

Perioperative Cetuximab with Cisplatin and 5-Fluorouracil in Esogastric Adenocarcinoma: A Phase II Study
 , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Background
2. Patients and Methods
2.1. Study Population
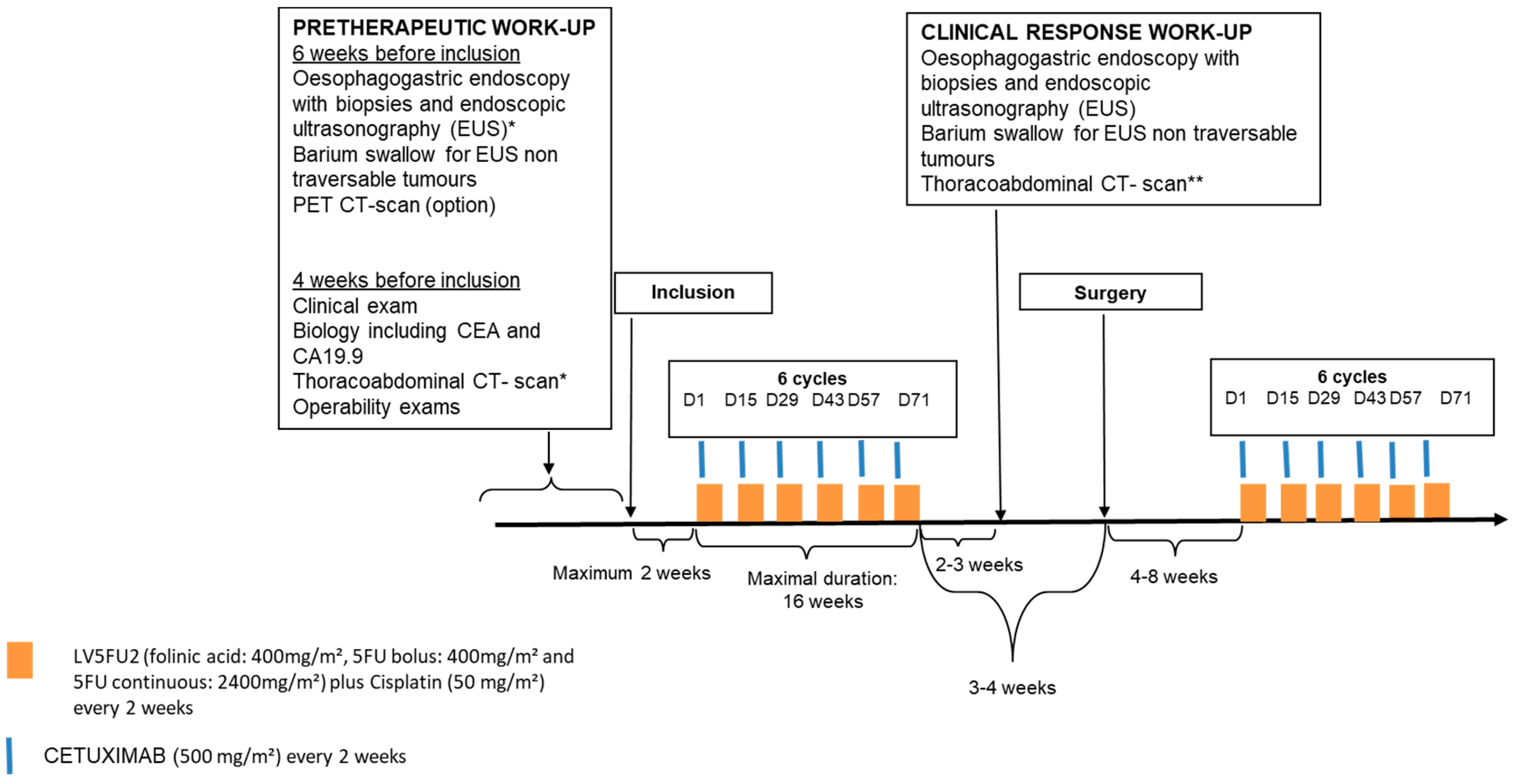
2.2. Study Design and Treatment (Figure 1)

2.3. Evaluation Criteria
2.4. Statistical Analysis
3. Results
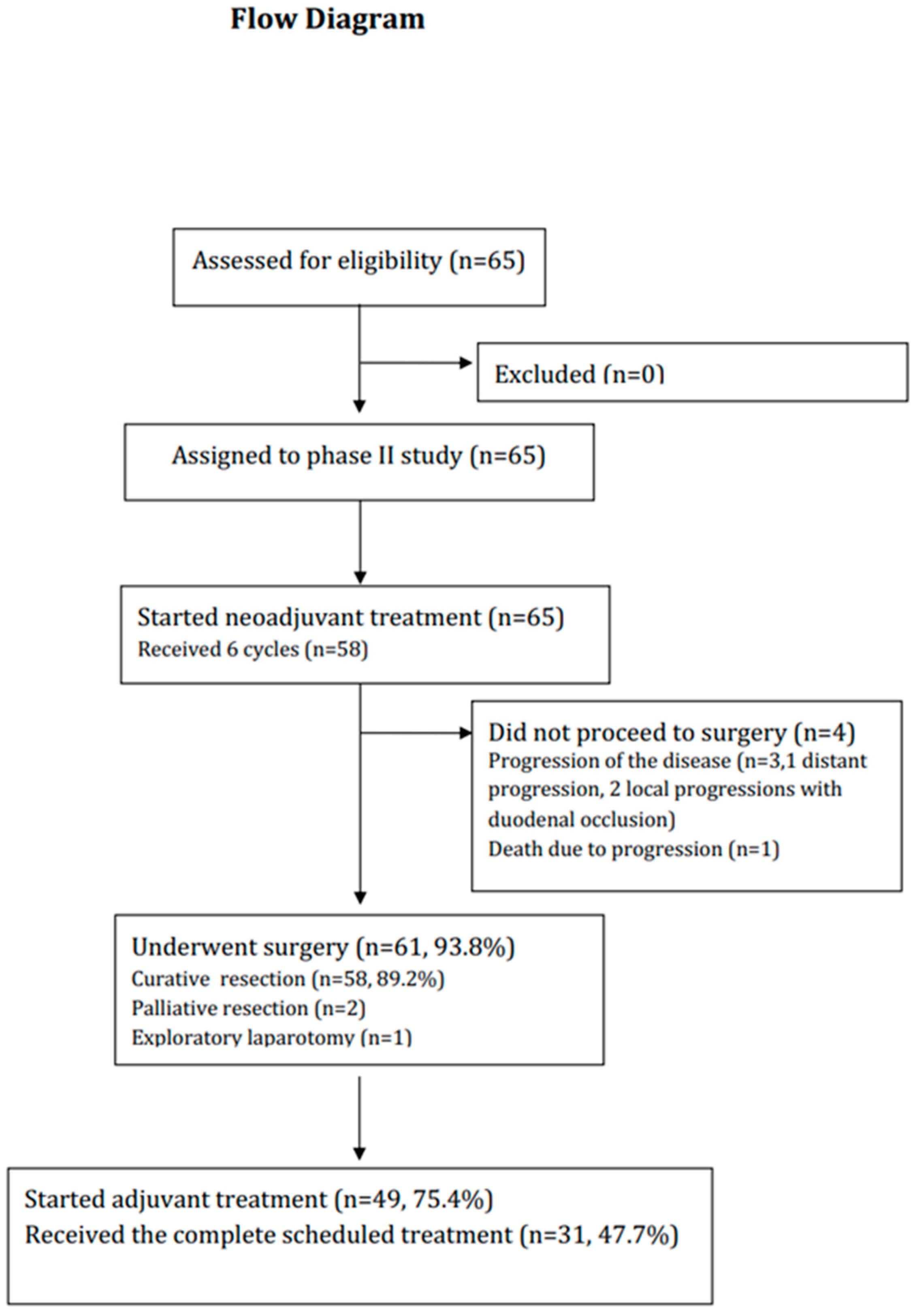
3.1. Patients
3.2. Neoadjuvant Chemotherapy
3.3. Primary Endpoint: Major Toxicities Leading to Discontinuation of Neoadjuvant CT and TOR
3.4. Surgical Treatment and Postoperative Outcomes
3.5. Adjuvant Chemotherapy
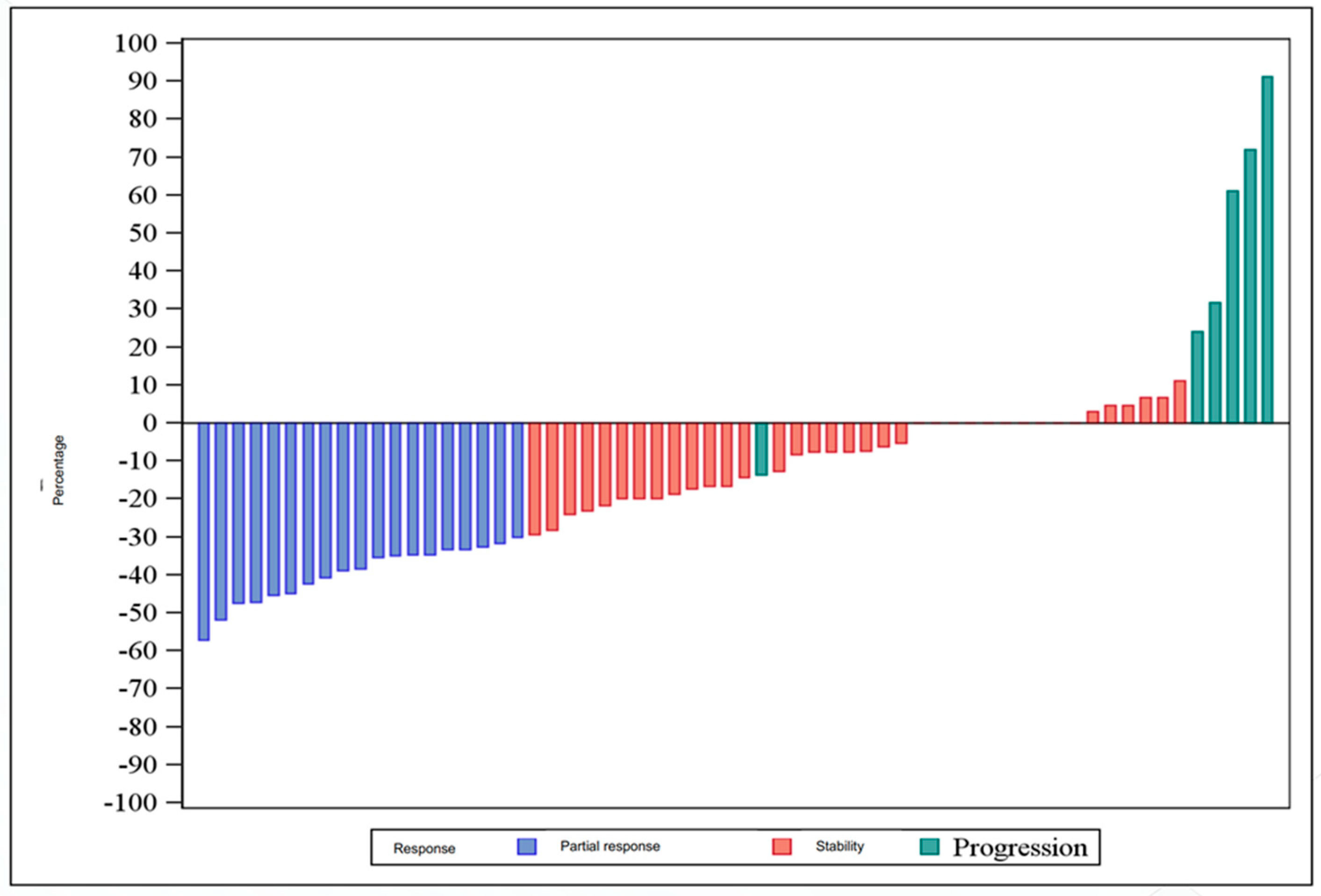
3.6. Efficacy
3.7. Health-Related Quality of Life
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blot, W.J.; Devesa, S.S.; Kneller, R.W.; Fraumeni, J.F. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 1991, 265, 1287–1289. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar] [CrossRef]
- Zaanan, A.; Bouché, O.; Benhaim, L.; Buecher, B.; Chapelle, N.; Dubreuil, O.; Fares, N.; Granger, V.; Lefort, C.; Gagniere, J.; et al. Gastric cancer: French intergroup clinical practice guidelines for diagnosis, treatments and follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO). Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2018, 50, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; Committee, E.G. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27 (Suppl. 5), v38–v49. [Google Scholar] [CrossRef]
- Ychou, M.; Boige, V.; Pignon, J.-P.; Conroy, T.; Bouché, O.; Lebreton, G.; Ducourtieux, M.; Bedenne, L.; Fabre, J.-M.; Saint-Aubert, B.; et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Alderson, D.; Cunningham, D.; Nankivell, M.; Blazeby, J.M.; Griffin, S.M.; Crellin, A.; Grabsch, H.I.; Langer, R.; Pritchard, S.; Okines, A.; et al. Neoadjuvant cisplatin and fluorouracil versus epirubicin, cisplatin, and capecitabine followed by resection in patients with oesophageal adenocarcinoma (UK MRC OE05): An open-label, randomised phase 3 trial. Lancet Oncol. 2017, 18, 1249–1260. [Google Scholar] [CrossRef] [Green Version]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.-G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef]
- De Mestier, L.; Lardière-Deguelte, S.; Volet, J.; Kianmanesh, R.; Bouché, O. Recent insights in the therapeutic management of patients with gastric cancer. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2016, 48, 984–994. [Google Scholar] [CrossRef]
- Moehler, M.; Mueller, A.; Trarbach, T.; Lordick, F.; Seufferlein, T.; Kubicka, S.; Geißler, M.; Schwarz, S.; Galle, P.; Kanzler, S. Cetuximab with irinotecan, folinic acid and 5-fluorouracil as first-line treatment in advanced gastroesophageal cancer: A prospective multi-center biomarker-oriented phase II study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2011, 22, 1358–1366. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, J. Targeting the epidermal growth factor receptor for cancer therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20 (Suppl. 18), 1S–13S. [Google Scholar]
- Salomon, D.S.; Brandt, R.; Ciardiello, F.; Normanno, N. Epidermal growth factor-related peptides and their receptors in human malignancies. Crit. Rev. Oncol. Hematol. 1995, 19, 183–232. [Google Scholar] [CrossRef]
- Wang, K.L.; Wu, T.-T.; Choi, I.S.; Wang, H.; Resetkova, E.; Correa, A.M.; Hofstetter, W.L.; Swisher, S.G.; Ajani, J.A.; Rashid, A.; et al. Expression of epidermal growth factor receptor in esophageal and esophagogastric junction adenocarcinomas: Association with poor outcome. Cancer 2007, 109, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Pinto, C.; Di Fabio, F.; Barone, C.; Siena, S.; Falcone, A.; Cascinu, S.; Llimpe, F.L.R.; Stella, G.; Schinzari, G.; Artale, S.; et al. Phase II study of cetuximab in combination with cisplatin and docetaxel in patients with untreated advanced gastric or gastro-oesophageal junction adenocarcinoma (DOCETUX study). Br. J. Cancer 2009, 101, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariette, C.; Balon, J.M.; Maunoury, V.; Taillier, G.; Van Seuningen, I.; Triboulet, J.P. Value of endoscopic ultrasonography as a predictor of long-term survival in oesophageal carcinoma. Br. J. Surg. 2003, 90, 1367–1372. [Google Scholar] [CrossRef]
- Siewert, J.R.; Stein, H.J. Classification of adenocarcinoma of the oesophagogastric junction. Br. J. Surg. 1998, 85, 1457–1459. [Google Scholar] [CrossRef]
- Tio, T.L.; Coene, P.P.; den Hartog Jager, F.C.; Tytgat, G.N. Preoperative TNM classification of esophageal carcinoma by endosonography. Hepatogastroenterology 1990, 37, 376–381. [Google Scholar]
- Mariette, C.; Piessen, G.; Briez, N.; Triboulet, J.P. The number of metastatic lymph nodes and the ratio between metastatic and examined lymph nodes are independent prognostic factors in esophageal cancer regardless of neoadjuvant chemoradiation or lymphadenectomy extent. Ann. Surg. 2008, 247, 365–371. [Google Scholar] [CrossRef]
- Hermanek, P. pTNM and residual tumor classifications: Problems of assessment and prognostic significance. World J. Surg. 1995, 19, 184–190. [Google Scholar] [CrossRef]
- Strong, V.E.; D’Amico, T.A.; Kleinberg, L.; Ajani, J. Impact of the 7th Edition AJCC staging classification on the NCCN clinical practice guidelines in oncology for gastric and esophageal cancers. J. Natl. Compr. Cancer Netw. 2013, 11, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Mandard, A.-M.; Dalibard, F.; Mandard, J.-C.; Marnay, J.; Henry-Amar, M.; Petiot, J.-F.; Roussel, A.; Jacob, J.-H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Available online: https://www.eortc.org/app/uploads/sites/2/2018/08/Specimen-QLQ-C30-English.pdf (accessed on 2 February 2023).
- Blazeby, J.M.; Conroy, T.; Bottomley, A.; Vickery, C.; Arraras, J.; Sezer, O.; Moore, J.; Koller, M.; Turhal, N.; Stuart, R.; et al. Clinical and psychometric validation of a questionnaire module, the EORTC QLQ-STO 22, to assess quality of life in patients with gastric cancer. Eur. J. Cancer 2004, 40, 2260–2268. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/Archive/CTCAE_4.0_2009-05-29_QuickReference_8.5x11.pdf (accessed on 2 February 2023).
- Schuhmacher, C.; Gretschel, S.; Lordick, F.; Reichardt, P.; Hohenberger, W.; Eisenberger, C.F.; Haag, C.; Mauer, M.E.; Hasan, B.; Welch, J.; et al. Neoadjuvant chemotherapy compared with surgery alone for locally advanced cancer of the stomach and cardia: European Organisation for Research and Treatment of Cancer randomized trial 40954. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 5210–5218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, C.; Di Fabio, F.; Siena, S.; Cascinu, S.; Llimpe, F.R.; Ceccarelli, C.; Mutri, V.; Giannetta, L.; Giaquinta, S.; Funaioli, C.; et al. Phase II study of cetuximab in combination with FOLFIRI in patients with untreated advanced gastric or gastroesophageal junction adenocarcinoma (FOLCETUX study). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2007, 18, 510–517. [Google Scholar] [CrossRef]
- Lordick, F.; Luber, B.; Lorenzen, S.; Hegewisch-Becker, S.; Folprecht, G.; Wöll, E.; Decker, T.; Endlicher, E.; Röthling, N.; Schuster, T.; et al. Cetuximab plus oxaliplatin/leucovorin/5-fluorouracil in first-line metastatic gastric cancer: A phase II study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Br. J. Cancer 2010, 102, 500–505. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Kang, Y.-K.; Chung, H.-C.; Salman, P.; Oh, S.C.; Bodoky, G.; Kurteva, G.; Volovat, C.; Moiseyenko, V.M.; Gorbunova, V.; et al. Capecitabine and cisplatin with or without cetuximab for patients with previously untreated advanced gastric cancer (EXPAND): A randomised, open-label phase 3 trial. Lancet Oncol. 2013, 14, 490–499. [Google Scholar] [CrossRef]
- Waddell, T.; Chau, I.; Cunningham, D.; Gonzalez, D.; Okines, A.F.C.; Wotherspoon, A.; Saffery, C.; Middleton, G.; Wadsley, J.; Ferry, D.; et al. Epirubicin, oxaliplatin, and capecitabine with or without panitumumab for patients with previously untreated advanced oesophagogastric cancer (REAL3): A randomised, open-label phase 3 trial. Lancet Oncol. 2013, 14, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Malka, D.; François, E.; Penault-Llorca, F.; Castan, F.; Bouché, O.; Bennouna, J.; Ghiringhelli, F.; de la Fouchardière, C.; Borg, C.; Samalin, E.; et al. FOLFOX alone or combined with rilotumumab or panitumumab as first-line treatment for patients with advanced gastroesophageal adenocarcinoma (PRODIGE 17-ACCORD 20-MEGA): A randomised, open-label, three-arm phase II trial. Eur. J. Cancer 2019, 115, 97–106. [Google Scholar] [CrossRef]
- Ruhstaller, T.; Pless, M.; Dietrich, D.; Kranzbuehler, H.; von Moos, R.; Moosmann, P.; Montemurro, M.; Schneider, P.M.; Rauch, D.; Gautschi, O.; et al. Cetuximab in combination with chemoradiotherapy before surgery in patients with resectable, locally advanced esophageal carcinoma: A prospective, multicenter phase IB/II Trial (SAKK 75/06). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Becerra, C.R.; Hanna, N.; McCollum, A.D.; Becharm, N.; Timmerman, R.D.; DiMaio, M.; Kesler, K.A.; Yu, M.; Yan, T.; alChoy, H. A phase II study with cetuximab and radiation therapy for patients with surgically resectable esophageal and GE junction carcinomas: Hoosier Oncology Group G05-92. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2013, 8, 1425–1429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.S.; Mamon, H.J.; Hong, T.S.; Choi, N.C.; Fidias, P.M.; Kwak, E.L.; Meyerhardt, J.A.; Ryan, D.P.; Bueno, R.; Donahue, D.M.; et al. Preoperative cetuximab, irinotecan, cisplatin, and radiation therapy for patients with locally advanced esophageal cancer. Oncologist 2013, 18, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Suntharalingam, M.; Winter, K.; Ilson, D.; Dicker, A.P.; Kachnic, L.; Konski, A.; Chakravarthy, A.B.; Anker, C.J.; Thakrar, H.; Horiba, N.; et al. Effect of the Addition of Cetuximab to Paclitaxel, Cisplatin, and Radiation Therapy for Patients With Esophageal Cancer: The NRG Oncology RTOG 0436 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2017, 3, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Crosby, T.; Hurt, C.N.; Falk, S.; Gollins, S.; Mukherjee, S.; Staffurth, J.; Ray, R.; Bashir, N.; Bridgewater, J.; Geh, J.I.; et al. Chemoradiotherapy with or without cetuximab in patients with oesophageal cancer (SCOPE1): A multicentre, phase 2/3 randomised trial. Lancet Oncol. 2013, 14, 627–637. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Köhne, C.-H.; Láng, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: Updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Fu, R.; Hu, Y.; Du, H.; Li, S.; Li, Z.; Liu, Y.; Li, Q.; Zhang, L.; Ji, J. EGFR gene status predicts response and survival benefit in a preclinical gastric cancer trial treating patient-derived xenografts with cetuximab. Oncol. Rep. 2017, 38, 2387–2393. [Google Scholar] [CrossRef] [Green Version]
- Raimúndez, E.; Keller, S.; Zwingenberger, G.; Ebert, K.; Hug, S.; Thetis, F.J.; Maier, D.; Luber, B.; Hasenauer, J. Model-based analysis of response and resistance factors of cetuximab treatment in gastric cancer cell lines. PLoS Comput. Biol. 2020, 16, e1007147. [Google Scholar] [CrossRef]
- Fontana, E.; Smyth, E.C. Novel targets in the treatment of advanced gastric cancer: A perspective review. Ther. Adv. Med. Oncol. 2016, 8, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Petty, R.D.; Dahle-Smith, A.; Stevenson, D.A.J.; Osborne, A.; Massie, D.; Clark, C.; Murray, G.I.; Dutton, S.J.; Roberts, C.; Chong, I.Y.; et al. Gefitinib and EGFR Gene Copy Number Aberrations in Esophageal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2279–2287. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients, N = 65 (%) |
|---|---|
| Sex | |
| Male | 54 (83.1) |
| Median age, years (range) | 60.5 (40.6–76.7) |
| WHO Performance Status | |
| 0 | 41 (63.1) |
| 1 | 23 (35.4) |
| 2 | 1 (1.5) |
| Malnutrition | 11 (16.9) |
| Primary tumor location | |
| Junctional cancer | 45 (69.2) |
| Siewert type I | 22 (48.9) |
| Siewert type II | 20 (44.4) |
| Siewert type III | 3 (6.7) |
| Gastric cancer | 20 (30.8) |
| Fundus | 3 (15.0) |
| Body | 6 (30.0) |
| Pyloric antrum | 11 (55.0) |
| Echoendoscopy done | 62 (95.4) |
| traversable tumor | 49 (79.0) |
| usT stage | |
| usT1 | 1/49 (2.0) |
| usT2 | 7/49 (14.3) |
| usT3 | 40/49 (81.6) |
| usT4 | 1/49 (2.0) |
| usN stage | |
| usN0 | 8/49 (16.3) |
| usN1 | 41/49 (83.7) |
| Clinical tumor stage at inclusion | |
| II | 14/49 (28.6) |
| III | 35/49 (71.4) |
| Poorly cohesive cells on biopsies | l0/61 (16.4) |
| Neoadjuvant Treatment | Adjuvant Treatment | |||
|---|---|---|---|---|
| AE | Grade 1–2 N = 65 (%) | Grade 3–4 N = 65 (%) | Grade 1–2 N = 49 (%) | Grade 3–4 N = 49 (%) |
| Diarrhea | 21 (32.3) | 3 (4.6) | 26 (53.1) | 1 (2.0) |
| Anorexia | 35 (53.8) | 6 (9.2) | 26 (53.1) | 9 (18.4) |
| Vomiting | 28 (43.1) | 4 (6.2) | 20 (40.8) | 4 (8.2) |
| Nausea | 42 (64.6) | 4 (6.2) | 32 (65.3) | 3 (6.1) |
| Dysphagia | 7 (10.8) | 4 (6.2) | 1 (2.0) | - |
| Constipation | 28 (43.1) | 2 (3.1) | 3 (6.1) | - |
| Stomatitis or mucositis | 36 (55.4) | 5 (7.7) | 18 (36.7) | 1 (2.0) |
| Dyspnea | 4 (6.2) | 1 (1.5) | 4 (8.2) | 2 (4.1) |
| Asthenia | 49 (75.4) | 6 (9.2) | 35 (71.4) | 8 (16.3) |
| Acneiform rash | 55 (84.6) | 5 (7.7) | 33 (67.3) | 4 (8.2) |
| Hand-foot syndrome | 6 (9.2) | 1 (1.5) | 2 (4.1) | - |
| Xerosis | 23 (35.4) | - | 11 (22.4) | - |
| Leukopenia | 37 (56.9) | 4 (6.2) | 25 (51.0) | 1 (2.0) |
| Neutropenia | 31 (47.7) | 18 (27.7) | 26 (53.1) | 5 (10.2) |
| Anemia | 53 (81.5) | 1 (1.5) | 45 (91.8) | 1 (2.0) |
| Thrombocytopenia | 35 (53.8) | - | 16 (32.7) | - |
| Serum AST | 5 (7.7) | - | 3 (6.1) | - |
| Serum ALT | 3 (4.6) | - | 7 (14.3) | - |
| Serum GGT | 17 (26.2) | 1 (1.5) | 18 (36.7) | 1 (2.0) |
| Alkaline phosphatase | 6 (9.2) | - | 8 (16.3) | - |
| Fever | 8 (12.3) | - | 2 (4.1) | - |
| Peripheral neuropathy | 7 (10.8) | - | 4 (8.2) | 1 (2.0) |
| Pain | 16 (24.6) | - | 10 (20.4) | 1 (2.0) |
| Alopecia | 14 (21.5) | - | 8 (16.3) | - |
| Renal insufficiency | 1 (1.5) | 1 (1.5) | 3 (6.1) | 2 (4.1) |
| Infection | 4 (6.2) | 1 (1.5) | 4 (8.2) | 2 (2.1) |
| Thrombosis | 3 (4.6) | 3 (4.6) | - | 1 (2.0) |
| Toxic death | - | - | - | - |
| N (%), n = 60 | |
|---|---|
| Surgical procedure | |
| Ivor Lewis procedure | 38 (63.4) |
| Total esogastrectomy with intrathoracic anastomosis | 13 (21.7) |
| Distal gastrectomy | 5 (8.3) |
| Total gastrectomy | 4 (6.7) |
| 30-day overall morbidity (n = 59) | 33 (55.9) |
| Significant postoperative complications | 25 (41.7) |
| 30-day postoperative deaths | 2 (3.3) |
| Surgical complications | 16 (26.7) |
| -anastomotic leak | 4 |
| -vocal cord paralysis | 2 |
| -intra-abdominal abscess | 3 |
| -wound infection | 2 |
| -gastroplasty necrosis | 2 |
| -small bowel occlusion | 2 |
| -chylothorax | 2 |
| -pancreatitis | 1 |
| -repeat surgery | 8 |
| Medical complications (%, n = 59) | 14 (23.7) |
| -pulmonary | 11 (18.6) |
| -cardiovascular | 6 (10.2) |
| -neurologic | 3 (5.1) |
| -renal | 2 (3.4) |
| -hepatic | 0 (0) |
| -sepsis | 4 (6.8) |
| Tumor differentiation (%, n = 55) | |
| Good | 15 (27.3) |
| Moderate | 18 (32.7) |
| Poor | 22 (40.0) |
| Median number of harvested lymph nodes | 25 [7–60] |
| Median percentage of invaded lymph nodes among harvested lymph nodes | 4.9 % [0–73] |
| Radicality of resection (%, n = 59) | |
| R0 | 53 (89.8) |
| R1 | 5(8.5) |
| R2 | 1 (1.7) |
| Tumor response (%, n = 56) | |
| pCR: no residual tumor cells | 4 (7.1) |
| pPR: rare residual tumor cells or more fibrosis without tumor cells | 12 (21.4) |
| pNR: more tumor cells than fibrosis or no histologic sign of response to chemotherapy | 40 (71.4) |
| pT0 | 3 (5.0) |
| pT1 | 7 (11.7) |
| pT2 | 5 (8.3) |
| pT3 | 38 (63.3) |
| pT4a | 6 (10.0) |
| pT4b | 1 (1.7) |
| pN0 | 23 (38.3) |
| pN1 | 14 (23.3) |
| pN2 | 11 (18.3) |
| pN3a | 11 (18.3) |
| pN3b | 1 (1.7) |
| pM0 | 59 (98.3) |
| pM1 | 1 (1.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gronnier, C.; Mariette, C.; Lepage, C.; Monterymard, C.; Jary, M.; Ferru, A.; Baconnier, M.; Adhoute, X.; Tavan, D.; Perrier, H.; et al. Perioperative Cetuximab with Cisplatin and 5-Fluorouracil in Esogastric Adenocarcinoma: A Phase II Study. Cancers 2023, 15, 2188. https://doi.org/10.3390/cancers15072188
Gronnier C, Mariette C, Lepage C, Monterymard C, Jary M, Ferru A, Baconnier M, Adhoute X, Tavan D, Perrier H, et al. Perioperative Cetuximab with Cisplatin and 5-Fluorouracil in Esogastric Adenocarcinoma: A Phase II Study. Cancers. 2023; 15(7):2188. https://doi.org/10.3390/cancers15072188
Chicago/Turabian StyleGronnier, Caroline, Christophe Mariette, Come Lepage, Carole Monterymard, Marine Jary, Aurélie Ferru, Mathieu Baconnier, Xavier Adhoute, David Tavan, Hervé Perrier, and et al. 2023. "Perioperative Cetuximab with Cisplatin and 5-Fluorouracil in Esogastric Adenocarcinoma: A Phase II Study" Cancers 15, no. 7: 2188. https://doi.org/10.3390/cancers15072188