
Rural–Urban Disparities in Patient Care Experiences among Prostate Cancer Survivors: A SEER-CAHPS Study

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Dataset
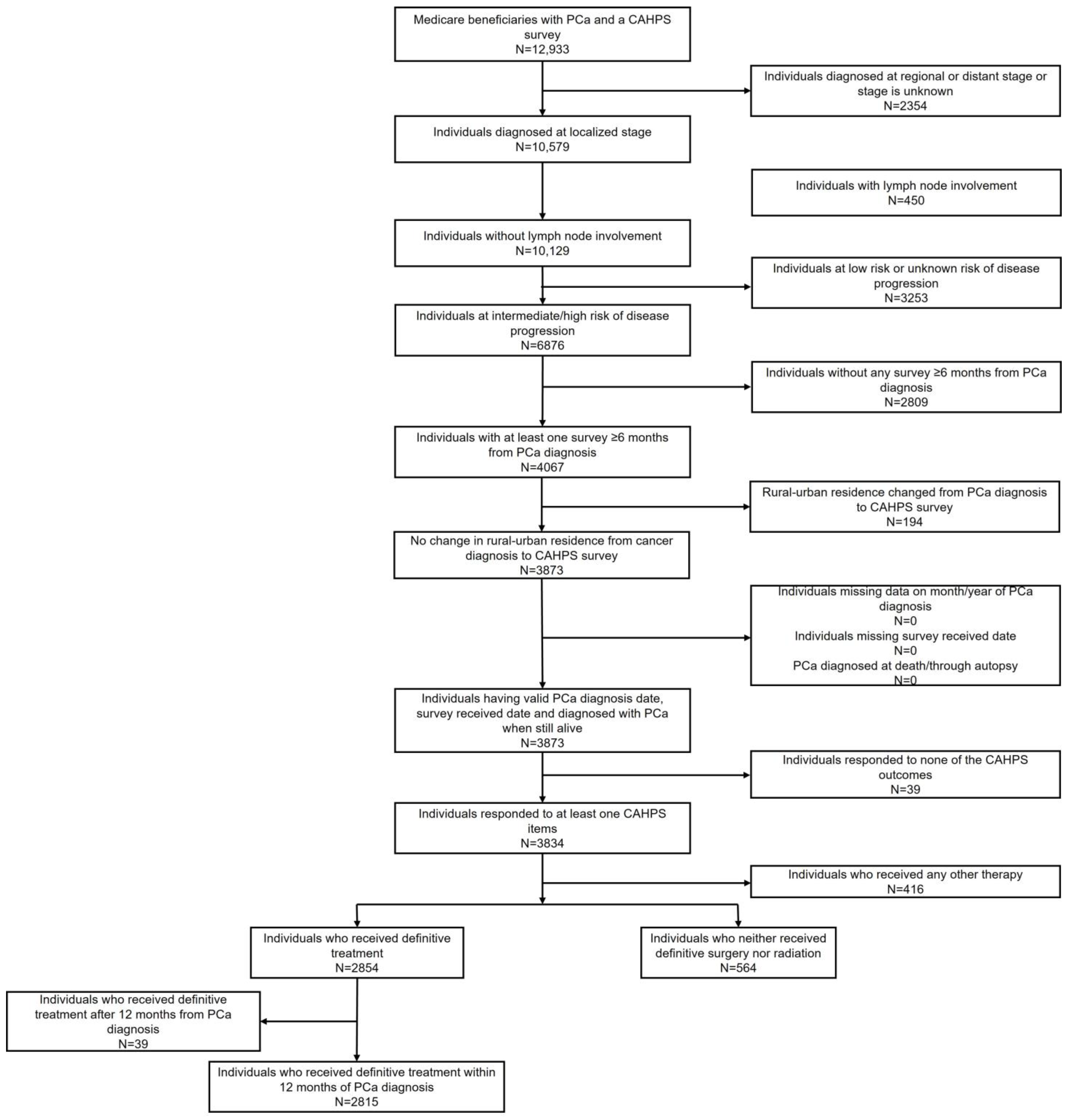
2.2. Study Population
2.3. Outcome Variables
2.4. Exposure Variables
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Study Cohort and Demographics
3.2. Regression Analyses
3.3. Startified Analyses by Treatment Status
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schmid, M.; Meyer, C.P.; Reznor, G.; Choueiri, T.K.; Hanske, J.; Sammon, J.D.; Abdollah, F.; Chun, F.K.H.; Kibel, A.S.; Tucker-Seeley, R.D.; et al. Racial Differences in the Surgical Care of Medicare Beneficiaries with Localized Prostate Cancer. JAMA Oncol. 2016, 2, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Arcaniolo, D.; Napolitano, L.; Barone, B.; La Rocca, R.; Capece, M.; Caputo, V.F.; Imbimbo, C.; De Sio, M.; Calace, F.P. Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 8500. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Barone, B.; Caputo, V.F.; Fontana, M.; de Cobelli, O.; Ferro, M. BRCA Germline Mutations in Prostate Cancer: The Future Is Tailored. Diagnostics 2021, 11, 908. [Google Scholar] [CrossRef]
- Surveillance Epidemiology and End Results (SEER). Prostate Cancer—Cancer Stat Facts. 2021. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 16 September 2021).
- Weiner, A.B.; Matulewicz, R.S.; Eggener, S.E.; Schaeffer, E.M. Increasing incidence of metastatic prostate cancer in the United States (2004–2013). Prostate Cancer Prostatic Dis. 2016, 19, 395–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Urological Association (AUA); American Society for Radiation Oncology (ASTRO); Society of Urologic Oncology (SUO); American Urological Association. Prostate Cancer: Clinically Localized Guideline—American Urological Association. 2017. Available online: https://www.auanet.org/guidelines/guidelines/prostate-cancer-clinically-localized-guideline (accessed on 2 September 2021).
- Maganty, A.; Sabik, L.M.; Sun, Z.J.; Eom, K.Y.; Li, J.; Davies, B.J.; Jacobs, B.L. Undertreatment of Prostate Cancer in Rural Locations. J. Urol. 2020, 203, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Andkhoie, M.; Szafron, M. The Impact of Geographic Location on Saskatchewan Prostate Cancer Patient Treatment Choices: A Multilevel and Spatial Analysis. J. Rural Health 2020, 36, 564–576. [Google Scholar] [CrossRef]
- Baldwin, L.M.; Andrilla, C.H.A.; Porter, M.P.; Rosenblatt, R.A.; Patel, S.; Doescher, M.P. Treatment of early-stage prostate cancer among rural and urban patients. Cancer 2013, 119, 3067–3075. [Google Scholar] [CrossRef]
- Meilleur, A.; Subramanian, S.V.; Plascak, J.J.; Fisher, J.L.; Paskett, E.D.; Lamont, E.B. Rural residence and cancer outcomes in the United States: Issues and challenges. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1657–1667. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.J.; Ndoye, M.; Fergus, K.B.; Lindsey, J.; Butler, C.; Patino, G.; Anger, J.T.; Breyer, B.N. Forecasting Limited Access to Urology in Rural Communities: Analysis of the American Urological Association Census. J. Rural Health 2020, 36, 300–306. [Google Scholar] [CrossRef]
- Quinn, T.P.; Sanda, M.G.; Howard, D.H.; Patil, D.; Filson, C.P. Disparities in magnetic resonance imaging of the prostate for traditionally underserved patients with prostate cancer. Cancer 2021, 127, 2974–2979. [Google Scholar] [CrossRef]
- Kaufman, B.G.; Thomas, S.R.; Randolph, R.K.; Perry, J.R.; Thompson, K.W.; Holmes, G.M.; Pink, G.H. The Rising Rate of Rural Hospital Closures. J. Rural Health 2016, 32, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, R.S.; Neuwahl, S.; Nielsen, M.E.; Fraher, E. Recent Trends in the Urology Workforce in the United States. Urology 2013, 82, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, P.; Baade, P.D.; Aitken, J.F.; Ralph, N.; Chambers, S.K.; Dunn, J. Geographical Variations in Prostate Cancer Outcomes: A Systematic Review of International Evidence. Front Oncol. 2019, 9, 238. [Google Scholar] [CrossRef] [Green Version]
- Frye, T.P.; Sadowski, D.J.; Zahnd, W.E.; Jenkins, W.D.; Dynda, D.I.; Mueller, G.S.; Alanee, S.R.; McVary, K.T. Impact of county rurality and urologist density on urological cancer mortality in Illinois. J. Urol. 2015, 193, 1608–1614. [Google Scholar] [CrossRef] [PubMed]
- Stolzenbach, L.F.; Deuker, M.; Collà-Ruvolo, C.; Nocera, L.; Tian, Z.; Maurer, T.; Tilki, D.; Briganti, A.; Saad, F.; Mirone, V.; et al. Differences between rural and urban prostate cancer patients. World J. Urol. 2021, 39, 2507–2514. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. What Is Patient Experience? 2017. Available online: https://www.ahrq.gov/cahps/about-cahps/patient-experience/index.html (accessed on 13 January 2020).
- Chawla, N.; Urato, M.; Ambs, A.; Chawla, N.; Urato, M.; Ambs, A.; Schussler, N.; Hays, R.D.; Clauser, S.B.; Zaslavsky, A.M.; et al. Unveiling SEER-CAHPS®®: A New Data Resource for Quality of Care Research. J. Gen. Intern. Med. 2015, 30, 641–650. [Google Scholar] [CrossRef]
- National Cancer Institute. Overview of the SEER Program. Available online: https://seer.cancer.gov/about/overview.html (accessed on 24 March 2022).
- National Cancer Institute. CAHPS Data Documentation. Available online: https://healthcaredelivery.cancer.gov/seer-cahps/aboutdata/documentation.html (accessed on 19 March 2023).
- United States Department of Agriculture Economic Research Service. Rural-Urban Continuum Codes. 2020. Available online: https://www.ers.usda.gov/data-products/rural-urban-continuum-codes.aspx (accessed on 28 January 2022).
- National Comprehensive Cancer Network (NCCN). Prostate Cancer Early Stage. 2020. Available online: https://www.nccn.org/patients/guidelines/content/PDF/prostate-early-patient.pdf (accessed on 15 September 2021).
- Jang, J.W.; Drumm, M.R.; Efstathiou, J.A.; Jang, J.W.; Drumm, M.R.; Efstathiou, J.A.; Paly, J.J.; Niemierko, A.; Ancukiewicz, M.; Talcott, J.A.; et al. Long-term quality of life after definitive treatment for prostate cancer: Patient-reported outcomes in the second posttreatment decade. Cancer Med. 2017, 6, 1827. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute. SEER-CAHPS Analytic Guidance. 2020. Available online: https://healthcaredelivery.cancer.gov/seer-cahps/researchers/approaches_guidance.html (accessed on 15 February 2020).
- Quigley, D.D.; Elliott, M.N.; Setodji, C.M.; Hays, R.D. Quantifying Magnitude of Group-Level Differences in Patient Experiences with Health Care. Health Serv. Res. 2018, 53 (Suppl. S1), 3027. [Google Scholar] [CrossRef]
- Halpern, M.T.; Urato, M.P.; Lines, L.M.; Cohen, J.B.; Arora, N.K.; Kent, E.E. Healthcare experience among older cancer survivors: Analysis of the SEER-CAHPS dataset. J. Geriatr. Oncol. 2018, 9, 194–203. [Google Scholar] [CrossRef]
- Farias, A.J.; Toledo, G.; Ochoa, C.Y.; Hamilton, A.S. Racial/ethnic Disparities in Patient Experiences with Health Care in Association with Earlier Stage at Colorectal Cancer Diagnosis: Findings from the SEER-CAHPS Data. Med. Care 2021, 59, 295–303. [Google Scholar] [CrossRef]
- Lines, L.M.; Cohen, J.; Halpern, M.T.; Smith, A.W.; Kent, E.E. Care experiences among dually enrolled older adults with cancer: SEER-CAHPS, 2005–2013. Cancer Causes Control 2019, 30, 1137–1144. [Google Scholar] [CrossRef] [PubMed]
- Warshaw, R. Health Disparities Affect Millions in Rural U.S. Communities. AAMCNews, 31 October 2017. Available online: https://www.aamc.org/news-insights/health-disparities-affect-millions-rural-us-communities (accessed on 6 April 2022).
- Cafer, A.; Rosenthal, M.; Laurent, B.; Conner, J.; Anderson, R. Health Landscapes in the South: Rurality, Racism, and a Path Forward. 2020. Available online: https://southernstudies.olemiss.edu/study-the-south/health-landscapes-in-the-south/ (accessed on 6 April 2022).
- US Department of Health and Human Services. Rural Action Plan—September 2020. 2020. Available online: https://www.hhs.gov/sites/default/files/hhs-rural-action-plan.pdf (accessed on 6 April 2022).
- Mollica, M.A.; Weaver, K.E.; McNeel, T.S.; Kent, E.E. Examining urban and rural differences in perceived timeliness of care among cancer patients: A SEER-CAHPS study. Cancer 2018, 124, 3257–3265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauer, A.; Wallner, L.P.; Davis, M.A.; Choi, S.W.; Friese, C.R. Health care experiences for older adults diagnosed with leukemia and lymphoma: Factors associated with emergency department use, timeliness and access of health care. J. Geriatr. Oncol. 2020, 12, 250–255. [Google Scholar] [CrossRef]
- Mollica, M.A.; Buckenmaier, S.S.; Halpern, M.T.; McNeel, T.S.; Weaver, S.J.; Doose, M.; Kent, E.E. Perceptions of care coordination among older adult cancer survivors: A SEER-CAHPS study. J. Geriatr. Oncol. 2020, 12, 446–452. [Google Scholar] [CrossRef]
- Mehta, R.; Tsilimigras, D.I.; Paredes, A.Z.; Dillhoff, M.; Cloyd, J.M.; Ejaz, A.; Tsung, A.; Pawlik, T.M. Is Patient Satisfaction Dictated by Quality of Care Among Patients Undergoing Complex Surgical Procedures for a Malignant Indication? Ann. Surg. Oncol. 2020, 27, 3126–3135. [Google Scholar] [CrossRef] [PubMed]
- Snyder, R.A.; Wardrop, R.; McLain, A.C.; Parikh, A.A.; Cass, A.L. Association of Patient Experience with Guideline-Concordant Colon Cancer Treatment in the Elderly. JCO Oncol. Pract. 2021, 17, e753–e763. [Google Scholar] [CrossRef]
- Bill-Axelson, A.; Holmberg, L.; Ruutu, M.; Häggman, M.; Andersson, S.O.; Bratell, S.; Spångberg, A.; Busch, C.; Nordling, S.; Garmo, H.; et al. Radical Prostatectomy versus Watchful Waiting in Early Prostate Cancer. N. Engl. J. Med. 2011, 364, 1708–1717. [Google Scholar] [CrossRef] [Green Version]
- Bill-Axelson, A.; Holmberg, L.; Garmo, H.; Taari, K.; Busch, C.; Nordling, S.; Häggman, M.; Andersson, S.O.; Andrén, O.; Steineck, G.; et al. Radical Prostatectomy or Watchful Waiting in Prostate Cancer—29-Year Follow-up. N. Engl. J. Med. 2018, 379, 2319–2329. [Google Scholar] [CrossRef]
- Sidana, A.; Hernandez, D.J.; Feng, Z.; Partin, A.W.; Trock, B.J.; Saha, S.; Epstein, J.I. Treatment Decision-Making for Localized Prostate Cancer: What Younger Men Choose and Why. Prostate 2012, 72, 58. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) Committee on Monitoring Access to Personal Health Care Services. Access to Health Care in America; Millman, M., Ed.; National Academies Press: Washington, DC, USA, 1993. [Google Scholar] [CrossRef]
- Parikh-Patel, A.; Morris, C.R.; Kizer, K.W.; Wun, T.; Keegan, T.H.M. Urban–Rural Variations in Quality of Care Among Patients with Cancer in California. Am. J. Prev. Med. 2021, 61, e279–e288. [Google Scholar] [CrossRef]
- Chow, C.J.; Al-Refaie, W.B.; Abraham, A.; Markin, A.; Zhong, W.; Rothenberger, D.A.; Kwaan, M.R.; Habermann, E.B. Does Patient Rurality Predict Quality Colon Cancer Care? A Population Based Study. Dis. Colon Rectum 2015, 58, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Shill, D.K.; Roobol, M.J.; Ehdaie, B.; Vickers, A.J.; Carlsson, S.V. Active surveillance for prostate cancer. Transl. Androl. Urol. 2021, 10, 2809–2819. [Google Scholar] [CrossRef]
- Klotz, L. Active surveillance in intermediate-risk prostate cancer. BJU Int. 2020, 125, 346–354. [Google Scholar] [CrossRef]
- Levit, L.A.; Byatt, L.; Lyss, A.P.; Paskett, E.D.; Levit, K.; Kirkwood, K.; Schenkel, C.; Schilsky, R.L. Closing the Rural Cancer Care Gap: Three Institutional Approaches. JCO Oncol. Pract. 2020, 16, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, T.C., III. Geography and disparities in health care. In Guidance for the National Healthcare Disparities Report, 1st ed.; Swift, E.K., Ed.; National Academies Press: Washington, DC, USA, 2002; p. 216. Available online: https://www.ncbi.nlm.nih.gov/books/NBK221045/ (accessed on 22 March 2023).
- Cyr, M.E.; Etchin, A.G.; Guthrie, B.J.; Benneyan, J.C. Access to specialty healthcare in urban versus rural US populations: A systematic literature review. BMC Health Serv. Res. 2019, 19, 974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute. SEER Treatment Data Limitations (November 2020 Submission)—SEER Data & Software. Available online: https://seer.cancer.gov/data-software/documentation/seerstat/nov2020/treatment-limitations-nov2020.html (accessed on 26 March 2022).



{kind=link}
{kind=link}
| Variable | Large Metro (n = 1798) | Metro (n = 1211) | Rural (n = 370) | p-Value a |
|---|---|---|---|---|
| Age when responding to survey | 74.4 ± 6.7 | 74.6 ± 6.3 | 74.0 ± 6.1 | 0.371 |
| Time between prostate cancer diagnosis and CAHPS survey | 0.905 | |||
| Less than 2 years | 657 (36.5) | 462 (38.2) | 133 (36.0) | |
| 2–5 years | 825 (45.9) | 542 (44.8) | 172 (46.5) | |
| >5 years | 316 (17.6) | 207 (17.1) | 65 (17.6) | |
| Health plan type at the time of CAHPS survey | <0.001 | |||
| Medicare Advantage | 830 (46.2) | 557 (46) | 229 (61.9) | |
| Fee-for-service | 968 (53.8) | 654 (54) | 141 (38.1) | |
| Race | <0.001 | |||
| Non-Hispanic White | 1224 (68.1) | 870 (71.8) | >290 (>78.4) | |
| Non-Hispanic Black | 272 (15.1) | 126 (10.4) | 38 (10.3) | |
| Hispanic | 171 (9.5) | 75 (6.2) | 15 (4.1) | |
| Non-Hispanic Asian | 88 (4.9) | 87 (7.2) | <11 (<3.0) | |
| Other | 43 (2.4) | 53 (4.4) | 16 (4.3) | |
| Education level | <0.001 | |||
| Some college or above | 1069 (59.5) | 687 (56.7) | 170 (46.0) | |
| High School or less | 637 (35.4) | 455 (37.6) | 184 (49.7) | |
| Missing | 92 (5.1) | 69 (5.7) | 16 (4.3) | |
| Proxy answered questions for the respondent | 0.586 | |||
| No | 1402 (78.0) | 915 (75.6) | 284 (76.8) | |
| Yes | 160 (8.9) | 114 (9.4) | 32 (8.7) | |
| Missing | 236 (13.1) | 182 (15) | 54 (14.6) | |
| Low-income subsidy | 0.084 | |||
| No | 1566 (87.1) | 1087 (89.8) | 325 (87.8) | |
| Yes | 232 (12.9) | 124 (10.2) | 45 (12.2) | |
| Dual eligibility for Medicare and Medicaid | 0.007 | |||
| No | 1590 (88.4) | 1106 (91.3) | 329 (88.9) | |
| Yes | 195 (10.9) | >94 (>7.8) | >30 (>8.1) | |
| Missing | 13 (0.7) | <11 (<0.9) | <11 (<3.0) | |
| Marital status | 0.271 | |||
| Not Married | 377 (21.0) | 220 (18.2) | 72 (19.5) | |
| Married | 1184 (65.9) | 841 (69.5) | 255 (68.9) | |
| Missing | 237 (13.2) | 150 (12.4) | 43 (11.6) | |
| Geographic region when answering the CAHPS survey | <0.001 | |||
| Northeast | 414 (23.0) | 151 (12.5) | 16 (4.3) | |
| Midwest | 205 (11.4) | 100 (8.3) | 57 (15.4) | |
| South | 349 (19.4) | 294 (24.3) | 151 (40.8) | |
| West | 830 (46.2) | 666 (55.0) | 146 (39.5) | |
| Census tract poverty indicator | <0.001 | |||
| 0–<5% poverty | 585 (32.5) | 276 (22.8) | 28 (7.6) | |
| 5% to <10% poverty | 517 (28.8) | 328 (27.1) | 69 (18.7) | |
| 10% to <20% poverty | 421 (23.4) | 386 (31.9) | 160 (43.2) | |
| 20% to 100% poverty | >264 (>14.7) | >210 (>17.3) | >102 (>27.6) | |
| Missing | <11 (<0.6) | <11 (<0.9) | <11 (<3.0) | |
| Smoking status | 0.074 | |||
| Non-Smoker | 1532 (85.2) | 1029 (85.0) | 303 (81.9) | |
| Smoker | 164 (9.1) | 122 (10.1) | 51 (13.8) | |
| Missing | 102 (5.7) | 60 (5.0) | 16 (4.3) | |
| Survey year | 0.018 | |||
| 2008 | 65 (3.6) | 35 (2.9) | 12 (3.2) | |
| 2009 | 136 (7.6) | 95 (7.8) | 32 (8.7) | |
| 2010 | 193 (10.7) | 124 (10.2) | 25 (6.8) | |
| 2011 | 218 (12.1) | 159 (13.1) | 54 (14.6) | |
| 2012 | 274 (15.2) | 238 (19.7) | 73 (19.7) | |
| 2013 | 316 (17.6) | 219 (18.1) | 60 (16.2) | |
| 2014 | 309 (17.2) | 196 (16.2) | 65 (17.6) | |
| 2015 | 287 (16.0) | 145 (12.0) | 49 (13.2) | |
| Comorbidity count | 0.816 | |||
| 0 | 778 (43.3) | 545 (45.0) | 166 (44.9) | |
| 1 | 629 (35.0) | 414 (34.2) | 116 (31.4) | |
| 2 | 300 (16.7) | 193 (15.9) | 68 (18.4) | |
| 3 or 4 | 91 (5.1) | 59 (4.9) | 20 (5.4) | |
| Tumor grade | 0.020 * | |||
| Well differentiated | <11 (<0.6) | <11 (<0.9) | <11 (<3.0) | |
| Moderately differentiated | 387 (21.5) | 300 (24.8) | 76 (20.5) | |
| Poorly differentiated | >1338 (>74.4) | >868 (>71.7) | >255 (>68.9) | |
| Undifferentiated | <11 (<0.6) | <11 (<0.9) | <11 (<3.0) | |
| Unknown | 51 (2.8) | 21 (1.7) | 17 (4.6) | |
| Time between prostate cancer diagnosis and receiving definitive treatment | <0.001 | |||
| Within a month from diagnosis | 469 (26.1) | 394 (32.5) | 122 (33) | |
| 2 months from diagnosis | 387 (21.5) | 294 (24.3) | 77 (20.8) | |
| 3 months from diagnosis | 297 (16.5) | 174 (14.4) | 41 (11.1) | |
| >3 months from diagnosis | 345 (19.2) | 166 (13.7) | 49 (13.2) | |
| Never | 300 (16.7) | 183 (15.1) | 81 (21.9) | |
| Receipt of radiation as a part of initial treatment | 0.342 * | |||
| No | >858 (>47.7) | >603 (>49.8) | >187 (>50.5) | |
| Yes | 929 (51.7) | 597 (49.3) | 172 (46.5) | |
| Missing | <11 (<0.6) | <11 (<0.9) | <11 (<3.0) | |
| Receipt of definitive surgery as a part of initial treatment | 0.091 * | |||
| No | 1218 (67.7) | >763 (>63.0) | 249 (67.3) | |
| Yes | 580 (32.3) | 437 (36.1) | 121 (32.7) | |
| Missing | 0 (0.0) | <11 (<0.9) | 0 (0.0) | |
| Risk of disease progression | 0.538 | |||
| Intermediate | 1333 (74.1) | 894 (73.8) | 264 (71.4) | |
| High | 465 (25.9) | 317 (26.2) | 106 (28.7) | |
| Number of prior cancers other than prostate cancer | 0.113 | |||
| 0 | 1611 (89.6) | 1101 (90.9) | 339 (91.6) | |
| 1 | 171 (9.5) | >83 (>6.9) | >20 (>5.4) | |
| 2 | 16 (0.9) | 16 (1.3) | <11 (<3.0) | |
| 3 | 0 (0) | <11 (<0.9) | 0 (0) | |
| General health status | 0.516 | |||
| Missing | 51 (2.8) | 42 (3.5) | 13 (3.5) | |
| Excellent | 153 (8.5) | 94 (7.8) | 26 (7.0) | |
| Very good | 520 (28.9) | 351 (29.0) | 100 (27.0) | |
| Good | 679 (37.8) | 463 (38.2) | 131 (35.4) | |
| Fair | 336 (18.7) | 216 (17.8) | 80 (21.6) | |
| Poor | 59 (3.3) | 45 (3.7) | 20 (5.4) | |
| Mental health status | 0.061 | |||
| Missing | 55 (3.1) | 38 (3.1) | 10 (2.7) | |
| Excellent | 610 (33.9) | 381 (31.5) | 97 (26.2) | |
| Very good | 563 (31.3) | 400 (33.0) | 143 (38.7) | |
| Good | 409 (22.8) | 299 (24.7) | 83 (22.4) | |
| Fair | 135 (7.5) | 83 (6.9) | 29 (7.8) | |
| Poor | 26 (1.5) | 10 (0.8) | 8 (2.2) |
| Variable | Treated LSM ± SE | Not Treated LSM ± SE | Adjusted Difference (95% CI) |
|---|---|---|---|
| Composite measures | |||
| Obtaining needed care (n = 2460) Obtaining care quickly (n = 2864) Doctor communication (n = 2504) | 85.3 ± 6.2 | 85.2 ± 6.2 | −0.1 (−2.4 to 2.2) |
| 61.1 ± 6.0 | 59.6 ± 6.0 | −1.4 (−4.1 to 1.2) | |
| 86.9 ± 4.9 | 84.9 ± 4.9 | −2.0 (−3.8 to −0.2) *,+ | |
| Obtaining needed prescription drugs (n = 1811) | 93.4 ± 6.2 | 92.3 ± 6.3 | −1.1 (−3.7 to 1.6) |
| Customer service (n = 878) | 68.5 ± 8.7 | 65.2 ± 8.8 | −3.3 (−8.2 to 1.6) |
| Ratings | |||
| Primary care provider rating (n = 2494) | 88.2 ± 4.4 | 86.9 ± 4.4 | −1.4 (−2.9 to 0.2) |
| Specialist rating (n = 2089) | 87.4 ± 5.1 | 84.9 ± 5.1 | −2.5 (−4.4 to −0.7) *,+ |
| Health plan rating (n = 2956) | 85.2 ± 4.5 | 83.6 ± 4.5 | −1.6 (−3.5 to 0.3) |
| Overall care rating (n = 2913) | 89.0 ± 4.1 | 86.6 ± 4.1 | −2.4 (−4.1 to −0.7) *,+ |
| Variable | Large Metro LSM ± SE | Metro LSM ± SE | Metro vs. Large Metro Adjusted Difference (95% CI) | Rural LSM ± SE | Rural vs. Large Metro Adjusted Difference (95% CI) |
|---|---|---|---|---|---|
| Treated | |||||
| Composite measures | |||||
| Obtaining needed care (n = 2460) | 82.8 ± 6.9 | 83.8 ± 6.9 | 1 (−0.8 to 2.8) | 86.4 ± 7.0 | 3.6 (0.5 to 6.7) *,++ |
| Obtaining care quickly (n = 2864) | 58.6 ± 6.3 | 59.1 ± 6.3 | 0.5 (−1.6 to 2.6) | 60.7 ± 6.5 | 2.1 (−1.5 to 5.7) |
| Doctor communication (n = 2504) | 86.6 ± 5.3 | 86.9 ± 5.3 | 0.3 (−1.1 to 1.7) | 88.7 ± 5.4 | 2.1 (−0.3 to 4.4) |
| Obtaining needed prescription drugs (n = 1811) | 90.7 ± 7.1 | 92.7 ± 7.0 | 2 (−0.1 to 4.1) | 92.7 ± 7.2 | 2 (−1.7 to 5.7) |
| Customer service (n = 716) | 64.5 ± 10.1 | 61.7 ± 10.2 | −2.8 (−6.8 to 1.3) | 63.7 ± 10.8 | −0.8 (−8.4 to 6.8) |
| Ratings | |||||
| Primary care provider rating (n = 2494) | 87.0 ± 4.8 | 87.5 ± 4.8 | 0.4 (−0.8 to 1.7) | 87.9 ± 4.9 | 0.9 (−1.2 to 3) |
| Specialist rating (n = 2089) | 84.0 ± 4.2 | 84.3 ± 4.2 | 0.3 (−1 to 1.7) | 84.5 ± 4.3 | 0.6 (−1.8 to 2.9) |
| Health plan rating (n = 2956) | 83.0 ± 4.7 | 82.3 ± 4.7 | −0.7 (−2.2 to 0.8) | 83.1 ± 4.8 | 0.1 (−2.5 to 2.7) |
| Overall care rating (n = 2913) | 88.6 ± 4.3 | 88.6 ± 4.2 | 0 (−1.3 to 1.3) | 89.4 ± 4.4 | 0.8 (−1.4 to 3.1) |
| Not Treated | |||||
| Composite measures | |||||
| Obtaining needed care (n = 391) | 86.1 ± 8.0 | 82.2 ± 8.0 | −3.9 (−8.2 to 0.4) | 79.1 ± 8.4 | −7.0 (−12.7 to −1.2) *,+++ |
| Obtaining care quickly (n = 474) | 62.0 ± 10.4 | 64.5 ± 10.4 | 2.5 (−2.7 to 7.7) | 58.2 ± 10.9 | −3.9 (−10.9 to 3.2) |
| Doctor communication (n = 411) | 78.0 ± 7.2 | 76.9 ± 7.3 | −1.1 (−4.7 to 2.5) | 78.2 ± 7.6 | 0.2 (−4.7 to 5.2) |
| Obtaining needed prescription drugs (n = 323) | 78.2 ± 8.9 | 76.3 ± 9.0 | −1.9 (−7.2 to 3.4) | 80.1 ± 9.2 | 1.9 (−5.3 to 9.1) |
| Customer service (n = 162) | 59.0 ± 12.0 | 60.9 ± 11.0 | 1.9 (−7.9 to 11.6) | 53.6 ± 13 | −5.4 (−19.5 to 8.6) |
| Ratings | |||||
| Primary care provider rating (n = 404) | 81.5 ± 5.9 | 80.2 ± 5.9 | −1.3 (−4.3 to 1.6) | 79.7 ± 6.2 | −1.8 (−5.8 to 2.3) |
| Specialist rating (n = 333) | 84.1 ± 8.0 | 83.2 ± 7.9 | −0.9 (−5.2 to 3.5) | 80.5 ± 8.4 | −3.7 (−9.6 to 2.3) |
| Health plan rating (n = 498) | 90.4 ± 8.0 | 87.5 ± 8.0 | −3.0 (−6.8 to 0.9) | 82.6 ± 8.3 | −7.9 (−13.1 to −2.6) *,+++ |
| Overall care rating (n = 476) | 83.0 ± 7.4 | 82.7 ± 7.4 | −0.3 (−4.1 to 3.5) | 78.2 ± 7.7 | −4.8 (−10 to 0.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandit, A.A.; Patil, N.N.; Mostafa, M.; Kamel, M.; Halpern, M.T.; Li, C. Rural–Urban Disparities in Patient Care Experiences among Prostate Cancer Survivors: A SEER-CAHPS Study. Cancers 2023, 15, 1939. https://doi.org/10.3390/cancers15071939
Pandit AA, Patil NN, Mostafa M, Kamel M, Halpern MT, Li C. Rural–Urban Disparities in Patient Care Experiences among Prostate Cancer Survivors: A SEER-CAHPS Study. Cancers. 2023; 15(7):1939. https://doi.org/10.3390/cancers15071939
Chicago/Turabian StylePandit, Ambrish A., Nilesh N. Patil, Mostafa Mostafa, Mohamed Kamel, Michael T. Halpern, and Chenghui Li. 2023. "Rural–Urban Disparities in Patient Care Experiences among Prostate Cancer Survivors: A SEER-CAHPS Study" Cancers 15, no. 7: 1939. https://doi.org/10.3390/cancers15071939