CrossRef]
- Böttner, M.; Thelen, P.; Jarry, H. Estrogen receptor beta: Tissue distribution and the still largely enigmatic physiological function. J. Steroid Biochem. Mol. Biol. 2013, 139, 245–251. [Google Scholar] [CrossRef]
- Van Herck, Y.; Feyaerts, A.; Alibhai, S.; Papamichael, D.; Decoster, L.; Lambrechts, Y.; Pinchuk, M.; Bechter, O.; Herrera-Caceres, J.; Bibeau, F.; et al. Is cancer biology different in older patients? Lancet Healthy Longev. 2021, 2, e663–e677. [Google Scholar] [CrossRef]
- McMenamin, C.; Trainor, J.; Coleman, H.G.; McManus, D.T.; McQuaid, S.; Bingham, V.; James, J.; Salto-Tellez, M.; Johnston, B.T.; Turkington, R. Sex hormone receptor expression and survival in esophageal adenocarcinoma: A prospective cohort study. Oncotarget 2018, 9, 35300–35312. [Google Scholar] [CrossRef]
- Kalayarasan, R.; Ananthakrishnan, N.; Kate, V.; Basu, D. Estrogen and progesterone receptors in esophageal carcinoma. Dis. Esophagus 2008, 21, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Al-Khyatt, W.; Tufarelli, C.; Khan, R.; Iftikhar, S.Y. Selective oestrogen receptor antagonists inhibit oesophageal cancer cell proliferation in vitro. BMC Cancer 2018, 18, 121. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Chirala, M.; Younes, M. Expression of estrogen receptor-beta isoforms in Barrett’s metaplasia, dysplasia and esophageal adenocarcinoma. Anticancer Res. 2004, 24, 2919–2924. [Google Scholar] [PubMed]
- Akgun, H.; Lechago, J.; Younes, M. Estrogen receptor-beta is expressed in Barrett’s metaplasia and associated adenocarcinoma of the esophagus. Anticancer Res. 2002, 22, 1459–1461. [Google Scholar]
- Tiffin, N.; Suvarna, S.K.; Trudgill, N.J.; Riley, S.A. Sex hormone receptor immunohistochemistry staining in Barrett’s oesophagus and adenocarcinoma. Histopathology 2003, 42, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Liu, R.; Yan, Y.; Pan, X.; Wang, M.; Han, X.; Ren, H.; Zhang, Z. Expression of estrogen receptors and androgen receptor and their clinical significance in gastric cancer. Oncotarget 2017, 8, 40765–40777. [Google Scholar] [CrossRef]
- Gan, L.; He, J.; Zhang, X.; Zhang, Y.-J.; Yu, G.-Z.; Chen, Y.; Pan, J.; Wang, J.-J.; Wang, X. Expression profile and prognostic role of sex hormone receptors in gastric cancer. BMC Cancer 2012, 12, 566. [Google Scholar] [CrossRef]
- Xu, C.Y.; Guo, J.L.; Jiang, Z.N.; Xie, S.D.; Shen, J.G.; Shen, J.Y.; Wang, L.B. Prognostic role of estrogen receptor alpha and estrogen receptor beta in gastric cancer. Ann. Surg. Oncol. 2010, 17, 2503–2509. [Google Scholar] [CrossRef]
- DA Silva, A.C.C.; Pereira, M.A.; Ramos, M.F.K.P.; Cardili, L.; Ribeiro, U., Jr.; Zilberstein, B.; Mello, E.S.; Castria, T.B. Gastric cancer with positive expression of estrogen receptor alpha: A case series from a single western center. Arq. Bras. Cir. Dig. 2022, 34, e1635. [Google Scholar] [CrossRef]
- Wang, M.; Pan, J.-Y.; Song, G.-R.; Chen, H.-B.; An, L.-J.; Qu, S.-X. Altered expression of estrogen receptor alpha and beta in advanced gastric adenocarcinoma: Correlation with prothymosin alpha and clinicopathological parameters. Eur. J. Surg. Oncol. (EJSO) 2007, 33, 195–201. [Google Scholar] [CrossRef]
- Zhou, F.; Xu, Y.; Shi, J.; Lan, X.; Zou, X.; Wang, L.; Huang, Q. Expression profile of E-cadherin, estrogen receptors, and P53 in early-onset gastric cancers. Cancer Med. 2016, 5, 3403–3411. [Google Scholar] [CrossRef] [PubMed]
- Ryu, W.-S.; Kim, J.-H.; Jang, Y.-J.; Park, S.-S.; Um, J.-W.; Park, S.-H.; Kim, S.-J.; Mok, Y.-J.; Kim, C.-S. Expression of estrogen receptors in gastric cancer and their clinical significance. J. Surg. Oncol. 2012, 106, 456–461. [Google Scholar] [CrossRef]
- Jukic, Z.; Radulovic, P.; Stojković, R.; Mijic, A.; Grah, J.; Kruslin, B.; Ferencic, Z.; Fucic, A. Gender Difference in Distribution of Estrogen and Androgen Receptors in Intestinal-type Gastric Cancer. Anticancer Res. 2017, 37, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Allred, D.C.; Clark, G.M.; Elledge, R.; Fuqua, S.A.W.; Brown, R.W.; Chamness, G.C.; Osborne, C.K.; McGuire, W.L. Association of p53 Protein Expression With Tumor Cell Proliferation Rate and Clinical Outcome in Node-Negative Breast Cancer. Gynecol. Oncol. 1993, 85, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Hendifar, A.; Lenz, C.; Togawa, K.; Lenz, F.; Lurje, G.; Pohl, A.; Winder, T.; Ning, Y.; Groshen, S.; et al. Survival of metastatic gastric cancer: Significance of age, sex and race/ethnicity. J. Gastrointest. Oncol. 2011, 2, 77–84. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ESR2 IHC Expression Group | ||||
|---|---|---|---|---|
| No Expression | Low Expression | Moderate/High Expression | p-Value | |
| (N = 57) | (N = 98) | (N = 39) | (q-Value) * | |
| Age Group | ||||
| <65 | 8 (14.0%) | 4 (4.1%) | 3 (7.7%) | 0.151 |
| 65–75 | 15 (26.3%) | 39 (39.8%) | 15 (38.5%) | (0.483) |
| >75 | 34 (59.6%) | 55 (56.1%) | 21 (53.8%) | |
| Sex | ||||
| Male | 38 (66.7%) | 76 (77.6%) | 31 (79.5%) | 0.241 |
| Female | 19 (33.3%) | 22 (22.4%) | 8 (20.5%) | (0.483) |
| ECOG PS | ||||
| 0 | 8 (14.0%) | 10 (10.2%) | 8 (20.5%) | 0.434 |
| 1 | 31 (54.4%) | 62 (63.3%) | 19 (48.7%) | (0.652) |
| 2+ | 18 (31.6%) | 26 (26.5%) | 12 (30.8%) | |
| Dose Level | ||||
| 100% OX | 20 (35.1%) | 37 (37.8%) | 9 (23.1%) | 0.2 |
| 80% OX | 16 (28.1%) | 32 (32.7%) | 10 (25.6%) | (0.483) |
| 60% OX | 21 (36.8%) | 29 (29.6%) | 20 (51.3%) | |
| Primary Site | ||||
| Oesophagus | 19 (33.3%) | 34 (34.7%) | 10 (25.6%) | 0.779 |
| GOJ | 18 (31.6%) | 29 (29.6%) | 11 (28.2%) | (0.827) |
| Gastric | 20 (35.1%) | 35 (35.7%) | 18 (46.2%) | |
| Metastasis present | ||||
| Metastasis | 36 (63.2%) | 64 (65.3%) | 27 (69.2%) | 0.827 |
| No metastasis | 21 (36.8%) | 34 (34.7%) | 12 (30.8%) | (0.827) |
| GO2 Frailty Group | ||||
| No/mild frailty | 7 (12.3%) | 15 (15.3%) | 11 (28.2%) | 0.109 |
| Moderate frailty | 19 (33.3%) | 22 (22.4%) | 6 (15.4%) | (0.422) |
| Severe frailty | 31 (54.4%) | 61 (62.2%) | 22 (56.4%) | |
| Age Group | ||||
|---|---|---|---|---|
| <65 (N = 15) | 65–75 (N = 69) | >75 (N = 110) | p-Value (q-Value) * | |
| ERβ expression | ||||
| No expression | 8 (53.3%) | 15 (21.7%) | 34 (30.9%) | 0.045 |
| Positive expression | 7 (46.7%) | 54 (78.3%) | 76 (69.1%) | −0.045 |
| Author | Year | Site | Age | Setting | Number | ERα | ERβ | Survival |
|---|---|---|---|---|---|---|---|---|
| Oesophageal Cancer | ||||||||
| McMenamin [20] | 2018 | EAC | Mean 63 | Radical | 139 | 4% | 31% | ERα—no impact on survival ERβ—non-significant improvements |
| Kalayarasan [21] | 2008 | GOA | Mean 57.6 | All stages | 15 | 0% | 100% | - |
| Al-Khyatt [22] | 2018 | OAC | Median 65 (range 30–79) | Radical | 28 | 2.9% | 41.2% | ERα and ERβ—poorer survival |
| Liu [23] | 2004 | OAC | Not available | Radical | 27 | - | ERβ1 85% ERβ2 81% ERβ3 100% ERβ5 100% | - |
| Akgun [24] | 2002 | OAC | Not available | Radical | 23 | - | 100% | - |
| Tiffan [25] | 2003 | OAC | Range 29–90 | Radical | 20 | 40% | - | - |
| Gastric Cancer | ||||||||
| Tang [26] | 2017 | Gastric | Median 58 | All stages | 150/153 | 6% | 93.5% | ERα—poorer survival ERβ—non-significant poorer survival |
| Gan [27] | 2012 | Gastric | Not available | All stages | 848/823 | 12% | 91.9% | ERα—improved survival ERβ—no impact on survival |
| Xu [28] | 2010 | Gastric | Mean 57 Range 31–79 | Radical | 211 | 25.6% | 49.3% | ERα—poorer survival ERβ—better survival |
| Da Silva [29] | 2022 | Gastric | Mean 62.4 | All stages | 345 | 1.8% | 98.2% | ERα—no impact on survival ERβ—no impact on survival |
| Wang [30] | 2007 | Gastric | Median 60 (range 32–87) | All stages | 39 | 18.2% | 43.6% | - |
| Zhou [31] | 2016 | Gastric | All under 40 (mean 33.8) | Radical | 139 | 49.6% | 87.8% | ERα—no impact on survival ERβ—no impact on survival |
| Ryu [32] | 2012 | Gastric | Unknown | Radical | 148 | - | 45.3% | ERβ—no impact on survival |
| Jukic [33] | 2017 | Gastric | Mean 69 Range 35–90 | Radical | 60 | 20% | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baxter, M.A.; Spender, L.C.; Walsh, S.; Bray, S.; Skinner, G.; King, S.; Hall, P.S.; Seymour, M.J.; Petty, R.D.; on behalf of the GO2 Investigators. Female Sex but Not Oestrogen Receptor Expression Predicts Survival in Advanced Gastroesophageal Adenocarcinoma—A Post-hoc Analysis of the GO2 Trial. Cancers 2023, 15, 2591. https://doi.org/10.3390/cancers15092591
Baxter MA, Spender LC, Walsh S, Bray S, Skinner G, King S, Hall PS, Seymour MJ, Petty RD, on behalf of the GO2 Investigators. Female Sex but Not Oestrogen Receptor Expression Predicts Survival in Advanced Gastroesophageal Adenocarcinoma—A Post-hoc Analysis of the GO2 Trial. Cancers. 2023; 15(9):2591. https://doi.org/10.3390/cancers15092591
Chicago/Turabian StyleBaxter, Mark A., Lindsay C. Spender, Shaun Walsh, Susan Bray, Gemma Skinner, Sharon King, Peter S. Hall, Matthew J. Seymour, Russell D. Petty, and on behalf of the GO2 Investigators. 2023. "Female Sex but Not Oestrogen Receptor Expression Predicts Survival in Advanced Gastroesophageal Adenocarcinoma—A Post-hoc Analysis of the GO2 Trial" Cancers 15, no. 9: 2591. https://doi.org/10.3390/cancers15092591