
Radiomics Analysis of 18F-FDG PET/CT for Prognosis Prediction in Patients with Stage III Non-Small Cell Lung Cancer Undergoing Neoadjuvant Chemoradiation Therapy Followed by Surgery
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
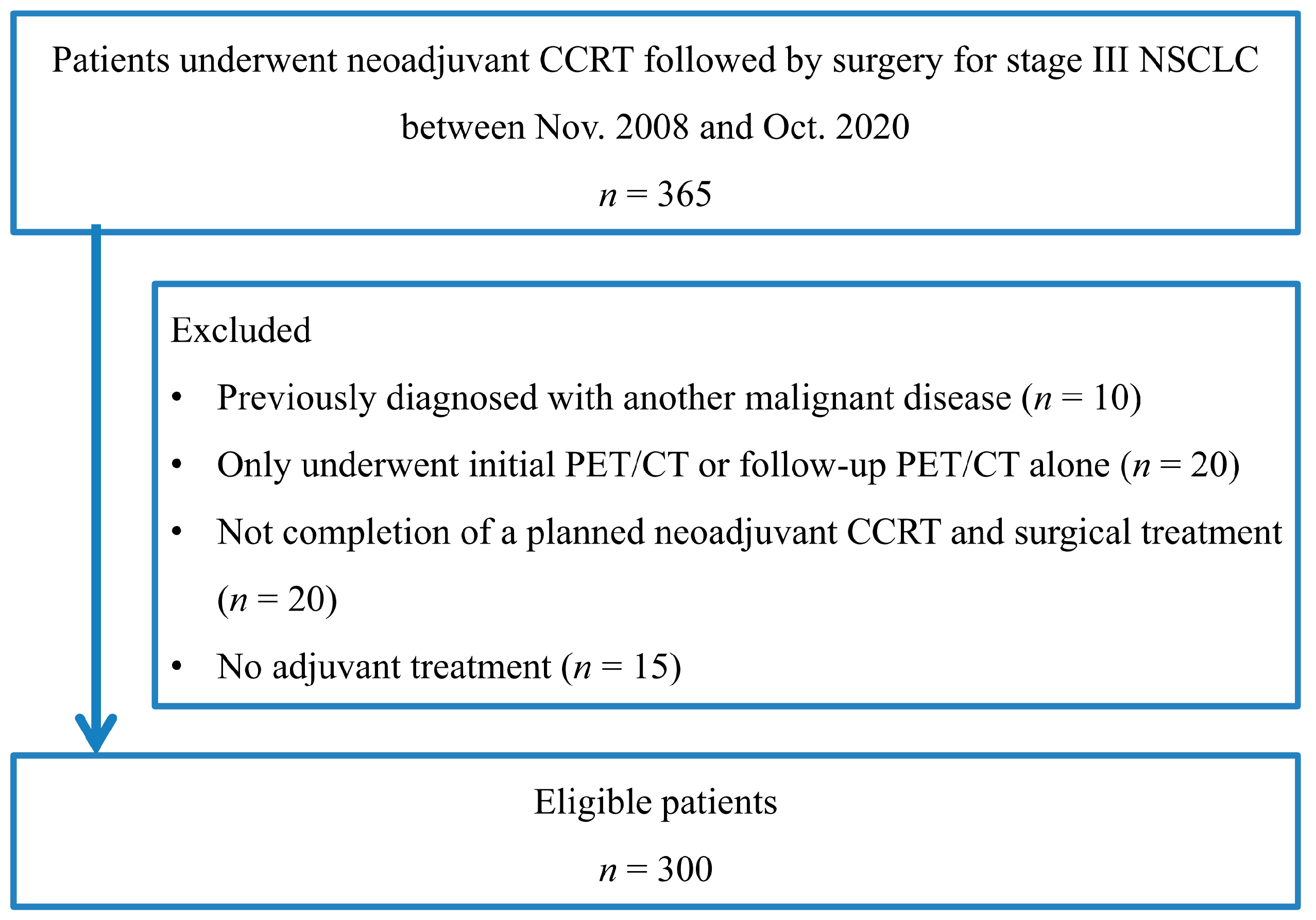
2.1. Subjects
2.2. 18F-FDG PET/CT Acquisition and Analysis
2.3. Neoadjuvant CCRT and Histopathologic Findings
2.4. Postoperative Treatment and Follow-Up
2.5. Feature Selection and Radiomic Feature Construction
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Conventional PET Parameters of Primary Tumors and Overall Survival
3.3. Feature Selection and LASSO Score for Predicting OS
3.4. Multivariate Survival Analysis
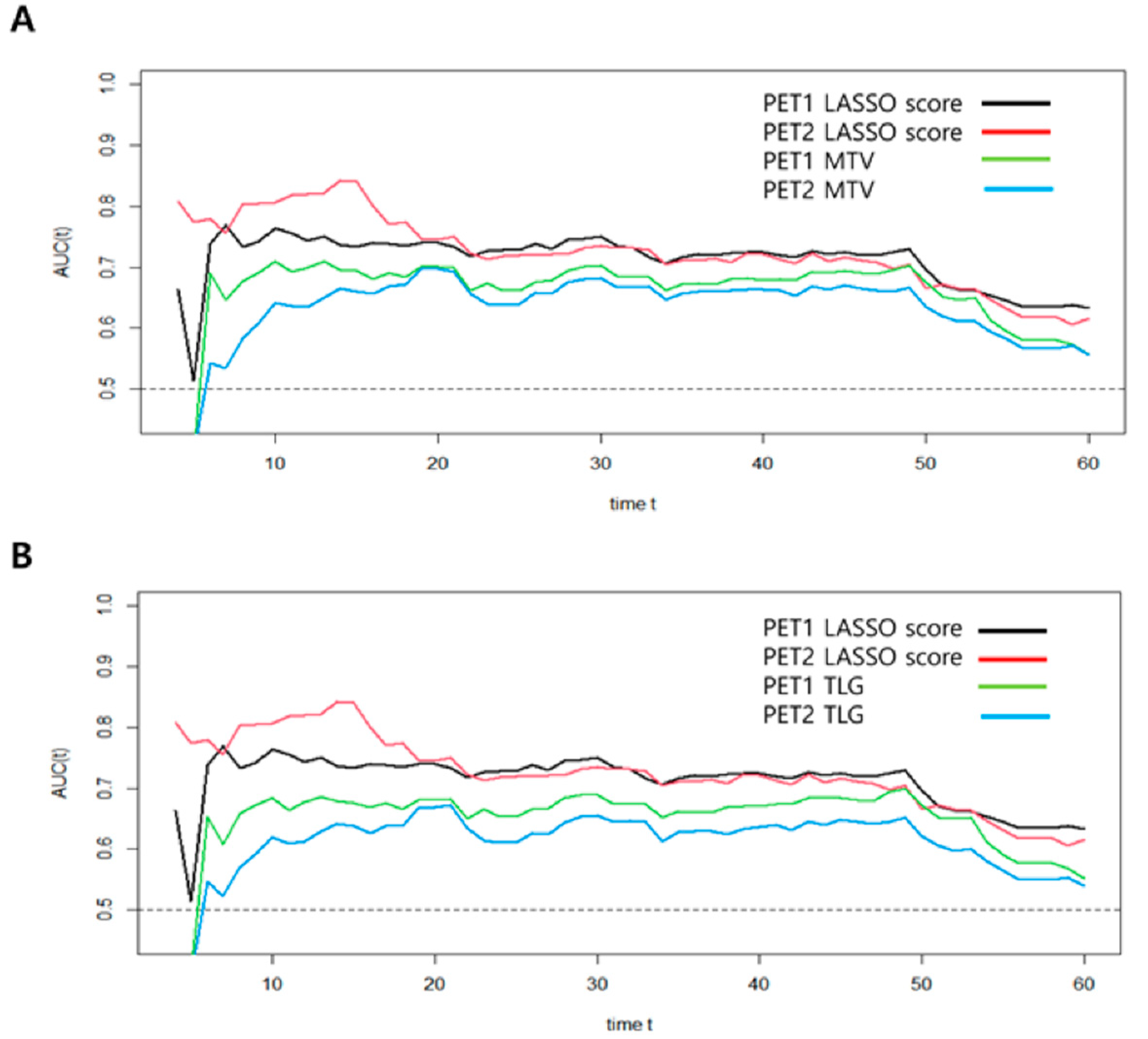
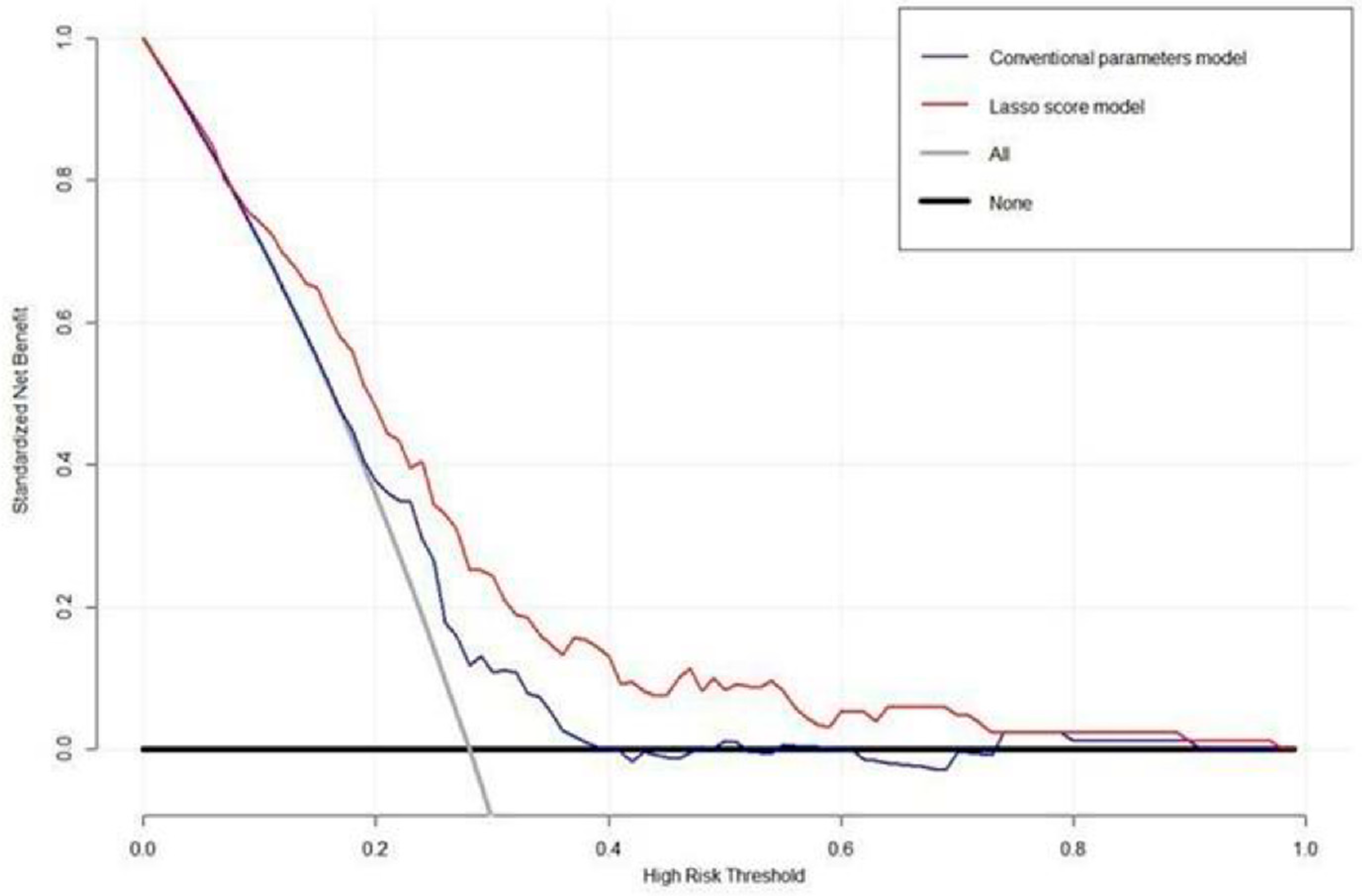
3.5. Assessment of Predictive Performance Using Time-Dependent ROC and Decision Curve Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics, 2014. CA Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef]
- Arbour, K.C.; Riely, G.J. Systematic therapy for locally advanced and metastatic non-small cell lung cancer: A review. JAMA 2019, 322, 764–774. [Google Scholar] [CrossRef]
- Morgensztern, D.; Ng, S.H.; Gao, F.; Govindan, R. Trends in Stage Distribution for Patients with Non-small Cell Lung Cancer: A National Cancer Database Survey. J. Thorac. Oncol. 2010, 5, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.K.; Cho, J.H.; Choi, Y.S.; Zo, J.I.; Shim, Y.M.; Park, K.; Ahn, M.-J.; Ahn, Y.C.; Kim, K.; Kim, J. Outcomes of neoadjuvant concurrent chemoradiotherapy followed by surgery for non-small-cell lung cancer with N2 disease. Lung Cancer 2016, 96, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.J.; Lee, H.Y.; Lee, K.S.; Han, J.; Kwon, O.J.; Park, K.; Ahn, Y.C.; Kim, B.T.; Shim, Y.M. Predictive factors for survival in stage IIIA N2 NSCLC paients treated with neoadjuvant CCRT followed by surgery. Cancer Chemother Pharmacol. 2015, 75, 77–85. [Google Scholar] [CrossRef]
- Hyun, S.H.; Ahn, H.K.; Ahn, M.-J.; Ahn, Y.C.; Kim, J.; Shim, Y.M.; Choi, J.Y. Volume-Based Assessment With 18F-FDG PET/CT Improves Outcome Prediction for Patients With Stage IIIA-N2 Non–Small Cell Lung Cancer. Am. J. Roentgenol. 2015, 205, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Kim, H.K.; Cho, J.H.; Choi, Y.S.; Kim, K.; Kim, J.; Zo, J.I.; Sun, J.-M.; Ahn, M.-J.; Park, K.; et al. Adjuvant therapy in stage IIIA-N2 non-small cell lung cancer after neoadjuvant concurrent chemoradiotherapy followed by surgery. J. Thorac. Dis. 2020, 12, 2602–2613. [Google Scholar] [CrossRef]
- Chen, H.H.W.; Chiu, N.-T.; Su, W.-C.; Guo, H.-R.; Lee, B.-F. Prognostic Value of Whole-Body Total Lesion Glycolysis at Pretreatment FDG PET/CT in Non–Small Cell Lung Cancer. Radiology 2012, 264, 559–566. [Google Scholar] [CrossRef]
- Hyun, S.H.; Choi, J.Y.; Kim, K.; Kim, J.; Shim, Y.M.; Um, S.-W.; Kim, H.; Lee, K.-H.; Kim, B.-T. Volume-Based Parameters of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography Improve Outcome Prediction in Early-Stage Non–Small Cell Lung Cancer After Surgical Resection. Ann. Surg. 2013, 257, 364–370. [Google Scholar] [CrossRef]
- Hyun, S.H.; Ahn, H.K.; Kim, H.; Ahn, M.-J.; Park, K.; Ahn, Y.C.; Kim, J.; Shim, Y.M.; Choi, J.Y. Volume-based assessment by 18F-FDG PET/CT predicts survival in patients with stage III non-small-cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2013, 41, 50–58. [Google Scholar] [CrossRef]
- Antunovic, L.; De Sanctis, R.; Cozzi, L.; Kirienko, M.; Sagona, A.; Torrisi, R.; Tinterri, C.; Santoro, A.; Chiti, A.; Zelic, R.; et al. PET/CT radiomics in breast cancer: Promising tool for prediction of pathological response to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Park, S.; Bang, J.I.; Kim, E.K.; Lee, H.Y. Metabolic radiomics for pretreatment (18)F-FDG PET/CT to characterize locally advanced breast cancer: Histopathologic characteristics, response to neoadjuvant chemotherapy, and prognosis. Sci. Rep. 2017, 7, 1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, S.H.; Kim, J.; Joung, J.-G.; Cha, H.; Park, W.-Y.; Ahn, J.S.; Ahn, M.-J.; Park, K.; Choi, J.Y.; Lee, K.-H.; et al. Correlations between metabolic texture features, genetic heterogeneity, and mutation burden in patients with lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 46, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Cheon, M.; Park, Y.J.; Hyun, S.H.; Zo, J.I.; Um, S.-W.; Won, H.-H.; Lee, K.-H.; Kim, B.-T.; Choi, J.Y. Machine learning-based diagnostic method of pre-therapeutic 18F-FDG PET/CT for evaluating mediastinal lymph nodes in non-small cell lung cancer. Eur. Radiol. 2021, 31, 4184–4194. [Google Scholar] [CrossRef]
- Yoo, J.; Lee, J.; Cheon, M.; Woo, S.-K.; Ahn, M.-J.; Pyo, H.R.; Choi, Y.S.; Han, J.H.; Choi, J.Y. Predictive Value of 18F-FDG PET/CT Using Machine Learning for Pathological Response to Neoadjuvant Concurrent Chemoradiotherapy in Patients with Stage III Non-Small Cell Lung Cancer. Cancers 2022, 14, 1987. [Google Scholar] [CrossRef]
- Yang, L.; Wang, S.; Zhou, Y.; Lai, S.; Xiao, G.; Gazdar, A.; Xie, Y. Evaluation of the 7th and 8th editions of the AJCC/UICC TNM staging systems for lung cancer in a large North American cohort. Oncotarget 2017, 8, 66784–66795. [Google Scholar] [CrossRef] [Green Version]
- O, J.H.; Lodge, M.A.; Wahl, R.L. Practical PERCIST: A Simplified Guide to PET Response Criteria in Solid Tumors 1.0. Radiology 2016, 280, 576–584. [Google Scholar] [CrossRef] [Green Version]
- Cottrell, T.; Thompson, E.; Forde, P.; Stein, J.; Duffield, A.; Anagnostou, V.; Rekhtman, N.; Anders, R.; Cuda, J.; Illei, P.; et al. Pathologic features of response to neoadjuvant anti-PD-1 in resected non-small-cell lung carcinoma: A proposal for quantitative immune-related pathologic response criteria (irPRC). Ann. Oncol. 2018, 29, 1853–1860. [Google Scholar] [CrossRef]
- Mouillet, G.; Monnet, E.; Milleron, B.; Puyraveau, M.; Quoix, E.; David, P.; Ducoloné, A.; Molinier, O.; Zalcman, G.; Depierre, A.; et al. Pathologic Complete Response to Preoperative Chemotherapy Predicts Cure in Early-Stage Non–Small-Cell Lung Cancer: Combined Analysis of Two IFCT Randomized Trials. J. Thorac. Oncol. 2012, 7, 841–849. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhang, Y.; Fang, Q.; Zhang, X.; Hou, P.; Wu, H.; Wang, X. Radiomics analysis of [18F]FDG PET/CT for microvascular invasion and prognosis prediction in very-early- and early-stage hepatocellular carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2599–2614. [Google Scholar] [CrossRef]
- Paesmans, M.; Berghmans, T.; Dusart, M.; Garcia, C.; Hossein-Foucher, C.; Lafitte, J.-J.; Mascaux, C.; Meert, A.-P.; Roelandts, M.; Scherpereel, A.; et al. Primary Tumor Standardized Uptake Value Measured on Fluorodeoxyglucose Positron Emission Tomography Is of Prognostic Value for Survival in Non-small Cell Lung Cancer: Update of a Systematic Review and Meta-Analysis by the European Lung Cancer Working Party for the International Association for the Study of Lung Cancer Staging Project. J. Thorac. Oncol. 2010, 5, 612–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoang, J.K.; Hoagland, L.F.; Coleman, R.E.; Coan, A.D.; Herndon, J.E., 2nd; Patz, E.F., Jr. Prognostic value of fluorine-18 fluorodeoxyglucose positron emission tomography imaging in patients with advanced-stage non-small-cell lung carcinoma. J. Clin. Oncol. 2008, 26, 1459–1464. [Google Scholar] [CrossRef]
- Vesselle, H.; Freeman, J.D.; Wiens, L.; Stern, J.; Nguyen, H.Q.; Hawes, S.E.; Bastian, P.; Salskov, A.; Vallières, E.; Wood, D.E. Fluorodeoxyglucose Uptake of Primary Non-Small Cell Lung Cancer at Positron Emission Tomography: New Contrary Data on Prognostic Role. Clin. Cancer Res. 2007, 13, 3255–3263. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, B.; Frenzel, T.; Schmitz, R.; Schumacher, U.; Wedemann, G. Modeling Growth of Tumors and Their Spreading Behavior Using Mathematical Functions. Methods Mol. Biol. 2019, 1878, 263–277. [Google Scholar] [CrossRef]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyka, T.; Bundschuh, R.A.; Andratschke, N.; Mayer, B.; Specht, H.M.; Papp, L.; Zsótér, N.; Essler, M. Textural features in pre-treatment [F18]-FDG-PET/CT are correlated with risk of local recurrence and disease-specific survival in early stage NSCLC patients receiving primary stereotactic radiation therapy. Radiat. Oncol. 2015, 10, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Yuan, Q.; Lv, W.; Xi, S.; Huang, W.; Sun, Z.; Chen, H.; Zhao, L.; Liu, W.; Hu, Y.; et al. Radiomic signature of 18F fluorodeoxyglucose PET/CT for prediction of gastric cancer survival and chemotherapeutic benefits. Theranostics 2018, 8, 5915–5928. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.P.; Choi, J.Y.; Choi, J.H.; Cho, Y.S.; Hur, S.M.; Kim, Z.; Lim, C.W.; Seo, S.; Moon, J.E.; Woo, S.-K.; et al. Prognostic Value of Axillary Lymph Node Texture Parameters Measured by Pretreatment 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Locally Advanced Breast Cancer with Neoadjuvant Chemotherapy. Diagnostics 2022, 12, 2285. [Google Scholar] [CrossRef]
- Huang, Y.; Liu, Z.; He, L.; Chen, X.; Pan, D.; Ma, Z.; Liang, C.; Tian, J.; Liang, C. Radiomics Signature: A Potential Biomarker for the Prediction of Disease-Free Survival in Early-Stage (I or II) Non—Small Cell Lung Cancer. Radiology 2016, 281, 947–957. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Lu, Z. Radiomics Analysis of PET and CT Components of 18F-FDG PET/CT Imaging for Prediction of Progression-Free Survival in Advanced High-Grade Serous Ovarian Cancer. Front. Oncol. 2021, 11, 638124. [Google Scholar] [CrossRef]
- Ma, J.; Guo, D.; Miao, W.; Wang, Y.; Yan, L.; Wu, F.; Zhang, C.; Zhang, R.; Zuo, P.; Yang, G.; et al. The value of 18F-FDG PET/CT-based radiomics in predicting perineural invasion and outcome in non-metastatic colorectal cancer. Abdom. Radiol. 2022, 47, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Iravani, A.; Turgeon, G.-A.; Akhurst, T.; Callahan, J.W.; Bressel, M.; Everitt, S.J.; Siva, S.; Hofman, M.S.; Hicks, R.J.; Ball, D.L.; et al. PET-detected pneumonitis following curative-intent chemoradiation in non-small cell lung cancer (NSCLC): Recognizing patterns and assessing the impact on the predictive ability of FDG-PET/CT response assessment. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1869–1877. [Google Scholar] [CrossRef] [PubMed]
- Werner-Wasik, M.; Nelson, A.D.; Choi, W.; Arai, Y.; Faulhaber, P.F.; Kang, P.; Almeida, F.D.; Xiao, Y.; Ohri, N.; Brockway, K.D.; et al. What Is the Best Way to Contour Lung Tumors on PET Scans? Multiobserver Validation of a Gradient-Based Method Using a NSCLC Digital PET Phantom. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1164–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Patients (%) | |
|---|---|---|
| Age, mean (range), year | 60.0 (31–77) | |
| Sex | Male | 202 (67.3) |
| Female | 98 (32.7) | |
| Histology | Adenocarcinoma | 211 (70.3) |
| Squamous cell carcinoma | 86 (28.7) | |
| Others | 3 (1.0) | |
| T stage | T1 | 89 (29.7) |
| T2 | 134 (44.7) | |
| T3 | 57 (19.0) | |
| T4 | 20 (6.6) | |
| N stage | N0 | 2 (0.7) |
| N1 | 2 (0.7) | |
| N2 | 289 (96.3) | |
| N3 | 7 (2.3) | |
| Tumor stage | IIIA | 222 (74.0) |
| IIIB | 74 (24.7) | |
| IIIC | 4 (1.3) | |
| Type of surgery | Lobectomy | 249 (83.0) |
| Bilobectomy | 15 (5.0) | |
| Pneumonectomy | 11 (3.7) | |
| Lobectomy with en bloc wedge resection | 25 (8.3) | |
| Pathologic response | pCR | 20 (6.7) |
| Non-pCR | 280 (93.3) | |
| MPR | 144 (48.0) | |
| Non-MPR | 156 (52.0) | |
| PERCIST | CMR | 44 (14.7) |
| PMR | 196 (65.3) | |
| SMD | 59 (19.7) | |
| PMD | 1 (0.3) | |
| Adjuvant therapy | Chemotherapy | 189 (63.0) |
| Radiotherapy | 92 (30.7) | |
| Chemoradiotherapy | 19 (6.3) |
| PET1 | Matrix | Index |
| Voxel-alignment matrix | Run percentage, low-intensity run emphasis | |
| Neighborhood intensity difference matrix | Busyness, strength | |
| Intensity size-zone matrix | Zone percentage, low-intensity zone emphasis, high-intensity short-zone emphasis | |
| Voxel statistics | SUV variance, SUV kurtosis, SUV kurtosis (bias corrected), tumor volume | |
| Texture spectrum | Max spectrum | |
| Texture feature coding co-occurrence matrix | Inverse difference moment, variance | |
| PET2 | Matrix | Index |
| Co-occurrence matrix | Contrast | |
| Voxel-alignment matrix | Low-intensity long-run emphasis, high-intensity long-run emphasis | |
| Neighborhood intensity difference matrix | Complexity | |
| Intensity size-zone matrix | Zone percentage, low-intensity short-zone emphasis, low-intensity large-zone emphasis, high-intensity large-zone emphasis | |
| Voxel statistics | Minimum SUV, SUV skewness, SUV kurtosis, SUV skewness (bias corrected), entropy | |
| Texture spectrum | Max spectrum, black-white symmetry | |
| Texture feature coding | Coarseness | |
| Texture feature coding co-occurrence matrix | Second angular moment, intensity |
| Variable | HR | 95% CI | p Value | |
|---|---|---|---|---|
| Age | 1.016 | 0.991–1.043 | 0.216 | |
| Sex | Male vs. female | 1.988 | 1.191–3.316 | 0.009 * |
| Histology | Non-ADC vs. ADC | 1.595 | 1.023–2.487 | 0.039 * |
| T stage | T3/4 vs. T1/2 | 1.966 | 1.256–3.079 | 0.003 * |
| N stage | N2/N3 vs. N0/N1 | 1.110 | 0.154–8.006 | 0.917 |
| Tumor stage | IIIb/IIIc vs. IIIa | 2.067 | 1.329–3.215 | 0.001 * |
| Pathologic response | Non-pCR vs. pCR | 1.741 | 0.839–3.615 | 0.137 |
| Non-MPR vs. MPR | 1.045 | 0.680–1.605 | 0.841 | |
| PERCIST | SMD/PMD vs. CMR/PMR | 1.193 | 0.692–2.058 | 0.525 |
| PET1 | SUVmax | 1.015 | 0.975–1.056 | 0.476 |
| SUVmean | 1.023 | 0.928–1.128 | 0.653 | |
| MTV | 1.005 | 1.002–1.008 | <0.001 * | |
| TLG | 1.002 | 1.001–1.003 | 0.005 * | |
| LASSO score | 3.164 | 2.048–4.887 | <0.001 * | |
| PET2 | SUVmax | 1.008 | 0.941–1.080 | 0.823 |
| SUVmean | 0.988 | 0.847–1.153 | 0.880 | |
| MTV | 1.010 | 1.003–1.016 | 0.003 * | |
| TLG | 1.003 | 1.001–1.005 | 0.036 * | |
| LASSO score | 2.836 | 2.102–3.826 | <0.001 * | |
| %ΔSUVmax | 1.003 | 0.994–1.011 | 0.538 | |
| %ΔSUVmean | 1.003 | 0.995–1.012 | 0.732 | |
| %ΔMTV | 1.001 | 0.998–1.002 | 0.876 | |
| %ΔTLG | 0.999 | 0.994–1.006 | 0.982 |
| HR | 95% CI | p Value | |
|---|---|---|---|
| MTV model | |||
| Sex (male vs. female) | 1.703 | 0.977–2.967 | 0.061 |
| Histology (non-ADC vs. ADC) | 1.309 | 0.793–2.162 | 0.293 |
| T stage (T3/T4 vs. T1/T2) | 1.589 | 0.217–1.822 | 0.629 |
| Tumor stage (IIIb/IIIc vs. IIIa) | 1.848 | 0.686–4.980 | 0.225 |
| PET1 MTV (>32.23 vs. ≤32.23) | 1.001 | 0.995–1.008 | 0.712 |
| PET2 MTV (> 8.78 vs. ≤8.78) | 0.994 | 0.981–1.008 | 0.393 |
| PET1 LASSO score (>−0.884 vs. ≤−0.884) | 1.707 | 0.907–3.212 | 0.097 |
| PET2 LASSO score (>−0.737 vs. ≤−0.737) | 2.297 | 1.437–3.669 | <0.001 * |
| TLG model | |||
| Sex (male vs. female) | 1.674 | 0.960–2.919 | 0.067 |
| Histology (non-ADC vs. ADC) | 1.352 | 0.812–2.249 | 0.246 |
| T stage (T3/T4 vs. T1/T2) | 1.565 | 0.222–1.844 | 0.408 |
| Tumor stage (IIIb/IIIc vs. IIIa) | 1.863 | 0.694–5.005 | 0.217 |
| PET1 TLG (>247.73 vs. ≤247.73) | 0.999 | 0.999–1.001 | 0.883 |
| PET2 TLG (>10.36 vs. ≤10.36) | 0.999 | 0.994–1.004 | 0.670 |
| PET1 LASSO score (>−0.884 vs. ≤−0.884) | 1.787 | 0.950–3.362 | 0.072 |
| PET2 LASSO score (>−0.737 vs. ≤−0.737) | 2.084 | 1.419–3.060 | <0.001 * |
| 12 Months | 24 Months | 36 Months | 48 Months | 60 Months | |
|---|---|---|---|---|---|
| PET1 | |||||
| MTV | 0.598 | 0.646 | 0.654 | 0.658 | 0.653 |
| TLG | 0.573 | 0.625 | 0.635 | 0.639 | 0.637 |
| LASSO score | 0.695 | 0.715 | 0.718 | 0.719 | 0.707 |
| PET2 | |||||
| MTV | 0.596 | 0.644 | 0.652 | 0.655 | 0.653 |
| TLG | 0.504 | 0.575 | 0.588 | 0.596 | 0.597 |
| LASSO score | 0.790 | 0.778 | 0.764 | 0.755 | 0.733 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.; Lee, J.; Cheon, M.; Kim, H.; Choi, Y.S.; Pyo, H.; Ahn, M.-J.; Choi, J.Y. Radiomics Analysis of 18F-FDG PET/CT for Prognosis Prediction in Patients with Stage III Non-Small Cell Lung Cancer Undergoing Neoadjuvant Chemoradiation Therapy Followed by Surgery. Cancers 2023, 15, 2012. https://doi.org/10.3390/cancers15072012
Yoo J, Lee J, Cheon M, Kim H, Choi YS, Pyo H, Ahn M-J, Choi JY. Radiomics Analysis of 18F-FDG PET/CT for Prognosis Prediction in Patients with Stage III Non-Small Cell Lung Cancer Undergoing Neoadjuvant Chemoradiation Therapy Followed by Surgery. Cancers. 2023; 15(7):2012. https://doi.org/10.3390/cancers15072012
Chicago/Turabian StyleYoo, Jang, Jaeho Lee, Miju Cheon, Hojoong Kim, Yong Soo Choi, Hongryull Pyo, Myung-Ju Ahn, and Joon Young Choi. 2023. "Radiomics Analysis of 18F-FDG PET/CT for Prognosis Prediction in Patients with Stage III Non-Small Cell Lung Cancer Undergoing Neoadjuvant Chemoradiation Therapy Followed by Surgery" Cancers 15, no. 7: 2012. https://doi.org/10.3390/cancers15072012