
Association between Chronic Gingivitis and Cancer: A Retrospective Cohort Study of 19,782 Outpatients from the United Kingdom

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Database
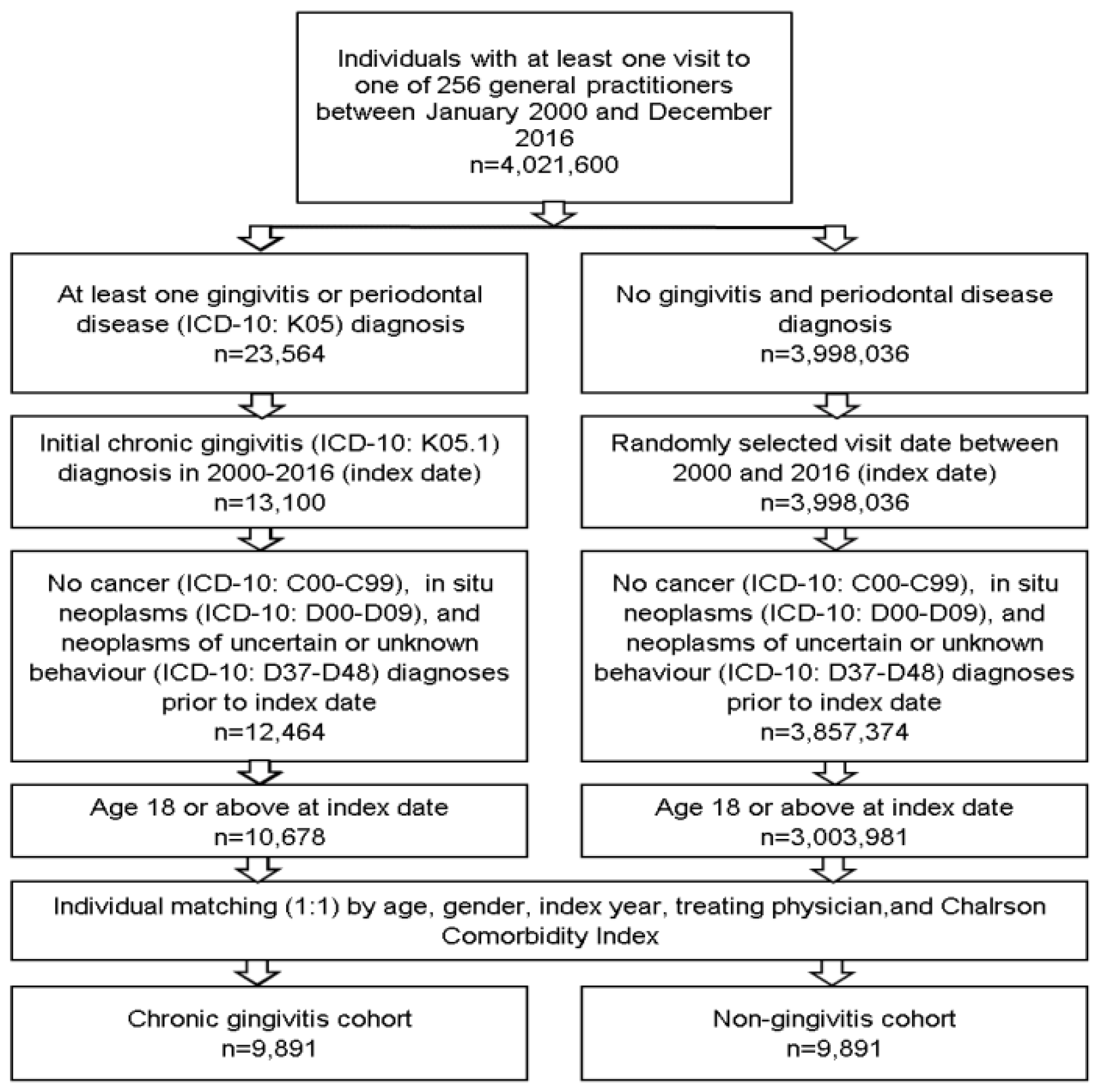
2.2. Study Population
2.3. Study Outcome and Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Sample
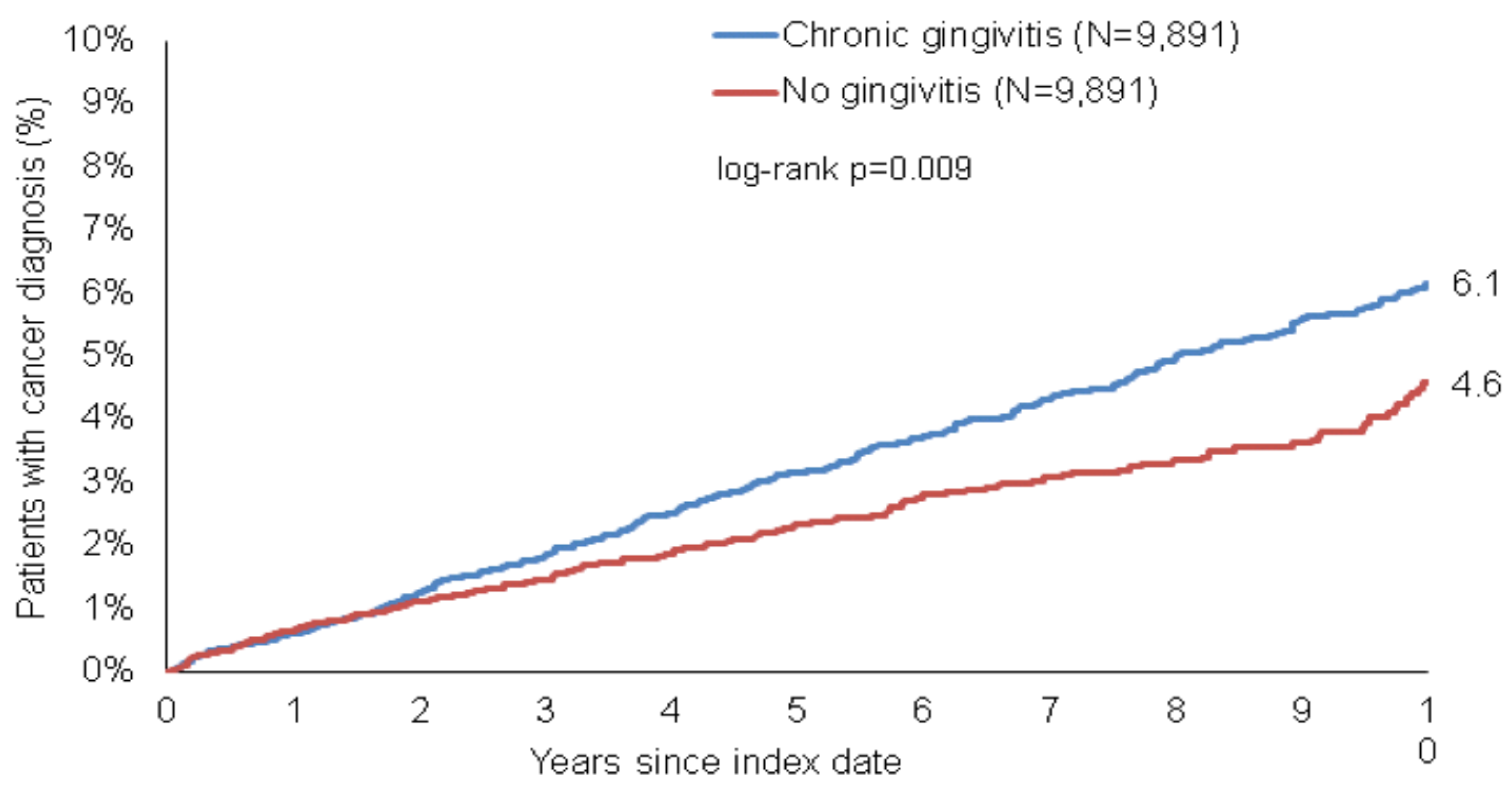
3.2. Gingivitis Is Associated with an Increased Incidence of Cancer
3.3. Age- and Sex Stratified Analyses
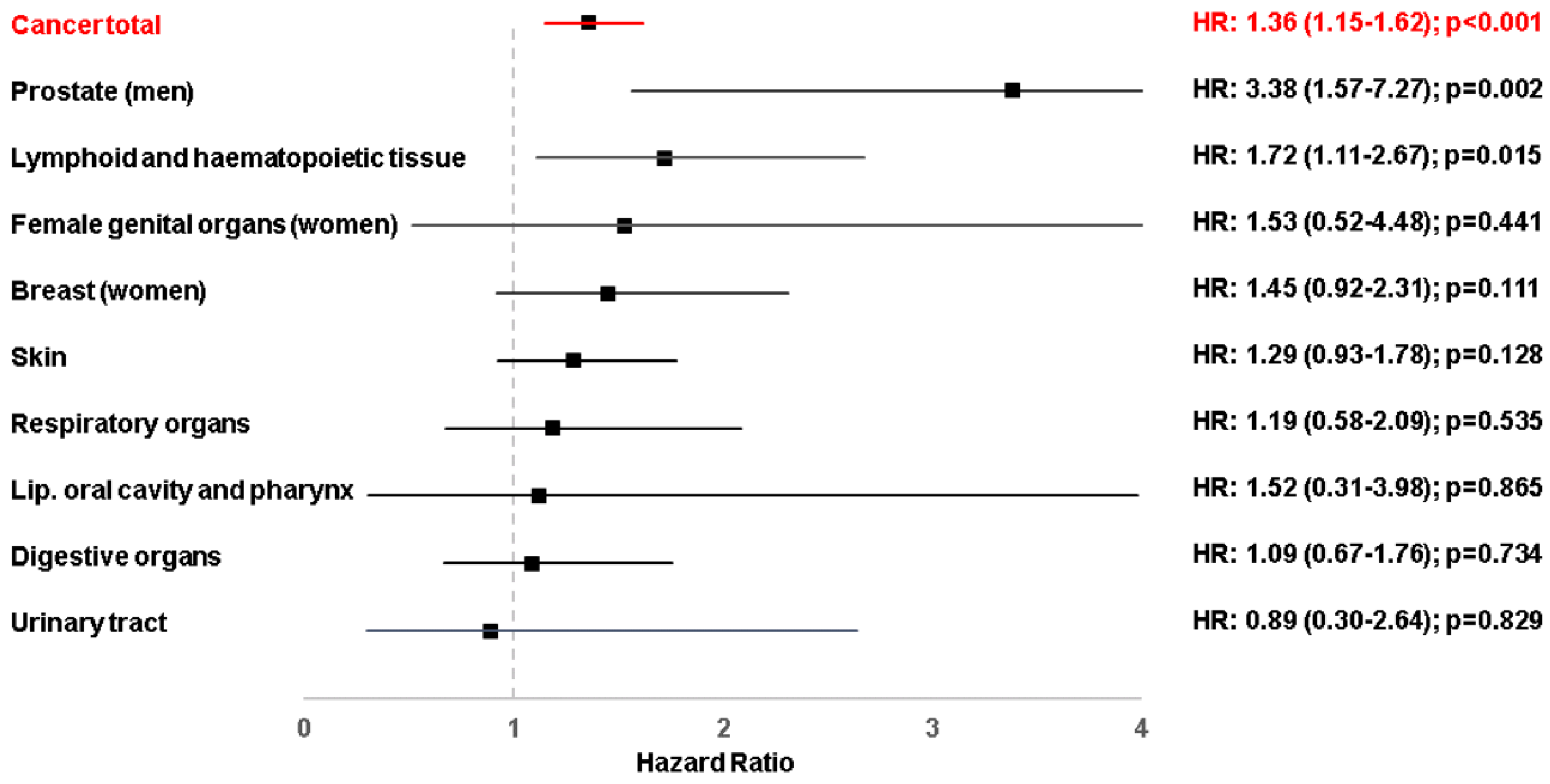
3.4. Cancer Site Stratified Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Michaud, D.S.; Fu, Z.; Shi, J.; Chung, M. Periodontal Disease, Tooth Loss, and Cancer Risk. Epidemiol. Rev. 2017, 39, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtfreter, B.; Kocher, T.; Hoffmann, T.; Desvarieux, M.; Micheelis, W. Prevalence of Periodontal Disease and Treatment Demands Based on a German Dental Survey (DMS IV). J. Clin. Periodontol. 2010, 37, 211–219. [Google Scholar] [CrossRef]
- Zeng, X.-T.; Xia, L.-Y.; Zhang, Y.-G.; Li, S.; Leng, W.-D.; Kwong, J.S.W. Periodontal Disease and Incident Lung Cancer Risk: A Meta-Analysis of Cohort Studies. J. Periodontol. 2016, 87, 1158–1164. [Google Scholar] [CrossRef]
- Alsalleeh, F.; Alhadlaq, A.S.; Althumiri, N.A.; AlMousa, N.; BinDhim, N.F. Public Awareness of the Association between Periodontal Disease and Systemic Disease. Healthcare 2022, 11, 88. [Google Scholar] [CrossRef] [PubMed]
- Fischer, R.G.; Filho, I.S.G.; da Cruz, S.S.; Oliveira, V.B.; Lira-Junior, R.; Scannapieco, F.A.; Rego, R.O. What Is the Future of Periodontal Medicine? Braz. Oral Res. 2021, 35, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Daltaban, Ö.; Enginar, A.Ü.; Üstün, K.; Hatipoğlu, M.; Kaçar, C.; Tuncer, T. Evaluating the Relationship between Ankylosing Spondylitis and Periodontal Disease: A Case-Control Study. Clin. Oral Investig. 2023, 27, 411–420. [Google Scholar] [CrossRef]
- King, S.; Church, L.; Garde, S.; Chow, C.K.; Akhter, R.; Eberhard, J. Targeting the Reduction of Inflammatory Risk Associated with Cardiovascular Disease by Treating Periodontitis Either Alone or in Combination with a Systemic Anti-Inflammatory Agent: Protocol for a Pilot, Parallel Group, Randomised Controlled Trial. BMJ Open 2022, 12, e063148. [Google Scholar] [CrossRef]
- Alhassani, A.A. The Influence of Periodontitis Case Definition on the Association between Periodontal Disease and Glycaemic Status. Community Dent. Oral Epidemiol. 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.-Z.; Liu, P.-Y.; Wu, T.-J.; Fan, C.-H.; Cheng, W.-C.; Huang, R.-Y.; Lin, G.-M. Localized Periodontitis and Kidney Function for the Risk of Proteinuria in Young Adults in the CHIEF Oral Health Study. Sci. Rep. 2022, 12, 19006. [Google Scholar] [CrossRef]
- Gao, B.; Wu, J.; Lv, K.; Shen, C.; Yao, H. Visualized Analysis of Hotspots and Frontiers in Diabetes-Associated Periodontal Disease Research: A Bibliometric Study. Ann. Transl. Med. 2022, 10, 1305. [Google Scholar] [CrossRef]
- Baciu, S.F.; Mesaroș, A.-Ș.; Kacso, I.M. Chronic Kidney Disease and Periodontitis Interplay-A Narrative Review. Int. J. Environ. Res. Public Health 2023, 20, 1298. [Google Scholar] [CrossRef] [PubMed]
- Terzic, M.; Aimagambetova, G.; Terzic, S.; Radunovic, M.; Bapayeva, G.; Laganà, A.S. Periodontal Pathogens and Preterm Birth: Current Knowledge and Further Interventions. Pathogens 2021, 10, 730. [Google Scholar] [CrossRef] [PubMed]
- Nannan, M.; Xiaoping, L.; Ying, J. Periodontal Disease in Pregnancy and Adverse Pregnancy Outcomes: Progress in Related Mechanisms and Management Strategies. Front. Med. 2022, 9, 963956. [Google Scholar] [CrossRef] [PubMed]
- Arora, M.; Weuve, J.; Fall, K.; Pedersen, N.L.; Mucci, L.A. An Exploration of Shared Genetic Risk Factors between Periodontal Disease and Cancers: A Prospective Co-Twin Study. Am. J. Epidemiol. 2010, 171, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Nwizu, N.N.; Marshall, J.R.; Moysich, K.; Genco, R.J.; Hovey, K.M.; Mai, X.; LaMonte, M.J.; Freudenheim, J.L.; Wactawski-Wende, J. Periodontal Disease and Incident Cancer Risk among Postmenopausal Women: Results from the Women’s Health Initiative Observational Cohort. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1255–1265. [Google Scholar] [CrossRef] [Green Version]
- Ogdie, A.; Langan, S.M.; Parkinson, J.; Dattani, H.; Kostev, K.; Gelfand, J.M. Medical Record Databases. In Pharmacoepidemiology; Wiley-Blackwell: Oxford, UK, 2012; pp. 224–243. [Google Scholar]
- Ebersole, J.L.; Machen, R.L.; Steffen, M.J.; Willmann, D.E. Systemic Acute-Phase Reactants, C-Reactive Protein and Haptoglobin, in Adult Periodontitis. Clin. Exp. Immunol. 1997, 107, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Wand, H.C.; Merchant, A.T.; Rimm, E.B. Periodontal Disease and Biomarkers Related to Cardiovascular Disease. J. Dent. Res. 2004, 83, 151–155. [Google Scholar] [CrossRef]
- Papadopoulos, G.; Kramer, C.D.; Slocum, C.S.; Weinberg, E.O.; Hua, N.; Gudino, C.v.; Hamilton, J.A.; Genco, C.A. A Mouse Model for Pathogen-Induced Chronic Inflammation at Local and Systemic Sites. J. Vis. Exp. 2014, 90, e51556. [Google Scholar] [CrossRef] [Green Version]
- Priyamvara, A.; Dey, A.K.; Bandyopadhyay, D.; Katikineni, V.; Zaghlol, R.; Basyal, B.; Barssoum, K.; Amarin, R.; Bhatt, D.L.; Lavie, C.J. Periodontal Inflammation and the Risk of Cardiovascular Disease. Curr. Atheroscler. Rep. 2020, 22, 28. [Google Scholar] [CrossRef]
- Zainal Abidin, Z.; Zainuren, Z.A.; Noor, E.; Mohd Nor, N.S.; Mohd Saffian, S.; Abdul Halim, R. Periodontal Health Status of Children and Adolescents with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Aust. Dent. J. 2021, 66, S15–S26. [Google Scholar] [CrossRef] [PubMed]
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuominen, H.; Rautava, J. Oral Microbiota and Cancer Development. Pathobiology 2021, 88, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Giovannucci, E.; Joshipura, K. Periodontal Disease, Tooth Loss, and Cancer Risk in Male Health Professionals: A Prospective Cohort Study. Lancet Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Michaud, D.S.; Lu, J.; Peacock-Villada, A.Y.; Barber, J.R.; Joshu, C.E.; Prizment, A.E.; Beck, J.D.; Offenbacher, S.; Platz, E.A. Periodontal Disease Assessed Using Clinical Dental Measurements and Cancer Risk in the ARIC Study. J. Natl. Cancer Inst. 2018, 110, 843–854. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Labonte, M.J.; Craig, S.G.; Finn, S.P.; Allott, E.H. Inflammation and Prostate Cancer: A Multidisciplinary Approach to Identifying Opportunities for Treatment and Prevention. Cancers 2022, 14, 1367. [Google Scholar] [CrossRef]
- Sfanos, K.S.; de Marzo, A.M. Prostate Cancer and Inflammation: The Evidence. Histopathology 2012, 60, 199–215. [Google Scholar] [CrossRef] [Green Version]
- Boyapati, R.; Swarna, C.; Devulapalli, N.; Sanivarapu, S.; Katuri, K.; Kolaparthy, L. Unveiling the Link between Prostatitis and Periodontitis. Contemp. Clin. Dent. 2018, 9, 524. [Google Scholar] [CrossRef]
- Noack, B.; Genco, R.J.; Trevisan, M.; Grossi, S.; Zambon, J.J.; De Nardin, E. Periodontal Infections Contribute to Elevated Systemic C-Reactive Protein Level. J. Periodontol. 2001, 72, 1221–1227. [Google Scholar] [CrossRef] [Green Version]
- Jang, T.L.; Schaeffer, A.J. The Role of Cytokines in Prostatitis. World J. Urol. 2003, 21, 95–99. [Google Scholar] [CrossRef]
- Joshi, N.; Bissada, N.F.; Bodner, D.; MacLennan, G.T.; Narendran, S.; Jurevic, R.; Skillicorn, R. Association Between Periodontal Disease and Prostate-Specific Antigen Levels in Chronic Prostatitis Patients. J. Periodontol. 2010, 81, 864–869. [Google Scholar] [CrossRef]
- Mao, M.; Zhu, H.; Xie, Y.; Ni, D.; Zhu, F.; Chen, Q. Correlation between Periodontitis and Prostate-Specific Antigen Levels in the Elderly Chinese Male Population. BMC Oral Health 2022, 22, 163. [Google Scholar] [CrossRef]
- Estemalik, J.; Demko, C.; Bissada, N.F.; Joshi, N.; Bodner, D.; Shankar, E.; Gupta, S. Simultaneous Detection of Oral Pathogens in Subgingival Plaque and Prostatic Fluid of Men with Periodontal and Prostatic Diseases. J. Periodontol. 2017, 88, 823–829. [Google Scholar] [CrossRef]
- Bissada, N.A.N.F. Periodontal Treatment Improves Prostate Symptoms and Lowers Serum PSA in Men with High PSA and Chronic Periodontitis. Dentistry 2015, 5, 1. [Google Scholar]
- Elebyary, O.; Barbour, A.; Fine, N.; Tenenbaum, H.C.; Glogauer, M. The Crossroads of Periodontitis and Oral Squamous Cell Carcinoma: Immune Implications and Tumor Promoting Capacities. Front. Oral Health 2020, 1, 584705. [Google Scholar] [CrossRef]
- Kurtzman, G.M.; Horowitz, R.A.; Johnson, R.; Prestiano, R.A.; Klein, B.I. The Systemic Oral Health Connection: Biofilms. Medicine 2022, 101, E30517. [Google Scholar] [CrossRef]
- Morrison, A.G.; Sarkar, S.; Umar, S.; Lee, S.T.M.; Thomas, S.M. The Contribution of the Human Oral Microbiome to Oral Disease: A Review. Microorganisms 2023, 11, 318. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Kanaan, M.; Siddiqi, K.; Sinha, D.N.; Mehrotra, R. Oral Cancer Risk Assessment for Different Types of Smokeless Tobacco Products Sold Worldwide: A Review of Reviews and Meta-Analyses. Cancer Prev. Res. 2022, 15, 733–745. [Google Scholar] [CrossRef]
- Bach, L.; Kostev, K.; Schiffmann, L.; Kalder, M. Association between Thyroid Gland Diseases and Breast Cancer: A Case–Control Study. Breast Cancer Res. Treat. 2020, 182, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Becher, H.; Kostev, K.; Schröder-Bernhardi, D. Validity and Representativeness of the “Disease Analyzer” Patient Database for Use in Pharmaco-Epidemiological and Pharmacoeconomic Studies. Int. J. Clin. Pharmacol. Ther. 2009, 47, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Labenz, C.; Kostev, K.; Kaps, L.; Galle, P.R.; Schattenberg, J.M. Incident Dementia in Elderly Patients with Nonalcoholic Fatty Liver Disease in Germany. Dig. Dis. Sci. 2020, 66, 3179–3185. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Kostev, K.; Keitel, V.; Tacke, F.; Roderburg, C.; Luedde, T. An Elevated FIB-4 Score Predicts Liver Cancer Development: A Longitudinal Analysis from 29,999 NAFLD Patients. J. Hepatol. 2021, 76, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Jördens, M.S.; Luedde, M.; Roderburg, C.; Demir, M.; Luedde, T.; Kostev, K.; Loosen, S.H. Pulmonary Hypertension Is Associated with an Increased Incidence of NAFLD: A Retrospective Cohort Study of 18,910 Patients. J. Intern. Med. 2021, 290, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Kostev, K.; Luedde, M.; Luedde, T.; Roderburg, C. Low Blood Levels of High-Density Lipoprotein (HDL) Cholesterol Are Positively Associated with Cancer. J. Cancer Res. Clin. Oncol. 2021, 148, 3039–3046. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with Chronic Gingivitis (n = 9891) | Patients without Chronic Gingivitis (n = 9891) | p-Value |
|---|---|---|---|
| Sex | |||
| Men | 4259 (43.1) | 4259 (43.1) | 1.000 |
| Women | 5632 (56.9) | 5632 (56.9) | |
| Age | |||
| Age in years (mean, standard deviation) | 41.6 (17.6) | 41.6 (17.6) | 1.000 |
| Age 18–40 years | 5325 (53.8) | 5325 (53.8) | 1.000 |
| Age 41–60 years | 2857 (28.9) | 2857 (28.9) | |
| Age >60 years | 1709 (17.3) | 1709 (17.3) | |
| Charlson Comorbidity Index (mean, standard deviation) | 0.4 (0.8) | 0.4 (0.8) | 1.000 |
| Population | Proportion in Patients with Chronic Gingivitis | Proportion in Patients without Chronic Gingivitis | Hazard Ratio (95% Confidence Interval) | p-Value |
|---|---|---|---|---|
| Overall | 6.1 | 4.6 | 1.36 (1.15–1.62) | <0.001 |
| Men | 6.0 | 4.1 | 1.46 (1.13–1.89) | 0.004 |
| Women | 6.2 | 5.0 | 1.29 (1.03–1.62) | 0.029 |
| Age 18–40 years | 1.1 | 0.9 | 1.51 (0.85–2.67) | 0.161 |
| Age 41–60 years | 8.4 | 4.4 | 1.74 (1.30–2.32) | <0.001 |
| Age >60 years | 18.2 | 16.6 | 1.19 (0.95–1.50) | 0.136 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beger-Luedde, J.; Loosen, S.H.; Luedde, T.; Roderburg, C.; Kostev, K. Association between Chronic Gingivitis and Cancer: A Retrospective Cohort Study of 19,782 Outpatients from the United Kingdom. Cancers 2023, 15, 2007. https://doi.org/10.3390/cancers15072007
Beger-Luedde J, Loosen SH, Luedde T, Roderburg C, Kostev K. Association between Chronic Gingivitis and Cancer: A Retrospective Cohort Study of 19,782 Outpatients from the United Kingdom. Cancers. 2023; 15(7):2007. https://doi.org/10.3390/cancers15072007
Chicago/Turabian StyleBeger-Luedde, Jane, Sven H. Loosen, Tom Luedde, Christoph Roderburg, and Karel Kostev. 2023. "Association between Chronic Gingivitis and Cancer: A Retrospective Cohort Study of 19,782 Outpatients from the United Kingdom" Cancers 15, no. 7: 2007. https://doi.org/10.3390/cancers15072007