

Functional Alteration in the Brain Due to Tumour Invasion in Paediatric Patients: A Systematic Review
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
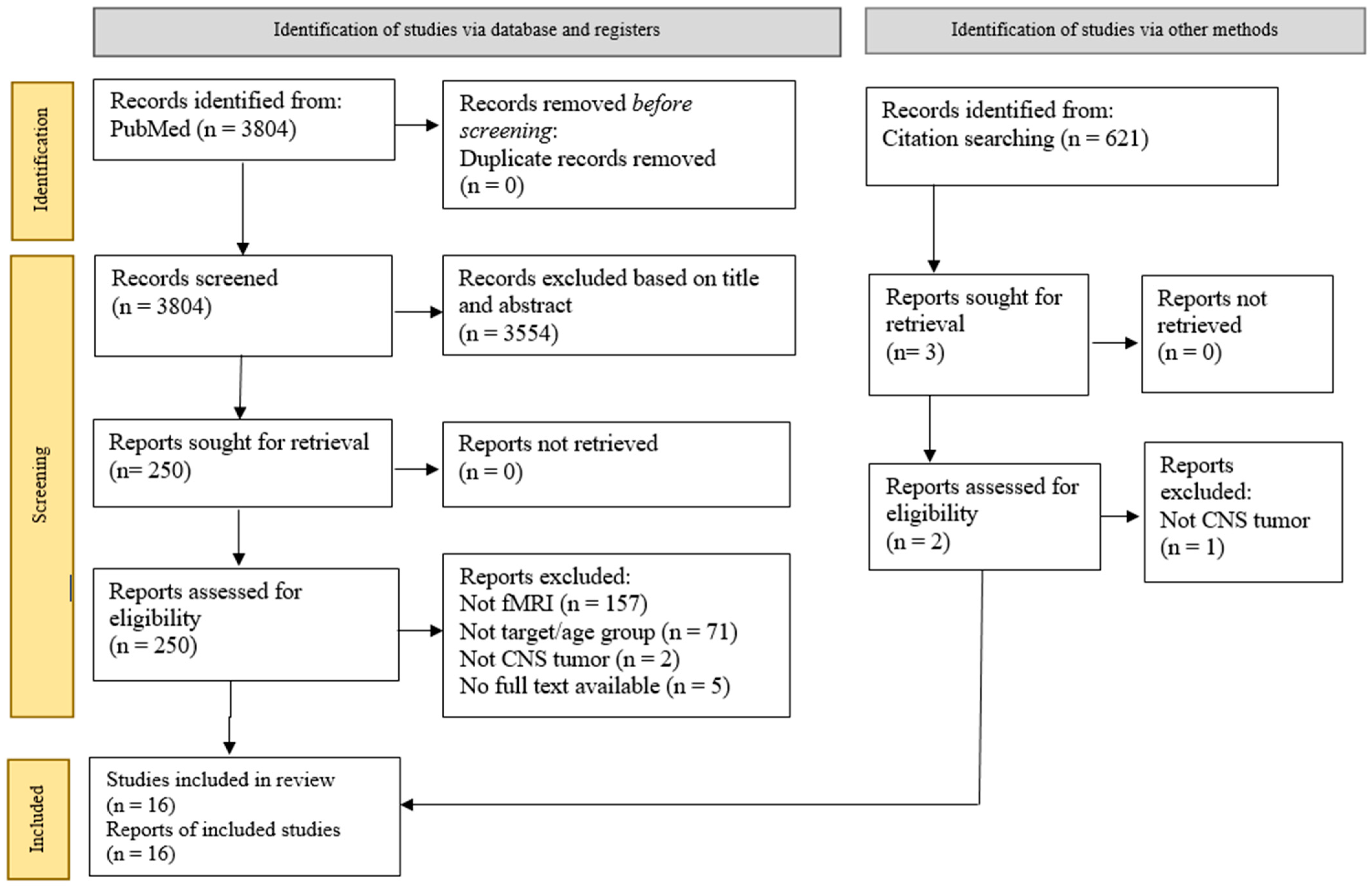
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. PICOS and Inclusion and Exclusion Criteria
3. Results
3.1. Data Extraction and Study Design
3.2. Participants
3.3. Resting-State fMRI
3.3.1. Working Memory Assessment
3.3.2. Language and Speech Alterations
3.3.3. Sensory or Motor Alterations
3.3.4. Visual Alterations
3.3.5. Rs-fMRI as Pre-Operative Surgical Planning in Hypothalamic Hematoma Induce Epilepsy
3.3.6. Rs-fMRI Evaluations and Brain Activation
Behavioural Inhibition
Default Mode Network
3.4. Task-Based fMRI and Psychological Assessment
3.4.1. Working Memory Assessment
3.4.2. Reading Scores Evaluation
3.4.3. Working Memory
3.4.4. Tb-fMRI as Pre-Operative Surgical Planning
Language
Sensory or Motor
Visual
3.4.5. Tb-fMRI Evaluations and Brain Activation
Working Memory
Brain Activation to Language Task and Lateralisation Indices
4. Discussion
4.1. Resting-State fMRI
4.1.1. Alterations and Modifications Due to the Tumour Invasion
Visual
Language
Epilepsy
Hydrocephalus in Tumour Invasion
Sensory or Motor
4.1.2. Alterations and Modifications Due to Treatments (Surgical Technique or Radiotherapy or Chemotherapy)
Sensory or Motor
Working Memory
4.1.3. Brain Plasticity and Functional Recovery
Alterations Due to Tumour Invasion
Alterations and Modifications Due to Surgery
- Working Memory
- Alterations of Default Mode Network
4.2. Task-Based fMRI
4.2.1. Alterations Due to Tumour Invasion
Working Memory
Reading Scores
4.2.2. Alterations Due to Surgery
Post-Operative Cerebellar Mutism (PCM)
4.2.3. Alterations and Modifications in Brain Activation Associated with Tumour Invasion
Working Memory
Language
Reading Intervention
4.3. Crucial Role of Neuroplasticity and Therapy
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Idowu, O.E.; Idowu, M.A. Environmental causes of childhood brain tumours. Afr. Health Sci. 2008, 8, 1–4. [Google Scholar]
- Azizah, A.M.; Nor Saleha, I.T.; Noor Hashimah, A.; Asmah, Z.A.; Mastulu, W. Malaysian Cancer Registry Report 2007–2011; National Cancer Institute, Ministry of Health: Putrajaya, Malaysia, 2016. Available online: http://nci.moh.gov.my (accessed on 19 January 2023).
- Finch, E.; Copland, D.A. Language outcomes following neurosurgery for brain tumours: A systematic review. Neurorehabilitation 2014, 34, 499–514. [Google Scholar] [CrossRef]
- Cheng, X.; Gao, P.-Y. Abnormal Neural Activity in Children with Diffuse Intrinsic Pontine Glioma Had Manifested Deficit in Behavioral Inhibition: A Resting-State Functional MRI Study. J. Comput. Assist. Tomogr. 2019, 43, 547–552. [Google Scholar] [CrossRef]
- Margelisch, K.; Studer, M.; Ritter, B.C.; Steinlin, M.; Leibundgut, K.; Heinks, T. Cognitive dysfunction in children with brain tumors at diagnosis. Pediatr. Blood Cancer 2015, 62, 1805–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iuvone, L.; Peruzzi, L.; Colosimo, C.; Tamburrini, G.; Caldarelli, M.; Di Rocco, C.; Battaglia, D.; Guzzetta, F.; Misciagna, S.; Di Giannatale, A.; et al. Pretreatment neuropsychological deficits in children with brain tumors. Neuro-Oncol. 2011, 13, 517–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, C.; Xie, R.; Cao, X.; Bao, W.; Yang, B.; Mao, Y.; Gao, C. Intelligence Deficits in Chinese Patients with Brain Tumor: The Impact of Tumor Resection. Sci. World J. 2013, 2013, 261236. [Google Scholar] [CrossRef]
- Delion, M.; Terminassian, A.; Lehousse, T.; Aubin, G.; Malka, J.; N’Guyen, S.; Mercier, P.; Menei, P. Specificities of Awake Craniotomy and Brain Mapping in Children for Resection of Supratentorial Tumors in the Language Area. World Neurosurg. 2015, 84, 1645–1652. [Google Scholar] [CrossRef]
- Riva, D.; Taddei, M.; Ghielmetti, F.; Erbetta, A.; Bulgheroni, S. Language Cerebro-cerebellar Reorganization in Children After Surgery of Right Cerebellar Astrocytoma: A fMRI Study. Cerebellum 2019, 18, 791–806. [Google Scholar] [CrossRef]
- Loughan, A.R.; Braun, S.E.; Lanoye, A. Executive dysfunction in neuro-oncology: Behavior Rating Inventory of Executive Function in adult primary brain tumor patients. Appl. Neuropsychol. Adult 2019, 27, 393–402. [Google Scholar] [CrossRef]
- Wolfe, K.R.; Madan-Swain, A.; Hunter, G.R.; Reddy, A.T.; Baños, J.; Kana, R.K. An fMRI investigation of working memory and its relationship with cardiorespiratory fitness in pediatric posterior fossa tumor survivors who received cranial radiation therapy. Pediatr. Blood Cancer 2012, 60, 669–675. [Google Scholar] [CrossRef] [Green Version]
- Kahalley, L.S.; Douglas Ris, M.; Mahajan, A.; Fatih Okcu, M.; Chintagumpala, M.; Paulino, A.C.; Whitehead, W.E.; Minard, C.G.; Stancel, H.H.; Orobio, J.; et al. Prospective, longitudinal comparison of neurocognitive change in pediatric brain tumor patients treated with proton radiotherapy versus surgery only. Neuro-Oncol. 2019, 21, 809–818. [Google Scholar] [CrossRef] [Green Version]
- Alias, H.; Morthy, S.K.; Zakaria, S.Z.S.; Muda, Z.; Tamil, A.M. Behavioral outcome among survivors of childhood brain tumor: A case control study. BMC Pediatr. 2020, 20, 53. [Google Scholar] [CrossRef] [PubMed]
- Taphoorn, M.J.; Klein, M. Cognitive deficits in adult patients with brain tumours. Lancet Neurol. 2004, 3, 159–168. [Google Scholar] [CrossRef]
- Keilani, M.; Krall, C.; Marosi, C.; Flechl, B.; Dieckmann, K.; Widhalm, G.; Marhold, M.; Crevenna, R. Strength of skeletal muscle and self-reported physical performance in Austrian glioblastoma-patients. Wien. Klin. Wochenschr. 2012, 124, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yap, K.H.; Manan, H.A.; Yahya, N.; Azmin, S.; Mukari, S.A.M.; Ibrahim, N.M. Magnetic Resonance Imaging and Its Clinical Correlation in Spinocerebellar Ataxia Type 3: A Systematic Review. Front. Neurosci. 2022, 16, 859651. [Google Scholar] [CrossRef] [PubMed]
- Manan, H.A.; Franz, E.A.; Yahya, N. Functional connectivity changes in patients with brain tumours—A systematic review on resting state-fMRI. Neurol. Psychiatry Brain Res. 2020, 36, 73–82. [Google Scholar] [CrossRef]
- Manan, H.A.; Franz, E.A.; Yahya, N. The utilisation of resting-state fMRI as a pre-operative mapping tool in patients with brain tumours in comparison to task-based fMRI and intraoperative mapping: A systematic review. Eur. J. Cancer Care 2021, 30, e13428. [Google Scholar] [CrossRef]
- Manan, H.; Yahya, N. Ageing and Olfactory Dysfunction in Trisomy 21: A Systematic Review. Brain Sci. 2021, 11, 952. [Google Scholar] [CrossRef]
- Yahya, N.; Manan, H.A. Diffusion tensor imaging indices to predict cognitive changes following adult radiotherapy. Eur. J. Cancer Care 2020, 30, e13329. [Google Scholar] [CrossRef]
- Yahya, N.; Manan, H.A. Neurocognitive impairment following proton therapy for paediatric brain tumour: A systematic review of post-therapy assessments. Support. Care Cancer 2020, 29, 3035–3047. [Google Scholar] [CrossRef] [PubMed]
- Yap, K.H.; Manan, H.A.; Sharip, S. Heterogeneity in brain functional changes of cognitive processing in ADHD across age: A systematic review of task-based fMRI studies. Behav. Brain Res. 2020, 397, 112888. [Google Scholar] [CrossRef] [PubMed]
- Hussein, F.A.; Manan, H.A.; Mustapha, A.W.M.M.; Sidek, K.; Yahya, N. Ultrasonographic Evaluation of Skin Toxicity Following Radiotherapy of Breast Cancer: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 13439. [Google Scholar] [CrossRef]
- Manan, A.A.; Yahya, N.; Idris, Z.; Manan, H.A. The Utilization of Diffusion Tensor Imaging as an Image-Guided Tool in Brain Tumor Resection Surgery: A Systematic Review. Cancers 2022, 14, 2466. [Google Scholar] [CrossRef] [PubMed]
- Manan, H.A.; Franz, E.A.; Yahya, N. Utilization of functional MRI language paradigms for pre-operative mapping: A systematic review. Neuroradiology 2019, 62, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Manan, H.A.; Yahya, N.; Han, P.; Hummel, T. A systematic review of olfactory-related brain structural changes in patients with congenital or acquired anosmia. Brain Struct. Funct. 2021, 227, 177–202. [Google Scholar] [CrossRef]
- Voon, N.; Lau, F.; Zakaria, R.; Rani, S.M.; Ismail, F.; Manan, H.; Yahya, N. MRI-based brain structural changes following radiotherapy of Nasopharyngeal Carcinoma: A systematic review. Cancer/Radiothérapie 2021, 25, 62–71. [Google Scholar] [CrossRef]
- Yahya, N.; Chua, X.-J.; Manan, H.A.; Ismail, F. Inclusion of dosimetric data as covariates in toxicity-related radiogenomic studies: A systematic review. Strahlenther. Onkol. 2018, 194, 780–786. [Google Scholar] [CrossRef]
- Yahya, N.; Manan, H.A. Utilisation of Diffusion Tensor Imaging in Intracranial Radiotherapy and Radiosurgery Planning for White Matter Dose Optimization: A Systematic Review. World Neurosurg. 2019, 130, e188–e198. [Google Scholar] [CrossRef]
- Talabaev, M.; Venegas, K.; Zabrodets, G.; Zmachinskaya, V.; Antonenko, A.; Naumenko, D.; Salauyeva, H.; Churyla, N. Result of awake surgery for pediatric eloquent brain area tumors: Single-center experience. Child’s Nerv. Syst. 2020, 36, 2667–2673. [Google Scholar] [CrossRef]
- He, J.; Li, Z.; Yu, Y.; Lu, Z.; Li, Z.; Gong, J. Cognitive function assessment and comparison on lateral ventricular tumors resection by the frontal transcortical approach and anterior transcallosal approach respectively in children. Neurosurg. Rev. 2020, 43, 619–632. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; He, J.; Li, X.; Wang, L.; Lu, Z.; Li, C.; Gong, J. Cognitive performance change of pediatric patients after conducting frontal transcortical approach to treat lateral ventricular tumor. Child’s Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2017, 33, 2099–2108. [Google Scholar] [CrossRef] [PubMed]
- Boerwinkle, V.L.; Foldes, S.T.; Torrisi, S.J.; Temkit, H.; Gaillard, W.D.; Kerrigan, J.F.; Desai, V.R.; Raskin, J.S.; Vedantam, A.; Jarrar, R.; et al. Subcentimeter epilepsy surgery targets by resting state functional magnetic resonance imaging can improve outcomes in hypothalamic hamartoma. Epilepsia 2018, 59, 2284–2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, J.; Zhao, Y.-P.; Zhang, Y.-Q. The rs-fMRI study of effects of fornix and hippocampus-related brain function after the transcallosal interforniceal approach. Brain Res. Bull. 2019, 150, 207–215. [Google Scholar] [CrossRef]
- Anwar, A.; Radwan, A.; Zaky, I.; El Ayadi, M.; Youssef, A. Resting state fMRI brain mapping in pediatric supratentorial brain tumors. Egypt. J. Radiol. Nucl. Med. 2022, 53, 35. [Google Scholar] [CrossRef]
- Roland, J.L.; Griffin, N.; Hacker, C.D.; Vellimana, A.K.; Akbari, S.H.; Shimony, J.S.; Smyth, M.D.; Leuthardt, E.C.; Limbrick, D.D. Resting-state functional magnetic resonance imaging for surgical planning in pediatric patients: A preliminary experience. J. Neurosurg. Pediatr. 2017, 20, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Zou, P.; Conklin, H.M.; Scoggins, M.A.; Li, Y.; Li, X.; Jones, M.M.; Palmer, S.L.; Gajjar, A.; Ogg, R.J. Functional MRI in medulloblastoma survivors supports prophylactic reading intervention during tumor treatment. Brain Imaging Behav. 2015, 10, 258–271. [Google Scholar] [CrossRef] [Green Version]
- Lorenzen, A.; Groeschel, S.; Ernemann, U.; Wilke, M.; Schuhmann, M.U. Role of presurgical functional MRI and diffusion MR tractography in pediatric low-grade brain tumor surgery: A single-center study. Child’s Nerv. Syst. 2018, 34, 2241–2248. [Google Scholar] [CrossRef]
- Hoang, D.H.; Pagnier, A.; Cousin, E.; Guichardet, K.; Schiff, I.; Icher, C.; Dilharreguy, B.; Grill, J.; Frappaz, D.; Berger, C.; et al. Anatomo-functional study of the cerebellum in working memory in children treated for medulloblastoma. J. Neuroradiol. 2019, 46, 207–213. [Google Scholar] [CrossRef]
- Robinson, K.E.; Pearson, M.M.; Cannistraci, C.J.; Anderson, A.W.; Kuttesch, J.F.; Wymer, K.; Smith, S.E.; Compas, B.E. Neuroimaging of executive function in survivors of pediatric brain tumors and healthy controls. Neuropsychology 2014, 28, 791–800. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Wait, S.D.; Ogg, R.J.; Scoggins, M.A.; Zou, P.; Wheless, J.W.; Boop, F.A. Functional magnetic resonance imaging of the visual cortex performed in children under sedation to assist in presurgical planning. J. Neurosurg. Pediatr. 2013, 11, 543–546. [Google Scholar] [CrossRef] [PubMed]
- Gomez, R.; Vance, A.; Watson, S. Structure of the Wechsler Intelligence Scale for Children—Fourth Edition in a Group of Children with ADHD. Front. Psychol. 2016, 7, 737. [Google Scholar] [CrossRef] [PubMed]
- Irby, S.M.; Floyd, R.G. Test Review: Wechsler Abbreviated Scale of Intelligence, Second Edition. Can. J. Sch. Psychol. 2013, 28, 295–299. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Ruffle, T.M. The Child Behavior Checklist and Related Forms for Assessing Behavioral/Emotional Problems and Competencies. Pediatr. Rev. 2000, 21, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg-Cohen, N.; Ehrenberg, M.; Toledano, H.; Kornreich, L.; Snir, M.; Yassur, I.; Cohen, I.J.; Michowiz, S. Preoperative Visual Loss is the Main Cause of Irreversible Poor Vision in Children with a Brain Tumor. Front. Neurol. 2011, 2, 62. [Google Scholar] [CrossRef] [Green Version]
- Wan, M.J.; Zapotocky, M.; Bouffet, E.; Bartels, U.; Kulkarni, A.V.; Drake, J.M. Long-term visual outcomes of craniopharyngioma in children. J. Neuro-Oncol. 2018, 137, 645–651. [Google Scholar] [CrossRef]
- Kedar, S.; Zhang, X.; Lynn, M.J.; Newman, N.J.; Biousse, V. Pediatric Homonymous Hemianopia. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2006, 10, 249–252. [Google Scholar] [CrossRef]
- Peragallo, J.H. Visual function in children with primary brain tumors. Curr. Opin. Neurol. 2019, 32, 75–81. [Google Scholar] [CrossRef]
- Harbert, M.J.; Yeh-Nayre, L.A.; O’Halloran, H.S.; Levy, M.L.; Crawford, J.R. Unrecognized visual field deficits in children with primary central nervous system brain tumors. J. Neuro-Oncol. 2012, 107, 545–549. [Google Scholar] [CrossRef]
- Masaya-Anon, P.; Lorpattanakasem, J. Intracranial tumors affecting visual system: 5-year review in Prasat Neurological Institute. J. Med. Assoc. Thail. 2008, 91, 515. [Google Scholar]
- Mishra, A.; Shankar, S.; Ahluwalia, T.; Bhattacharjee, R. Progressive severe bilateral loss of vision in a relatively young patient: Think beyond malingering. Med. J. Armed Forces India 2016, 72 (Suppl. 1), S196–S200. [Google Scholar] [CrossRef] [Green Version]
- Sefi-Yurdakul, N. Visual findings as primary manifestations in patients with intracranial tumors. Int. J. Ophthalmol. 2015, 8, 800–803. [Google Scholar] [CrossRef]
- Peeler, C.E. A Review of Visual and Oculomotor Outcomes in Children With Posterior Fossa Tumors. Semin. Pediatr. Neurol. 2017, 24, 100–103. [Google Scholar] [CrossRef]
- Acharya, A.B.; Wroten, M. Broca Aphasia. [Updated 2022 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Pub-lishing; 2022 Jan. Available online: https://www.ncbi.nlm.nih.gov/books/NBK436010/ (accessed on 15 December 2022).
- Denslow, E.O. Damage to Wernicke’s Area: Understanding the Causes, Symptoms, & Stages of Recovery. Flint Rehab. Available online: https://www.flintrehab.com/damage-to-wernickes-area/ (accessed on 14 December 2022).
- Bello, L.; Gallucci, M.; Fava, M.; Carrabba, G.; Giussani, C.; Acerbi, F.; Baratta, P.; Songa, V.; Conte, V.; Branca, V.; et al. Intraoperative Subcortical Languagetract Mapping Guides Surgical Removalof Gliomas Involving Speech Areas. Neurosurgery 2007, 60, 67–82. [Google Scholar] [CrossRef] [PubMed]
- Ilmberger, J.; Ruge, M.; Kreth, F.-W.; Briegel, J.; Reulen, H.-J.; Tonn, J.-C. Intraoperative mapping of language functions: A longitudinal neurolinguistic analysis. J. Neurosurg. 2008, 109, 583–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desmurget, M.; Bonnetblanc, F.; Duffau, H. Contrasting acute and slow-growing lesions: A new door to brain plasticity. Brain 2006, 130 Pt 4, 898–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koekkoek, J.A.; Dirven, L.; Reijneveld, J.C.; Postma, T.J.; Grant, R.; Pace, A.; Oberndorfer, S.; Heimans, J.J.; Taphoorn, M.J. Epilepsy in the end of life phase of brain tumor patients: A systematic review. Neuro-Oncol. Pract. 2014, 1, 134–140. [Google Scholar] [CrossRef]
- Michelucci, R.; Pasini, E.; Meletti, S.; Fallica, E.; Rizzi, R.; Florindo, I.; Chiari, A.; Monetti, C.; Cremonini, A.M.; Forlivesi, S.; et al. Epilepsy in primary cerebral tumors: The characteristics of epilepsy at the onset (results from the PERNO study—Project of Emilia Romagna Region on Neuro-Oncology). Epilepsia 2013, 54, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Engel, J.; Pedley, T.A.; Aicardi, J. Epilepsy: A Comprehensive Textbook; Lippincott-Raven: New York, NY, USA, 1998; Volume 3. [Google Scholar]
- You, G.; Sha, Z.; Jiang, T. The pathogenesis of tumor-related epilepsy and its implications for clinical treatment. Seizure 2012, 21, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Fallah, A.; Weil, A.G.; Sur, S.; Miller, I.; Jayakar, P.; Morrison, G.; Bhatia, S.; Ragheb, J. Epilepsy surgery related to pediatric brain tumors: Miami Children’s Hospital experience. J. Neurosurg. Pediatr. 2015, 16, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Hennessy, M.J.; Elwes, R.D.C.; Honavar, M.; Rabe-Hesketh, S.; Binnie, C.D.; E Polkey, C. Predictors of outcome and pathological considerations in the surgical treatment of intractable epilepsy associated with temporal lobe lesions. J. Neurol. Neurosurg. Psychiatry 2001, 70, 450–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, M.; Keller, S.; Nicolson, A.; Biswas, S.; Smith, D.; Farah, J.O.; Eldridge, P.; Wieshmann, U. The long-term outcomes of epilepsy surgery. PLoS ONE 2018, 13, e0196274. [Google Scholar] [CrossRef] [Green Version]
- Bjellvi, J.; Olsson, I.; Malmgren, K.; Ramsay, K.W. Epilepsy duration and seizure outcome in epilepsy surgery: A systematic review and meta-analysis. Neurology 2019, 93, e159–e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, W.; Holland, S.K.; Shimony, J.S.; Altaye, M.; Mangano, F.T.; Limbrick, D.D.; Jones, B.V.; Nash, T.; Rajagopal, A.; Simpson, S.; et al. Abnormal structural connectivity in the brain networks of children with hydrocephalus. NeuroImage Clin. 2015, 8, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Ogata, Y.; Ozaki, A.; Ota, M.; Oka, Y.; Nishida, N.; Tabu, H.; Sato, N.; Hanakawa, T. Interhemispheric Resting-State Functional Connectivity Predicts Severity of Idiopathic Normal Pressure Hydrocephalus. Front. Neurosci. 2017, 11, 470. [Google Scholar] [CrossRef] [Green Version]
- Del Bigio, M.R.; Wilson, M.J.; Enno, T. Chronic hydrocephalus in rats and humans: White matter loss and behavior changes. Ann. Neurol. 2003, 53, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Di Curzio, D.L. Neuropathological Changes in Hydrocephalus—A Comprehensive Review. Open J. Mod. Neurosurg. 2018, 8, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Hattori, T.; Ito, K.; Aoki, S.; Yuasa, T.; Sato, R.; Ishikawa, M.; Sawaura, H.; Hori, M.; Mizusawa, H. White Matter Alteration in Idiopathic Normal Pressure Hydrocephalus: Tract-Based Spatial Statistics Study. Am. J. Neuroradiol. 2011, 33, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Fisher, M.; Recht, L.D. Brain tumor presenting as an acute pure motor hemiparesis. Stroke 1989, 20, 288–291. [Google Scholar] [CrossRef] [Green Version]
- Piscione, P.J.; Bouffet, E.; Mabbott, D.J.; Shams, I.; Kulkarni, A.V. Physical functioning in pediatric survivors of childhood posterior fossa brain tumors. Neuro-Oncol. 2013, 16, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Chaichana, K.L.; Chaichana, K.K.; Olivi, A.; Weingart, J.D.; Bennett, R.; Brem, H.; Quiñones-Hinojosa, A. Surgical outcomes for older patients with glioblastoma multiforme: Preoperative factors associated with decreased survival: Clinical article. J. Neurosurg. 2011, 114, 587–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaichana, K.L.; Martinez-Gutierrez, J.C.; De la Garza-Ramos, R.; Weingart, J.D.; Olivi, A.; Gallia, G.L.; Lim, M.; Brem, H.; Quinones-Hinojosa, A. Factors associated with survival for patients with glioblastoma with poor pre-operative functional status. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2013, 20, 818–823. [Google Scholar] [CrossRef] [Green Version]
- Amidei, C.; Kushner, D.S. Clinical implications of motor deficits related to brain tumors†. Neuro-Oncol. Pract. 2015, 2, 179–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGirt, M.J.; Mukherjee, D.; Chaichana, K.L.; Than, K.D.; Weingart, J.D.; Quinones-Hinojosa, A. Association Of Surgically Acquired Motor And Language Deficits On Overall Survival After Resection Of Glioblastoma Multiforme. Neurosurgery 2009, 65, 463–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asanuma, H.; Arissian, K. Experiments on functional role of peripheral input to motor cortex during voluntary movements in the monkey. J. Neurophysiol. 1984, 52, 212–227. [Google Scholar] [CrossRef]
- Nudo, R.J.; Friel, K.M.; Delia, S.W. Role of sensory deficits in motor impairments after injury to primary motor cortex. Neuropharmacology 2000, 39, 733–742. [Google Scholar] [CrossRef]
- Lv, Q.; Zhang, J.; Pan, Y.; Liu, X.; Miao, L.; Peng, J.; Song, L.; Zou, Y.; Chen, X. Somatosensory Deficits After Stroke: Insights From MRI Studies. Front. Neurol. 2022, 13, 891283. [Google Scholar] [CrossRef]
- Carey, L.M.; Seitz, R.J.; Parsons, M.; Levi, C.; Farquharson, S.; Tournier, J.-D.; Palmer, S.; Connelly, A. Beyond the lesion: Neuroimaging foundations for post-stroke recovery. Futur. Neurol. 2013, 8, 507–527. [Google Scholar] [CrossRef] [Green Version]
- Fraser, C.; Power, M.; Hamdy, S.; Rothwell, J.; Hobday, D.; Hollander, I.; Tyrell, P.; Hobson, A.; Williams, S.; Thompson, D. Driving Plasticity in Human Adult Motor Cortex Is Associated with Improved Motor Function after Brain Injury. Neuron 2002, 34, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Hamdy, S.; Rothwell, J.; Aziz, Q.; Singh, K.; Thompson, D.G. Long-term reorganization of human motor cortex driven by short-term sensory stimulation. Nat. Neurosci. 1998, 1, 64–68. [Google Scholar] [CrossRef]
- Hirsch, J.F.; Renier, D.; Czernichow, P.; Benveniste, L.; Pierre-Kahn, A. Medulloblastoma in childhood. Survival and functional results. Acta Neurochir. 1979, 48, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Shortman, R.I.; Lowis, S.P.; Penn, A.; McCarter, R.J.; Hunt, L.P.; Brown, C.C.; Stevens, M.; Curran, A.L.; Sharples, P.M. Cognitive function in children with brain tumors in the first year after diagnosis compared to healthy matched controls. Pediatr. Blood Cancer 2014, 61, 464–472. [Google Scholar] [CrossRef]
- Tucha, O.; Smely, C.; Preier, M.; Lange, K.W. Cognitive Deficits before Treatment among Patients with Brain Tumors. Neurosurgery 2000, 47, 324–334. [Google Scholar] [CrossRef]
- Peterson, C.C.; Johnson, C.E.; Ramirez, L.Y.; Huestis, S.; Pai, A.L.; Demaree, H.A.; Drotar, D. A meta-analysis of the neuropsychological sequelae of chemotherapy-only treatment for pediatric acute lymphoblastic leukemia. Pediatr. Blood Cancer 2008, 51, 99–104. [Google Scholar] [CrossRef]
- Duffner, P.K. Risk factors for cognitive decline in children treated for brain tumors. Eur. J. Paediatr. Neurol. 2010, 14, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Pietilä, S.; Korpela, R.; Lenko, H.L.; Haapasalo, H.; Alalantela, R.; Nieminen, P.; Koivisto, A.-M.; Mäkipernaa, A. Neurological outcome of childhood brain tumor survivors. J. Neuro-Oncol. 2012, 108, 153–161. [Google Scholar] [CrossRef]
- Postle, B. Working memory as an emergent property of the mind and brain. Neuroscience 2006, 139, 23–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Haan, E.H.F.; Corballis, P.M.; Hillyard, S.A.; Marzi, C.A.; Seth, A.; Lamme, V.A.F.; Volz, L.; Fabri, M.; Schechter, E.; Bayne, T.; et al. Split-Brain: What We Know Now and Why This is Important for Understanding Consciousness. Neuropsychol. Rev. 2020, 30, 224–233. [Google Scholar] [CrossRef]
- Castellanos, F.X. Quantitative Brain Magnetic Resonance Imaging in Attention-Deficit Hyperactivity Disorder. Arch. Gen. Psychiatry 1996, 53, 607–616. [Google Scholar] [CrossRef]
- Castellanos, F.X. Developmental Trajectories of Brain Volume Abnormalities in Children and Adolescents With Attention-Deficit/Hyperactivity Disorder. JAMA 2002, 288, 1740–1748. [Google Scholar] [CrossRef] [Green Version]
- Castellanos, F.X.; Proal, E. Large-scale brain systems in ADHD: Beyond the prefrontal–striatal model. Trends Cogn. Sci. 2012, 16, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, D.E.; Yeo, R.A.; Campbell, R.A.; Hart, B.; Vigil, J.; Brooks, W. Magnetic resonance imaging correlates of attention-deficit/hyperactivity disorder in children. Neuropsychology 2003, 17, 496–506. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.; Sergeant, J.A.; Nigg, J.; Willcutt, E. Executive Dysfunction and Delay Aversion in Attention Deficit Hyperactivity Disorder: Nosologic and Diagnostic Implications. Child Adolesc. Psychiatr. Clin. N. Am. 2008, 17, 367–384. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, D. Prefrontal Cortex and Impulsive Decision Making. Biol. Psychiatry 2011, 69, 1140–1146. [Google Scholar] [CrossRef] [Green Version]
- Funahashi, S. Neuronal mechanisms of executive control by the prefrontal cortex. Neurosci. Res. 2001, 39, 147–165. [Google Scholar] [CrossRef] [PubMed]
- Karatekin, C.; Lazareff, J.A.; Asarnow, R.F. Relevance of the cerebellar hemispheres for executive functions. Pediatr. Neurol. 2000, 22, 106–112. [Google Scholar] [CrossRef]
- Wang, P.; Yang, J.; Yin, Z.; Duan, J.; Zhang, R.; Sun, J.; Xu, Y.; Liu, L.; Chen, X.; Li, H.; et al. Amplitude of low-frequency fluctuation (ALFF) may be associated with cognitive impairment in schizophrenia: A correlation study. BMC Psychiatry 2019, 19, 30. [Google Scholar] [CrossRef] [Green Version]
- Fassbender, C.; Schweitzer, J.B. Is there evidence for neural compensation in attention deficit hyperactivity disorder? A review of the functional neuroimaging literature. Clin. Psychol. Rev. 2006, 26, 445–465. [Google Scholar] [CrossRef] [Green Version]
- Voytek, B.; Davis, M.; Yago, E.; Barceló, F.; Vogel, E.K.; Knight, R.T. Dynamic Neuroplasticity after Human Prefrontal Cortex Damage. Neuron 2010, 68, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Gusnard, D.A.; Raichle, M.E. Searching for a baseline: Functional imaging and the resting human brain. Nat. Rev. Neurosci. 2001, 2, 685–694. [Google Scholar] [CrossRef]
- Raichle, M.E.; Snyder, A.Z. A default mode of brain function: A brief history of an evolving idea. Neuroimage 2007, 37, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Esposito, R.; Mattei, P.A.; Briganti, C.; Romani, G.L.; Tartaro, A.; Caulo, M. Modifications of Default-Mode Network Connectivity in Patients with Cerebral Glioma. PLoS ONE 2012, 7, e40231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, R.J.; Bookheimer, S.; Cloughesy, T.F.; Kim, H.J.; Pope, W.; Lai, A.; Nghiemphu, P.L.; Liau, L.; Ellingson, B.M. Altered functional connectivity of the default mode network in diffuse gliomas measured with pseudo-resting state fMRI. J. Neuro-Oncol. 2014, 116, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Maniar, Y.; Peck, K.; Jenabi, M.; Gene, M.; Holodny, A. Functional MRI Shows Altered Deactivation and a Corresponding Decrease in Functional Connectivity of the Default Mode Network in Patients with Gliomas. Am. J. Neuroradiol. 2021, 42, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Boly, M.; Phillips, C.; Tshibanda, L.; Vanhaudenhuyse, A.; Schabus, M.; Dang-Vu, T.; Moonen, G.; Hustinx, R.; Maquet, P.; Laureys, S. Intrinsic Brain Activity in Altered States of Consciousness: How conscious is the default mode of brain function? Ann. N. Y. Acad. Sci. 2008, 1129, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Vanhaudenhuyse, A.; Noirhomme, Q.; Tshibanda, L.J.-F.; Bruno, M.-A.; Boveroux, P.; Schnakers, C.; Soddu, A.; Perlbarg, V.; Ledoux, D.; Brichant, J.-F.; et al. Default network connectivity reflects the level of consciousness in non-communicative brain-damaged patients. Brain 2010, 133, 161–171. [Google Scholar] [CrossRef] [Green Version]
- Dall’Acqua, P.; Johannes, S.; Mica, L.; Simmen, H.-P.; Glaab, R.; Fandino, J.; Schwendinger, M.; Meier, C.; Ulbrich, E.J.; Müller, A.; et al. Functional and Structural Network Recovery after Mild Traumatic Brain Injury: A 1-Year Longitudinal Study. Front. Hum. Neurosci. 2017, 11, 280. [Google Scholar] [CrossRef]
- Threlkeld, Z.D.; Bodien, Y.G.; Rosenthal, E.S.; Giacino, J.T.; Nieto-Castanon, A.; Wu, O.; Whitfield-Gabrieli, S.; Edlow, B.L. Functional networks reemerge during recovery of consciousness after acute severe traumatic brain injury. Cortex 2018, 106, 299–308. [Google Scholar] [CrossRef]
- Di Rocco, C.; Chieffo, D.; Pettorini, B.L.; Massimi, L.; Caldarelli, M.; Tamburrini, G. Preoperative and postoperative neurological, neuropsychological and behavioral impairment in children with posterior cranial fossa astrocytomas and medulloblastomas: The role of the tumor and the impact of the surgical treatment. Child’s Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2010, 26, 1173–1188. [Google Scholar] [CrossRef]
- Lazareff, J.A.; Castro-Sierra, E. Preoperative and postoperative analysis of visual and auditory memory in children with cerebellar tumors. Child’s Nerv. Syst. 1996, 12, 81–86. [Google Scholar] [CrossRef]
- Stargatt, R.; Rosenfeld, J.V.; Maixner, W.; Ashley, D. Multiple Factors Contribute to Neuropsychological Outcome in Children With Posterior Fossa Tumors. Dev. Neuropsychol. 2007, 32, 729–748. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.M.; Ewing-Cobbs, L.; Miner, M.E.; Levin, H.S.; Eisenberg, H.M. Behavioral changes after closed head injury in children. J. Consult. Clin. Psychol. 1990, 58, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Zou, P.; Li, Y.; Conklin, H.M.; Mulhern, R.K.; Butler, R.W.; Ogg, R.J. Evidence of Change in Brain Activity among Childhood Cancer Survivors Participating in a Cognitive Remediation Program. Arch. Clin. Neuropsychol. 2012, 27, 915–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillam, R.B.; Loeb, D.F.; Hoffman, L.M.; Bohman, T.; Champlin, C.A.; Thibodeau, L.; Widen, J.; Brandel, J.; Friel-Patti, S. The Efficacy of Fast ForWord Language Intervention in School-Age Children with Language Impairment: A Randomized Controlled Trial. J. Speech Lang. Hear. Res. JSLHR 2008, 51, 97–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loeb, D.F.; Gillam, R.B.; Hoffman, L.; Brandel, J.; Marquis, J. The Effects of Fast ForWord Language on the Phonemic Awareness and Reading Skills of School-Age Children with Language Impairments and Poor Reading Skills. Am. J. Speech-Lang. Pathol. 2009, 18, 376–387. [Google Scholar] [CrossRef]
- Wibroe, M.; Rochat, P.; Juhler, M. Cerebellar Mutism Syndrome and Other Complications After Surgery in the Posterior Fossa in Adults: A Prospective Study. World Neurosurg. 2018, 110, e738–e746. [Google Scholar] [CrossRef]
- Paquier, P.F.; Walsh, K.S.; Docking, K.M.; Hartley, H.; Kumar, R.; Catsman-Berrevoets, C.E. Post-operative cerebellar mutism syndrome: Rehabilitation issues. Child’s Nerv. Syst. 2020, 36, 1215–1222. [Google Scholar] [CrossRef] [Green Version]
- Nayak, R.; Menon, G. Rathod SCerebellar mutism following the posterior fossa tumour excision. BMJ Case Rep. CP 2020, 13, e239969. [Google Scholar]
- Wells, E.M.; Khademian, Z.P.; Walsh, K.S.; Vezina, G.; Sposto, R.; Keating, R.F.; Packer, R.J. Postoperative cerebellar mutism syndrome following treatment of medulloblastoma: Neuroradiographic features and origin. J. Neurosurg. Pediatr. 2010, 5, 329–334. [Google Scholar] [CrossRef]
- Richards, T.L.; Aylward, E.H.; Field, K.M.; Grimme, A.C.; Raskind, W.; Richards, A.L.; Nagy, W.; Eckert, M.; Leonard, C.; Abbott, R.D.; et al. Converging Evidence for Triple Word Form Theory in Children with Dyslexia. Dev. Neuropsychol. 2006, 30, 547–589. [Google Scholar] [CrossRef]
- Stoodley, C.J. The Cerebellum and Cognition: Evidence from Functional Imaging Studies. Cerebellum 2011, 11, 352–365. [Google Scholar] [CrossRef]
- Stoodley, C.J.; Schmahmann, J.D. Functional topography in the human cerebellum: A meta-analysis of neuroimaging studies. Neuroimage 2009, 44, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Hokkanen, L.S.K.; Kauranen, V.; Roine, R.O.; Salonen, O.; Kotila, M. Subtle cognitive deficits after cerebellar infarcts. Eur. J. Neurol. 2006, 13, 161–170. [Google Scholar] [CrossRef]
- Gottwald, B.; Wilde, B.; Mihajlovic, Z.; Mehdorn, H.M. Evidence for distinct cognitive deficits after focal cerebellar lesions. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1524–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botez-Marquard, T.; Bard, C.; Leveille, J.; Botez, M.I. A severe frontal-parietal lobe syndrome following cerebellar damage. Eur. J. Neurol. 2001, 8, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.B.; Stoodley, C.J.; Anslow, P.; Paul, C.; Stein, J.F.; Sugden, E.M.; Mitchell, C.D. Lateralized cognitive deficits in children following cerebellar lesions. Dev. Med. Child Neurol. 2001, 43, 685–691. [Google Scholar] [CrossRef]
- Wallesch, C.-W.; Horn, A. Long-term effects of cerebellar pathology on cognitive functions. Brain Cogn. 1990, 14, 19–25. [Google Scholar] [CrossRef]
- Owen, A.M.; McMillan, K.M.; Laird, A.R.; Bullmore, E. N-back working memory paradigm: A meta-analysis of normative functional neuroimaging studies. Hum. Brain Mapp. 2005, 25, 46–59. [Google Scholar] [CrossRef] [Green Version]
- Robinson, K.E.; Livesay, K.L.; Campbell, L.K.; Scaduto, M.; Cannistraci, C.J.; Anderson, A.W.; Whitlock, J.A.; Compas, B.E. Working memory in survivors of childhood acute lymphocytic Leukemia: Functional neuroimaging analyses. Pediatr. Blood Cancer 2009, 54, 585–590. [Google Scholar] [CrossRef] [Green Version]
- Guzzetta, A.; Pecini, C.; Biagi, L.; Tosetti, M.; Brizzolara, D.; Chilosi, A.; Cipriani, P.; Petacchi, E.; Cioni, G. Language Organisation in Left Perinatal Stroke. Neuropediatrics 2008, 39, 157–163. [Google Scholar] [CrossRef]
- Kadis, D.S.; Iida, K.; Kerr, E.N.; Logan, W.J.; Mcandrews, M.P.; Ochi, A.; Otsubo, H.; Rutka, J.T.; Iii, O.C.S.; Weiss, S.K.; et al. Intrahemispheric reorganization of language in children with medically intractable epilepsy of the left hemisphere. J. Int. Neuropsychol. Soc. 2007, 13, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Liegeois, F.; Connelly, A.; Cross, J.H.; Boyd, S.G.; Gadian, D.G.; Vargha-Khadem, F.; Baldeweg, T. Language reorganization in children with early-onset lesions of the left hemisphere: An fMRI study. Brain 2004, 127, 1229–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beharelle, A.R.; Dick, A.S.; Josse, G.; Solodkin, A.; Huttenlocher, P.R.; Levine, S.C.; Small, S. Left hemisphere regions are critical for language in the face of early left focal brain injury. Brain 2010, 133, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Lidzba, K.; Wilke, M.; Staudt, M.; Krägeloh-Mann, I.; Grodd, W. Reorganization of the cerebro-cerebellar network of language production in patients with congenital left-hemispheric brain lesions. Brain Lang. 2008, 106, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Gebauer, D.; Fink, A.; Kargl, R.; Reishofer, G.; Koschutnig, K.; Purgstaller, C.; Fazekas, F.; Enzinger, C. Differences in Brain Function and Changes with Intervention in Children with Poor Spelling and Reading Abilities. PLoS ONE 2012, 7, e38201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Shaywitz, B.; E Shaywitz, S.; A Blachman, B.; Pugh, K.R.; Fulbright, R.K.; Skudlarski, P.; Mencl, W.; Constable, R.; Holahan, J.M.; E Marchione, K.; et al. Development of left occipitotemporal systems for skilled reading in children after a phonologically- based intervention. Biol. Psychiatry 2004, 55, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Temple, E.; Deutsch, G.K.; Poldrack, R.A.; Miller, S.L.; Tallal, P.; Merzenich, M.M.; Gabrieli, J.D.E. Neural deficits in children with dyslexia ameliorated by behavioral remediation: Evidence from functional MRI. Proc. Natl. Acad. Sci. USA 2003, 100, 2860–2865. [Google Scholar] [CrossRef] [Green Version]
- Friederici, A.D. What’s in control of language? Nat. Neurosci. 2006, 9, 991–992. [Google Scholar] [CrossRef]
- Pugh, K.R.; Landi, N.; Preston, J.L.; Mencl, W.E.; Austin, A.C.; Sibley, D.; Fulbright, R.K.; Seidenberg, M.S.; Grigorenko, E.L.; Constable, R.T.; et al. The relationship between phonological and auditory processing and brain organization in beginning readers. Brain Lang. 2012, 125, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]


{kind=link}
| PICOS | Criteria |
|---|---|
| Patient | Children with brain tumours (Age < 18 years old) |
| Intervention | Resting-state and task-based functional magnetic resonance imaging |
| Comparison | Types, sizes and location of brain tumours |
| Outcome | Alteration of cognitive functions/neural network due to brain tumour invasion |
| Study | All studies related to children with brain tumours examined with functional magnetic resonance imaging |
| No | Author (Year): Country | No. of Patients (Male/Female) | Mean Age (Age Range) | Tumour Type | Tumour Location | Tumour Size | fMRI | RSNs | Eloquent Area | Assessment | Test (Cognition) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Talabaev et al. (2020): Belarus [31] | 12 (6/6) | 14.5 (8–17) | DNET, Ganglioma, PA, GBM | Supra-tentorial region | NR | Rs | NR | Visual, speech and motor cortex | Pre-operative and post-operative | Speech testing |
| 2 | He et al. (2020): China [32] | 30 (17/13) | 9.38 (6–16) | Lateral ventricular tumour | Unilateral ventricle, frontal horn, foramen of Monro, septum pellucidum | 21–49 mm | Rs | NR | Working memory | Pre-operative and post-operative | Wechsler Intelligence Scale for Children 4th version: Chinese version |
| 3 | Cheng et al. (2019): China [4] | 17 (10/7) | 7.8 (4–14) | DIPG | Brainstem | NR | Rs | NR | Behavioural inhibition | Pre-operative | Child Behaviour Checklist |
| 4 | Delion et al. (2015): France [8] | 6 (3/3) | 13.6 (11–16) | Cavernoma, ganglioma, ependymoma | Supra-tentorial region | NR | Rs | NR | Language/speech | Pre-operative and post-operative | Object denomination task |
| 5 | Zhu et al. (2017): China [33] | 15 (8/7) | 9.21 (6–14) | Lateral ventricular tumour | Frontal horn, foramen of Monro, septum pellucidum, lateral ventricle | 23–47 mm | Rs | NR | Working memory | Pre-operative and post-operative | Wechsler Intelligence Scale for Children 4th version |
| 6 | Boerwinkle et al. (2018): USA [34] | 36 (24/12) | 7.7 (1–18) | Hypothalamic hamartoma | Hypothalamus | 0.9–28.3 cm3 | Rs | NR | Epileptogenic Onset Zone | Pre-operative and post-operative | NR |
| 7 | Zhu et al. (2019): China [35] | 9 (5/4) | 11 (8–14) | Mixed germ cell tumour | Third ventricle | 3–5 cm | Rs | Default mode network | Default mode network | Pre-operative and post-operative | NR |
| 8 | Anwar et al. (2022): Egypt [36] | 22 (15/7) | 8.6 (2–18) | Ganglioglioma, DNET, GBM, ETMR, Anaplastic PXA, Anaplastic ependymoma, Meningioma, Anaplastic astrocytoma, LGG, PA, AFH | Supra-tentorial region | NR | Rs | SMN, LAN, DMN, DAN, medial visual and lateral visual network | Motor, language, visual, sensory | Pre-operative and post-operative | Paediatric NIH Stroke Scale |
| 9 | Roland et al. (2017): USA [37] | 20 (12/8) | 12.2 (2–18) | Cavernoma, right cingulate tumour | Left inferior frontal lobe | NR | Rs and Tb | SMN, LAN, DMN, Visual network | Motor, visual, language | Pre-operative and post-operative | Reading paradigm, finger tapping |
| No | Author (Year): Country | No. of Patients (Male/Female) | Mean Age (Age Range) | Tumour Type | Tumour Location | Tumour Size | Experimental Design | Task Paradigm | Eloquent Area | Assessment | Test (Cognition) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Zou et al. (2016): USA [38] | 40 (27/13) | 11.7 (Not reported) | Medulloblastoma | Cerebellum | NR | RAN, CPT, implicit reading, ORTHOPHONO, story reading | Event-related | L and R vOT, L and R STS, MTG, L and R IFG | Post-operative | Woodcock–Johnson III Battery, sound awareness, word attack, reading fluency |
| 2 | Lorenzen et al. (2018): Germany [39] | 26 (13/13) | 11.0 (3–17) | LGG, Choroid plexus papilloma | Cortical regions/sub-cortical structures | NR | Beep story, picture story, vowel identification, synonym task, finger tapping, flexion toes | Event-related | Visual, motor, language, | Pre-operative and post-operative | NR |
| 3 | Hoang et al. (2019): France [40] | 8 (6/2) | 13.1 (8–14) | Medulloblastoma | Posterior fossa (left posterior cerebellar lobe) | NR | n-back task (n-1 back and n-2 back); auditory verbal, auditory non-verbal, visual verbal, visual non-verbal | Block design | Working memory | Pre-operative and post-operative | WISC-IV (French), Trail Making Test, D’Alboy Working Memory Procedure |
| 4 | Robinson et al. (2014): USA [41] | 17 (7/10) | 12.6 (8–16) | PA, PFM, DNET, craniopharyngioma | Posterior fossa, parietal lobe, temporal lobe, pituitary gland | NR | n-back task; conditions were presented as 0-back, 1-back, 2-back, 3-back, and repeated in three cycles. | Block design and Event-related | Working memory | Post-operative | CBCL, BRIEF, WISC-IV, D-KEFS |
| 5 | Wolfe et al. (2013): USA [11] | 9 (8/1) | 14.89 (11–18) | Posterior fossa tumour | Posterior fossa | NR | n-back task; 0-back, 1-back and 2-back and counterbalanced in reverse order | Block design | Working memory | Post-operative | Weschler Abbreviated Scale of Intelligence, Lansky Score |
| 6 | Riva et al. (2019): Italy [9] | 6 (5/1) | 11 (8–17) | PA | Cerebellum | 5–53 mm | Phonemic verbal fluency task | Block design | Language | Post-operative | WISC-III |
| 7 | Li et al. (2013): USA [42] | 6 (5/1) | 6.3 (2–8) | ATRT, grade 2 astrocytoma | Visual cortex | NR | Alternating black/white screen | Block design | Visual | Pre-operative | NR |
| No | Author (Year) | Brain Region/Area Affected | Assessment of Affected Brain Region During | Behaviour and Cognitive Changes | Main Findings | |
|---|---|---|---|---|---|---|
| Pre-Operative | Post-Operative | |||||
| Resting-state fMRI | ||||||
| 1 | Talabaev et al. (2020) [31] | Precentral, postcentral, Wernicke, Broca, visual cortex | Pre-operative fMRI of eloquent brain areas depicted for surgical planning | Eloquent areas were detected during cortex stimulation. No neurological defects post-operative. | Temporary neurological deficit in 3 cases that completely regressed within a month. | ABS towards paediatric PT is quite safe with proper preliminary preparation and planning of each stage of operation. |
| 2 | He et al. (2020) [32] | Unilateral ventricle, frontal horn, foramen of Monro, septum pellucidum | WISC-IV scores < 90, prompts below average results (normal level) | All patients undergo FT and AT approach operation scored lower level in all indices of WISC-IV compared to pre-operative scores. | Functional connection between surgical injury area and bilateral cerebral hemispheres ↓ significantly but enhanced after 6 months post-surgery | AT approach impairs patients’ WM and IQ |
| 3 | Cheng et al. (2019) [4] | Brainstem | PT showed significant ↓ and ↑ in ALFF in several brain regions | NR | DIPG group with deficit in behavioural inhibition had abnormal brain activities in several brain regions served to deficit in behavioural inhibition processing | Focal spontaneous hyper- and hypofunction findings suggested that PT brain regions may need to exert extra energy to perform task of same degree as HC |
| 4 | Delion et al. (2015) [8] | L precentral sulcus, L parietal opercula, L frontopolar area, L parietal postcentral sulcus, L temporal, parietal and occipital lobes | 4th PT presented a discreet dysarthria w/o aphasia. 5th PT felt subjective word finding, no objective language disorder identified | Some PT presented with temporary deficits but improved after rehabilitation. Some deficits persisted. | Some PT had discreet abnormalities in terms of memory and language and developed facial palsy, but conditions improved after rehabilitation. | ABS is feasible in paediatric PT and allows GTR w/o major neurologic sequelae |
| 5 | Zhu et al. (2017) [33] | Unilateral ventricle, frontal horn, foramen of Monro, septum pellucidum | WISC-IV scores < 100, prompts below average results (normal level) | All PT scored lower level in all indices of WISC-IV compared to pre-operative scores | The level of co-activation and the functional connectivity significantly ↓ after surgery | There is a cognitive dysfunction in paediatric PT with lateral ventricular tumour with 1st year after FT approach |
| 6 | Boerwinkle et al. (2018) [34] | Hypothalamus (Epileptic zone) | Pre-operative fMRI of eloquent brain areas depicted for surgical planning | Percentage of total EZ volume ablated was ↑ in 83% of subjects; indicated ↑ accuracy in targeting and ablation of EZ | All PT connectivity patterns demonstrated connectivity to the areas previously reported as the primary areas of ictal propagation | Seizures (gelastic, partial and generalised) were reduced by >30% |
| 7 | Zhu et al. (2019) [35] | Third ventricle | ReHo: ↑ mainly in OL, decreased in saddle area ALFF: ↑ value in OL, FL, and cistern around brainstem fALFF: ↑ value in OL and part of FL, ↓ in FL neighbouring frontal horn of lateral ventricle | ReHo: ↑ area was mainly in the OL, ReHo around surgical pathway restored to pre-operative state ALFF: ↑ in OL, FL and cistern around brainstem, areas around surgical pathway gradually ↓ fALFF: Restored to pre-operative state | DMN: Intensity of connection between bilateral FG and other brain regions ↑ in 1-month post-surgery but restored to pre-operative state gradually. | Short-term effects of ReHo, ALFF, and fALFF in brain regions of PT can recover over time. |
| 8 | Anwar et al. (2022) [36] | Parietal, temporal, frontal, intra-ventricular, occipital, fronto-parietal | Pre-operative fMRI of eloquent brain areas depicted for surgical planning | SMN was identified in all PT, followed by DMN, and LAN. FC maps of the SMN extracted by SBA were more extensive. | 9 patients presented with signs of increased ICT but 8 resolved 3 months post-operative. 10 patients presented with neurological deficits: 1 deceased. 3 months post-operative, improvement in 6 patients, stationary course in 2 patients, 1 showed worsening scale, 1 presented a mass (Ewing Sarcoma) | Rs-fMRI is a promising tool for localising different functional brain networks in pre-operative assessments of brain areas |
| 9 | Roland et al. (2017) [37] | Left inferior frontal lobe | Pre-operative fMRI of eloquent brain areas depicted for surgical planning | 1st PT: no neurological deficits 2nd PT: full power throughout bilateral upper and lower extremities | 1st PT: speech remained fluently intact; had mild right facial weakness. 2 years post-op, remain seizure free. 2nd PT: Suffered a period of aphasia and right hemiparesis. 3 months post-op, completely recovered. | Rs-fMRI is an ideal technology for cerebral mapping in paediatric neurosurgical PT |
| Task-based fMRI | ||||||
| 10 | Zou et al. (2016) [38] | Cerebellum | NR | The activation maps of INT group resembled TD group more than the maps of SOC group during the four language tasks. | Reading scores suggested an apparent preservation of the phonological skills in INT survivors | Sustained neural and behavioural effects of prophylactic intervention in INT survivors |
| 11 | Lorenzen et al. (2018) [39] | Cortical regions (visual, motor, language) | Pre-operative fMRI of eloquent brain areas depicted for surgical planning | 90% fMRI were interpretable in terms of clearly delineating eloquent cortex | 16% PT developed permanent neurological deficits after resection (3 visual, 1 motor) | fMRI plays a profound role for pre-operative risk assessment and decision making, neurosurgical planning, and intra-operative monitoring in PT with LGG |
| 12 | Hoang et al. (2019) [40] | Cerebellum (left posterior cerebellar lobe) | PT had lower scores than HC in verbal comprehension, perceptual reasoning and processing speed | PT: no significant activation could be detected in the cerebellum for n-1 and n-2 back tasks. HC: activations related to main effects were mainly found in posterior cerebellar lobe | back: ↑ reaction times in PT for VINV back: ↓ accuracy rates in PT for VIVE, AUVE, and AUNV, ↑ reaction time for AUNV | Cerebellum plays a major role in non-verbal WM. |
| 13 | Robinson et al. (2014) [41] | Posterior fossa, parietal lobe, temporal lobe, pituitary gland | NR | PT accuracy ↓ than HC in 1-back, 3-back, and overall accuracy task | PT performed poorly on WISC-IV, D-KEFS and Trails Letter/Number Switching. PT displayed ↑ attention problems and ↓ executive function | PT performed poorly than HC on several cognitive and neurocognitive tasks. |
| 14 | Wolfe et al. (2013) [11] | Posterior fossa | NR | Significant activation in RIFG, SMA, LINS, RINS, LIPL, RIPL and RMOG | Average reaction times increase across conditions as WM load increased | Higher cardiorespiratory fitness was associated with better WM across a couple of measures |
| 15 | Riva et al. (2019) [9] | Inferior lateral hemispherical zone 1, medial hemispherical zone, inferior vermis, VII A, VIIB, VIIIA-VIIIB, superior vermis, inferior medial hemispherical zone 1, paravermian zone, superior medial hemispherical zone 1, lateral hemispherical zone 2, Crus I-Crus II | NR | Frontal and cerebellar lateralisation of PT is ↓ than HC | PT mean verbal IQ and phonemic fluency scores ↓ than HC | Functional lateralization of cerebro-cerebellar language system is globally ↓ in subjects with early right cerebellar lesion |
| 16 | Li et al. (2013) [42] | Visual cortex | Case 2: fMRI revealed right parahippocampal gyrus LGG, visual cortex was adjacent to the tumour | NR | PT visual field remained normal | Sedated fMRI in uncooperative paediatric PT using a passive visual stimulation protocol is safe and reliably predicts functional visual cortex |
| Working Memory | ||
|---|---|---|
| Authors | Neurological Deficits/Alterations | Brain Activation |
| Hoang et al. (2019) [40] | WISC-IV: PT < scored compared to HC. No significant difference between PT and HC in the phonological loop. ↑ reaction times in VINV, ↓ accuracy in VIVE, AUVE, and AUNV | No significant activation in the cerebellum for n-1 and n-2 back tasks. |
| He et al. (2020) [32] | Pre-operative: WISC-IV scores < 90 (normal) Post-operative: PT < scores in all indices of WISC-IV compared to pre-operative | Functional connection between surgical injury area and bilateral cerebral hemispheres ↓ significantly but enhanced after 6 months of follow-up |
| Robinson et al. (2014) [41] | PT < scores in WISC-IV, D-KEFS, CBCL, and BRIEF compared to HC. PT < accuracy on 0-back, 1-back, 2-back, 3-back, and overall task compared to HC. | n-back task load interactions: PT > BOLD signal in left DACC during all levels in n-back task compared to HC Between-group analyses: HC > BOLD signal in right MiFG and left MeFG |
| Zhu et al. (2017) [33] | Pre-operative: WISC-IV scores < 100 (normal) Post-operative: PT < scores in all indices of WISC-IV compared to pre-operative | ↓ level of co-activation in PFC and parietal-occipital brain regions after surgery. |
| Wolfe et al. (2013) [11] | NR | Clusters of activation are noted primarily in frontal and parietal areas |
| Language and Speech | ||
| Riva et al. (2019) [9] | Mean verbal IQ and phonemic fluency scores PT < HC | Frontal and cerebellar lateralization PT < HC |
| Lorenzen et al. (2018) [39] | One PT showed transient post-operative sequelae (conduction aphasia) | NR |
| Delion et al. (2015) [8] | 4th PT: Presented with discreet dysarthria w/o aphasia 5th PT: Mental clouding that affect language fluidity | NR |
| Talabaev et al. (2020) [31] | 2 PT developed mild disorders post-operation | NR |
| Motor or Sensory | ||
| Anwar et al. (2022) [36] | 2 PT presented with attacks of localised motor seizures w/o deficits | NR |
| Roland et al. (2017) [37] | Case 4: Mild motor dexterity deficits in left upper extremity, but demonstrates full strength in power | The SMN localised to the bilateral precentral and postcentral gyrus |
| Lorenzen et al. (2018) [39] | ¼ PT with permanent deficits involved sensorimotor | NR |
| Talabaev et al. (2020) [31] | 1 PT had mild distal hemiparesis post-operative | NR |
| Visual Network | ||
| Lorenzen et al. (2018) [39] | 3 PT presented with visual deficits post-operative | NR |
| Anwar et al. (2022) [36] | 1 PT showed partial hemianopia | NR |
| Talabaev et al. (2020) [31] | PT experienced white and black flashes | NR |
| Epilepsy | ||
| Li et al. (2013) [42] | PT presented a history of several weeks of complex partial epilepsy | Overlays demonstrated primary visual cortex activation |
| Roland et al. (2017) [37] | 1st PT: bimple partial seizure limited to right face and subsequently involving right arm and leg. 4th PT: began having seizures post-operative and persisted despite treatment with multiple AEDs | 1st PT: SMN localised in the precentral and postcentral gyrus laterally, including part of the posterior superior frontal gyrus representing SMA. 4th PT: SMN localised to bilateral precentral and postcentral gyrus. |
| Boerwinkle et al. (2018) [34] | PT presented intractable epilepsy due to HH | rs-fMRI demonstrated connectivity to the primary areas of ictal propagation |
| Behaviour | ||
| Cheng et al. (2019) [4] | PT demonstrated deficits in behavioural inhibition | ↑ and ↓ ALFF in several brain regions |
| Default Mode Network | ||
| Zhu et al. (2019) [35] | ↑ of ReHo and ALFF values in several brain regions, ↓ fALFF in several brain regions | ↑ intensity of connection between bilateral FG and other brain regions |
| Reading Intervention | ||
| Zou et al. (2016) [38] | Reading scores indicate visible preservation of phonological skills in PT | Line orientation judgement: right hemisphere Letter identification: left hemisphere language areas and sub-cortical areas |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sahrizan, N.S.A.; Manan, H.A.; Abdul Hamid, H.; Abdullah, J.M.; Yahya, N. Functional Alteration in the Brain Due to Tumour Invasion in Paediatric Patients: A Systematic Review. Cancers 2023, 15, 2168. https://doi.org/10.3390/cancers15072168
Sahrizan NSA, Manan HA, Abdul Hamid H, Abdullah JM, Yahya N. Functional Alteration in the Brain Due to Tumour Invasion in Paediatric Patients: A Systematic Review. Cancers. 2023; 15(7):2168. https://doi.org/10.3390/cancers15072168
Chicago/Turabian StyleSahrizan, Nur Shaheera Aidilla, Hanani Abdul Manan, Hamzaini Abdul Hamid, Jafri Malin Abdullah, and Noorazrul Yahya. 2023. "Functional Alteration in the Brain Due to Tumour Invasion in Paediatric Patients: A Systematic Review" Cancers 15, no. 7: 2168. https://doi.org/10.3390/cancers15072168