
Stereotactic Radiation Therapy for Brain Metastases: Factors Affecting Outcomes and Radiation Necrosis
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Population Selection and Data Collection
2.2. Simulation, Planning, and Treatment
2.3. Follow-Up
2.4. Outcome Measure
2.5. Radiation Necrosis Evaluation
2.6. Dosimetric Analysis
2.7. Statistical Analysis
3. Results
3.1. Study Population and Treatments
3.2. Survival Outcomes
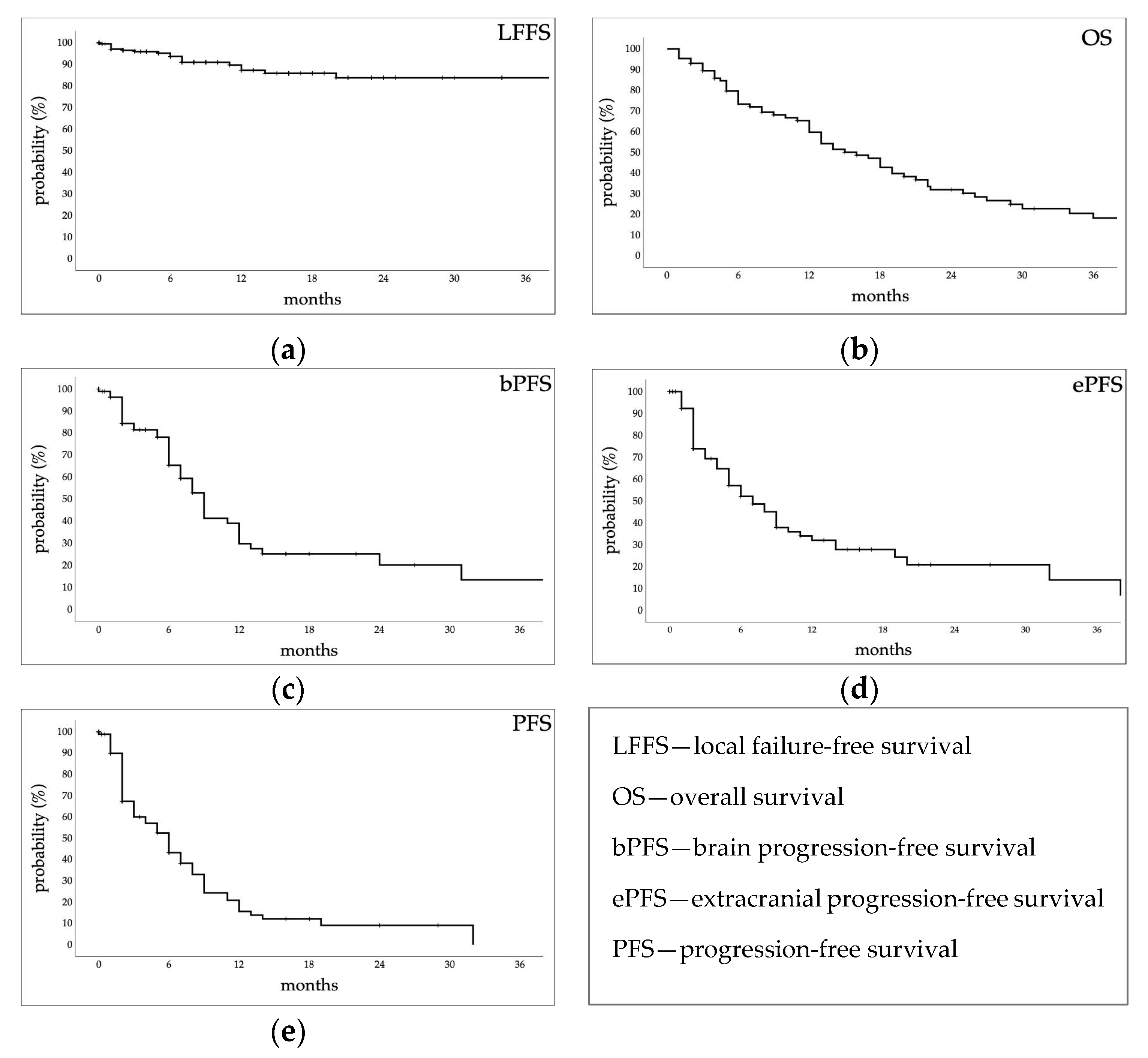
3.2.1. Estimated Survival Probabilities
3.2.2. Retreatments
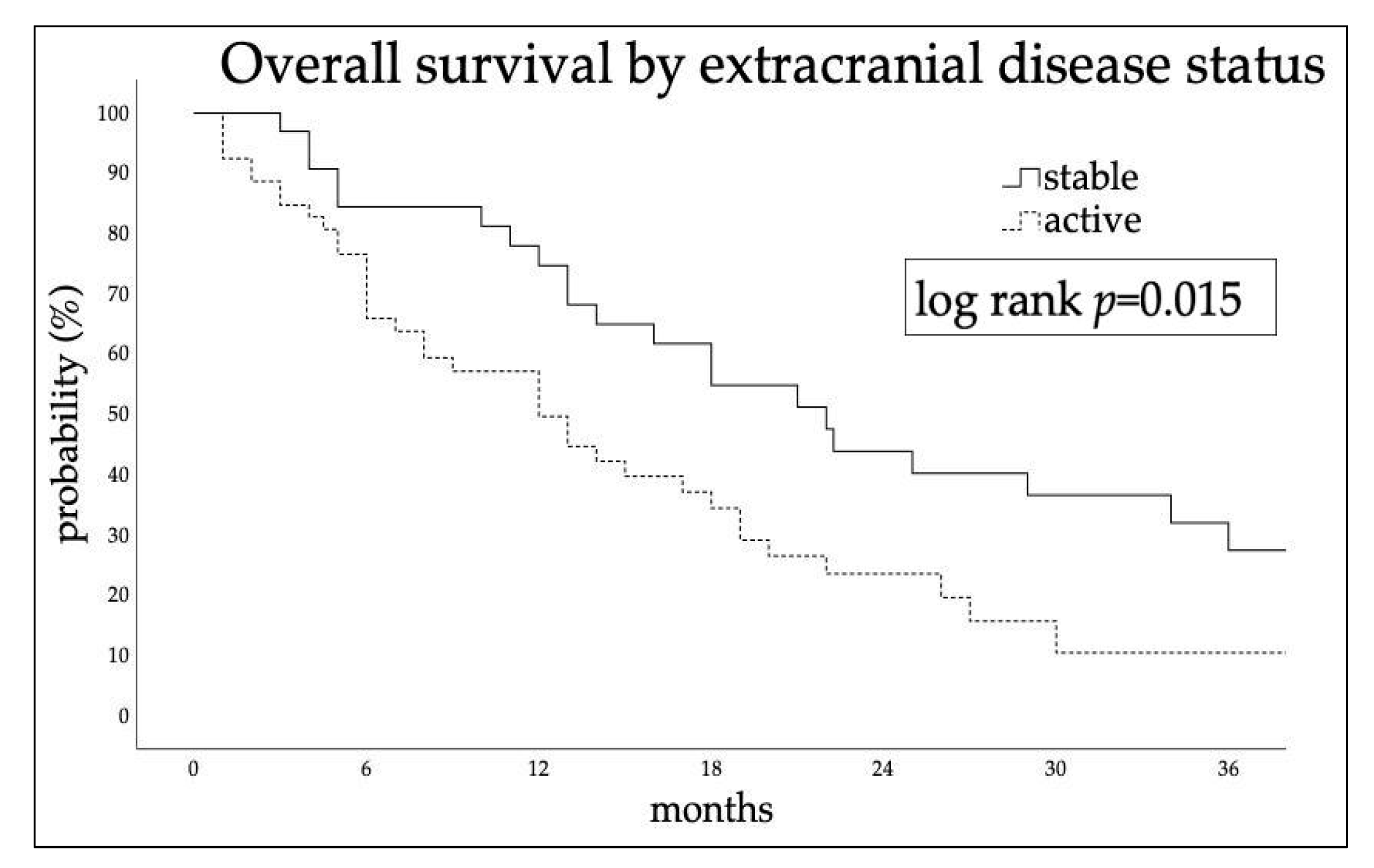
3.2.3. Factors Affecting Outcomes
3.3. Radiation Necrosis
3.3.1. Radiation Necrosis Adverse Events
3.3.2. Factors Affecting Radiation Necrosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valiente, M.; Ahluwalia, M.S.; Boire, A.; Brastianos, P.K.; Goldberg, S.B.; Lee, E.Q.; Le Rhun, E.; Preusser, M.; Winkler, F.; Soffietti, R. The Evolving Landscape of Brain Metastasis. Trends Cancer 2018, 4, 176–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Rhun, E.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO–ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up of Patients with Brain Metastasis from Solid Tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef] [PubMed]
- Venur, V.A.; Ahluwalia, M.S. Prognostic scores for brain metastasis patients: Use in clinical practice and trial design. Chin. Clin. Oncol. 2015, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Yin, Q.; Dong, Y.; Li, F.; Li, W.; Wang, X. Microsurgery vs. radiosurgery for the treatment of multiple metastases in the brain: A retrospective cohort study. Cancer Biol. Med. 2022, 19, 884–892. [Google Scholar] [CrossRef]
- Iwadate, Y.; Namba, H.; Yamaura, A. Significance of surgical resection for the treatment of multiple brain metastases. Anticancer. Res. 2000, 20, 573–577. [Google Scholar] [PubMed]
- Churilla, T.M.; Chowdhury, I.H.; Handorf, E.; Collette, L.; Collette, S.; Dong, Y.; Alexander, B.M.; Kocher, M.; Soffietti, R.; Claus, E.B.; et al. Comparison of Local Control of Brain Metastases With Stereotactic Radiosurgery vs Surgical Resection: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2019, 5, 243. [Google Scholar] [CrossRef]
- Di Rito, A.; Chaikh, A.; Troussier, I.; Darmon, I.; Thariat, J. Radiosurgery and Stereotactic Irradiation of Multiple and Contiguous Brain Metastases: A Practical Proposal of Dose Prescription Methods and a Literature Review. Cancer/Radiothérapie 2021, 25, 92–102. [Google Scholar] [CrossRef]
- Ali, M.A.; Hirshman, B.R.; Wilson, B.; Carroll, K.T.; Proudfoot, J.A.; Goetsch, S.J.; Alksne, J.F.; Ott, K.; Aiyama, H.; Nagano, O.; et al. Survival Patterns of 5750 Stereotactic Radiosurgery–Treated Patients with Brain Metastasis as a Function of the Number of Lesions. World Neurosurg. 2017, 107, 944–951.e1. [Google Scholar] [CrossRef] [Green Version]
- Brennan, C.; Yang, T.J.; Hilden, P.; Zhang, Z.; Chan, K.; Yamada, Y.; Chan, T.A.; Lymberis, S.C.; Narayana, A.; Tabar, V.; et al. A Phase 2 Trial of Stereotactic Radiosurgery Boost After Surgical Resection for Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Ruben, J.D.; Dally, M.; Bailey, M.; Smith, R.; McLean, C.A.; Fedele, P. Cerebral Radiation Necrosis: Incidence, Outcomes, and Risk Factors with Emphasis on Radiation Parameters and Chemotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 499–508. [Google Scholar] [CrossRef]
- Katsura, M.; Sato, J.; Akahane, M.; Furuta, T.; Mori, H.; Abe, O. Recognizing Radiation-Induced Changes in the Central Nervous System: Where to Look and What to Look For. RadioGraphics 2021, 41, 224–248. [Google Scholar] [CrossRef]
- Cuccurullo, V.; Di Stasio, G.D.; Cascini, G.L.; Gatta, G.; Bianco, C. The Molecular Effects of Ionizing Radiations on Brain Cells: Radiation Necrosis vs. Tumor Recurrence. Diagnostics 2019, 9, 127. [Google Scholar] [CrossRef] [Green Version]
- Balentova, S.; Adamkov, M. Molecular, Cellular and Functional Effects of Radiation-Induced Brain Injury: A Review. Int. J. Mol. Sci. 2015, 16, 27796–27815. [Google Scholar] [CrossRef] [Green Version]
- Remler, M.P.; Marcussen, W.H.; Tiller-Borsich, J. The Late Effects of Radiation on the Blood Brain Barrier. Int. J. Radiat. Oncol. Biol. Phys. 1986, 12, 1965–1969. [Google Scholar] [CrossRef]
- Nordal, R.A.; Wong, C.S. Molecular Targets in Radiation-Induced Blood-Brain Barrier Disruption. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 279–287. [Google Scholar] [CrossRef]
- Vellayappan, B.; Tan, C.L.; Yong, C.; Khor, L.K.; Koh, W.Y.; Yeo, T.T.; Detsky, J.; Lo, S.; Sahgal, A. Diagnosis and Management of Radiation Necrosis in Patients With Brain Metastases. Front. Oncol. 2018, 8, 395. [Google Scholar] [CrossRef]
- Xu, Y.; Rong, X.; Hu, W.; Huang, X.; Li, Y.; Zheng, D.; Cai, Z.; Zuo, Z.; Tang, Y. Bevacizumab Monotherapy Reduces Radiation-Induced Brain Necrosis in Nasopharyngeal Carcinoma Patients: A Randomized Controlled Trial. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1087–1095. [Google Scholar] [CrossRef]
- Yang, X.; Ren, H.; Fu, J. Treatment of Radiation-Induced Brain Necrosis. Oxid. Med. Cell. Longev. 2021, 2021, 4793517. [Google Scholar] [CrossRef]
- Jeong, W.J.; Park, J.H.; Lee, E.J.; Kim, J.H.; Kim, C.J.; Cho, Y.H. Efficacy and Safety of Fractionated Stereotactic Radiosurgery for Large Brain Metastases. J. Korean Neurosurg. Soc. 2015, 58, 217. [Google Scholar] [CrossRef]
- Pacelli, R.; Cella, L.; Conson, M.; Tranfa, F.; Strianese, D.; Liuzzi, R.; Solla, R.; Farella, A.; Salvatore, M.; Bonavolontà, G. Fractionated Stereotactic Radiation Therapy for Orbital Optic Nerve Sheath Meningioma—A Single Institution Experience and a Short Review of the Literature. JRR 2011, 52, 82–87. [Google Scholar] [CrossRef]
- Pacelli, R.; Caroprese, M.; Palma, G.; Oliviero, C.; Clemente, S.; Cella, L.; Conson, M. Technological Evolution of Radiation Treatment: Implications for Clinical Applications. Semin. Oncol. 2019, 46, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Milano, M.T.; Grimm, J.; Niemierko, A.; Soltys, S.G.; Moiseenko, V.; Redmond, K.J.; Yorke, E.; Sahgal, A.; Xue, J.; Mahadevan, A.; et al. Single- and Multifraction Stereotactic Radiosurgery Dose/Volume Tolerances of the Brain. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 68–86. [Google Scholar] [CrossRef] [PubMed]
- Redmond, K.J.; Gui, C.; Benedict, S.; Milano, M.T.; Grimm, J.; Vargo, J.A.; Soltys, S.G.; Yorke, E.; Jackson, A.; El Naqa, I.; et al. Tumor Control Probability of Radiosurgery and Fractionated Stereotactic Radiosurgery for Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Palma, G.; Monti, S.; Conson, M.; Pacelli, R.; Cella, L. Normal Tissue Complication Probability (NTCP) Models for Modern Radiation Therapy. Semin. Oncol. 2019, 46, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Loi, M.; Caini, S.; Scoccianti, S.; Bonomo, P.; De Vries, K.; Francolini, G.; Simontacchi, G.; Greto, D.; Desideri, I.; Meattini, I.; et al. Stereotactic Reirradiation for Local Failure of Brain Metastases Following Previous Radiosurgery: Systematic Review and Meta-Analysis. Crit. Rev. Oncol. Hematol. 2020, 153, 103043. [Google Scholar] [CrossRef]
- Lehrer, E.J.; Peterson, J.L.; Zaorsky, N.G.; Brown, P.D.; Sahgal, A.; Chiang, V.L.; Chao, S.T.; Sheehan, J.P.; Trifiletti, D.M. Single versus Multifraction Stereotactic Radiosurgery for Large Brain Metastases: An International Meta-Analysis of 24 Trials. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 618–630. [Google Scholar] [CrossRef]
- Kerschbaumer, J.; Demetz, M.; Krigers, A.; Nevinny-Stickel, M.; Thomé, C.; Freyschlag, C.F. Risk Factors for Radiation Necrosis in Patients Undergoing Cranial Stereotactic Radiosurgery. Cancers 2021, 13, 4736. [Google Scholar] [CrossRef]
- Valéry, C.A.; Cornu, P.; Noël, G.; Duyme, M.; Boisserie, G.; Sakka, L.J.; Mazeron, J.-J.; van Effenterre, R. Predictive Factors of Radiation Necrosis after Radiosurgery for Cerebral Metastases. Stereotact. Funct. Neurosurg. 2003, 81, 115–119. [Google Scholar] [CrossRef]
- Williams, B.J.; Suki, D.; Fox, B.D.; Pelloski, C.E.; Maldaun, M.V.C.; Sawaya, R.E.; Lang, F.F.; Rao, G. Stereotactic Radiosurgery for Metastatic Brain Tumors: A Comprehensive Review of Complications: Clinical Article. JNS 2009, 111, 439–448. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.A.; Bennett, E.E.; Xiao, R.; Kotecha, R.; Chao, S.T.; Vogelbaum, M.A.; Barnett, G.H.; Angelov, L.; Murphy, E.S.; Yu, J.S.; et al. Association Between Radiation Necrosis and Tumor Biology After Stereotactic Radiosurgery for Brain Metastasis. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 1060–1069. [Google Scholar] [CrossRef]
- Miller, J.A.; Kotecha, R.; Ahluwalia, M.S.; Mohammadi, A.M.; Suh, J.H.; Barnett, G.H.; Murphy, E.S.; Vogelbaum, M.A.; Angelov, L.; Chao, S.T. The Impact of Tumor Biology on Survival and Response to Radiation Therapy among Patients with Non–Small Cell Lung Cancer Brain Metastases. Pract. Radiat. Oncol. 2017, 7, e263–e273. [Google Scholar] [CrossRef]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic Radiosurgery for Brain Metastases: Analysis of Outcome and Risk of Brain Radionecrosis. Radiat. Oncol. 2011, 6, 48. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Hong, A.; Wang, T.; Lo, S.; Chen, B.; Silva, I.; Kapoor, R.; Hsiao, E.; Fogarty, G.B.; Carlino, M.S.; et al. Risk of Radiation Necrosis after Stereotactic Radiosurgery for Melanoma Brain Metastasis by Anatomical Location. Strahlenther. Onkol. 2021, 197, 1104–1112. [Google Scholar] [CrossRef]
- Ohtakara, K.; Hayashi, S.; Nakayama, N.; Ohe, N.; Yano, H.; Iwama, T.; Hoshi, H. Significance of Target Location Relative to the Depth from the Brain Surface and High-Dose Irradiated Volume in the Development of Brain Radionecrosis after Micromultileaf Collimator-Based Stereotactic Radiosurgery for Brain Metastases. J. Neurooncol. 2012, 108, 201–209. [Google Scholar] [CrossRef]
- Colaco, R.J.; Martin, P.; Kluger, H.M.; Yu, J.B.; Chiang, V.L. Does Immunotherapy Increase the Rate of Radiation Necrosis after Radiosurgical Treatment of Brain Metastases? JNS 2016, 125, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.M.; Cagney, D.N.; Catalano, P.J.; Alexander, B.M.; Redig, A.J.; Schoenfeld, J.D.; Aizer, A.A. Immunotherapy and Symptomatic Radiation Necrosis in Patients With Brain Metastases Treated With Stereotactic Radiation. JAMA Oncol. 2018, 4, 1123. [Google Scholar] [CrossRef]
- Tallet, A.V.; Dhermain, F.; Le Rhun, E.; Noël, G.; Kirova, Y.M. Combined Irradiation and Targeted Therapy or Immune Checkpoint Blockade in Brain Metastases: Toxicities and Efficacy. Ann. Oncol. 2017, 28, 2962–2976. [Google Scholar] [CrossRef]
- Carlson, J.A.; Nooruddin, Z.; Rusthoven, C.; Elias, A.; Borges, V.F.; Diamond, J.R.; Kavanagh, B.; Kabos, P. Trastuzumab Emtansine and Stereotactic Radiosurgery: An Unexpected Increase in Clinically Significant Brain Edema. Neuro-Oncology 2014, 16, 1006–1009. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Ren, H.; Xu, Y.; Peng, X.; Yu, W.; Shen, Z. Combination of Radiotherapy and Targeted Therapy for HER2-Positive Breast Cancer Brain Metastases. Eur. J. Med. Res. 2023, 28, 27. [Google Scholar] [CrossRef]
- Dohm, A.; McTyre, E.R.; Okoukoni, C.; Henson, A.; Cramer, C.K.; LeCompte, M.C.; Ruiz, J.; Munley, M.T.; Qasem, S.; Lo, H.-W.; et al. Staged Stereotactic Radiosurgery for Large Brain Metastases: Local Control and Clinical Outcomes of a One-Two Punch Technique. Neurosurgery 2018, 83, 114–121. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic | N/Median | %/Range |
|---|---|---|
| Sex | ||
| M | 50 | 57% |
| F | 37 | 43% |
| Age at RT (yr) | 61 | 36–86 |
| Primary | ||
| Breast | 27 | 31% |
| Lung | 21 | 24% |
| Melanoma | 9 | 10% |
| GI | 17 | 20% |
| Other | 13 | 15% |
| Stage at diagnosis | ||
| Localized or locally advanced | 59 | 68% |
| Metastatic | 28 | 32% |
| Time from diagnosis to BM (mth) | 25 | 0–221 |
| Previous brain treatment | 22 | 25% |
| WB | 19 | 22% |
| Surgery | 3 | 3% |
| Baseline KPS | 90 | 50–100 |
| ≥70 | 74 | 85% |
| <70 | 13 | 15% |
| Extracranial disease | ||
| Controlled | 34 | 39% |
| Active or new diagnosis | 53 | 61% |
| Neurological symptoms | ||
| Yes | 45 | 52% |
| No | 42 | 48% |
| Systemic therapy | 49 | 56% |
| CHT | 32 | 37% |
| Immunotherapy | 9 | 10% |
| Target therapy | 8 | 9% |
| Treatment characteristic | N°/median | %/range |
| SRT | 46 | 53% |
| 15 Gy | 13 | 15% |
| 18 Gy | 18 | 21% |
| 21 Gy | 10 | 12% |
| 24 Gy | 3 | 3% |
| Other | 2 | 2% |
| FSRT/dose fraction | 41 | 47% |
| 27/9 Gy | 16 | 18% |
| 24/8 Gy | 8 | 9% |
| 21/7 Gy | 5 | 6% |
| Other | 12 | 14% |
| Prescription dose, Gy | 31.1 | 17.4–57.6 |
| BM Characteristic | All (n = 127) N (%)/Median (Range) | Radiation Necrosis | |||
|---|---|---|---|---|---|
| G0 (n = 107) N (%)/Median (Range) | G1–G2 (n = 20) N (%)/Median (Range) | Univariate p-Value | Multivariate p-Value | ||
| Primary histotype | |||||
| Adenocarcinoma | 39 (31%) | 28 (26%) | 11 (55%) | 0.016 | 0.011 |
| SCC | 6 (5%) | 5 (5%) | 1 (5%) | 1 | - |
| Neuroendocrine | 10 (8%) | 10 (9%) | 0 (0%) | 0.361 | - |
| Urothelial | 5 (4%) | 5 (5%) | 0 (0%) | 1 | - |
| Clear cell | 2 (2%) | 2 (2%) | 0 (0%) | 1 | - |
| Melanoma | 9 (7%) | 8 (7%) | 1 (5%) | 1 | - |
| Breast | 42 (33%) | 37 (35%) | 5 (25%) | 0.451 | - |
| Sarcoma | 2 (2%) | 2 (2%) | 0 (0%) | 1 | - |
| Target volume | |||||
| PTV (cc) | 1.46 (0.02–89.4) | 1.17 (0.02–25.1) | 2.41 (0.51–89.4) | 0.002 | 0.565 |
| Site | |||||
| Supratentorial | 78 (61%) | 64 (60%) | 14 (70%) | 0.46 | - |
| Infratentorial | 49 (39%) | 43 (40%) | 6 (30%) | ||
| Deep | |||||
| Cortical | 75 (59%) | 63 (59%) | 12 (60%) | 1 | - |
| White matter | 34 (27%) | 31 (29%) | 3 (15%) | 0.274 | - |
| Deep location | 18 (14%) | 13 (12%) | 5 (25%) | 0.16 | - |
| Lobe | |||||
| Frontal | 36 (28%) | 31 (29%) | 5 (25%) | 0.794 | - |
| Occipital | 44 (35%) | 38 (36%) | 6 (30%) | 0.799 | - |
| Temporal | 21 (17%) | 17 (16%) | 4 (20%) | 0.743 | - |
| Parietal | 20 (15%) | 15 (14%) | 5 (25%) | 0.311 | - |
| Insula | 2 (2%) | 2 (2%) | 0 (0%) | 1 | - |
| Laterality | |||||
| Right | 48 (38%) | 43 (40%) | 5 (25%) | 0.221 | - |
| Left | 67 (53%) | 52 (49%) | 15 (75%) | 0.049 | 0.018 |
| Medial | 12 (9%) | 12 (11%) | 0 (0%) | 0.211 | - |
| Oncological treatment | |||||
| Immunotherapy | 32 (25%) | 25 (23%) | 7 (35%) | 0.406 | - |
| Target therapy | 7 (6%) | 5 (5%) | 2 (10%) | 0.311 | - |
| Chemotherapy | 46 (36%) | 44 (41%) | 2 (10%) | 0.006 | 0.043 |
| Previous whole brain | 23 (18%) | 21 (20%) | 2 (10%) | 0.526 | - |
| Concomitant smoke | 36 (28%) | 28 (26%) | 8 (40%) | 0.279 | - |
| Dosimetric factors | |||||
| Dmax (Gy) | 81.26 (49.5–175.97) | 80.96 (49.5–175.97) | 94.89 (79.25–168.89) | 0.046 | 0.423 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barillaro, A.; Caroprese, M.; Cella, L.; Viggiano, A.; Buccelli, F.; Daponte, C.; Feoli, C.; Oliviero, C.; Clemente, S.; Farella, A.; et al. Stereotactic Radiation Therapy for Brain Metastases: Factors Affecting Outcomes and Radiation Necrosis. Cancers 2023, 15, 2094. https://doi.org/10.3390/cancers15072094
Barillaro A, Caroprese M, Cella L, Viggiano A, Buccelli F, Daponte C, Feoli C, Oliviero C, Clemente S, Farella A, et al. Stereotactic Radiation Therapy for Brain Metastases: Factors Affecting Outcomes and Radiation Necrosis. Cancers. 2023; 15(7):2094. https://doi.org/10.3390/cancers15072094
Chicago/Turabian StyleBarillaro, Angela, Mara Caroprese, Laura Cella, Anna Viggiano, Francesca Buccelli, Chiara Daponte, Chiara Feoli, Caterina Oliviero, Stefania Clemente, Antonio Farella, and et al. 2023. "Stereotactic Radiation Therapy for Brain Metastases: Factors Affecting Outcomes and Radiation Necrosis" Cancers 15, no. 7: 2094. https://doi.org/10.3390/cancers15072094