

Radiation-Induced Retinopathy and Optic Neuropathy after Radiation Therapy for Brain, Head, and Neck Tumors: A Systematic Review

Abstract
:Simple Summary
Abstract
1. Introduction
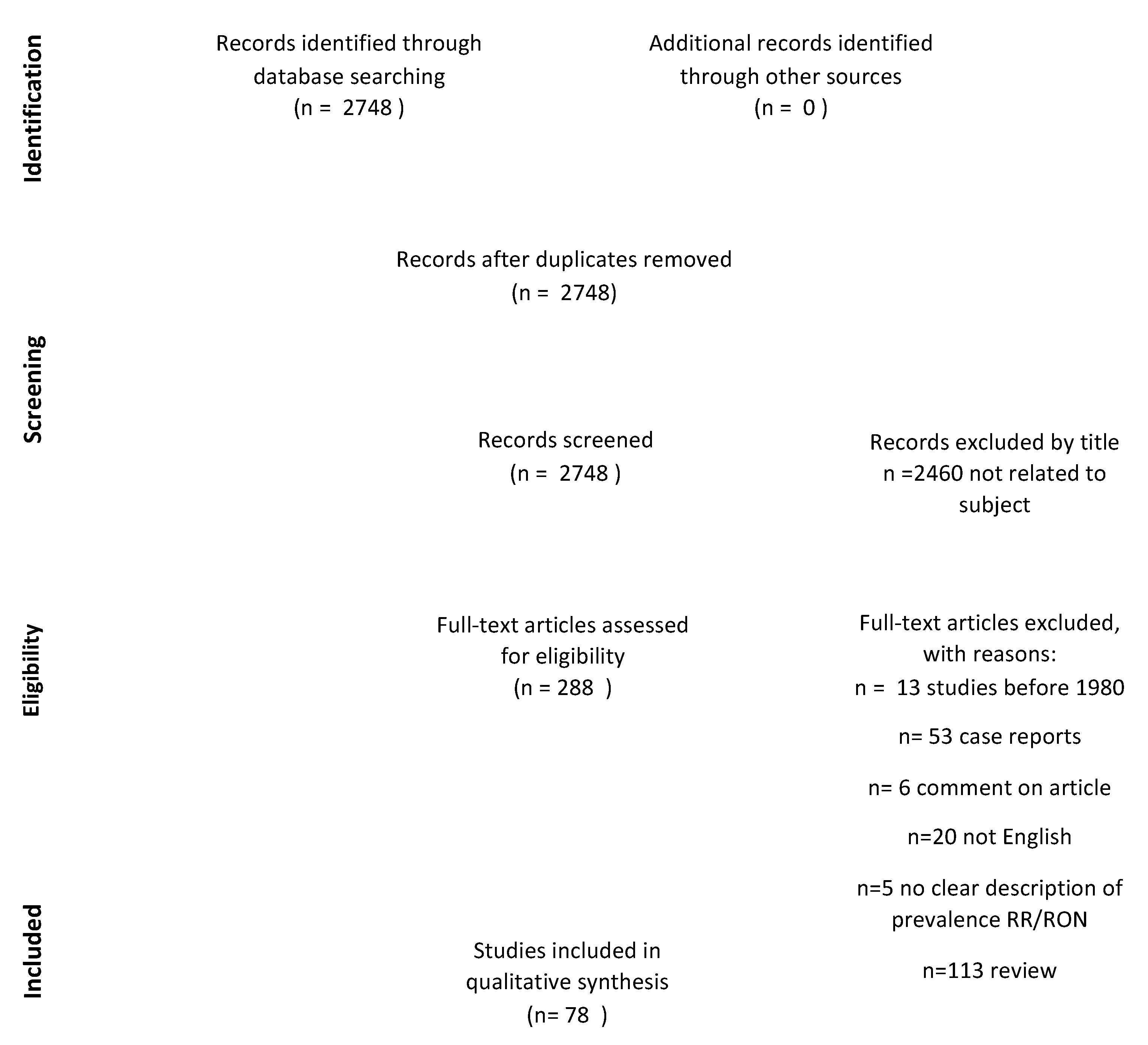
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection Process
2.3. Data Extraction
2.4. Outcome Definition
3. Results
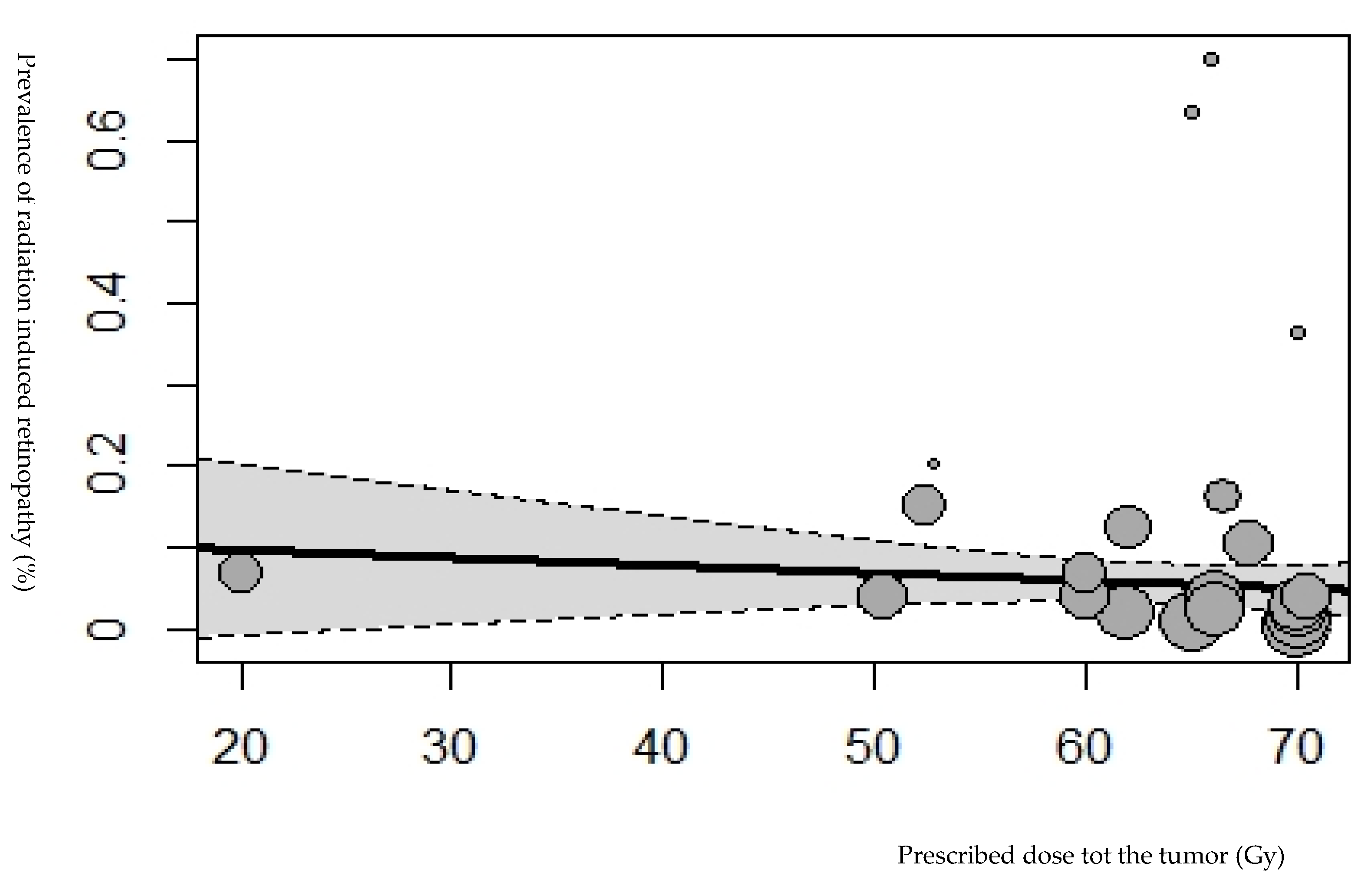
3.1. Retinopathy and Radiation Dose Parameters
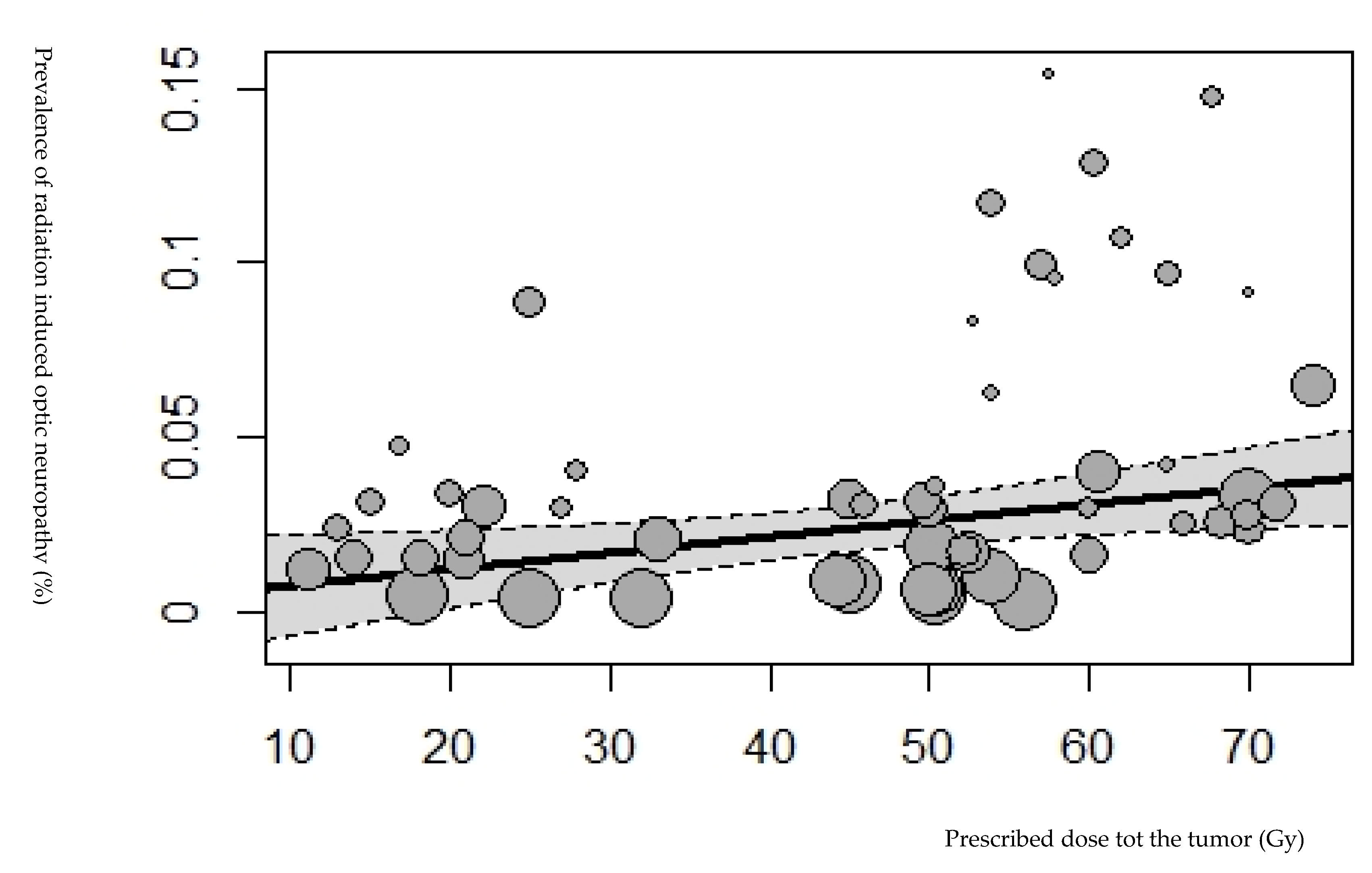
3.2. Optic Neuropathy and Radiation Dose Parameters
3.3. Data concerning Patients’ Characteristics and Prescribed Doses for the Retina, Optic Nerve, and Chiasm
4. Discussion
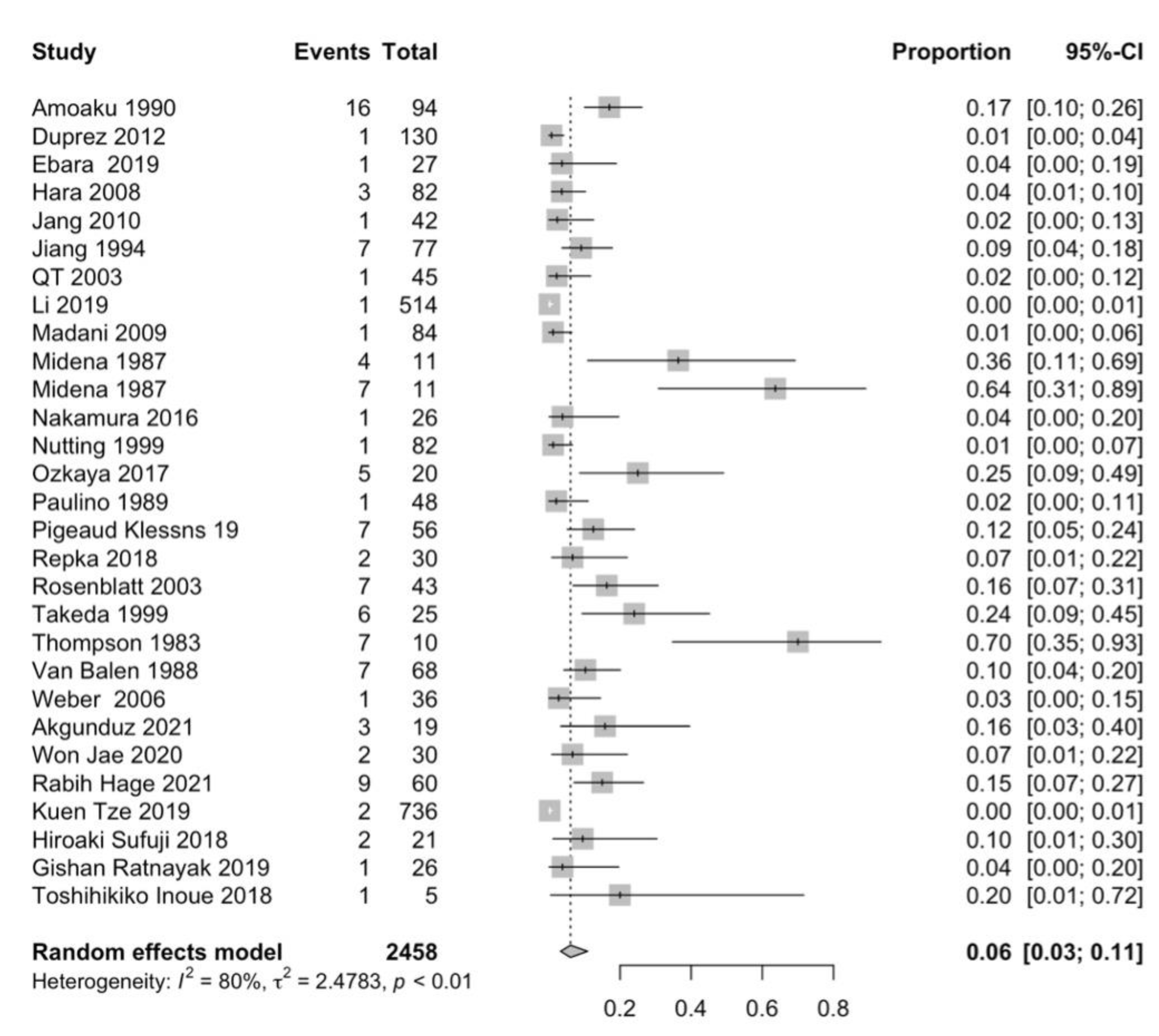
4.1. Prevalence of Retinopathy
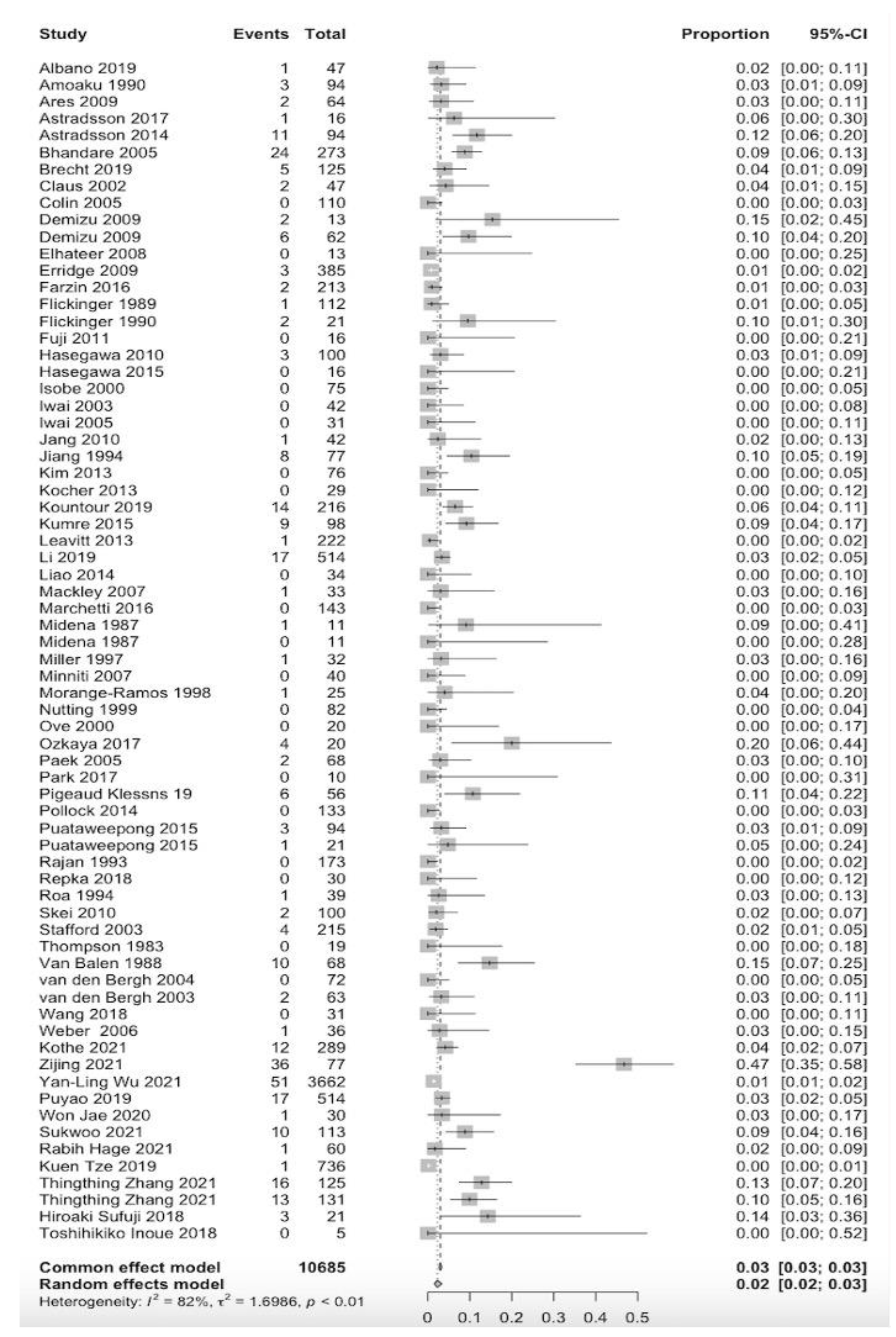
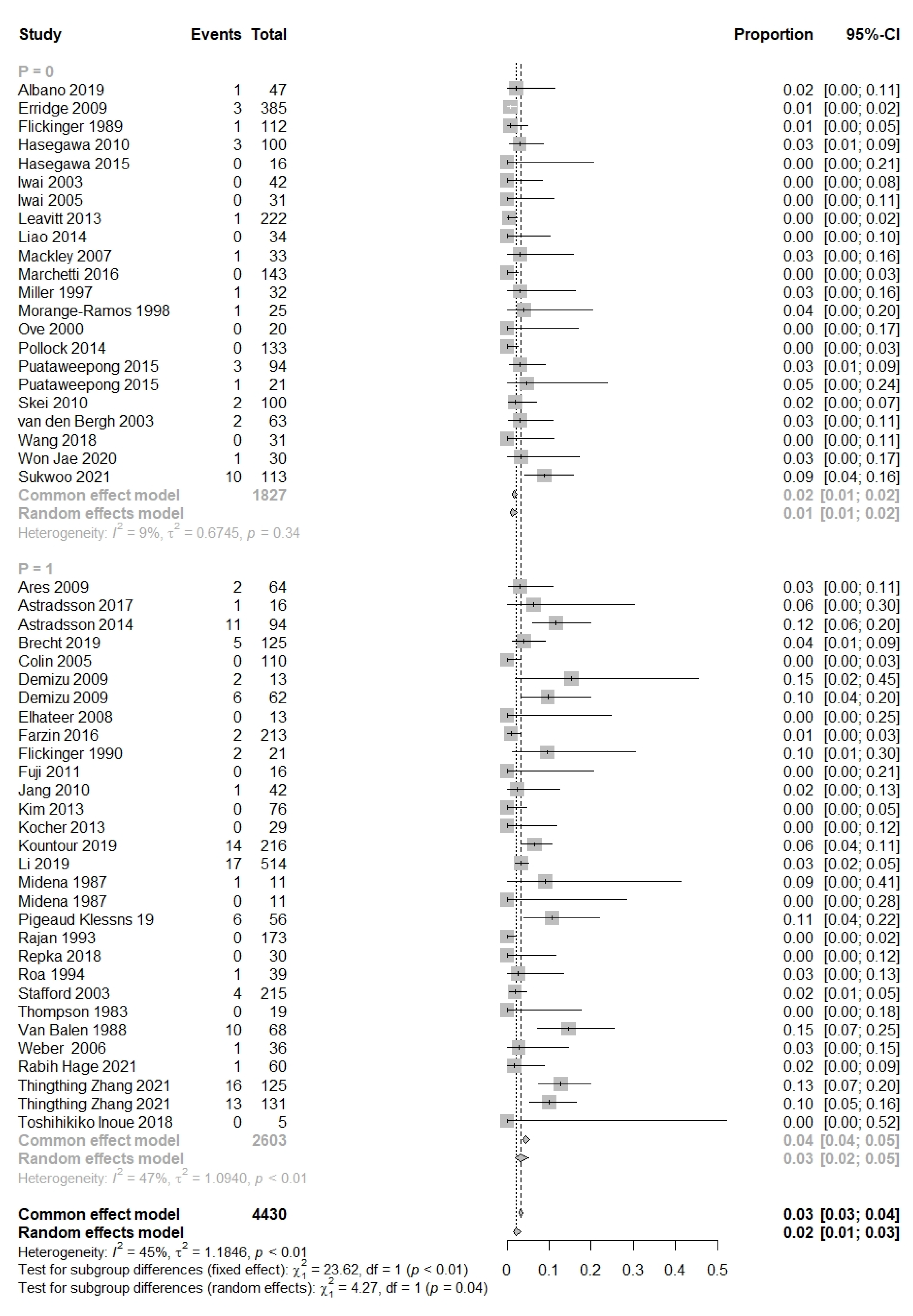
4.2. Prevalence of Optic Neuropathy
4.3. Limitations
4.4. Future Perspective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Jiang, G.L.; Tucker, S.L.; Guttenberger, R.; Peters, L.J.; Morrison, W.H.; Garden, A.S.; Ha, C.S.; Ang, K.K. Radiation-induced injury to the visual pathway. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 1994, 30, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Mayo, C.; Martel, M.K.; Marks, L.B.; Flickinger, J.; Nam, J.; Kirkpatrick, J. Radiation dose-volume effects of optic nerves and chiasm. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. S3), S28–S35. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.P.; Dewit, L.G.; van Herk, M.; Bartelink, H. Target volumes in radiotherapy for high-grade malignant glioma of the brain. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2000, 56, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.P.; Keus, R.B.; Hilgers, F.J.; Haas, R.L.; Tan, I.B.; Bartelink, H. Does the combination of radiotherapy and debulking surgery favor survival in paranasal sinus carcinoma? Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 27–35. [Google Scholar] [CrossRef]
- Reichstein, D. Current treatments and preventive strategies for radiation retinopathy. Curr. Opin. Ophthalmol. 2015, 26, 157–166. [Google Scholar] [CrossRef]
- Parsons, J.T.; Bova, F.J.; Fitzgerald, C.R.; Mendenhall, W.M.; Million, R.R. Radiation retinopathy after external-beam irradiation: Analysis of time-dose factors. Int. J. Radiat. Oncol. Biol. Phys. 1994, 30, 765–773. [Google Scholar] [CrossRef]
- Takeda, A.; Shigematsu, N.; Suzuki, S.; Fujii, M.; Kawata, T.; Kawaguchi, O.; Uno, T.; Takano, H.; Kubo, A.; Ito, H. Late retinal complications of radiation therapy for nasal and paranasal malignancies: Relationship between irradiated-dose area and severity. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 599–605. [Google Scholar] [CrossRef]
- Monroe, A.T.; Bhandare, N.; Morris, C.G.; Mendenhall, W.M. Preventing radiation retinopathy with hyperfractionation. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 856–864. [Google Scholar] [CrossRef]
- Langelaan, M.; de Boer, M.R.; van Nispen, R.M.; Wouters, B.; Moll, A.C.; van Rens, G.H. Impact of visual impairment on quality of life: A comparison with quality of life in the general population and with other chronic conditions. Ophthalmic Epidemiol. 2007, 14, 119–126. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Taphoorn, M.J.; Heimans, J.J.; Postma, T.J.; Gundy, C.M.; Beute, G.N.; Slotman, B.J.; Klein, M. Compromised health-related quality of life in patients with low-grade glioma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 4430–4435. [Google Scholar] [CrossRef]
- Taphoorn, M.J.; Schiphorst, A.K.; Snoek, F.J.; Lindeboom, J.; Wolbers, J.G.; Karim, A.B.; Huijgens, P.C.; Heimans, J.J. Cognitive functions and quality of life in patients with low-grade gliomas: The impact of radiotherapy. Ann. Neurol. 1994, 36, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Dhawahir-Scala, F.; Smith, A.; Young, L.; Charles, S. Radiation retinopathy: Case report and review. BMC Ophthalmol. 2007, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeganathan, V.S.; Wirth, A.; MacManus, M.P. Ocular risks from orbital and periorbital radiation therapy: A critical review. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Stallard, H.B. The Histological Appearances of an Eye Successfully Treated by Diathermy for Retinal Detachment. Fatal Termination from Pulmonary Thrombosis on the Nineteenth Day after Operation. Br. J. Ophthalmol. 1933, 17, 294–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Yang, H.; Guo, L.; Su, H.; Wei, S.; Zhang, X. Radiation-induced optic neuropathy following external beam radiation therapy for nasopharyngeal carcinoma: A retrospective case-control study. Mol. Clin. Oncol. 2016, 4, 868–872. [Google Scholar] [CrossRef] [Green Version]
- Hayreh, S.S. Blood supply of the optic nerve head and its role in optic atrophy, glaucoma, and oedema of the optic disc. Br. J. Ophthalmol. 1969, 53, 721–748. [Google Scholar] [CrossRef] [Green Version]
- Foulds, W.S. Visual disturbances in systemic disorders. Optic neuropathy and systemic disease. Trans. Ophthalmol. Soc. UK 1970, 89, 125–146. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Demizu, Y.; Murakami, M.; Miyawaki, D.; Niwa, Y.; Akagi, T.; Sasaki, R.; Terashima, K.; Suga, D.; Kamae, I.; Hishikawa, Y. Analysis of Vision loss caused by radiation-induced optic neuropathy after particle therapy for head-and-neck and skull-base tumors adjacent to optic nerves. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1487–1492. [Google Scholar] [CrossRef]
- Puataweepong, P.; Dhanachai, M.; Hansasuta, A.; Dangprasert, S.; Sitathanee, C.; Swangsilpa, T.; Vitoonpanich, P.; Yongvithisatid, P. Outcomes for Pituitary Adenoma Patients Treated with Linac—Based Stereotactic Radiosurgery and Radiotherapy: A Long Term Experience in Thailand. Asian Pac. J. Cancer Prev. APJCP 2015, 16, 5279–5284. [Google Scholar] [CrossRef] [Green Version]
- Midena, E.; Segato, T.; Piermarocchi, S.; Corti, L.; Zorat, P.L.; Moro, F. Retinopathy following radiation therapy of paranasal sinus and nasopharyngeal carcinoma. Retina 1987, 7, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xu, M.; Mi, J.; Yang, H.; Liu, Z.; Huang, L.; Hu, K.; Wang, R. Loosening Neuro-Optic Structures Dosimetric Constraints Provides High 5-Year Local Recurrence-Free Survival with Acceptable Toxicity in T4 Nasopharyngeal Carcinoma Patients Treated with Intensity-Modulated Radiotherapy. Front. Oncol. 2021, 11, 598320. [Google Scholar] [CrossRef] [PubMed]
- Duprez, F.; Madani, I.; Morbee, L.; Bonte, K.; Deron, P.; Domjan, V.; Boterberg, T.; De Gersem, W.; De Neve, W. IMRT for sinonasal tumors minimizes severe late ocular toxicity and preserves disease control and survival. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 252–259. [Google Scholar] [CrossRef]
- Hara, W.; Loo, B.W., Jr.; Goffinet, D.R.; Chang, S.D.; Adler, J.R.; Pinto, H.A.; Fee, W.E.; Kaplan, M.J.; Fischbein, N.J.; Le, Q.T. Excellent local control with stereotactic radiotherapy boost after external beam radiotherapy in patients with nasopharyngeal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Ebara, T.; Ando, K.; Eishima, J.; Suzuki, M.; Kawakami, T.; Horikoshi, H.; Tamaki, Y. Radiation with concomitant superselective intra-arterial cisplatin infusion for maxillary sinus squamous cell carcinoma. Jpn. J. Radiol. 2019, 37, 494–499. [Google Scholar] [CrossRef]
- Jang, N.Y.; Wu, H.G.; Park, C.I.; Heo, D.S.; Kim, D.W.; Lee, S.H.; Rhee, C.S. Definitive radiotherapy with or without chemotherapy for T3-4N0 squamous cell carcinoma of the maxillary sinus and nasal cavity. Jpn. J. Clin. Oncol. 2010, 40, 542–548. [Google Scholar] [CrossRef] [Green Version]
- Le, Q.T.; Tate, D.; Koong, A.; Gibbs, I.C.; Chang, S.D.; Adler, J.R.; Pinto, H.A.; Terris, D.J.; Fee, W.E.; Goffinet, D.R. Improved local control with stereotactic radiosurgical boost in patients with nasopharyngeal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 1046–1054. [Google Scholar] [CrossRef]
- Li, P.C.; Liebsch, N.J.; Niemierko, A.; Giantsoudi, D.; Lessell, S.; Fullerton, B.C.; Adams, J.; Shih, H.A. Radiation tolerance of the optic pathway in patients treated with proton and photon radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 131, 112–119. [Google Scholar] [CrossRef]
- Madani, I.; Bonte, K.; Vakaet, L.; Boterberg, T.; De Neve, W. Intensity-modulated radiotherapy for sinonasal tumors: Ghent University Hospital update. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 424–432. [Google Scholar] [CrossRef]
- Nakamura, T.; Azami, Y.; Ono, T.; Yamaguchi, H.; Hayashi, Y.; Suzuki, M.; Hatayama, Y.; Tsukiyama, I.; Hareyama, M.; Kikuchi, Y.; et al. Preliminary results of proton beam therapy combined with weekly cisplatin intra-arterial infusion via a superficial temporal artery for treatment of maxillary sinus carcinoma. Jpn. J. Clin. Oncol. 2016, 46, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Amoaku, W.M.; Archer, D.B. Cephalic radiation and retinal vasculopathy. Eye 1990, 4 Pt 1, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Nutting, C.; Brada, M.; Brazil, L.; Sibtain, A.; Saran, F.; Westbury, C.; Moore, A.; Thomas, D.G.; Traish, D.; Ashley, S. Radiotherapy in the treatment of benign meningioma of the skull base. J. Neurosurg. 1999, 90, 823–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozkaya Akagunduz, O.; Guven Yilmaz, S.; Yalman, D.; Yuce, B.; Demirkilinc Biler, E.; Afrashi, F.; Esassolak, M. Evaluation of the Radiation Dose-Volume Effects of Optic Nerves and Chiasm by Psychophysical, Electrophysiologic Tests, and Optical Coherence Tomography in Nasopharyngeal Carcinoma. Technol. Cancer Res. Treat. 2016, 16, 969–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulino, A.C.; Marks, J.E.; Bricker, P.; Melian, E.; Reddy, S.P.; Emami, B. Results of treatment of patients with maxillary sinus carcinoma. Cancer 1998, 83, 457–465. [Google Scholar] [CrossRef]
- Pigeaud-Klessens, M.L.; Kralendonk, J.H. Radiation retino- and opticopathy. A prospective study. Doc. Ophthalmol. Adv. Ophthalmol. 1992, 79, 285–291. [Google Scholar] [CrossRef]
- Repka, M.C.; Lei, S.; Campbell, L.; Suy, S.; Voyadzis, J.M.; Kalhorn, C.; McGrail, K.; Jean, W.; Subramaniam, D.S.; Lischalk, J.W.; et al. Long-Term Outcomes Following Conventionally Fractionated Stereotactic Boost for High-Grade Gliomas in Close Proximity to Critical Organs at Risk. Front. Oncol. 2018, 8, 373. [Google Scholar] [CrossRef]
- Rosenblatt, E.; Brook, O.R.; Erlich, N.; Miller, B.; Joachims, H.Z.; Kuten, A. Late visual and auditory toxicity of radiotherapy for nasopharyngeal carcinoma. Tumori 2003, 89, 68–74. [Google Scholar] [CrossRef]
- Thompson, G.M.; Migdal, C.S.; Whittle, R.J. Radiation retinopathy following treatment of posterior nasal space carcinoma. Br. J. Ophthalmol. 1983, 67, 609–614. [Google Scholar] [CrossRef] [Green Version]
- Van Balen, A.T.; Pigeaud-Klessens, M.L. Radiation-retino and opticopathy. Doc. Ophthalmol. Adv. Ophthalmol. 1988, 68, 239–245. [Google Scholar] [CrossRef]
- Weber, D.C.; Chan, A.W.; Lessell, S.; McIntyre, J.F.; Goldberg, S.I.; Bussiere, M.R.; Fitzek, M.M.; Thornton, A.F.; Delaney, T.F. Visual outcome of accelerated fractionated radiation for advanced sinonasal malignancies employing photons/protons. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2006, 81, 243–249. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Li, W.-F.; Yang, K.-B.; Chen, L.; Shi, J.-R.; Chen, F.-P.; Huang, X.-D.; Lin, L.; Zhang, X.-M.; Li, J. Long-Term Evaluation and Normal Tissue Complication Probability (NTCP) Models for Predicting Radiation-Induced Optic Neuropathy after Intensity-Modulated Radiation Therapy (IMRT) for Nasopharyngeal Carcinoma: A Large Retrospective Study in China. J. Oncol. 2022, 2022, 3647462. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Cho, K.R.; Choi, J.W.; Kong, D.S.; Seol, H.J.; Nam, D.H.; Kim, Y.D.; Woo, K.I.; Lee, J.I. Stereotactic radiosurgery for orbital cavernous venous malformation: A single center’s experience for 15 years. Acta Neurochir. 2021, 163, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Sato, K.; Kagawa, K.; Ichi, S. The long-term outcome of CyberKnife-based stereotactic radiotherapy for central skull base meningiomas: A single-center experience. Neurosurg. Rev. 2021, 44, 3519–3526. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Mimura, O.; Masai, N.; Ohashi, A.; Ikenaga, K.; Okuno, Y.; Nishiguchi, I.; Oh, R. Early intervention using high-precision radiotherapy preserved visual function for five consecutive patients with optic nerve sheath meningioma. Int. J. Clin. Oncol. 2018, 23, 826–834. [Google Scholar] [CrossRef] [Green Version]
- Hage, R.; Alapetite, C.; Brisse, H.; Zuber, K.; Lecler, A.; Lot, G.; Le Guerinel, C.; Vignal-Clermont, C.; Boissonnet, H. Efficacy and Safety of Proton Beam Therapy for Primary Optic Nerve Sheath Meningioma. Eye Brain 2021, 13, 219–229. [Google Scholar] [CrossRef]
- Ratnayake, G.; Oh, T.; Mehta, R.; Hardy, T.; Woodford, K.; Haward, R.; Ruben, J.D.; Dally, M.J. Long-term treatment outcomes of patients with primary optic nerve sheath meningioma treated with stereotactic radiotherapy. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2019, 68, 162–167. [Google Scholar] [CrossRef]
- Akagunduz, O.O.; Yilmaz, S.G.; Tavlayan, E.; Baris, M.E.; Afrashi, F.; Esassolak, M. Radiation-Induced Ocular Surface Disorders and Retinopathy: Ocular Structures and Radiation Dose-Volume Effect. Cancer Res. Treat. 2022, 54, 417–423. [Google Scholar] [CrossRef]
- Lin, K.T.; Lee, S.Y.; Liu, S.C.; Tsao, C.C.; Hsu, S.D.; Chien, W.C.; Chung, C.H.; Chang, W.K.; Chen, Y.W.; Lin, C.S. Risk of ocular complications following radiation therapy in patients with nasopharyngeal carcinoma. Laryngoscope 2019, 130, 1270–1277. [Google Scholar] [CrossRef]
- Suefuji, H.; Koto, M.; Demizu, Y.; Saitoh, J.I.; Shioyama, Y.; Tsuji, H.; Okimoto, T.; Ohno, T.; Nemoto, K.; Nakano, T.; et al. A Retrospective Multicenter Study of Carbon Ion Radiotherapy for Locally Advanced Olfactory Neuroblastomas. Anticancer. Res. 2018, 38, 1665–1670. [Google Scholar]
- Albano, L.; Losa, M.; Nadin, F.; Barzaghi, L.R.; Parisi, V.; Del Vecchio, A.; Bolognesi, A.; Mortini, P. Safety and efficacy of multisession gamma knife radiosurgery for residual or recurrent pituitary adenomas. Endocrine 2019, 64, 639–647. [Google Scholar] [CrossRef]
- Ares, C.; Hug, E.B.; Lomax, A.J.; Bolsi, A.; Timmermann, B.; Rutz, H.P.; Schuller, J.C.; Pedroni, E.; Goitein, G. Effectiveness and safety of spot scanning proton radiation therapy for chordomas and chondrosarcomas of the skull base: First long-term report. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Astradsson, A.; Munck Af Rosenschold, P.; Feldt-Rasmussen, U.; Poulsgaard, L.; Wiencke, A.K.; Ohlhues, L.; Engelholm, S.A.; Broholm, H.; Hansen Moller, E.; Klose, M.; et al. Visual outcome, endocrine function and tumor control after fractionated stereotactic radiation therapy of craniopharyngiomas in adults: Findings in a prospective cohort. Acta Oncol. 2017, 56, 415–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astradsson, A.; Wiencke, A.K.; Munck af Rosenschold, P.; Engelholm, S.A.; Ohlhues, L.; Roed, H.; Juhler, M. Visual outcome after fractionated stereotactic radiation therapy of benign anterior skull base tumors. J. Neuro Oncol. 2014, 118, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandare, N.; Monroe, A.T.; Morris, C.G.; Bhatti, M.T.; Mendenhall, W.M. Does altered fractionation influence the risk of radiation-induced optic neuropathy? Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1070–1077. [Google Scholar] [CrossRef]
- Brecht, S.; Boda-Heggemann, J.; Budjan, J.; Siebenlist, K.; Stieler, F.; Steil, V.; Wenz, F.; Lohr, F.; Buergy, D. Radiation-induced optic neuropathy after stereotactic and image guided intensity-modulated radiation therapy (IMRT). Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 134, 166–177. [Google Scholar] [CrossRef]
- Claus, F.; Boterberg, T.; Ost, P.; Huys, J.; Vermeersch, H.; Braems, S.; Bonte, K.; Moerman, M.; Verhoye, C.; De Neve, W. Postoperative radiotherapy for adenocarcinoma of the ethmoid sinuses: Treatment results for 47 patients. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 1089–1094. [Google Scholar] [CrossRef]
- Colin, P.; Jovenin, N.; Delemer, B.; Caron, J.; Grulet, H.; Hecart, A.C.; Lukas, C.; Bazin, A.; Bernard, M.H.; Scherpereel, B.; et al. Treatment of pituitary adenomas by fractionated stereotactic radiotherapy: A prospective study of 110 patients. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 333–341. [Google Scholar] [CrossRef]
- Elhateer, H.; Muanza, T.; Roberge, D.; Ruo, R.; Eldebawy, E.; Lambert, C.; Patrocinio, H.; Shenouda, G.; Souhami, L. Fractionated stereotactic radiotherapy in the treatment of pituitary macroadenomas. Curr. Oncol. 2008, 15, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Erridge, S.C.; Conkey, D.S.; Stockton, D.; Strachan, M.W.; Statham, P.F.; Whittle, I.R.; Grant, R.; Kerr, G.R.; Gregor, A. Radiotherapy for pituitary adenomas: Long-term efficacy and toxicity. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2009, 93, 597–601. [Google Scholar] [CrossRef]
- Farzin, M.; Molls, M.; Kampfer, S.; Astner, S.; Schneider, R.; Roth, K.; Dobrei, M.; Combs, S.; Straube, C. Optic toxicity in radiation treatment of meningioma: A retrospective study in 213 patients. J. Neuro Oncol. 2016, 127, 597–606. [Google Scholar] [CrossRef]
- Flickinger, J.C.; Lunsford, L.D.; Singer, J.; Cano, E.R.; Deutsch, M. Megavoltage external beam irradiation of craniopharyngiomas: Analysis of tumor control and morbidity. Int. J. Radiat. Oncol. Biol. Phys. 1990, 19, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Flickinger, J.C.; Nelson, P.B.; Martinez, A.J.; Deutsch, M.; Taylor, F. Radiotherapy of nonfunctional adenomas of the pituitary gland. Results with long-term follow-up. Cancer 1989, 63, 2409–2414. [Google Scholar] [CrossRef] [PubMed]
- Fuji, H.; Nakasu, Y.; Ishida, Y.; Horiguchi, S.; Mitsuya, K.; Kashiwagi, H.; Murayama, S. Feasibility of proton beam therapy for chordoma and chondrosarcoma of the skull base. Skull Base 2011, 21, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, T.; Kobayashi, T.; Kida, Y. Tolerance of the optic apparatus in single-fraction irradiation using stereotactic radiosurgery: Evaluation in 100 patients with craniopharyngioma. Neurosurgery 2010, 66, 688–694; discussion 694–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, T.; Shintai, K.; Kato, T.; Iizuka, H. Stereotactic Radiosurgery as the Initial Treatment for Patients with Nonfunctioning Pituitary Adenomas. World Neurosurg. 2015, 83, 1173–1179. [Google Scholar] [CrossRef]
- Isobe, K.; Ohta, M.; Yasuda, S.; Uno, T.; Hara, R.; Machida, N.; Saeki, N.; Yamaura, A.; Shigematsu, N.; Ito, H. Postoperative radiation therapy for pituitary adenoma. J. Neuro Oncol. 2000, 48, 135–140. [Google Scholar] [CrossRef]
- Iwai, Y.; Yamanaka, K.; Ishiguro, T. Gamma knife radiosurgery for the treatment of cavernous sinus meningiomas. Neurosurgery 2003, 52, 517–524; discussion 523–514. [Google Scholar] [CrossRef] [Green Version]
- Iwai, Y.; Yamanaka, K.; Yoshioka, K. Radiosurgery for nonfunctioning pituitary adenomas. Neurosurgery 2005, 56, 699–705; discussion 699–705. [Google Scholar] [CrossRef]
- Kim, J.O.; Ma, R.; Akagami, R.; McKenzie, M.; Johnson, M.; Gete, E.; Nichol, A. Long-term outcomes of fractionated stereotactic radiation therapy for pituitary adenomas at the BC Cancer Agency. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 528–533. [Google Scholar] [CrossRef]
- Kocher, M.; Treuer, H.; Hoevels, M.; Semrau, R.; Sturm, V.; Mueller, R.P. Endocrine and visual function after fractionated stereotactic radiotherapy of perioptic tumors. Strahlenther. Onkol. 2013, 189, 137–141. [Google Scholar] [CrossRef]
- Kountouri, M.; Pica, A.; Walser, M.; Albertini, F.; Bolsi, A.; Kliebsch, U.; Bachtiary, B.; Combescure, C.; Lomax, A.J.; Schneider, R.; et al. Radiation-induced optic neuropathy after pencil beam scanning proton therapy for skull-base and head and neck tumours. Br. J. Radiol. 2020, 93, 20190028. [Google Scholar] [CrossRef] [PubMed]
- Kumre, D.; Jeswani, V.; Benurwar, S.; Tumram, N.K. Role of total dose and hyperfractionation in reducing risk of radiation-induced optic neuropathy. Oman J. Ophthalmol. 2015, 8, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Leavitt, J.A.; Stafford, S.L.; Link, M.J.; Pollock, B.E. Long-term evaluation of radiation-induced optic neuropathy after single-fraction stereotactic radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 524–527. [Google Scholar] [CrossRef]
- Liao, H.I.; Wang, C.C.; Wei, K.C.; Chang, C.N.; Hsu, Y.H.; Lee, S.T.; Huang, Y.C.; Chen, H.C.; Hsu, P.W. Fractionated stereotactic radiosurgery using the Novalis system for the management of pituitary adenomas close to the optic apparatus. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2014, 21, 111–115. [Google Scholar] [CrossRef]
- Mackley, H.B.; Reddy, C.A.; Lee, S.Y.; Harnisch, G.A.; Mayberg, M.R.; Hamrahian, A.H.; Suh, J.H. Intensity-modulated radiotherapy for pituitary adenomas: The preliminary report of the Cleveland Clinic experience. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, M.; Bianchi, S.; Pinzi, V.; Tramacere, I.; Fumagalli, M.L.; Milanesi, I.M.; Ferroli, P.; Franzini, A.; Saini, M.; DiMeco, F.; et al. Multisession Radiosurgery for Sellar and Parasellar Benign Meningiomas: Long-term Tumor Growth Control and Visual Outcome. Neurosurgery 2016, 78, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.C.; Foote, R.L.; Coffey, R.J.; Gorman, D.A.; Earle, J.D.; Schomberg, P.J.; Kline, R.W. The role of stereotactic radiosurgery in the treatment of malignant skull base tumors. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 977–981. [Google Scholar] [CrossRef]
- Minniti, G.; Osti, M.; Jaffrain-Rea, M.L.; Esposito, V.; Cantore, G.; Maurizi Enrici, R. Long-term follow-up results of postoperative radiation therapy for Cushing’s disease. J. Neuro Oncol. 2007, 84, 79–84. [Google Scholar] [CrossRef]
- Morange-Ramos, I.; Regis, J.; Dufour, H.; Andrieu, J.M.; Grisoli, F.; Jaquet, P.; Peragut, J.C. Gamma-knife surgery for secreting pituitary adenomas. Acta Neurochir. 1998, 140, 437–443. [Google Scholar] [CrossRef]
- Ove, R.; Kelman, S.; Amin, P.P.; Chin, L.S. Preservation of visual fields after peri-sellar gamma-knife radiosurgery. Int. J. Cancer 2000, 90, 343–350. [Google Scholar] [CrossRef]
- Paek, S.H.; Downes, M.B.; Bednarz, G.; Keane, W.M.; Werner-Wasik, M.; Curran, W.J., Jr.; Andrews, D.W. Integration of surgery with fractionated stereotactic radiotherapy for treatment of nonfunctioning pituitary macroadenomas. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 795–808. [Google Scholar] [CrossRef]
- Park, S.; Yoon, S.M.; Lee, S.; Park, J.H.; Song, S.Y.; Lee, S.W.; Ahn, S.D.; Kim, J.H.; Choi, E.K. Role of fractionated radiotherapy in patients with hemangioma of the cavernous sinus. Radiat. Oncol. J. 2017, 35, 268–273. [Google Scholar] [CrossRef]
- Pollock, B.E.; Link, M.J.; Leavitt, J.A.; Stafford, S.L. Dose-volume analysis of radiation-induced optic neuropathy after single-fraction stereotactic radiosurgery. Neurosurgery 2014, 75, 456–460; discussion 460. [Google Scholar] [CrossRef] [PubMed]
- Rajan, B.; Ashley, S.; Gorman, C.; Jose, C.C.; Horwich, A.; Bloom, H.J.; Marsh, H.; Brada, M. Craniopharyngioma—A long-term results following limited surgery and radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 1993, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Roa, W.H.; Hazuka, M.B.; Sandler, H.M.; Martel, M.K.; Thornton, A.F.; Turrisi, A.T.; Urba, S.; Wolf, G.T.; Lichter, A.S. Results of primary and adjuvant CT-based 3-dimensional radiotherapy for malignant tumors of the paranasal sinuses. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Skeie, B.S.; Enger, P.O.; Skeie, G.O.; Thorsen, F.; Pedersen, P.H. Gamma knife surgery of meningiomas involving the cavernous sinus: Long-term follow-up of 100 patients. Neurosurgery 2010, 66, 661–668; discussion 668–669. [Google Scholar] [CrossRef]
- Stafford, S.L.; Pollock, B.E.; Leavitt, J.A.; Foote, R.L.; Brown, P.D.; Link, M.J.; Gorman, D.A.; Schomberg, P.J. A study on the radiation tolerance of the optic nerves and chiasm after stereotactic radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 1177–1181. [Google Scholar] [CrossRef]
- Van den Bergh, A.C.; Dullaart, R.P.; Hoving, M.A.; Links, T.P.; ter Weeme, C.A.; Szabo, B.G.; Pott, J.W. Radiation optic neuropathy after external beam radiation therapy for acromegaly. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2003, 68, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Van den Bergh, A.C.; Schoorl, M.A.; Dullaart, R.P.; van der Vliet, A.M.; Szabo, B.G.; ter Weeme, C.A.; Pott, J.W. Lack of radiation optic neuropathy in 72 patients treated for pituitary adenoma. J. Neuro Ophthalmol. Off. J. North Am. Neuro Ophthalmol. Soc. 2004, 24, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhu, H.; Knisely, J.; Mei, G.; Liu, X.; Dai, J.; Mao, Y.; Pan, L.; Qin, Z.; Wang, E. Hypofractionated stereotactic radiosurgery: A new treatment strategy for giant cavernous sinus hemangiomas. J. Neurosurg. 2018, 128, 60–67. [Google Scholar] [CrossRef]
- Köthe, A.; van Luijk, P.; Safai, S.; Kountouri, M.; Lomax, A.J.; Weber, D.C.; Fattori, G. Combining clinical and dosimetric features in a PBS proton therapy cohort to develop a NTCP model for radiation-induced optic neuropathy. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhan, Z.; Xiao, J.; Lan, Y. Radiation-Induced Optical Coherence Tomography Angiography Retinal Alterations in Patients with Nasopharyngeal Carcinoma. Front. Med. 2020, 7, 630880. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.C.; Schneider, R.; Goitein, G.; Koch, T.; Ares, C.; Geismar, J.H.; Schertler, A.; Bolsi, A.; Hug, E.B. Spot scanning-based proton therapy for intracranial meningioma: Long-term results from the Paul Scherrer Institute. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 865–871. [Google Scholar] [CrossRef]
- Noel, G.; Habrand, J.L.; Mammar, H.; Pontvert, D.; Haie-Meder, C.; Hasboun, D.; Moisson, P.; Ferrand, R.; Beaudre, A.; Boisserie, G.; et al. Combination of photon and proton radiation therapy for chordomas and chondrosarcomas of the skull base: The Centre de Protontherapie D’Orsay experience. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 392–398. [Google Scholar] [CrossRef]
- Weber, D.C.; Malyapa, R.; Albertini, F.; Bolsi, A.; Kliebsch, U.; Walser, M.; Pica, A.; Combescure, C.; Lomax, A.J.; Schneider, R. Long term outcomes of patients with skull-base low-grade chondrosarcoma and chordoma patients treated with pencil beam scanning proton therapy. Radiother. Oncol. 2016, 120, 169–174. [Google Scholar] [CrossRef]
- Ferguson, I.; Huang, J.Y.; Levi, L.; Van Stavern, G. Radiation Optic Neuropathy after Whole-Brain Radiation Therapy. J. Neuro Ophthalmol. 2019, 39, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, I.; Huecker, J.; Huang, J.; McClelland, C.; Van Stavern, G. Risk factors for radiation-induced optic neuropathy: A case-control study. Clin. Exp. Ophthalmol. 2017, 45, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drummond, J.B.; Ribeiro-Oliveira, A., Jr.; Soares, B.S. Non-Functioning Pituitary Adenomas. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Hofland, J., Dungan, K., et al., Eds.; Mdtext.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Kuehlewein, L.; An, L.; Durbin, M.K.; Sadda, S.R. Imaging areas of retinal nonperfusion in ischemic branch retinal vein occlusion with swept-source OCT microangiography. Ophthalmic Surg. Lasers Imaging Retin. 2015, 46, 249–252. [Google Scholar] [CrossRef]
- Kashani, A.H.; Chen, C.L.; Gahm, J.K.; Zheng, F.; Richter, G.M.; Rosenfeld, P.J.; Shi, Y.; Wang, R.K. Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications. Prog. Retin. Eye Res. 2017, 60, 66–100. [Google Scholar] [CrossRef]
- Kashani, A.H.; Lee, S.Y.; Moshfeghi, A.; Durbin, M.K.; Puliafito, C.A. Optical Coherence Tomography Angiography of Retinal Venous Occlusion. Retina 2015, 35, 2323–2331. [Google Scholar] [CrossRef]
- Green, K.M.; Toy, B.C.; Ashimatey, B.S.; Mustafi, D.; Jennelle, R.L.; Astrahan, M.A.; Chu, Z.; Wang, R.K.; Kim, J.; Berry, J.L.; et al. Quantifying Subclinical and Longitudinal Microvascular Changes Following Episcleral Plaque Brachytherapy Using Spectral Domain-Optical Coherence Tomography Angiography. J. Vitreoretin. Dis. 2020, 4, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.Y.; Chu, Z.; Shahidzadeh, A.; Wang, R.K.; Puliafito, C.A.; Kashani, A.H. Quantifying Microvascular Density and Morphology in Diabetic Retinopathy Using Spectral-Domain Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT362–OCT370. [Google Scholar] [CrossRef] [PubMed]
- Finger, P.T.; Kurli, M. Laser photocoagulation for radiation retinopathy after ophthalmic plaque radiation therapy. Br. J. Ophthalmol. 2005, 89, 730–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horgan, N.; Shields, C.L.; Mashayekhi, A.; Shields, J.A. Classification and treatment of radiation maculopathy. Curr. Opin. Ophthalmol. 2010, 21, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Veverka, K.K.; AbouChehade, J.E.; Iezzi, R., Jr.; Pulido, J.S. Noninvasive Grading of Radiation Retinopathy: The Use of Optical Coherence Tomography Angiography. Retina 2015, 35, 2400–2410. [Google Scholar] [CrossRef] [PubMed]
- McCannel, T.A.; Kim, E.; Kamrava, M.; Lamb, J.; Caprioli, J.; Yang, D.; McCannel, C.A. New Ultra-Wide-Field Angiographic Grading Scheme for Radiation Retinopathy after Iodine-125 Brachytherapy for Uveal Melanoma. Retina 2018, 38, 2415–2421. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.N.; Shi, A.; Wibbelsman, T.D.; Klufas, M.A. Ultra-widefield retinal imaging: An update on recent advances. Ther. Adv. Ophthalmol. 2020, 12, 2515841419899495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parrozzani, R.; Frizziero, L.; Londei, D.; Trainiti, S.; Modugno, R.L.; Leonardi, F.; Pulze, S.; Miglionico, G.; Pilotto, E.; Midena, E. Peripapillary vascular changes in radiation optic neuropathy: An optical coherence tomography angiography grading. Br. J. Ophthalmol. 2018, 102, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.O., 3rd; Albert, M.A., Jr.; Persaud, T.O.; Vail, R.S. Intravitreal bevacizumab treatment for radiation macular edema after plaque radiotherapy for choroidal melanoma. Retina 2007, 27, 903–907. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Muecke, J.S. Treatment of radiation maculopathy with intravitreal injection of bevacizumab (Avastin). Retina 2008, 28, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Gunther, J.B.; Altaweel, M.M. Bevacizumab (Avastin) for the treatment of ocular disease. Surv. Ophthalmol. 2009, 54, 372–400. [Google Scholar] [CrossRef] [PubMed]
- Finger, P.T.; Chin, K. Anti-vascular endothelial growth factor bevacizumab (Avastin) for radiation retinopathy. Arch. Ophthalmol. 2007, 125, 751–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finger, P.T. Radiation retinopathy is treatable with anti-vascular endothelial growth factor bevacizumab (Avastin). Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 974–977. [Google Scholar] [CrossRef]
- Chaudhuri, P.R.; Austin, D.J.; Rosenthal, A.R. Treatment of radiation retinopathy. Br. J. Ophthalmol. 1981, 65, 623–625. [Google Scholar] [CrossRef]
- Kinyoun, J.L.; Lawrence, B.S.; Barlow, W.E. Proliferative radiation retinopathy. Arch. Ophthalmol. 1996, 114, 1097–1100. [Google Scholar] [CrossRef]
- Kinyoun, J.L.; Chittum, M.E.; Wells, C.G. Photocoagulation treatment of radiation retinopathy. Am. J. Ophthalmol. 1988, 105, 470–478. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinaci-Tas, B.; Alderliesten, T.; Verbraak, F.D.; Rasch, C.R.N. Radiation-Induced Retinopathy and Optic Neuropathy after Radiation Therapy for Brain, Head, and Neck Tumors: A Systematic Review. Cancers 2023, 15, 1999. https://doi.org/10.3390/cancers15071999
Kinaci-Tas B, Alderliesten T, Verbraak FD, Rasch CRN. Radiation-Induced Retinopathy and Optic Neuropathy after Radiation Therapy for Brain, Head, and Neck Tumors: A Systematic Review. Cancers. 2023; 15(7):1999. https://doi.org/10.3390/cancers15071999
Chicago/Turabian StyleKinaci-Tas, Buket, Tanja Alderliesten, Frank D. Verbraak, and Coen R. N. Rasch. 2023. "Radiation-Induced Retinopathy and Optic Neuropathy after Radiation Therapy for Brain, Head, and Neck Tumors: A Systematic Review" Cancers 15, no. 7: 1999. https://doi.org/10.3390/cancers15071999