

Interleukin-8 and Interleukin-6 Are Biomarkers of Poor Prognosis in Esophageal Squamous Cell Carcinoma
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Human Samples
2.1.1. Patients and Healthy Volunteers
2.1.2. Blood Sample Collection and Analysis of Serum Cytokines
2.2. Animal Model
2.2.1. Cell Lines and Animals
2.2.2. Flow Cytometry Analysis
2.2.3. Real-Time RT-PCR
3. Statistical Analyses
4. Results
4.1. Characterization of the Study Population and Risk Factors to Develop Disease
4.2. Serum Cytokine Analysis Reveals a Subset of Cytokines Differentially Produced by ESCC Patients
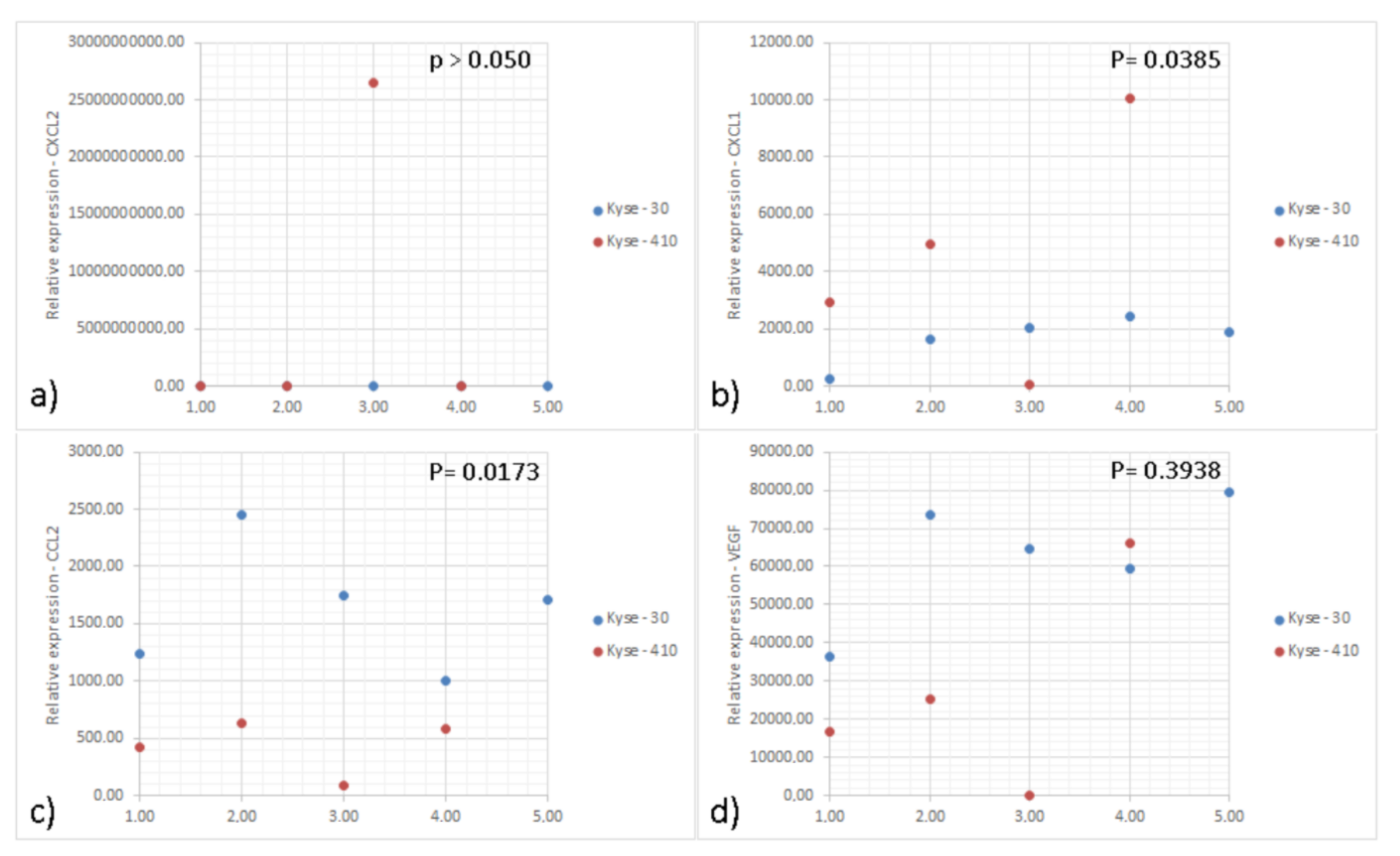
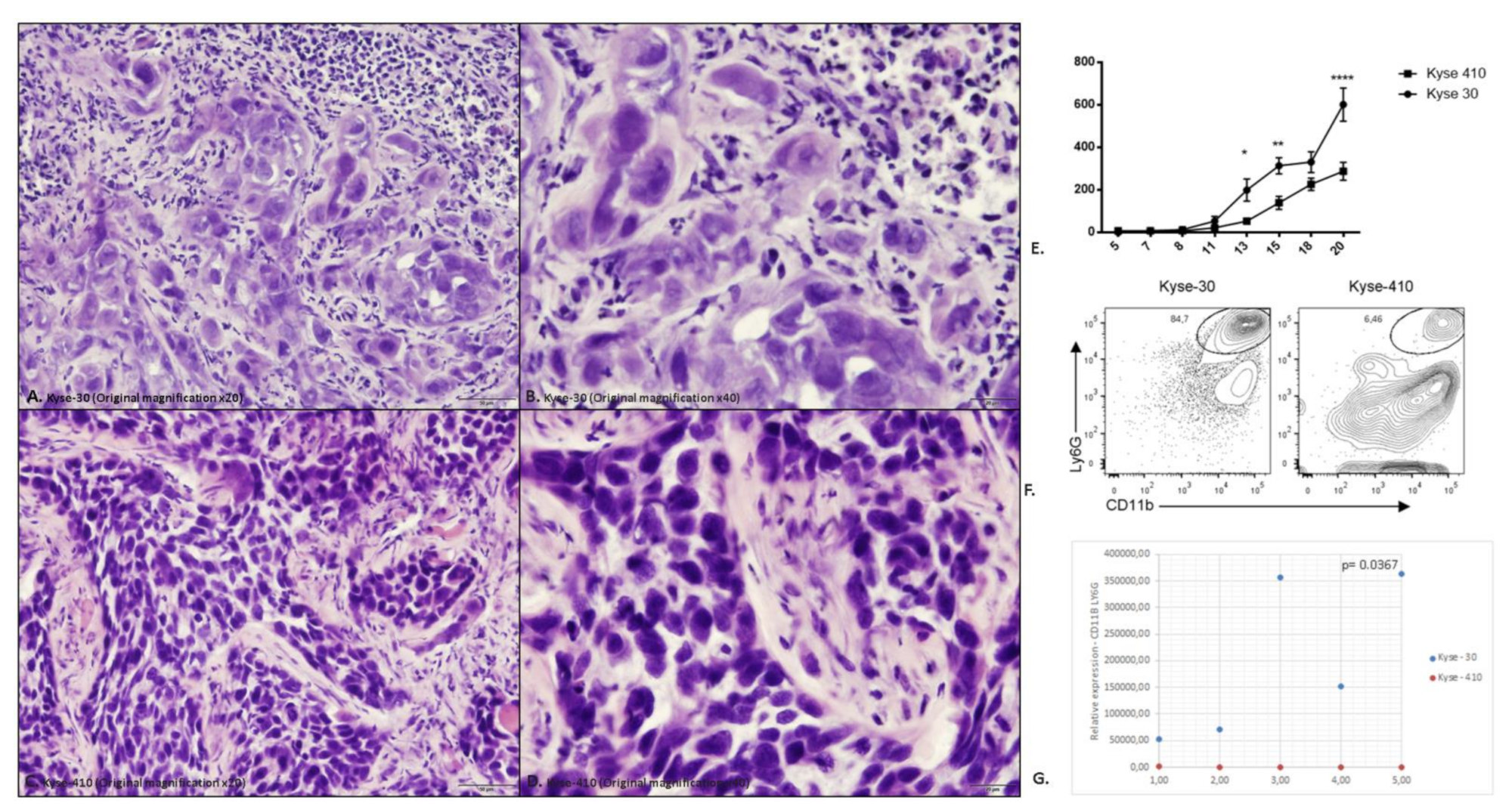
4.3. The Enhanced Growth of ESCC Cell Lines in Mice Associates with Increased Tumor Neutrophil Infiltration
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CBA | Cytometric Bead Array |
| ESCC | Esophageal squamous cell carcinoma |
| IL | Interleukin |
| TNF-α | Tumor necrosis factor-α |
| IFN- γ | Interferon gamma |
| SCC-Ag | Squamous cell cancer antigen |
| CEA | Carcinoembryonic antigen |
| CXCL-8 | C-X-C motif ligand 8 |
| CRP | C-reactive protein |
| ROC | Receiver operating characteristics |
| EDTA | Ethylenediamine tetraacetic acid |
| RH | Hospital record |
| RPMI | Serum-free medium |
| NSG | NOD SCID gamma |
| OR | Odds Ratio |
| SEM | Standard error of mean |
| CI | Confidence interval |
| IARC | International Agency for Research on Cancer |
| AUC | Area under the curve |
| HR | Hazard Ratio |
| Tregs | Regulatory T cells |
| MMP | Matrix metalloproteinases |
| VEGF | Vascular endothelial growth factor |
| EMT | Epithelialmesenchymal transition |
| TNM | Classification system for the anatomical extent of tumor cancers. T = tumor; N = lymph node; M = metastasis |
References
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of esophageal cancer: Update in global trends, etiology and risk factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Musa, I.H.; Musa, T.H.; Musa, H.H.; Ahmed, M.E. Esophageal cancer epidemiology, diagnosis, and management in Sudan—A review. Med. J. Malays. 2021, 76, 691–697. [Google Scholar]
- Pennathur, A.; Gibson, M.K.; Jobe, B.A.; Luketich, J.D. Oesophageal carcinoma. Lancet 2013, 381, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Rumgay, H.; Arnold, M.; Laversanne, M.; Whiteman, D.C.; Thrift, A.P.; Wei, W.; Lemmens, V.E.P.P.; Soerjomataram, I. International Trends in Esophageal Squamous Cell Carcinoma and Adenocarcinoma Incidence. Am. J. Gastroenterol. 2021, 116, 1072–1076. [Google Scholar] [CrossRef]
- Grille, V.J.; Campbell, S.; Gibbs, J.F.; Bauer, T.L. Esophageal cancer: The rise of adenocarcinoma over squamous cell carcinoma in the Asian belt. J. Gastrointest. Oncol. 2021, 12 (Suppl. S2), S339–S349. [Google Scholar] [CrossRef]
- GBD 2017 Oesophageal Cancer Collaborators. The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 582–597. [Google Scholar] [CrossRef]
- Lin, E.W.; Karakasheva, T.A.; Hicks, P.D.; Bass, A.J.; Rustgi, A.K. The tumor microenvironment in esophageal cancer. Oncogene 2016, 35, 5337–5349. [Google Scholar] [CrossRef]
- Bhat, A.A.; Nisar, S.; Maacha, S.; Carneiro-Lobo, T.C.; Akhtar, S.; Siveen, K.S.; Wani, N.A.; Rizwan, A.; Bagga, P.; Singh, M.; et al. Cytokine-chemokine network driven metastasis in esophageal cancer; promising avenue for targeted therapy. Mol. Cancer 2021, 20, 2. [Google Scholar] [CrossRef]
- Goto, M.; Liu, M. Chemokines and their receptors as biomarkers in esophageal cancer. Esophagus 2020, 17, 113–121. [Google Scholar] [CrossRef]
- Waters, J.K.; Reznik, S.I. Update on Management of Squamous Cell Esophageal Cancer. Curr. Oncol. Rep. 2022, 24, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Tang, H.; Fang, Y.; Tan, L.; Yin, J.; Shen, Y.; Zeng, Z.; Zhu, J.; Hou, Y.; Du, M.; et al. Morbidity and Mortality of Patients Who Underwent Minimally Invasive Esophagectomy After Neoadjuvant Chemoradiotherapy vs. Neoadjuvant Chemotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Randomized Clinical Trial. JAMA Surg. 2021, 156, 444–451. [Google Scholar] [CrossRef]
- Zhang, H.; Xia, J.; Wang, K.; Zhang, J. Serum autoantibodies in the early detection of esophageal cancer: A systematic review. Tumor Biol. 2015, 36, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewicz-Zając, M.; Pączek, S.; Muszyński, P.; Kozłowski, M.; Mroczko, B. Comparison between clinical significance of serum CXCL-8 and classical tumor markers in oesophageal cancer (OC) patients. Clin. Exp. Med. 2019, 19, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Tao, C.J.; Lin, G.; Xu, Y.P.; Mao, W.M. Predicting the Response of Neoadjuvant Therapy for Patients with Esophageal Carcinoma: An In-depth Literature Review. J. Cancer 2015, 6, 1179–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhu, Z.; Liu, Y.; Jin, X.; Xu, Z.; Yu, Q.; Li, K. Diagnostic value of multiple tumor markers for patients with esophageal carcinoma. PLoS ONE 2015, 10, e0116951. [Google Scholar] [CrossRef] [Green Version]
- Pastrez, P.R.A.; Mariano, V.S.; da Costa, A.M.; Silva, E.M.; Scapulatempo-Neto, C.; Guimaraes, D.P.; Fava, G.; Neto, S.A.Z.; Nunes, E.M.; Sichero, L.; et al. The Relation of HPV Infection and Expression of p53 and p16 Proteins in Esophageal Squamous Cells Carcinoma. J. Cancer 2017, 8, 1062–1070. [Google Scholar] [CrossRef] [Green Version]
- Da Costa, A.M.; Fregnani, J.; Pastrez, P.R.A.; Mariano, V.S.; Silva, E.M.; Neto, C.S.; Guimarães, D.P.; Villa, L.L.; Sichero, L.; Syrjanen, K.J.; et al. HPV infection and p53 and p16 expression in esophageal cancer: Are they prognostic factors? Infect. Agents Cancer 2017, 12, 54. [Google Scholar] [CrossRef]
- Tarnok, A.; Hambsch, J.; Chen, R.; Varro, R. Cytometric bead array to measure six cytokines in twenty-five microliters of serum. Clin. Chem. 2003, 49 Pt 1, 1000–1002. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.M.; Mariano, V.S.; Pastrez, P.R.A.; Pinto, M.C.; Castro, A.G.; Syrjanen, K.J.; Longatto-Filho, A. High systemic IL-6 is associated with worse prognosis in patients with non-small cell lung cancer. PLoS ONE 2017, 12, e0181125. [Google Scholar] [CrossRef] [Green Version]
- Kyse-30 Cell Line Description. Available online: https://www.culturecollections.org.uk/products/celllines/generalcell/detail.jsp?refId=94072011&collection=ecacc_gc (accessed on 9 October 2020).
- Kyse-410 Cell Line Description [09/10/2020]. Available online: https://www.sigmaaldrich.com/catalog/product/sigma/cb_94072023?lang=pt®ion=BR&gclid=CjwKCAjwnef6BRAgEiwAgv8mQQv8h8If4K4zvhNFBqEJH5Qt30G74-HEHow54IoM93MjDSJl2-imWxoC580QAvD_BwE (accessed on 9 October 2020).
- Barrios, E.S.M.; Musetti, C.; Forman, D. Etiology of Oesophageal Cancer (C15) in Central and South America; International Agency for Research on Cancer: Lyon, France, 2016; Available online: http://www-dep.iarc.fr/CSU_resources.htm (accessed on 9 October 2020).
- Brierley, J.G.M.; Wittekind, C. UICC TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Chichester, UK, 2017. [Google Scholar]
- Bilusic, M.; Heery, C.R.; Collins, J.M.; Donahue, R.N.; Palena, C.; Madan, R.A.; Karzai, F.; Marté, J.L.; Strauss, J.; Gatti-Mays, M.E.; et al. Phase I trial of HuMax-IL8 (BMS-986253), an anti-IL-8 monoclonal antibody, in patients with metastatic or unresectable solid tumors. J. Immunother. Cancer 2019, 7, 240. [Google Scholar] [CrossRef] [PubMed]
- Groblewska, M.; Mroczko, B.; Sosnowska, D.; Szmitkowski, M. Interleukin 6 and C-reactive protein in esophageal cancer. Clinica chimica acta. Int. J. Clin. Chem. 2012, 413, 1583–1590. [Google Scholar]
- Alfaro, C.; Sanmamed, M.F.; Rodriguez-Ruiz, M.E.; Teijeira, A.; Onate, C.; Gonzalez, A.; Ponz, M.; Schalper, K.A.; Pérez-Gracia, J.L.; Melero, I. Interleukin-8 in cancer pathogenesis, treatment and follow-up. Cancer Treat. Rev. 2017, 60, 24–31. [Google Scholar] [CrossRef]
- Bozic, C.R.; Gerard, N.P.; von Uexkull-Guldenband, C.; Kolakowski, L.F., Jr.; Conklyn, M.J.; Breslow, R.; Showell, H.J.; Gerard, C. The murine interleukin 8 type B receptor homologue and its ligands. Expression and biological characterization. J. Biol. Chem. 1994, 269, 29355–29358. [Google Scholar] [CrossRef]
- Lee, J.; Cacalano, G.; Camerato, T.; Toy, K.; Moore, M.W.; Wood, W.I. Chemokine binding and activities mediated by the mouse IL-8 receptor. J. Immunol. 1995, 155, 2158–2164. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.X.; Chen, Z.H.; Xu, Y.; Chen, J.W.; Weng, H.W.; Yun, M.; Zheng, Z.S.; Chen, C.; Wu, B.L.; Li, E.M.; et al. Downregulation of MicroRNA-644a Promotes Esophageal Squamous Cell Carcinoma Aggressiveness and Stem Cell-like Phenotype via Dysregulation of PITX2. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 298–310. [Google Scholar] [CrossRef] [Green Version]
- Graham, L.; Wikman, A. Toward improved survivorship: Supportive care needs of esophageal cancer patients, a literature review. Dis. Esophagus 2015, 29, 1081–1089. [Google Scholar] [CrossRef]
- Short, M.W.; Burgers, K.G.; Fry, V.T. Esophageal Cancer. Am. Fam. Physician 2017, 95, 22–28. [Google Scholar]
- Huang, F.L.; Yu, S.J. Esophageal cancer: Risk factors, genetic association, and treatment. Asian J. Surg. 2018, 41, 210–215. [Google Scholar] [CrossRef]
- Rustgi, A.K.; El-Serag, H.B. Esophageal carcinoma. N. Engl. J. Med. 2014, 371, 2499–2509. [Google Scholar] [CrossRef]
- Ogura, M.; Takeuchi, H.; Kawakubo, H.; Nishi, T.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Saikawa, Y.; Omori, T.; et al. Clinical significance of CXCL-8/CXCR-2 network in esophageal squamous cell carcinoma. Surgery 2013, 154, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Matusiewicz, M.; Diakowska, D.; Grabowski, K.; Blachut, K.; Konieczny, D.; Kustrzeba-Wojcicka, I.; Terlecki, G.; Banas, T. Elevation of circulating interleukin-8 is related to lymph node and distant metastases in esophageal squamous cell carcinomas--implication for clinical evaluation of cancer patient. Cytokine 2008, 41, 232–239. [Google Scholar] [CrossRef]
- Sethi, G.; Shanmugam, M.K.; Ramachandran, L.; Kumar, A.P.; Tergaonkar, V. Multifaceted link between cancer and inflammation. Biosci. Rep. 2012, 32, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazennec, G.; Richmond, A. Chemokines and chemokine receptors: New insights into cancer-related inflammation. Trends Mol. Med. 2010, 16, 133–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruizinga, R.C.; Bestebroer, J.; Berghuis, P.; de Haas, C.J.; Links, T.P.; de Vries, E.G.; Walenkamp, A.M. Role of chemokines and their receptors in cancer. Curr. Pharm. Des. 2009, 15, 3396–3416. [Google Scholar] [CrossRef]
- Konno, H.; Ohta, M.; Baba, M.; Suzuki, S.; Nakamura, S. The role of circulating IL-8 and VEGF protein in the progression of gastric cancer. Cancer Sci. 2003, 94, 735–740. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, T.; Matsushima, K.; Tanaka, S.; Robinson, E.A.; Appella, E.; Oppenheim, J.J.; Leonard, E.J. Purification of a human monocyte-derived neutrophil chemotactic factor that has peptide sequence similarity to other host defense cytokines. Proc. Natl. Acad. Sci. USA 1987, 84, 9233–9237. [Google Scholar] [CrossRef] [Green Version]
- Matsushima, K.; Morishita, K.; Yoshimura, T.; Lavu, S.; Kobayashi, Y.; Lew, W.; Appella, E.; Kung, H.F.; Leonard, E.J.; Oppenheim, J.J. Molecular cloning of a human monocyte-derived neutrophil chemotactic factor (MDNCF) and the induction of MDNCF mRNA by interleukin 1 and tumor necrosis factor. J. Exp. Med. 1988, 167, 1883–1893. [Google Scholar] [CrossRef] [Green Version]
- Fridlender, Z.G.; Albelda, S.M. Tumor-associated neutrophils: Friend or foe? Carcinogenesis 2012, 33, 949–955. [Google Scholar] [CrossRef] [Green Version]
- Nozawa, H.; Chiu, C.; Hanahan, D. Infiltrating neutrophils mediate the initial angiogenic switch in a mouse model of multistage carcinogenesis. Proc. Natl. Acad. Sci. USA 2006, 103, 12493–12498. [Google Scholar] [CrossRef] [Green Version]
- Hiramatsu, S.; Tanaka, H.; Nishimura, J.; Sakimura, C.; Tamura, T.; Toyokawa, T.; Muguruma, K.; Yashiro, M.; Hirakawa, K.; Ohira, M. Neutrophils in primary gastric tumors are correlated with neutrophil infiltration in tumor-draining lymph nodes and the systemic inflammatory response. BMC Immunol. 2018, 19, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dvorak, K.; Dvorak, B. Role of interleukin-6 in Barrett’s esophagus pathogenesis. World J. Gastroenterol. 2013, 19, 2307–2312. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.W.; Huang, P.M.; Yong, L.S.; Chang, Y.H.; Wu, C.W.; Hua, K.T.; Hsieh, M.S.; Lee, J.M. Circulating Interleukin-6 is Associated with Prognosis and Genetic Polymorphisms of MIR608 in Patients with Esophageal Squamous Cell Carcinoma. Ann. Surg. Oncol. 2018, 25, 2449–2456. [Google Scholar] [CrossRef]
- Tong, Q.; Wang, X.L.; Li, S.B.; Yang, G.L.; Jin, S.; Gao, Z.Y.; Liu, X.B. Combined detection of IL-6 and IL-8 is beneficial to the diagnosis of early stage esophageal squamous cell cancer: A preliminary study based on the screening of serum markers using protein chips. OncoTargets Ther. 2018, 11, 5777–5787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinocha, A.; Grover, R.K.; Deepak, R. Clinical significance of interleukin-6 in diagnosis of lung, oral, esophageal, and gall bladder carcinomas. J. Cancer Res. Ther. 2018, 14, S758–S760. [Google Scholar] [CrossRef]
- Nikiteas, N.I.; Tzanakis, N.; Gazouli, M.; Rallis, G.; Daniilidis, K.; Theodoropoulos, G.; Kostakis, A.; Peros, G. Serum IL-6, TNFalpha and CRP levels in Greek colorectal cancer patients: Prognostic implications. World J. Gastroenterol. 2005, 11, 1639–1643. [Google Scholar] [CrossRef]
- Yoneda, M.; Fujiwara, H.; Furutani, A.; Ikai, A.; Tada, H.; Shiozaki, A.; Komatsu, S.; Kubota, T.; Ichikawa, D.; Okamoto, K.; et al. Prognostic impact of tumor IL-6 expression after preoperative chemoradiotherapy in patients with advanced esophageal squamous cell carcinoma. Anticancer. Res. 2013, 33, 2699–2705. [Google Scholar]
- Shaul, M.E.; Fridlender, Z.G. Cancer-related circulating and tumor-associated neutrophils-subtypes, sources and function. FEBS J. 2018, 285, 4316–4342. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable/Category | N Cases (N Events) | OR (CI95%) | p |
|---|---|---|---|
| Alcohol | |||
| Never | 15 (3) | 1 | - |
| Yes, currently (if it was stopped in the last 12 months) | 85 (36) | 3.9 (0.4–35.9) | 0.227 |
| Yes, in the past | 40 (31) | 14.5 (1.3–163.6) | 0.030 |
| Tobacco | |||
| Never | 47 (10) | 1 | - |
| Yes, currently (if it was stopped in the last 12 months) | 58 (47) | 11.3 (2.9–44.3) | <0.001 |
| Yes, in the past | 35 (13) | 1.5 (0.3–6.6) | 0.581 |
| Exposure to pesticide or insecticide | |||
| No | 78 (28) | 1 | - |
| Yes | 60 (42) | 3.2 (1.1–9.4) | 0.033 |
| IL-8 | 140 (70) | 1.6 (1.3–2.0) | <0.001 |
| Cytokines | Groups | ||||
|---|---|---|---|---|---|
| Case | Control | p | |||
| Mean (SD) pg/mL | Median (Min–Max) pg/mL | Mean (SD) pg/mL | Median (Min–Max) pg/mL | ||
| IL-12p70 | 0.78 (0.99) | 0.39 (0.00–4.83) | 0.93 (1.61) | 0.28 (0.00–11.51) | 0.991 |
| TNF-α | 0.95 (2.24) | 0.05 (0.00–16.37) | 0.86 (2.14) | 0.05 (0.00–14.27) | 0.772 |
| IL-10 | 12.98 (97.53) | 0.68 (0.00–816.59) | 0.55 (0.78) | 0.42 (0.00–5.73) | 0.027 |
| IL-6 | 1157.20 (9614.02) | 6.72 (0.21–80446.68) | 2.07 (2.49) | 1.62 (0.00–18.18) | <0.001 |
| IL-1β | 1.21 (3.07) | 0.49 (0.00–24.60) | 0.66 (1.87) | 0.00 (0.00–13.76) | 0.032 |
| IL-8 | 196.31 (1529.42) | 7.51 (2.40–12806.73) | 3.52 (3.05) | 3.16 (0.64–25.59) | <0.001 |
| Total | 70 | 70 | |||
| Variable/Category | n Cases (n Events) | % Probability of Survival | p | ||
|---|---|---|---|---|---|
| 12 Months | 36 Months | 60 Months | |||
| Overall survival | 70 (52) | 60.8 | 36.0 | 21.5 | - |
| Sex | |||||
| Female | 11 (7) | 60.0 | 50.0 | 18.8 | 0.403 |
| Male | 59 (45) | 60.7 | 33.2 | 21.1 | |
| Race | |||||
| White | 50 (38) | 64.0 | 35.1 | 23.6 | 0.208 |
| Non-white | 18 (14) | 48.1 | 34.4 | 0.00 | |
| Exposure to pesticide or insecticide | |||||
| No | 28 (21) | 64.3 | 46.4 | 26.7 | 0.360 |
| Yes | 42 (31) | 58.6 | 28.0 | 17.4 | |
| Place residence | |||||
| Urban area only | 12 (8) | 66.7 | 41.7 | 41.7 | 0.553 |
| Rural area only | 8 (7) | 62.5 | 25.0 | 12.5 | |
| Both areas | 50 (37) | 59.1 | 36.5 | 17.7 | |
| Alcohol | |||||
| Never/In the past | 34 (26) | 58.0 | 36.7 | 17.8 | 0.839 |
| Yes, currently (if it was stopped in the last 12 months) | 36 (26) | 63.5 | 35.1 | 24.6 | |
| Tobacco | |||||
| Never | 10 (8) | 30.0 | 20.0 | 20.0 | 0.315 |
| Yes, currently (if it was stopped in the last 12 months) | 47 (35) | 60.8 | 39.1 | 20.3 | |
| Yes, in the past | 13 (9) | 84.6 | 38.5 | 28.8 | |
| Degree of differentiation | |||||
| Well-differentiated | 9 (7) | 55.6 | 22.2 | 22.2 | 0.807 |
| Moderately differentiated | 35 (26) | 56.4 | 37.6 | 23.9 | |
| Little-differentiated | 21 (16) | 66.0 | 30.5 | 16.9 | |
| TNF-α | |||||
| <0.825 | 48 (39) | 58.3 | 25.9 | 18.9 | 0.100 |
| ≥0.825 | 22 (13) | 66.7 | 61.2 | 28.5 | |
| IL-10 | |||||
| <1.34 | 50 (38) | 59.1 | 29.6 | 22.0 | 0.470 |
| ≥1.34 | 20 (14) | 65.0 | 53.2 | 19.7 | |
| IL-6 | |||||
| <4.7 | 27 (14) | 80.4 | 64.3 | 45.1 | <0.001 |
| ≥4.7 | 43 (38) | 48.8 | 18.2 | 6.9 | |
| IL-1β | |||||
| <1.35 | 52 (40) | 62.6 | 29.2 | 19.6 | 0.364 |
| ≥1.35 | 18 (12) | 55.6 | 55.6 | 28.8 | |
| IL-8 | |||||
| <6.75 | 29 (16) | 89.1 | 50.4 | 41.2 | 0.001 |
| ≥6.75 | 41 (36) | 41.5 | 25.9 | 9.3 | |
| Surgery | |||||
| No | 44 (40) | 47.1 | 16.5 | 8.2 | <0.001 |
| Yes | 20 (9) | 90.0 | 80.0 | 51.3 | |
| Radiotherapy | |||||
| No | 25 (22) | 56.0 | 28.0 | 7.0 | 0.117 |
| Yes | 43 (29) | 61.8 | 41.2 | 29.7 | |
| Chemotherapy | |||||
| No | 24 (20) | 41.7 | 33.3 | 15.6 | 0.186 |
| Yes | 45 (32) | 70.3 | 36.3 | 24.6 | |
| TNM | |||||
| I/II | 17 (8) | 87.8 | 81.6 | 49.8 | <0.001 |
| III/IV | 42 (38) | 52.4 | 16.7 | 9.5 | |
| Topography of the tumor | |||||
| Upper/Middle third | 33 (27) | 69.7 | 42.4 | 20.5 | 0.447 |
| SOE | 19 (14) | 51.3 | 22.8 | 22.8 | |
| Variable/Category | n Cases (n Events) | HR (IC95%) | p |
|---|---|---|---|
| Race | |||
| White | 43 (34) | - | - |
| Non-white | 13 (11) | 5.99 (2.28–15.72) | <0.001 |
| IL-12p70 | |||
| <1.23 | 40 (33) | - | - |
| ≥1.23 | 16 (12) | 0.33 (0.15–0.73) | 0.007 |
| TNF-α | |||
| <0.825 | 41 (36) | - | - |
| ≥0.825 | 15 (9) | 0.23 (0.09–0.59) | 0.003 |
| IL-8 | |||
| <6.75 | 22 (14) | - | - |
| ≥6.75 | 34 (31) | 4.56 (2.21–9.41) | 0.002 |
| Surgery | |||
| No | 40 (37) | - | - |
| Yes | 16 (8) | 0.21 (0.08–0.55) | 0.002 |
| Radiotherapy | |||
| No | 25 (22) | - | |
| Yes | 31 (23) | 0.27 (0.14–0.54) | <0.001 |
| TNM | |||
| I/II | 16 (8) | - | |
| III/IV | 40 (37) | 3.68 (1.45–9.37) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pastrez, P.R.A.; Barbosa, A.M.; Mariano, V.S.; Causin, R.L.; Castro, A.G.; Torrado, E.; Longatto-Filho, A. Interleukin-8 and Interleukin-6 Are Biomarkers of Poor Prognosis in Esophageal Squamous Cell Carcinoma. Cancers 2023, 15, 1997. https://doi.org/10.3390/cancers15071997
Pastrez PRA, Barbosa AM, Mariano VS, Causin RL, Castro AG, Torrado E, Longatto-Filho A. Interleukin-8 and Interleukin-6 Are Biomarkers of Poor Prognosis in Esophageal Squamous Cell Carcinoma. Cancers. 2023; 15(7):1997. https://doi.org/10.3390/cancers15071997
Chicago/Turabian StylePastrez, Paula Roberta Aguiar, Ana Margarida Barbosa, Vânia Sammartino Mariano, Rhafaela Lima Causin, Antonio Gil Castro, Egídio Torrado, and Adhemar Longatto-Filho. 2023. "Interleukin-8 and Interleukin-6 Are Biomarkers of Poor Prognosis in Esophageal Squamous Cell Carcinoma" Cancers 15, no. 7: 1997. https://doi.org/10.3390/cancers15071997