
Evaluation of Bortezomib-BeEAM (2BeEAM) as Chemotherapy Regimen Prior to ASCT in Patients with Mantle Cell Lymphoma
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Characteristics of the Patients
3.2. Clinical Status at the Time of HDCT/ASCT
3.3. Toxicities and Adverse Events Following HDCT/ASCT
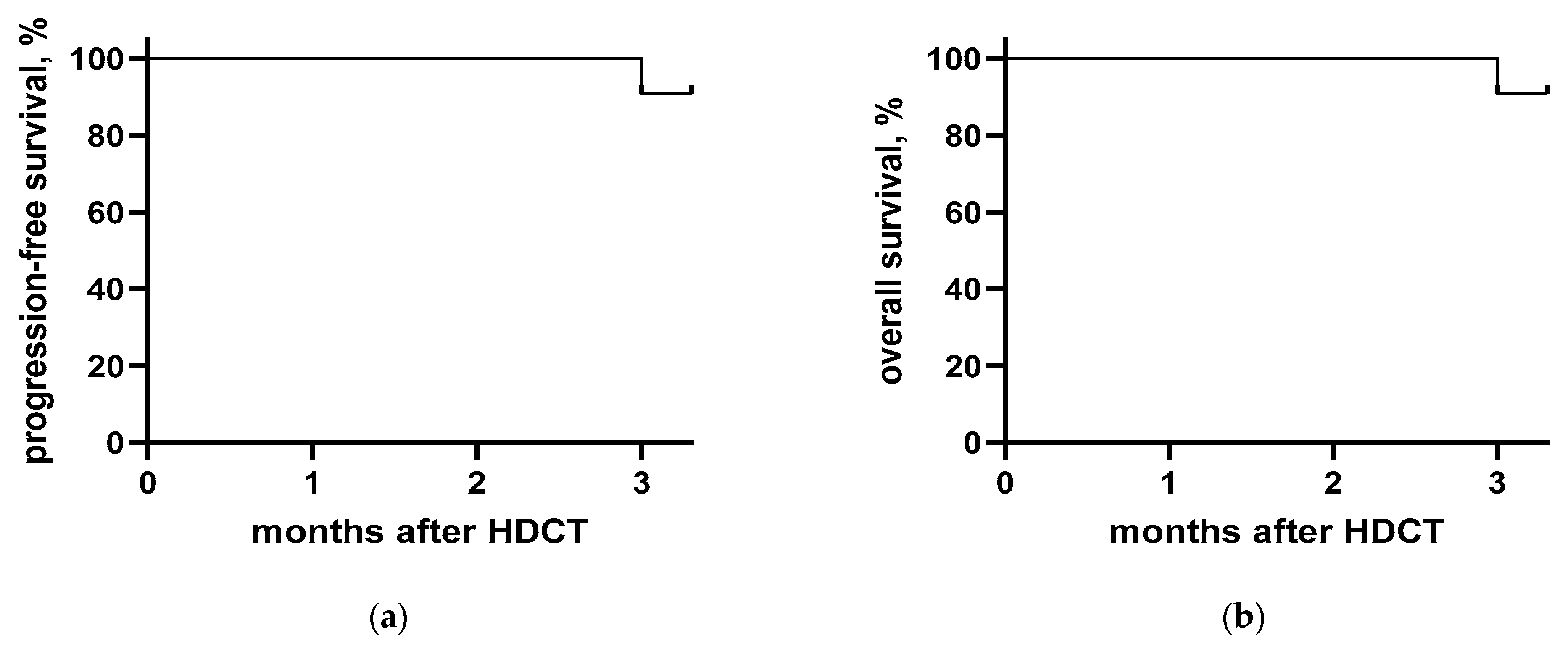
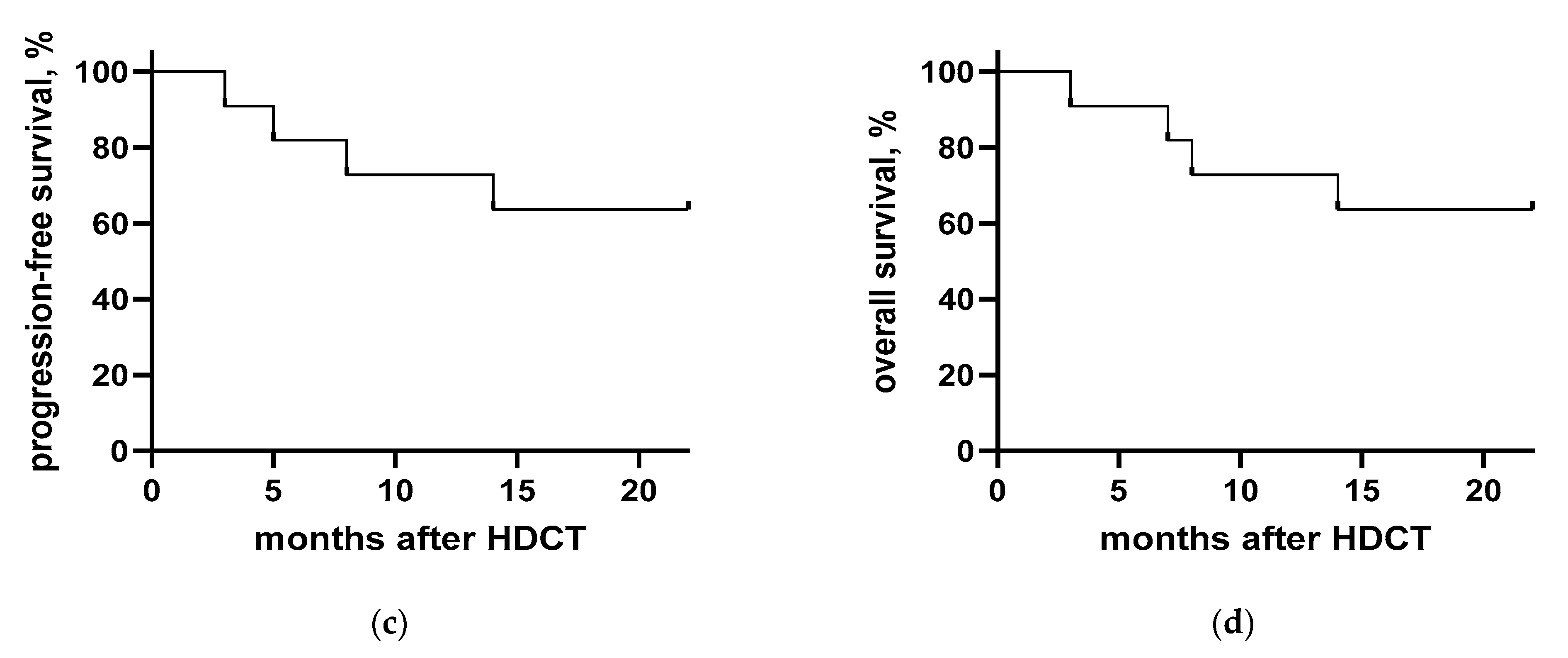
3.4. Clinical Course after HDCT/ASCT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dreyling, M.; Campo, E.; Hermine, O.; Jerkeman, M.; Le Gouill, S.; Rule, S.; Shpilberg, O.; Walewski, J.; Ladetto, M. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv62–iv71, Erratum in Am. J. Hematol. 2018, 93, E134. [Google Scholar] [CrossRef]
- Vose, J.M. Mantle cell lymphoma: 2017 update on diagnosis, risk-stratification, and clinical management. Am. J. Hematol. 2017, 92, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Ghielmini, M.; Zucca, E. How I treat mantle cell lymphoma. Blood 2009, 114, 1469–1476. [Google Scholar] [CrossRef] [Green Version]
- Hermine, O.; Hoster, E.; Walewski, J.; Ribrag, V.; Brousse, N.; Thieblemont, C.; Bouabdallah, R.; Stilgenbauer, M.S.; Feugier, P.; Forstpointner, R.; et al. Alternating Courses of 3x CHOP and 3x DHAP Plus Rituximab Followed by a High Dose ARA-C Containing Myeloablative Regimen and Autologous Stem Cell Transplantation (ASCT) Is Superior to 6 Courses CHOP Plus Rituximab Followed by Myeloablative Radiochemotherapy and ASCT In Mantle Cell Lymphoma: Results of the MCL Younger Trial of the European Mantle Cell Lymphoma Network (MCL net). Blood 2010, 116, 110. [Google Scholar] [CrossRef]
- Damon, L.E.; Johnson, J.L.; Niedzwiecki, D.; Cheson, B.D.; Hurd, D.D.; Bartlett, N.L.; LaCasce, A.S.; Blum, K.A.; Byrd, J.C.; Kelly, M.; et al. Immunochemotherapy and Autologous Stem-Cell Transplantation for Untreated Patients With Mantle-Cell Lymphoma: CALGB 59909. J. Clin. Oncol. 2009, 27, 6101–6108. [Google Scholar] [CrossRef] [Green Version]
- Mathys, A.; Bacher, U.; Banz, Y.; Legros, M.; Taleghani, B.M.; Novak, U.; Pabst, T. Outcome of patients with mantle cell lymphoma after autologous stem cell transplantation in the pre-CAR T-cell era. Hematol. Oncol. 2021, 40, 292–296. [Google Scholar] [CrossRef]
- Ribrag, V.; Saleh, K.; Danu, A.; Koscielny, S.; Pilorge, S.; Castilla-Lorente, C.; Ghez, D.; Lazarovici, J.; Michot, J.-M.; Lapierre, V.; et al. BEAM or BeEAM High-Dose Chemotherapy Followed By ASCT: A Single Center Comparative Analysis of Toxicity. Blood 2016, 128, 4648. [Google Scholar] [CrossRef]
- Hueso, T.; Gastinne, T.; Garciaz, S.; Tchernonog, E.; Delette, C.; Casasnovas, R.-O.; Durot, E.; Houot, R.; Tessoulin, B.; Tournilhac, O.; et al. Bendamustine-EAM versus BEAM regimen in patients with mantle cell lymphoma undergoing autologous stem cell transplantation in the frontline setting: A multicenter retrospective study from Lymphoma Study Association (LYSA) centers. Bone Marrow Transplant. 2020, 55, 1076–1084. [Google Scholar] [CrossRef]
- Berger, M.D.; Branger, G.; Klaeser, B.; Taleghani, B.M.; Novak, U.; Banz, Y.; Mueller, B.U.; Pabst, T. Zevalin and BEAM (Z-BEAM) versus rituximab and BEAM (R-BEAM) conditioning chemotherapy prior to autologous stem cell transplantation in patients with mantle cell lymphoma. Hematol. Oncol. 2015, 34, 133–139. [Google Scholar] [CrossRef]
- Belch, A.; Kouroukis, C.; Crump, M.; Sehn, L.; Gascoyne, R.; Klasa, R.; Powers, J.; Wright, J.; Eisenhauer, E. A phase II study of bortezomib in mantle cell lymphoma: The National Cancer Institute of Canada Clinical Trials Group trial IND.150. Ann. Oncol. 2006, 18, 116–121. [Google Scholar] [CrossRef]
- Fisher, R.I.; Bernstein, S.H.; Kahl, B.S.; Djulbegovic, B.; Robertson, M.J.; de Vos, S.; Epner, E.; Krishnan, A.; Leonard, J.P.; Lonial, S.; et al. Multicenter Phase II Study of Bortezomib in Patients With Relapsed or Refractory Mantle Cell Lymphoma. J. Clin. Oncol. 2006, 24, 4867–4874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robak, T.; Huang, H.; Jin, J.; Zhu, J.; Liu, T.; Samoilova, O.; Pylypenko, H.; Verhoef, G.; Siritanaratkul, N.; Osmanov, E.; et al. Bortezomib-Based Therapy for Newly Diagnosed Mantle-Cell Lymphoma. N. Engl. J. Med. 2015, 372, 944–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robak, T.; Jin, J.; Pylypenko, H.; Verhoef, G.; Siritanaratkul, N.; Drach, J.; Raderer, M.; Mayer, J.; Pereira, J.; Tumyan, G.; et al. Frontline bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone (VR-CAP) versus rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) in transplantation-ineligible patients with newly diagnosed mantle cell lymphoma: Final overall survival results of a randomised, open-label, phase 3 study. Lancet Oncol. 2018, 19, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.D.; Maurer, M.J.; Stock, W.; Bartlett, N.; Fulton, N.; Pettinger, A.; Byrd, J.C.; Blum, K.A.; LaCasce, A.S.; Hsi, E.D.; et al. Bortezomib consolidation or maintenance following immunochemotherapy and autologous stem cell transplantation for mantle cell lymphoma: CALGB /Alliance 50403. Am. J. Hematol. 2020, 95, 583–593. [Google Scholar] [CrossRef]
- Prediletto, I.; Farag, S.A.; Bacher, U.; Jeker, B.; Taleghani, B.M.; Brégy, R.; Zander, T.; Betticher, D.; Egger, T.; Novak, U.; et al. High incidence of reversible renal toxicity of dose-intensified bendamustine-based high-dose chemotherapy in lymphoma and myeloma patients. Bone Marrow Transplant. 2019, 54, 1923–1925. [Google Scholar] [CrossRef]
- Philip, T.; Guglielmi, C.; Hagenbeek, A.; Somers, R.; Van Der Lelie, H.; Bron, D.; Sonneveld, P.; Gisselbrecht, C.; Cahn, J.-Y.; Harousseau, J.-L.; et al. Autologous Bone Marrow Transplantation as Compared with Salvage Chemotherapy in Relapses of Chemotherapy-Sensitive Non-Hodgkin's Lymphoma. N. Engl. J. Med. 1995, 333, 1540–1545. [Google Scholar] [CrossRef]
- Kumar, A.; Sha, F.; Toure, A.; Dogan, A.; Ni, A.; Batlevi, C.L.; Palomba, M.L.M.; Portlock, C.; Straus, D.J.; Noy, A.; et al. Patterns of survival in patients with recurrent mantle cell lymphoma in the modern era: Progressive shortening in response duration and survival after each relapse. Blood Cancer J. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.D.; Branger, G.; Leibundgut, K.; Baerlocher, G.M.; Seipel, K.; Mueller, B.U.; Gregor, M.; Ruefer, A.; Pabst, T. CD34+ selected versus unselected autologous stem cell transplantation in patients with advanced-stage mantle cell and diffuse large B-cell lymphoma. Leuk. Res. 2015, 39, 561–567. [Google Scholar] [CrossRef]
- Chen, Y.-B.; Lane, A.A.; Logan, B.R.; Zhu, X.; Akpek, G.; Aljurf, M.D.; Artz, A.S.; Bredeson, C.N.; Cooke, K.R.; Ho, V.T.; et al. Impact of Conditioning Regimen on Outcomes for Patients with Lymphoma Undergoing High-Dose Therapy with Autologous Hematopoietic Cell Transplantation. Biol. Blood Marrow Transplant. 2015, 21, 1046–1053. [Google Scholar] [CrossRef] [Green Version]
- Flowers, C.R.; Costa, L.J.; Pasquini, M.C.; Le-Rademacher, J.; Lill, M.; Shore, T.B.; Vaughan, W.; Craig, M.; Freytes, C.O.; Shea, T.C.; et al. Efficacy of Pharmacokinetics-Directed Busulfan, Cyclophosphamide, and Etoposide Conditioning and Autologous Stem Cell Transplantation for Lymphoma: Comparison of a Multicenter Phase II Study and CIBMTR Outcomes. Biol. Blood Marrow Transplant. 2016, 22, 1197–1205. [Google Scholar] [CrossRef] [Green Version]
- Sellner, L.; Boumendil, A.; Finel, H.; Choquet, S.; de Rosa, G.; Falzetti, F.; Scime, R.; Kobbe, G.; Ferrara, F.; Delmer, A.; et al. Thiotepa-based high-dose therapy for autologous stem cell transplantation in lymphoma: A retrospective study from the EBMT. Bone Marrow Transplant. 2015, 51, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visani, G.; Malerba, L.; Stefani, P.M.; Capria, S.; Galieni, P.; Gaudio, F.; Specchia, G.; Meloni, G.; Gherlinzoni, F.; Giardini, C.; et al. BeEAM (bendamustine, etoposide, cytarabine, melphalan) before autologous stem cell transplantation is safe and effective for resistant/relapsed lymphoma patients. Blood 2011, 118, 3419–3425. [Google Scholar] [CrossRef] [PubMed]
- Visani, G.; Stefani, P.M.; Capria, S.; Malerba, L.; Galieni, P.; Gaudio, F.; Specchia, G.; Meloni, G.; Gherlinzoni, F.; Gonella, R.; et al. Bendamustine, etoposide, cytarabine, melphalan, and autologous stem cell rescue produce a 72% 3-year PFS in resistant lymphoma. Blood 2014, 124, 3029–3031. [Google Scholar] [CrossRef] [Green Version]
- Gilli, S.; Novak, U.; Taleghani, B.M.; Baerlocher, G.M.; Leibundgut, K.; Banz, Y.; Zander, T.; Betticher, D.; Egger, T.; Rauch, D.; et al. BeEAM conditioning with bendamustine-replacing BCNU before autologous transplantation is safe and effective in lymphoma patients. Ann. Hematol. 2016, 96, 421–429. [Google Scholar] [CrossRef]
- Furtado, M.; Johnson, R.; Kruger, A.; Turner, D.; Rule, S. Addition of bortezomib to standard dose chop chemotherapy improves response and survival in relapsed mantle cell lymphoma. Br. J. Haematol. 2014, 168, 55–62. [Google Scholar] [CrossRef] [PubMed]
- William, B.M.; Allen, M.S.; Loberiza, F.R.; Bociek, R.G.; Bierman, P.J.; Armitage, J.O.; Vose, J.M. Phase I/II Study of Bortezomib-BEAM and Autologous Hematopoietic Stem Cell Transplantation for Relapsed Indolent Non-Hodgkin Lymphoma, Transformed, or Mantle Cell Lymphoma. Biol. Blood Marrow Transplant. 2014, 20, 536–542. [Google Scholar] [CrossRef] [Green Version]
- Hoster, E.; Klapper, W.; Hermine, O.; Kluin-Nelemans, J.C.; Walewski, J.; Van Hoof, A.; Trneny, M.; Geisler, C.H.; Di Raimondo, F.; Szymczyk, M.; et al. Confirmation of the Mantle-Cell Lymphoma International Prognostic Index in Randomized Trials of the European Mantle-Cell Lymphoma Network. J. Clin. Oncol. 2014, 32, 1338–1346. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food and Drug Administration (FDA). FDA Approves First Cell-Based Gene Therapy for Adult Patients with Relapsed or Refractory MCL. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-cell-based-gene-therapy-adult-patients-relapsed-or-refractory-mcl (accessed on 24 July 2020).
- European Medicines Agency (EMA). Tecartus (Autologous Anti-CD19-Transduced CD3+ Cells): An Overview of Tecartus and Why It Is Authorized in the EU. Available online: https://www.ema.europa.eu/en/documents/overview/tecartus-epar-medicine-overview_en.pdf (accessed on 14 July 2020).
- Schweizerisches Heilmittelinstitut Swissmedic. Tecartus, Infusionsdispersion (Autologe Anti-CD19-Transduzierte CD3+ Zellen). Available online: https://www.swissmedic.ch/swissmedic/de/home/humanarzneimittel/authorisations/new-medicines/tecartus-infusiondispersion.html (accessed on 1 February 2023).
- Heini, A.D.; Bacher, U.; Kronig, M.-N.; Wiedemann, G.; Novak, U.; Zeerleder, S.; Taleghani, B.M.; Daskalakis, M.; Pabst, T. Chimeric antigen receptor T-cell therapy for relapsed mantle cell lymphoma: Real-world experience from a single tertiary care center. Bone Marrow Transplant. 2022, 57, 1010–1012. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| General Parameters | Result |
|---|---|
| Patients, number | 11 |
| Demographic characteristics | |
| Males:females (ratio) | 8:3 (2.7) |
| Median age at the time of diagnosis (years; range) | 66 (46–70) |
| Disease Parameters at Initial Diagnosis | |
| Mantle cell lymphoma | 11 (100%) |
| Ann Arbor stage | |
| I/II | 0 (0%) |
| III | 3 (27%) |
| IV | 8 (73%) |
| B-symptoms at lymphoma diagnosis 1 | 7 (64%) |
| MIPI risk category 1 | |
| Low risk | 2 (18%) |
| Intermediate/low risk | 1 (9%) |
| Intermediate risk | 2 (18%) |
| High risk | 4 (36%) |
| Morphologic grading 2 | |
| Classical type | 8 (73%) |
| Blastoid variant | 2 (18%) |
| Average Ki-67 index 1 (SD) | 36% (16.6) |
| Remission Status | Number (%) |
|---|---|
| CR | 5 (45%) |
| PR | 6 (55%) |
| Prior chemotherapy | |
| First line induction chemotherapy | 11 (100%) |
| R-CHOP/R-DHAP | 5 (45%) |
| R-CHOP/R-DHAO | 6 (55%) |
| Second line therapy | 1 (9%) |
| Median number of therapy lines (range) | 1 (1–2) |
| MIPI risk category | |
| Low risk | 1 (9%) |
| Intermediate risk | 5 (45%) |
| High risk | 5 (45%) |
| Comorbidities and ECOG status | |
| Clinically important comorbidities | 6 (55%) |
| ECOG status 1 (range) | 0 (0) |
| Hematologic recovery | |
| Median time (days) until ANC >0.5 G/l (range) | 11 (9–13) |
| Median time (days) until Tc >20 G/l (range) | 22.5 (13–97) |
| Parameter | Number (%) |
|---|---|
| Median days in hospital (range) | 27 (19–89) |
| Febrile neutropenia | 11 (100%) |
| Median febrile neutropenia CTCAE grade 1 (range) | 4 (4) |
| Anemia | 11 (100%) |
| Preexisting anemia | 11 (100%) |
| Median anemia CTCAE grade 1 (range) | 3 (2–3) |
| Thrombocytopenia | 11 (100%) |
| Median thrombocytopenia CTCAE grade 1 (range) | 4 (4) |
| Preexisting thrombocytopenia | 4 (36%) |
| New/intensified neuropathy at hospitalization | 6 (55%) |
| New/intensified peripheral sensory neuropathy | 5 (45%) |
| Median peripheral sensory neuropathy CTCAE grade (range) | 2 (1–3) |
| New/intensified peripheral motoric neuropathy | 2 (18%) |
| Median peripheral motoric neuropathy CTCAE grade (range) | 2.5 (2–3) |
| Diarrhea | 11 (100%) |
| Weight loss 1 | 10 (91%) |
| Rash | 10 (91%) |
| Xerostomy | 10 (91%) |
| Hypotension | 9 (82%) |
| Nausea | 9 (82%) |
| Mucositis | 9 (82%) |
| Decline in renal function | 7 (64%) |
| Fatigue | 7 (64%) |
| Constipation | 6 (55%) |
| Dyspnea | 6 (55%) |
| Severe infections 2 | 3 (27%) |
| Infections with detected microbial pathogen | 10 (91%) |
| Infections with detected bacterial pathogen | 10 (91%) |
| Infections with detected fungal pathogen | 6 (55%) |
| Infections with detected viral pathogen | 2 (18%) |
| Best Response Rate | Number (%) |
|---|---|
| 100-day follow-up | |
| Complete remission | 7 (64%) |
| Partial remission | 3 (27%) |
| Death between HDCT and follow-up | 1 (9%) |
| Last follow-up | |
| Complete remission | 6 (55%) |
| Partial remission | 1 (9%) |
| Relapse following HDCT/ASCT | 1 (9%) |
| Death after partial remission | 2 (18%) |
| Death after relapse after 100-day follow-up | 1 (9%) |
| Patients with further MCL therapy after HDCT/ASCT | 9 (82%) |
| Overall mortality | 4 (36%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huwyler, F.; Kunz, R.; Bacher, U.; Hoffmann, M.; Novak, U.; Daskalakis, M.; Banz, Y.; Pabst, T. Evaluation of Bortezomib-BeEAM (2BeEAM) as Chemotherapy Regimen Prior to ASCT in Patients with Mantle Cell Lymphoma. Cancers 2023, 15, 2091. https://doi.org/10.3390/cancers15072091
Huwyler F, Kunz R, Bacher U, Hoffmann M, Novak U, Daskalakis M, Banz Y, Pabst T. Evaluation of Bortezomib-BeEAM (2BeEAM) as Chemotherapy Regimen Prior to ASCT in Patients with Mantle Cell Lymphoma. Cancers. 2023; 15(7):2091. https://doi.org/10.3390/cancers15072091
Chicago/Turabian StyleHuwyler, Fabrizio, Rebekka Kunz, Ulrike Bacher, Michèle Hoffmann, Urban Novak, Michael Daskalakis, Yara Banz, and Thomas Pabst. 2023. "Evaluation of Bortezomib-BeEAM (2BeEAM) as Chemotherapy Regimen Prior to ASCT in Patients with Mantle Cell Lymphoma" Cancers 15, no. 7: 2091. https://doi.org/10.3390/cancers15072091