
Progression-Free and Overall Survival of First-Line Treatments for Advanced Renal Cell Carcinoma: Indirect Comparison of Six Combination Regimens

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
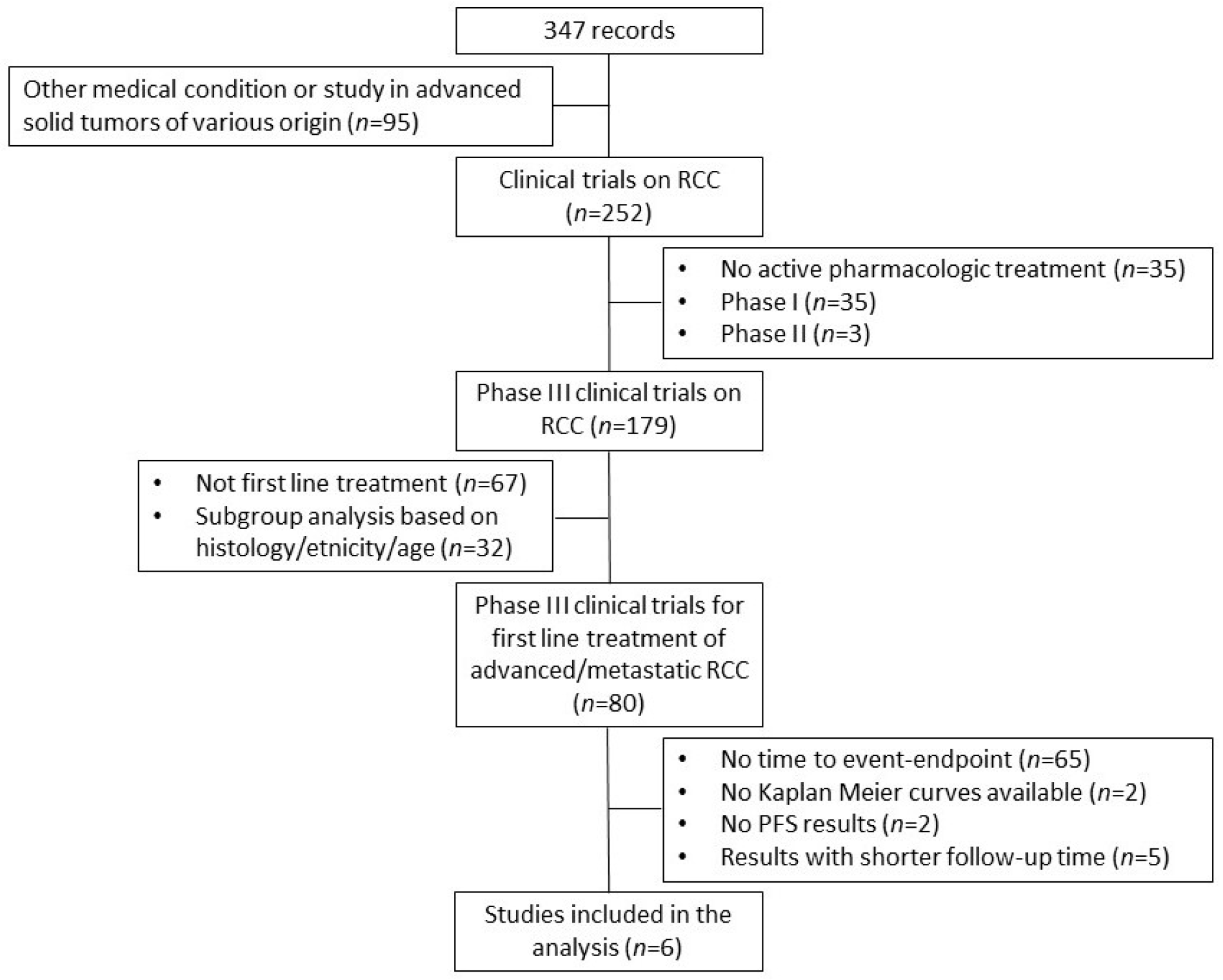
2.1. Literature Search
2.2. Reconstruction of Individual Patient Data
2.3. Statistical Analysis
3. Results
3.1. Included Trials and Application of the Shiny Method
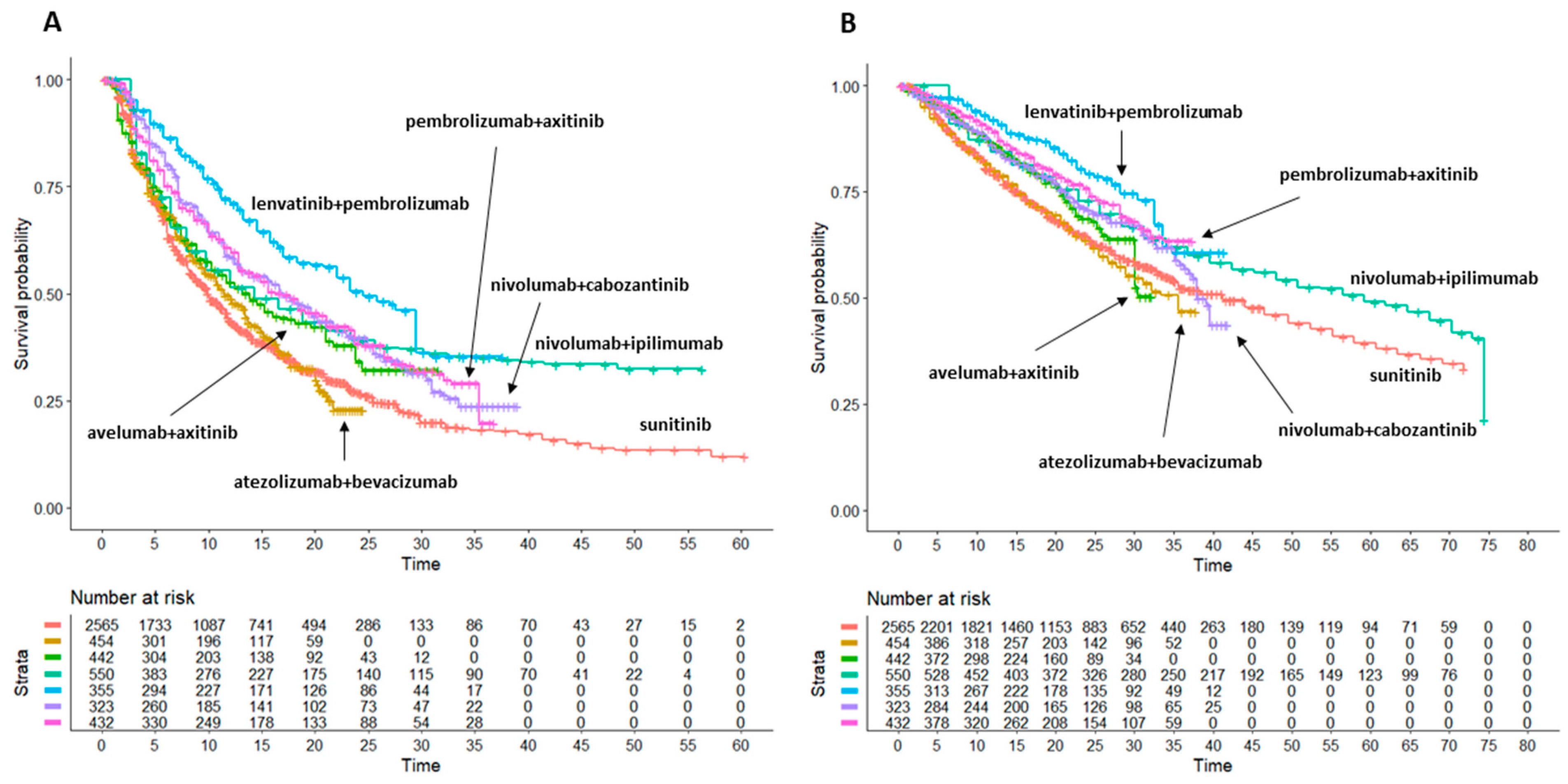
3.2. Progression-Free Survival: Indirect Comparisons of the Six Combination Treatments Plus Sunitinib with One Another
- pembrolizumab + lenvatinib: median PFS 24.52 months (95%CI 22.02 to 29.5); this combination treatment is significantly better than all other combination treatments, in particular of nivolumab + cabozantinib, which ranks second, with HR = 0.714 (95%CI 0.574 to 0.889);
- nivolumab + cabozantinib: median PFS 17.12 months (13.01 to 20.2);
- pembrolizumab + axitinib: median PFS 16.99 months (14.21 to 21.1);
- nivolumab + ipilimumab: median PFS 14.29 months (12.02 to 18.8); these three combinations produced similar gains of survival with respect to sunitinib (see Supplementary Table S1), with no difference in the head-to-head comparisons; in contrast, they were significantly superior to atezolizumab + bevacizumab and numerically superior to avelumab + axitinib;
- avelumab + axitinib: median PFS 13.85 months (95%CI 10.99 to 16.7) was inferior to all other combinations except atezolizumab + bevacizumab (HR = 0.817, 95%CI 0.678 to 0.985);
- atezolizumab + bevacizumab: median PFS 11.45 months (95%CI 9.87 to 13.5) was significantly inferior to all other treatments, and it does not produce any significant gain of function compared to sunitinib (HR = 0.9822, 95%CI 0.8637 to 1.117).
- sunitinib (6 control arms pooled together): median PFS 9.92 months (95%CI 9.53 to 10.09) was inferior to 5 out of six combination treatments, with the exception of atezolizumab + bevacizumab.
3.3. Overall Survival: Indirect Comparisons of the 6 Combination Treatments Plus Sunitinib with One Another
- pembrolizumab + lenvatinib: median OS not reached, but this treatment is expected to rank first based on the HR analysis vs. sunitinib (HR = 0.57, 95%CI 0.45 to 0.72); in the head-to head comparison, pembrolizumab + lenvatinib was numerically superior to both pembrolizumab + axitinib (HR = 0.868, 95%CI 0.634 to 1.189) and nivolumab + ipilimumab (HR = 0.781, 95%CI 0.592 to 1.031) but significantly better than other combinations.
- pembrolizumab + axitinib: median OS not reached, but this treatment is expected to rank second based on the HR analysis vs. sunitinib (HR = 0.6601, 95%CI 0.5369 to 0.8116); in the head-to head comparison, pembrolizumab + axitinib was numerically superior to nivolumab + ipilimumab, nivolumab + cabozantinib and avelumab + axitinib and significantly superior to atezolizumab + bevacizumab;
- nivolumab + ipilimumab: median OS 59.2 months (48 to 70.3). This treatment was numerically superior to nivolumab + cabozantinib and avelumab + axitinib;
- nivolumab + cabozantinib: median OS 37.9 months (95%CI 36.3 to NA). This combination failed to demonstrate any significant advantage compared to other treatments but it was numerically superior to atezolizumab + bevacizumab and almost similar to avelumab + axitinib;
- avelumab + axitinib: median OS not reached. This treatment was numerically superior only to atezolizumab + bevacizumab and sunitinib monotherapy;
- sunitinib (6 control arms pooled together): median OS 41.2 months (95%CI 35.6 to 46.5) was inferior to 5 out of six combination treatments, with the exception of atezolizumab + bevacizumab;
- atezolizumab + bevacizumab: median OS 35.5 months (95%CI 28.9 to NA). This treatment was significantly worse than most of the comparators, including sunitinib monotherapy. The HR analysis vs. sunitinib failed to demonstrate a significant gain in survival (HR = 1.0818, 95%CI 0.9148 to 1.2794).
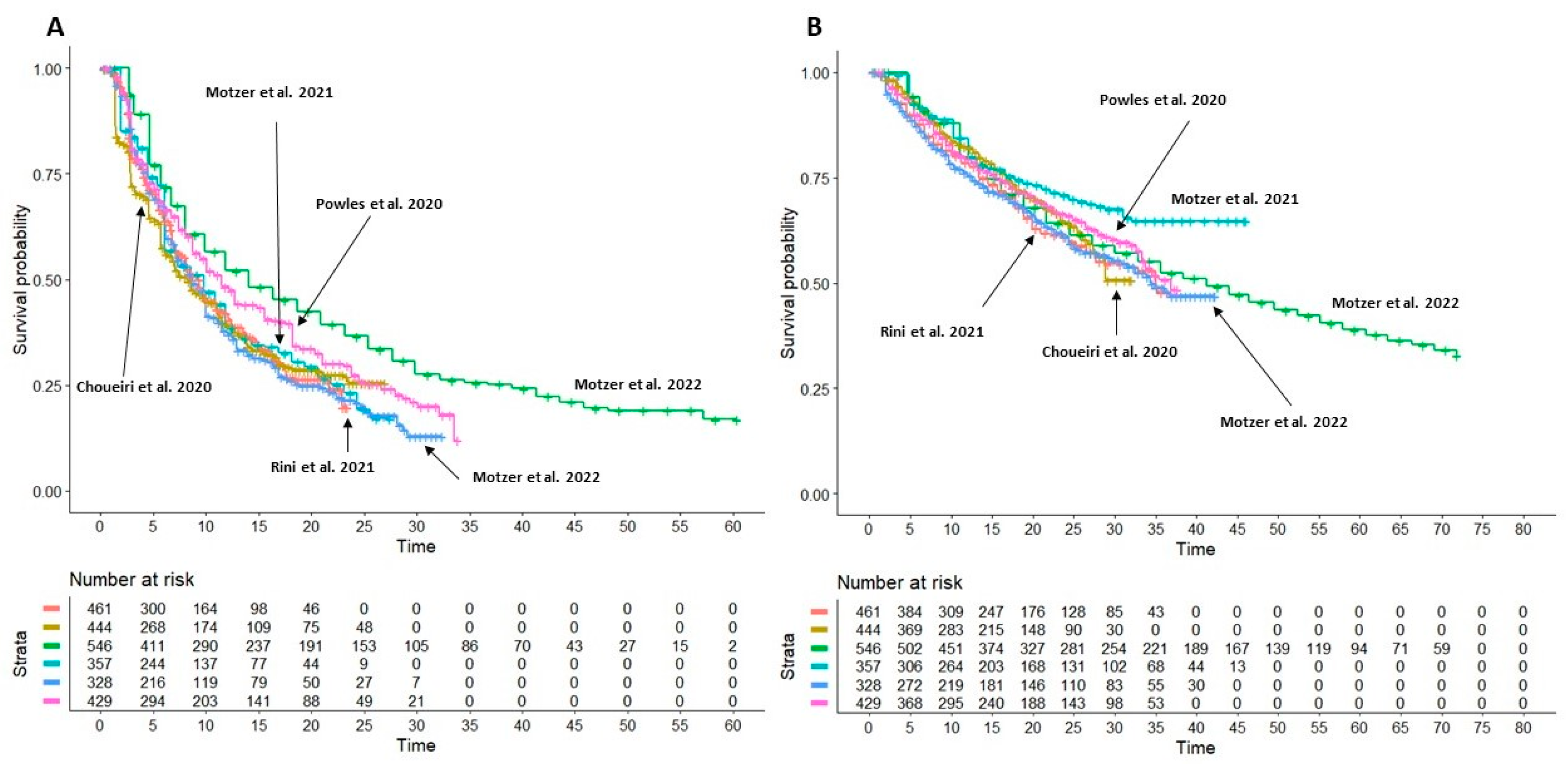
3.4. Heterogeneity Analysis on Sunitinib Monotherapy Curves
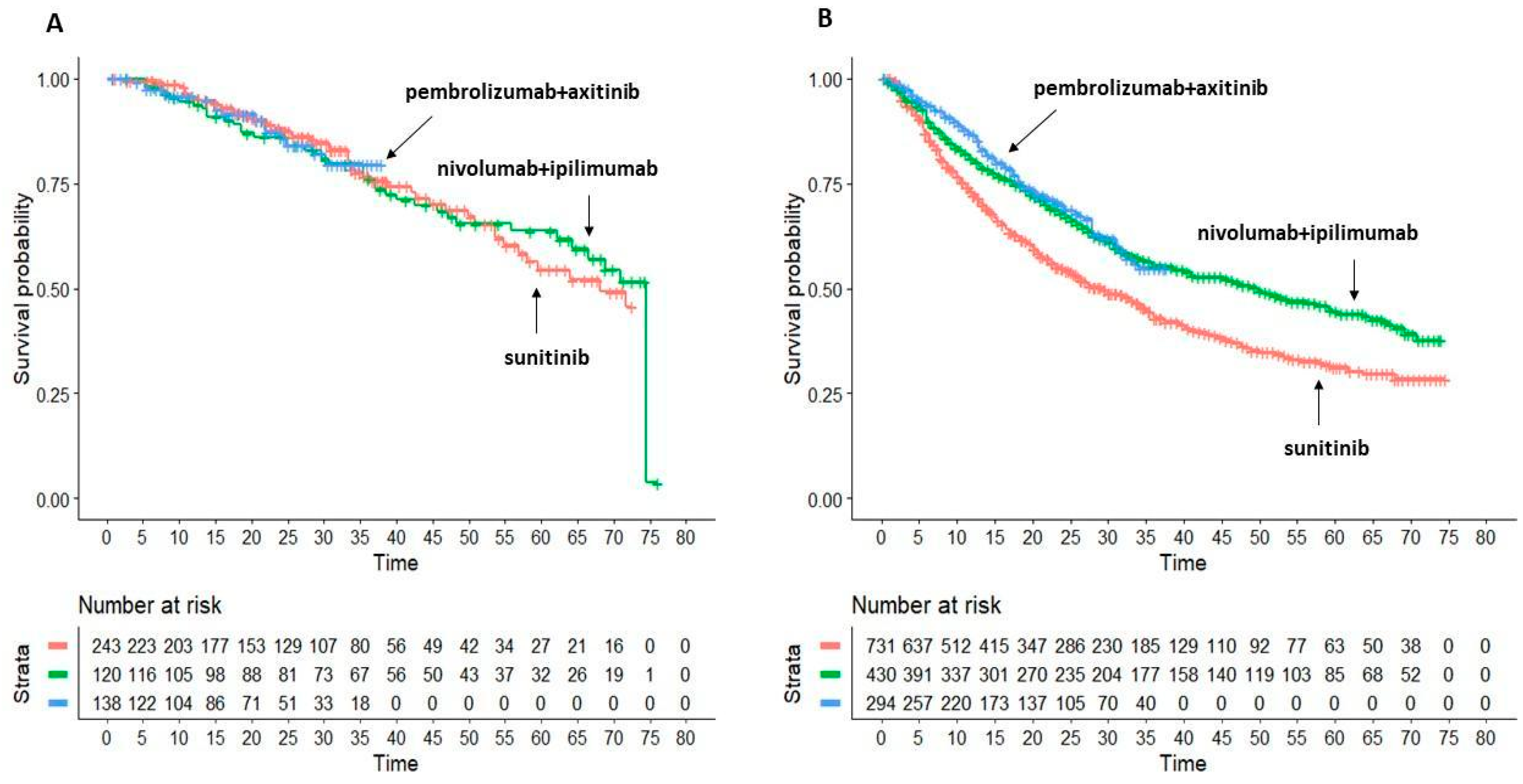
3.5. Subgroup Analysis: Overall Survival in Favourable vs. Intermediate/Poor Risk Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guillaume, Z.; Auvray, M.; Vano, Y.; Oudard, S.; Helley, D.; Mauge, L. Renal Carcinoma and Angiogenesis: Therapeutic Target and Biomarkers of Response in Current Therapies. Cancers 2022, 14, 6167. [Google Scholar] [CrossRef] [PubMed]
- Dutcher, J.P.; Flippot, R.; Fallah, J.; Escudier, B. On the Shoulders of Giants: The Evolution of Renal Cell Carcinoma Treatment-Cytokines, Targeted Therapy, and Immunotherapy. Am. Soc. Clin. Oncol. Educ. Book Am. Soc. Clin. Oncol. Annu. Meet. 2020, 40, 418–435. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The Blockade of Immune Checkpoints in Cancer Immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Grünwald, V.; Bergmann, L.; Brehmer, B.; Eberhardt, B.; Kastrati, K.; Gauler, T.; Gehbauer, G.; Gschwend, J.; Johannsen, M.; Klotz, T.; et al. Systemic Therapy in Metastatic Renal Cell Carcinoma (MRCC): An Evidence-Based Recommendation of the German Interdisciplinary RCC Guidelines Group. World J. Urol. 2022, 40, 2381–2386. [Google Scholar] [CrossRef]
- Bedke, J.; Albiges, L.; Capitanio, U.; Giles, R.H.; Hora, M.; Lam, T.B.; Ljungberg, B.; Marconi, L.; Klatte, T.; Volpe, A.; et al. The 2021 Updated European Association of Urology Guidelines on Renal Cell Carcinoma: Immune Checkpoint Inhibitor-Based Combination Therapies for Treatment-Naive Metastatic Clear-Cell Renal Cell Carcinoma Are Standard of Care. Eur. Urol. 2021, 80, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhou, Y.; Lee, J.J. IPDfromKM: Reconstruct Individual Patient Data from Published Kaplan-Meier Survival Curves. BMC Med. Res. Methodol. 2021, 21, 111. [Google Scholar] [CrossRef]
- Messori, A. Synthetizing Published Evidence on Survival by Reconstruction of Patient-Level Data and Generation of a Multi-Trial Kaplan-Meier Curve. Cureus 2021, 13, e19422. [Google Scholar] [CrossRef]
- Damuzzo, V.; Rivano, M.; Baldo, P.; Cancanelli, L.; Di Spazio, L.; Ossato, A.; Chiumente, M.; Messori, A.; Mengato, D. Application of artificial intelligence for an early comparison of efficacy between new cancer drugs. Recent. Prog. Med. 2022, 113, 680–687. [Google Scholar] [CrossRef]
- Messori, A.; Damuzzo, V.; Rivano, M.; Cancanelli, L.; Di Spazio, L.; Ossato, A.; Chiumente, M.; Mengato, D. Application of the IPDfromKM-Shiny Method to Compare the Efficacy of Novel Treatments Aimed at the Same Disease Condition: A Report of 14 Analyses. Cancers 2023, 15, 1633. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Rini, B.I.; Powles, T.; Atkins, M.B.; Escudier, B.; McDermott, D.F.; Suarez, C.; Bracarda, S.; Stadler, W.M.; Donskov, F.; Lee, J.L.; et al. Atezolizumab plus Bevacizumab versus Sunitinib in Patients with Previously Untreated Metastatic Renal Cell Carcinoma (IMmotion151): A Multicentre, Open-Label, Phase 3, Randomised Controlled Trial. Lancet 2019, 393, 2404–2415. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Motzer, R.J.; Rini, B.I.; Haanen, J.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Gravis-Mescam, G.; Uemura, M.; Lee, J.L.; et al. Updated Efficacy Results from the JAVELIN Renal 101 Trial: First-Line Avelumab plus Axitinib versus Sunitinib in Patients with Advanced Renal Cell Carcinoma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; McDermott, D.F.; Escudier, B.; Burotto, M.; Choueiri, T.K.; Hammers, H.J.; Barthélémy, P.; Plimack, E.R.; Porta, C.; George, S.; et al. Conditional Survival and Long-Term Efficacy with Nivolumab plus Ipilimumab versus Sunitinib in Patients with Advanced Renal Cell Carcinoma. Cancer 2022, 128, 2085–2097. [Google Scholar] [CrossRef]
- Motzer, R.; Alekseev, B.; Rha, S.-Y.; Porta, C.; Eto, M.; Powles, T.; Grünwald, V.; Hutson, T.E.; Kopyltsov, E.; Méndez-Vidal, M.J.; et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N. Engl. J. Med. 2021, 384, 1289–1300. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Shah, A.Y.; Suárez, C.; Hamzaj, A.; Porta, C.; Hocking, C.M.; et al. Nivolumab plus Cabozantinib versus Sunitinib in First-Line Treatment for Advanced Renal Cell Carcinoma (CheckMate 9ER): Long-Term Follow-up Results from an Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2022, 23, 888–898. [Google Scholar] [CrossRef]
- Powles, T.; Plimack, E.R.; Soulières, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I.; et al. Pembrolizumab plus Axitinib versus Sunitinib Monotherapy as First-Line Treatment of Advanced Renal Cell Carcinoma (KEYNOTE-426): Extended Follow-up from a Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef]
- Bosma, N.A.; Warkentin, M.T.; Gan, C.L.; Karim, S.; Heng, D.Y.C.; Brenner, D.R.; Lee-Ying, R.M. Efficacy and Safety of First-Line Systemic Therapy for Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-Analysis. Eur. Urol. Open Sci. 2022, 37, 14–26. [Google Scholar] [CrossRef]
- Santoni, M.; Rizzo, A.; Mollica, V.; Rosellini, M.; Marchetti, A.; Fragomeno, B.; Battelli, N.; Massari, F. Pembrolizumab plus Lenvatinib or Axitinib Compared to Nivolumab plus Ipilimumab or Cabozantinib in Advanced Renal Cell Carcinoma: A Number Needed to Treat Analysis. Expert Rev. Pharmacoecon. Outcomes Res. 2022, 22, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Quhal, F.; Mori, K.; Bruchbacher, A.; Resch, I.; Mostafaei, H.; Pradere, B.; Schuettfort, V.M.; Laukhtina, E.; Egawa, S.; Fajkovic, H.; et al. First-Line Immunotherapy-Based Combinations for Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-Analysis. Eur. Urol. Oncol. 2021, 4, 755–765. [Google Scholar] [CrossRef]
- Dimagli, A.; Cancelli, G.; Soletti, G.J.; Perezgrovas, O.R.; Chadow, D.; Rahouma, M.; Girardi, L.; Gaudino, M. Percutaneous coronary intervention versus repeat surgical revascularization in patients with prior coronary artery bypass grafting: A systematic review and meta-analysis. JTCVS Open 2022, 12, 177–191. [Google Scholar] [CrossRef]
- Leung, Y.Y.R.; Bera, K.; Urriza, R.D.; Dardik, A.; Mas, J.L.; Simonte, G.; Rerkasem, K.; Howard, D.P.J. Safety of Carotid Endarterectomy for Symptomatic Stenosis by Age: Meta-Analysis with Individual Patient Data. Stroke 2023, 54, 457–467. [Google Scholar] [CrossRef]
- Magouliotis, D.E.; Zotos, P.A.; Karamolegkou, A.P.; Tatsios, E.; Spiliopoulos, K.; Athanasiou, T. Long-Term Survival after Extended Sleeve Lobectomy (ESL) for Central Non-Small Cell Lung Cancer (NSCLC): A Meta-Analysis with Reconstructed Time-to-Event Data. J. Clin. Med. 2022, 12, 204. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with COVID-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef] [PubMed]
- Yap, D.W.T.; Leone, A.G.; Wong, N.Z.H.; Zhao, J.J.; Tey, J.C.S.; Sundar, R.; Pietrantonio, F. Effectiveness of Immune Checkpoint Inhibitors in Patients with Advanced Esophageal Squamous Cell Carcinoma: A Meta-analysis Including Low PD-L1 Subgroups. JAMA Oncol. 2023, 9, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.Y.; Zhao, J.J.; Sultana, R.; Lee, J.J.X.; Lee, S.Y.; Chan, S.L.; Yau, T.; Tai, D.W.M.; Sundar, R.; Too, C.W. First-Line Systemic Therapies for Advanced Hepatocellular Carcinoma: A Systematic Review and Patient-Level Network Meta-Analysis. Liver Cancer 2022, 12, 7–18. [Google Scholar] [CrossRef]
- Schmidt, A.L.; Tabakin, A.L.; Singer, E.A.; Choueiri, T.K.; McKay, R.R. Next Steps: Sequencing Therapies in Metastatic Kidney Cancer in the Contemporary Era. Am. Soc. Clin. Oncol. Educ. Book Am. Soc. Clin. Oncol. Annu. Meet. 2021, 41, 187–197. [Google Scholar] [CrossRef]
- Quhal, F.; Mori, K.; Remzi, M.; Fajkovic, H.; Shariat, S.F.; Schmidinger, M. Adverse Events of Systemic Immune-Based Combination Therapies in the First-Line Treatment of Patients with Metastatic Renal Cell Carcinoma: Systematic Review and Network Meta-Analysis. Curr. Opin. Urol. 2021, 31, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.; Porta, C.; Alekseev, B.; Rha, S.Y.; Choueiri, T.K.; Mendez-Vidal, M.J.; Hong, S.-H.; Kapoor, A.; Goh, J.C.; Eto, M.; et al. Health-Related Quality-of-Life Outcomes in Patients with Advanced Renal Cell Carcinoma Treated with Lenvatinib plus Pembrolizumab or Everolimus versus Sunitinib (CLEAR): A Randomised, Phase 3 Study. Lancet Oncol. 2022, 23, 768–780. [Google Scholar] [CrossRef]
- Zarrabi, K.K.; Handorf, E.; Miron, B.; Zibelman, M.R.; Anari, F.; Ghatalia, P.; Plimack, E.R.; Geynisman, D.M. Comparative Effectiveness of Front-Line Ipilimumab and Nivolumab or Axitinib and Pembrolizumab in Metastatic Clear Cell Renal Cell Carcinoma. Oncologist 2023, 28, 157–164. [Google Scholar] [CrossRef]
- Messori, A.; Rivano, M.; Cancanelli, L.; Damuzzo, V.; Ossato, A.; Chiumente, M.; Mengato, D. The “One-to-Many” Survival Analysis to Evaluate a New Treatment in Comparison with Therapeutic Alternatives Based on Reconstructed Patient Data: Enfortumab Vedotin Versus Standard of Care in Advanced or Metastatic Urothelial Carcinoma. Cureus 2022, 14, e28369. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PFS | OS | ||||||
|---|---|---|---|---|---|---|---|
| # | Trial | Reference | Treatments under Comparison | Treatment Group (Events/ Patients) | Controls (Events/ Patients) | Treatment Group (Events/ Patients) | Controls (Events/ Patients) |
| RCC1 | IMmotion151 trial (two-arm) | Rini et al. [11] | atezolizumab (1200 mg) + bevacizumab (15 mg/kg) intravenously, every 3 weeks; | 283/454 | 309/461 | 194/454 | 192/461 |
| sunitinib (50 mg) orally once daily for 4 weeks (6 weeks cycle). | |||||||
| RCC2 | JAVELIN Renal 101 Trial (two-arm) | Choueiri et al. [12] | avelumab (10 mg/kg) intravenously, every 2 weeks + axitinib (5 mg) orally twice daily; | 242/442 | 336/444 | 109/442 | 129/444 |
| sunitinib (50 mg) orally once daily for 4 weeks (6 weeks cycle). | |||||||
| RCC3 | CheckMate 214 Trial (two-arm) | Motzer et al. [13] | nivolumab (3 mg/kg) + ipilimumab (1 mg/kg) every 3 weeks for four cycles; | 266/550 | 358/546 | 297/550 | 339/546 |
| sunitinib (50 mg) orally once daily for 4 weeks (6 weeks cycle). | |||||||
| RCC4 | CLEAR Trial (three-arm) § | Motzer et al. [14] | lenvatinib (20 mg) orally once daily + pembrolizumab (200 mg) intravenously, every 3 weeks; | 160/355 | 205/357 | 80/355 | 105/357 |
| sunitinib (50 mg) orally once daily for 4 weeks (6 weeks cycle). | |||||||
| RCC5 | CheckMate 9ER Trial (two-arm) | Motzer et al. [15] | nivolumab (240 mg) intravenously, every 2 weeks + cabozantinib (40 mg) orally once daily; | 206/323 | 223/328 | 121/323 | 150/328 |
| sunitinib (50 mg) orally once daily for 4 weeks (6 weeks cycle). | |||||||
| RCC6 | KEYNOTE-426 Trial (two-arm) | Powles et al. [16] | pembrolizumab (200 mg) intravenously every 3 weeks (35 cycles) + axitinib (5 mg) orally twice daily; | 264/432 | 281/429 | 142/432 | 178/429 |
| sunitinib (50 mg) orally once daily for 4 weeks (6 weeks cycle). | |||||||
| HR | Lower 0.95 | Upper 0.95 | |
|---|---|---|---|
| atezolizumab + bevacizumab vs. avelumab + axitinib | 1.223 | 1.015 | 1.474 |
| atezolizumab + bevacizumab vs. nivolumab + ipilimumab | 1.462 | 1.227 | 1.743 |
| atezolizumab + bevacizumab vs. pembrolizumab + lenvatinib | 1.981 | 1.611 | 2.435 |
| atezolizumab + bevacizumab vs. nivolumab + cabozantinib | 1.415 | 1.163 | 1.721 |
| atezolizumab + bevacizumab vs. pembrolizumab + axitinib | 1.401 | 1.165 | 1.685 |
| avelumab + axitinib vs. atezolizumab + bevacizumab | 0.817 | 0.678 | 0.985 |
| avelumab + axitinib vs. nivolumab + ipilimumab | 1.195 | 0.998 | 1.432 |
| avelumab + axitinib vs. pembrolizumab + lenvatinib | 1.619 | 1.311 | 1.999 |
| avelumab + axitinib vs. nivolumab + cabozantinib | 1.156 | 0.946 | 1.413 |
| avelumab + axitinib vs. pembrolizumab + axitinib | 1.145 | 0.948 | 1.384 |
| nivolumab + ipilimumab vs. atezolizumab + bevacizumab | 0.684 | 0.574 | 0.815 |
| nivolumab + ipilimumab vs. avelumab + axitinib | 0.837 | 0.698 | 1.002 |
| nivolumab + ipilimumab vs. pembrolizumab + lenvatinib | 1.355 | 1.108 | 1.657 |
| nivolumab + ipilimumab vs. nivolumab + cabozantinib | 0.968 | 0.800 | 1.170 |
| nivolumab + ipilimumab vs. pembrolizumab + axitinib | 0.958 | 0.802 | 1.145 |
| pembrolizumab + lenvatinib vs. atezolizumab + bevacizumab | 0.505 | 0.411 | 0.621 |
| pembrolizumab + lenvatinib vs. avelumab + axitinib | 0.618 | 0.500 | 0.763 |
| pembrolizumab + lenvatinib vs. nivolumab + ipilimumab | 0.738 | 0.604 | 0.903 |
| pembrolizumab + lenvatinib vs. nivolumab + cabozantinib | 0.714 | 0.574 | 0.889 |
| pembrolizumab + lenvatinib vs. pembrolizumab + axitinib | 0.707 | 0.574 | 0.872 |
| nivolumab + cabozantinib vs. atezolizumab + bevacizumab | 0.707 | 0.581 | 0.860 |
| nivolumab + cabozantinib vs. avelumab + axitinib | 0.865 | 0.708 | 1.057 |
| nivolumab + cabozantinib vs. nivolumab + ipilimumab | 1.033 | 0.854 | 1.250 |
| nivolumab + cabozantinib vs. pembrolizumab + lenvatinib | 1.400 | 1.125 | 1.743 |
| nivolumab + cabozantinib vs. pembrolizumab + axitinib | 0.990 | 0.812 | 1.208 |
| pembrolizumab + axitinib vs. atezolizumab + bevacizumab | 0.714 | 0.594 | 0.858 |
| pembrolizumab + axitinib vs. avelumab + axitinib | 0.873 | 0.723 | 1.055 |
| pembrolizumab + axitinib vs. nivolumab + ipilimumab | 1.043 | 0.873 | 1.247 |
| pembrolizumab + axitinib vs. pembrolizumab + lenvatinib | 1.414 | 1.147 | 1.742 |
| pembrolizumab + axitinib vs. nivolumab + cabozantinib | 1.010 | 0.828 | 1.231 |
| HR | Lower 0.95 | Upper 0.95 | |
|---|---|---|---|
| atezolizumab + bevacizumab vs. avelumab + axitinib | 1.263 | 0.97 | 1.645 |
| atezolizumab + bevacizumab vs. nivolumab + ipilimumab | 1.474 | 1.181 | 1.840 |
| atezolizumab + bevacizumab vs. pembrolizumab + lenvatinib | 1.888 | 1.412 | 2.523 |
| atezolizumab + bevacizumab vs. nivolumab + cabozantinib | 1.270 | 0.976 | 1.654 |
| atezolizumab + bevacizumab vs. pembrolizumab + axitinib | 1.639 | 1.256 | 2.138 |
| avelumab + axitinib vs. atezolizumab + bevacizumab | 0.791 | 0.608 | 1.030 |
| avelumab + axitinib vs. nivolumab + ipilimumab | 1.167 | 0.909 | 1.498 |
| avelumab + axitinib vs. pembrolizumab + lenvatinib | 1.494 | 1.093 | 2.042 |
| avelumab + axitinib vs. nivolumab + cabozantinib | 1.005 | 0.754 | 1.341 |
| avelumab + axitinib vs. pembrolizumab + axitinib | 1.297 | 0.970 | 1.734 |
| nivolumab + ipilimumab vs. atezolizumab + bevacizumab | 0.678 | 0.543 | 0.847 |
| nivolumab + ipilimumab vs. avelumab + axitinib | 0.857 | 0.667 | 1.1 |
| nivolumab + ipilimumab vs. pembrolizumab + lenvatinib | 1.28 | 0.970 | 1.690 |
| nivolumab + ipilimumab vs. nivolumab + cabozantinib | 0.862 | 0.671 | 1.106 |
| nivolumab + ipilimumab vs. pembrolizumab + axitinib | 1.112 | 0.864 | 1.431 |
| pembrolizumab + lenvatinib vs. atezolizumab + bevacizumab | 0.530 | 0.396 | 0.708 |
| pembrolizumab + lenvatinib vs. avelumab + axitinib | 0.669 | 0.490 | 0.915 |
| pembrolizumab + lenvatinib vs. nivolumab + ipilimumab | 0.781 | 0.592 | 1.031 |
| pembrolizumab + lenvatinib vs. nivolumab + cabozantinib | 0.673 | 0.492 | 0.920 |
| pembrolizumab + lenvatinib vs. pembrolizumab + axitinib | 0.868 | 0.634 | 1.189 |
| nivolumab + cabozantinib vs. atezolizumab + bevacizumab | 0.787 | 0.605 | 1.025 |
| nivolumab + cabozantinib vs. avelumab + axitinib | 0.995 | 0.746 | 1.327 |
| nivolumab + cabozantinib vs. nivolumab + ipilimumab | 1.161 | 0.904 | 1.490 |
| nivolumab + cabozantinib vs. pembrolizumab + lenvatinib | 1.486 | 1.087 | 2.031 |
| nivolumab + cabozantinib vs. pembrolizumab + axitinib | 1.29 | 0.965 | 1.724 |
| pembrolizumab + axitinib vs. atezolizumab + bevacizumab | 0.61 | 0.468 | 0.796 |
| pembrolizumab + axitinib vs. avelumab + axitinib | 0.771 | 0.577 | 1.03 |
| pembrolizumab + axitinib vs. nivolumab + ipilimumab | 0.9 | 0.699 | 1.158 |
| pembrolizumab + axitinib vs. pembrolizumab + lenvatinib | 1.152 | 0.841 | 1.577 |
| pembrolizumab + axitinib vs. nivolumab + cabozantinib | 0.775 | 0.58 | 1.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ossato, A.; Mengato, D.; Chiumente, M.; Messori, A.; Damuzzo, V. Progression-Free and Overall Survival of First-Line Treatments for Advanced Renal Cell Carcinoma: Indirect Comparison of Six Combination Regimens. Cancers 2023, 15, 2029. https://doi.org/10.3390/cancers15072029
Ossato A, Mengato D, Chiumente M, Messori A, Damuzzo V. Progression-Free and Overall Survival of First-Line Treatments for Advanced Renal Cell Carcinoma: Indirect Comparison of Six Combination Regimens. Cancers. 2023; 15(7):2029. https://doi.org/10.3390/cancers15072029
Chicago/Turabian StyleOssato, Andrea, Daniele Mengato, Marco Chiumente, Andrea Messori, and Vera Damuzzo. 2023. "Progression-Free and Overall Survival of First-Line Treatments for Advanced Renal Cell Carcinoma: Indirect Comparison of Six Combination Regimens" Cancers 15, no. 7: 2029. https://doi.org/10.3390/cancers15072029