
Quantitative MRI to Characterize Hypoxic Tumors in Comparison to FMISO PET/CT for Radiotherapy in Oropharynx Cancers
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Method
2.1. Study
2.2. FDG PET Imaging
2.3. FMISO PET-MRI Imaging
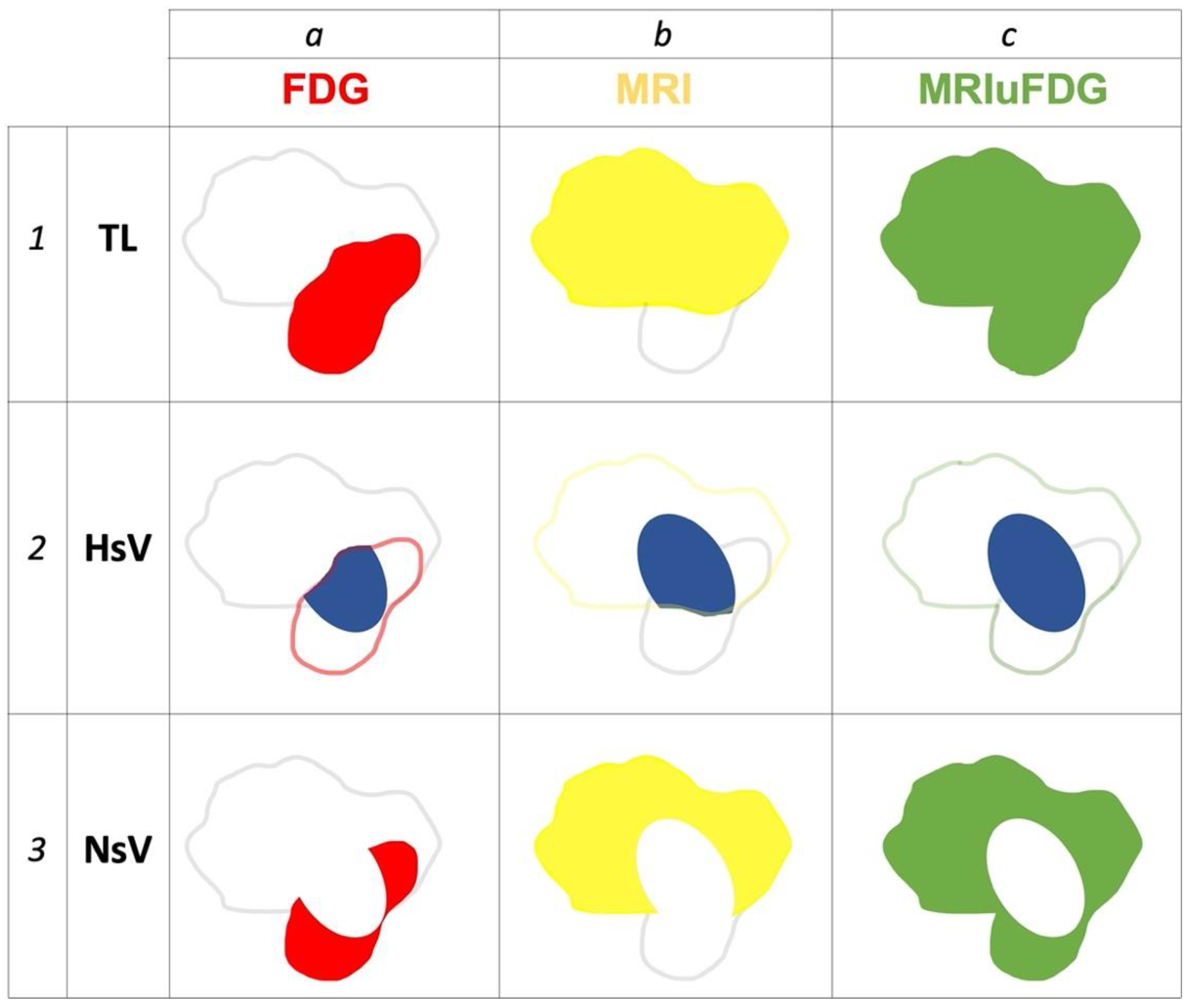
2.4. Registration, Segmentation, and Definition of Tumor Volumes as Well as Hypoxic and Normoxic Sub Volumes
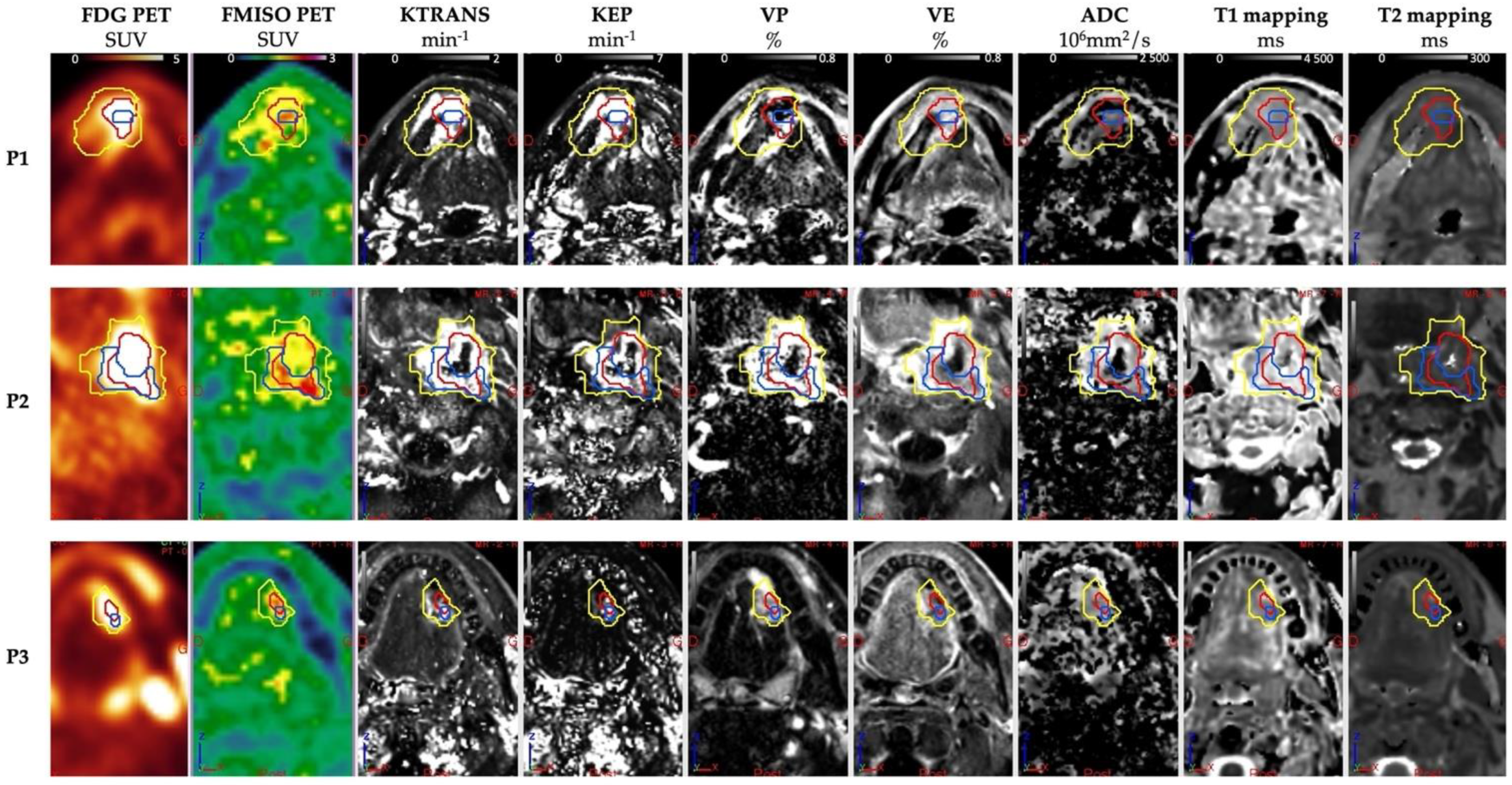
2.5. Quantitative Parameters
2.6. Statistical Analysis
3. Results
3.1. Quantitative Parameters of PET and MRI
3.1.1. Analysis of PET Data and MRI Volume
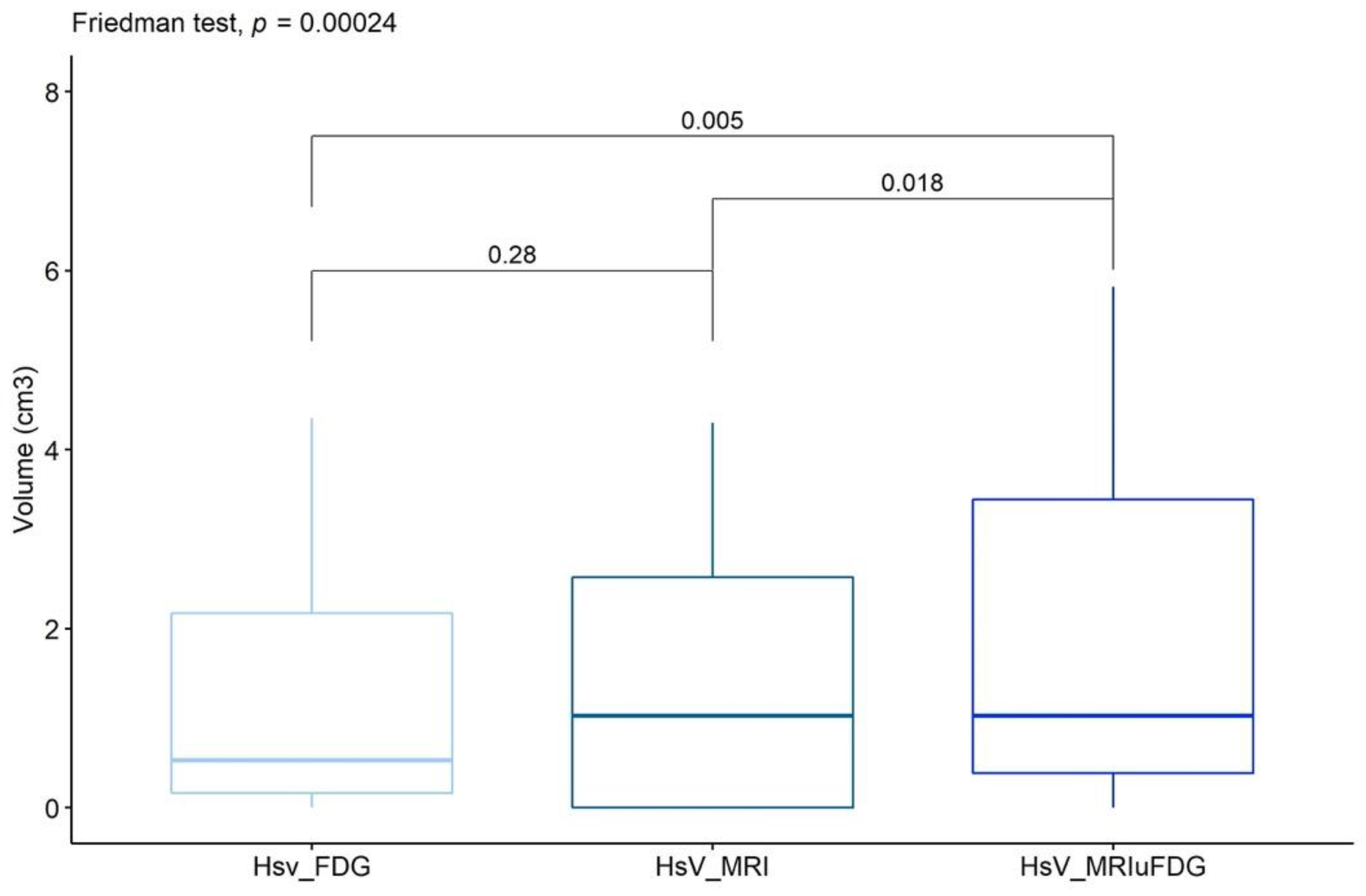
3.1.2. Comparison of Hypoxic Sub-Volumes
3.1.3. Comparison of PET and MRI Parameters between Patients with and without Measurable Hypoxic Volumes
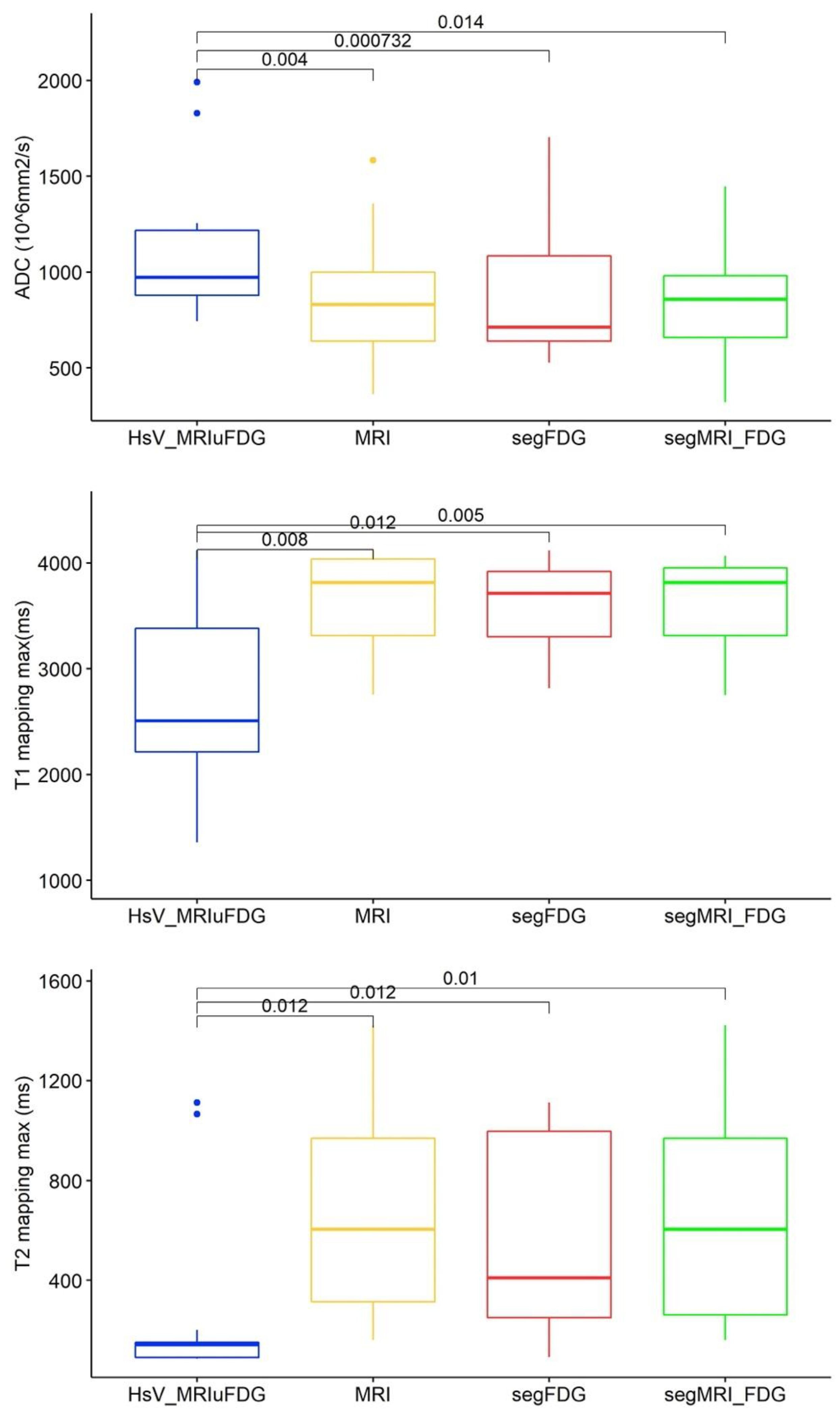
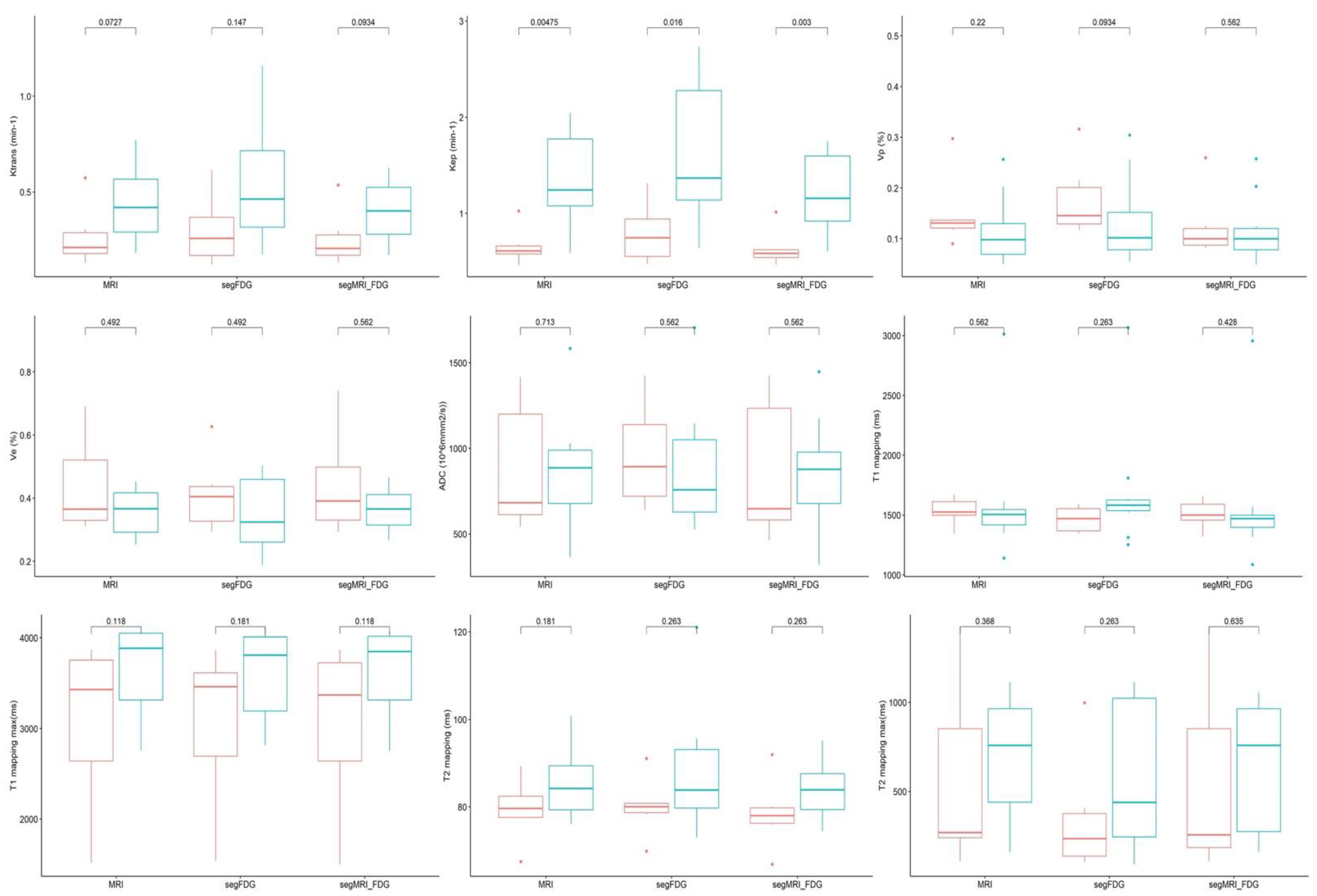
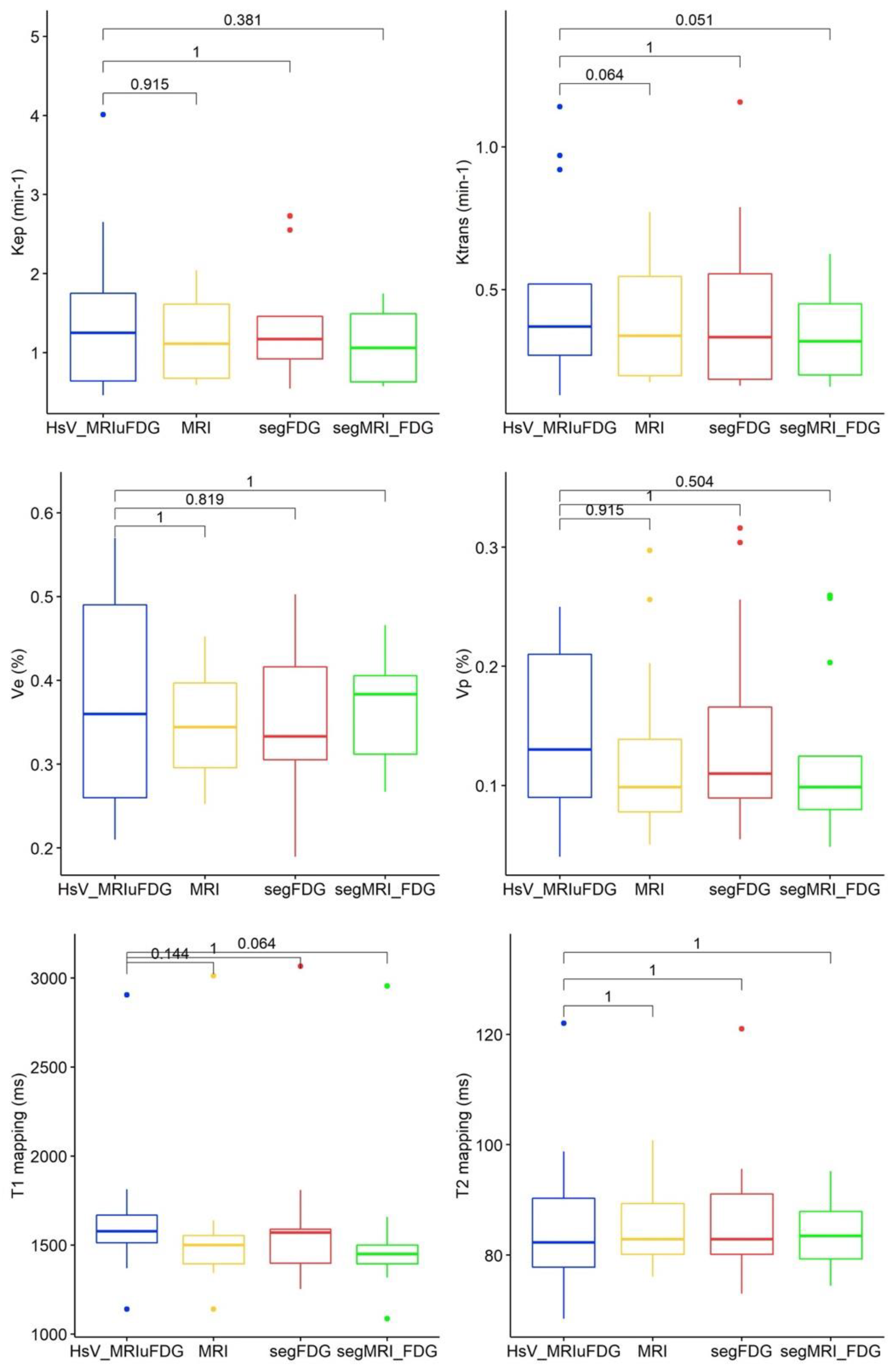
3.2. Quantitative MRI Parameters According to Hypoxic Segmentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Thorwarth, D.; Welz, S.; Mönnich, D.; Pfannenberg, C.; Nikolaou, K.; Reimold, M.; La Fougère, C.; Reischl, G.; Mauz, P.-S.; Paulsen, F.; et al. Prospective Evaluation of a Tumor Control Probability Model Based on Dynamic 18F-FMISO PET for Head and Neck Cancer Radiotherapy. J. Nucl. Med. 2019, 60, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Schoder, H.; Beattie, B.; Lanning, R.; Riaz, N.; McBride, S.; Katabi, N.; Li, D.; Yarusi, B.; Chan, S.; et al. Strategy of Using Intratreatment Hypoxia Imaging to Selectively and Safely Guide Radiation Dose De-escalation Concurrent With Chemotherapy for Locoregionally Advanced Human Papillomavirus-Related Oropharyngeal Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 9–17. [Google Scholar] [CrossRef]
- Rischin, D.; Hicks, R.J.; Fisher, R.; Binns, D.; Corry, J.; Porceddu, S.; Peters, L.J. Prognostic significance of [18F]-misonidazole positron emission tomography-detected tumor hypoxia in patients with advanced head and neck cancer randomly assigned to chemoradiation with or without tirapazamine: A Substudy of Trans-Tasman Radiation Oncology Group Study 98.02. J. Clin. Oncol. 2006, 24, 2098–2104. [Google Scholar] [CrossRef] [Green Version]
- Zschaeck, S.; Löck, S.; Hofheinz, F.; Zips, D.; Mortensen, L.S.; Zöphel, K.; Troost, E.G.; Boeke, S.; Saksø, M.; Mönnich, D.; et al. Individual patient data meta-analysis of FMISO and FAZA hypoxia PET scans from head and neck cancer patients undergoing definitive radio-chemotherapy. Radiother. Oncol. 2020, 149, 189–196. [Google Scholar] [CrossRef]
- Stieb, S.; Eleftheriou, A.; Warnock, G.; Guckenberger, M.; Riesterer, O. Longitudinal PET imaging of tumor hypoxia during the course of radiotherapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2201–2217. [Google Scholar] [CrossRef] [PubMed]
- Dolezel, M.; Slavik, M.; Blazek, T.; Kazda, T.; Koranda, P.; Veverkova, L.; Burkon, P.; Cvek, J. FMISO-Based Adaptive Radiotherapy in Head and Neck Cancer. J. Pers. Med. 2022, 12, 1245. [Google Scholar]
- Qiu, J.; Lv, B.; Fu, M.; Wang, X.; Zheng, X.; Zhuo, W. 18F-Fluoromisonidazole positron emission tomography/CT-guided volumetric-modulated arc therapy-based dose escalation for hypoxic subvolume in nasopharyngeal carcinomas: A feasibility study. Head Neck 2017, 39, 2519–2527. [Google Scholar] [CrossRef]
- Lazzeroni, M.; Ureba, A.; Wiedenmann, N.; Nicolay, N.H.; Mix, M.; Thomann, B.; Baltas, D.; Toma-Dasu, I.; Grosu, A.L. Evolution of the hypoxic compartment on sequential oxygen partial pressure maps during radiochemotherapy in advanced head and neck cancer. Phys. Imaging Radiat. Oncol. 2021, 17, 100–105. [Google Scholar] [CrossRef]
- Bittner, M.-I.; Wiedenmann, N.; Bucher, S.; Hentschel, M.; Mix, M.; Rücker, G.; Weber, W.A.; Meyer, P.T.; Werner, M.; Grosu, A.-L.; et al. Analysis of relation between hypoxia PET imaging and tissue-based biomarkers during head and neck radiochemotherapy. Acta Oncol. 2016, 55, 1299–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamming-Vrieze, O.; Navran, A.; Al-Mamgani, A.; Vogel, W.V. Biological PET-guided adaptive radiotherapy for dose escalation in head and neck cancer: A systematic review. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 349–368. [Google Scholar] [CrossRef] [PubMed]
- Wiedenmann, N.; Grosu, A.-L.; Büchert, M.; Rischke, H.C.; Ruf, J.; Bielak, L.; Majerus, L.; Rühle, A.; Bamberg, F.; Baltas, D.; et al. The utility of multiparametric MRI to characterize hypoxic tumor subvolumes in comparison to FMISO PET/CT. Consequences for diagnosis and chemoradiation treatment planning in head and neck cancer. Radiother. Oncol. 2020, 150, 128–135. [Google Scholar] [CrossRef]
- Gaustad, J.-V.; Hauge, A.; Wegner, C.S.; Simonsen, T.G.; Lund, K.V.; Hansem, L.M.K.; Rofstad, E.K. DCE-MRI of tumor hypoxia and hypoxia-associated aggressiveness. Cancers 2020, 12, 1979. [Google Scholar] [CrossRef] [PubMed]
- Serša, I.; Bajd, F.; Savarin, M.; Jesenko, T.; Čemažar, M.; Serša, G. Multiparametric high-resolution MRI as a tool for mapping of hypoxic level in tumors. Technol. Cancer Res. Treat. 2018, 17, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shu, C.Y.; Herman, P.; Coman, D.; Sanganahalli, B.G.; Wang, H.; Juchem, C.; Rothman, D.L.; de Graaf, R.A.; Hyder, F. Brain region and activity-dependent properties of M for calibrated fMRI. Neuroimage 2016, 125, 848–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferda, J.; Ferdová, E.; Vítovec, M.; Glanc, D.; Mírka, H. The imaging of the hypoxic microenvironment in tumorous tissue using PET/CT and PET/MRI. Eur. J. Radiol. 2022, 154, 110458. [Google Scholar] [CrossRef] [PubMed]
- Texte, E.; Gouel, P.; Thureau, S.; LeQuesne, J.; Barres, B.; Edet-Sanson, A.; Decazes, P.; Vera, P.; Hapdey, S. Impact of the Bayesian penalized likelihood algorithm (Q.Clear®) in comparison with the OSEM reconstruction on low contrast PET hypoxic images. EJNMMI Phys. 2020, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Widmann, G.; Henninger, B.; Kremser, C.; Jaschke, W. MRI Sequences in Head & Neck Radiology—State of the Art. RoFo 2017, 189, 413–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, K.; Al-Farra, G.; Dejanovic, D.; Eriksen, J.G.; Loft, A.; Hansen, C.R.; Pameijer, F.A.; Zukauskaite, R.; Grau, C. Imaging for Target Delineation in Head and Neck Cancer Radiotherapy. Semin. Nucl. Med. 2021, 51, 59–67. [Google Scholar] [CrossRef]
- Pyatigorskaya, N.; De Laroche, R.; Bera, G.; Giron, A.; Bertolus, C.; Herve, G.; Chambenois, E.; Bergeret, S.; Dormont, D.; Amor-Sahli, M.; et al. Are Gadolinium-Enhanced MR Sequences Needed in Simultaneous 18F-FDG-PET/MRI for Tumor Delineation in Head and Neck Cancer? AJNR Am. J. Neuroradiol. 2020, 41, 1888–1896. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, S.; Shiga, T.; Yasuda, K.; Ito, Y.M.; Magota, K.; Kasai, K.; Kuge, Y.; Shirato, H.; Tamaki, N. High reproducibility of tumor hypoxia evaluated by 18F-fluoromisonidazole pet for head and neck cancer. J. Nucl. Med. 2013, 54, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, M.; Hirata, K.; Gafita, A.; Watanabe, S.; Okamoto, S.; Magota, K.; Shiga, T.; Kuge, Y.; Tamaki, N. Voxel based comparison and texture analysis of 18 F-FDG and 18 F-FMISO PET of patients with head-and-neck cancer. PLoS ONE 2019, 14, e0213111. [Google Scholar] [CrossRef] [PubMed]
- Rogasch, J.; Beck, M.; Stromberger, C.; Hofheinz, F.; Ghadjar, P.; Wust, P.; Budach, V.; Amthauer, H.; Tinhofer, I.; Furth, C.; et al. PET measured hypoxia and MRI parameters in re-irradiated head and neck squamous cell carcinomas: Findings of a prospective pilot study. F1000Research 2020, 9, 1350. [Google Scholar] [CrossRef] [PubMed]
- Thureau, S.; Piton, N.; Gouel, P.; Modzelewski, R.; Dujon, A.; Baste, J.-M.; Melki, J.; Rinieri, P.; Peillon, C.; Rastelli, O.; et al. First Comparison between [18f]-FMISO and [18f]-Faza for Preoperative Pet Imaging of Hypoxia in Lung Cancer. Cancers 2021, 13, 4101. [Google Scholar] [CrossRef] [PubMed]
- Welz, S.; Paulsen, F.; Pfannenberg, C.; Reimold, M.; Reischl, G.; Nikolaou, K.; La Fougère, C.; Alber, M.; Belka, C.; Zips, D.; et al. Dose escalation to hypoxic subvolumes in head and neck cancer: A randomized phase II study using dynamic [(18)F]FMISO PET/CT. Radiother. Oncol. 2022, 171, 30–36. [Google Scholar] [CrossRef]
- Gagel, B.; Reinartz, P.; Demirel, C.; Kaiser, H.J.; Zimny, M.; Piroth, M.; Pinkawa, M.; Stanzel, S.; Asadpour, B.; Hamacher, K.; et al. [18F] fluromisonidazole and [18F] fluorodeoxyglucose positron emission tomography in response evaluation after chemo-/radiotherapy of non-small-cell lung cancer: A feasibility study. BMC Cancer 2006, 6, 51. [Google Scholar] [CrossRef] [Green Version]
- Zimny, M.; Gagel, B.; DiMartino, E.; Hamacher, K.; Coenen, H.H.; Westhofen, M.; Eble, M.; Buell, U.; Reinartz, P. FDG—A marker of tumour hypoxia? A comparison with [18F]fluoromisonidazole and pO2-polarography in metastatic head and neck cancer. Eur. J. Nucl. Med. 2006, 33, 1426–1431. [Google Scholar] [CrossRef]
- Dunn, J.F.; Ding, S.; O’Hara, J.A.; Liu, K.J.; Rhodes, E.; Goda, F.; Swartz, H.M. Can NMR diffusion-weighted imaging provide quantitative information on tumor interstital pO2? Adv. Exp. Med. Biol. 1997, 411, 209–214. [Google Scholar] [CrossRef]
- Miyasaka, N.; Nagaoka, T.; Kuroiwa, T.; Akimoto, H.; Haku, T.; Kubota, T.; Aso, T. Histopathologic correlates of temporal diffusion changes in a rat model of cerebral hypoxia/ischemia. AJNR Am. J. Neuroradiol. 2000, 21, 60–66. [Google Scholar] [PubMed]
- Thoeny, H.C.; Ross, B.D. Predicting and monitoring cancer treatment response with diffusion-weighted MRI. J. Magn. Reson. Imaging 2010, 32, 2–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swartz, J.E.; Driessen, J.P.; van Kempen, P.M.; de Bree, R.; Janssen, L.M.; Pameijer, F.A.; Terhaard, C.H.; Philippens, M.E.; Willems, S. Influence of tumor and microenvironment characteristics on diffusion-weighted imaging in oropharyngeal carcinoma: A pilot study. Oral Oncol. 2018, 77, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Mills, A.F.; Sakai, O.; Anderson, S.W.; Jara, H. Principles of Quantitative MR Imaging with Illustrated Review of Applicable Modular Pulse Diagrams. RadioGraphics 2017, 37, 2083–2105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouel, P.; Hapdey, S.; Dumouchel, A.; Gardin, I.; Torfeh, E.; Hinault, P.; Vera, P.; Thureau, S.; Gensanne, D. Synthetic MRI for Radiotherapy Planning for Brain and Prostate Cancers: Phantom Validation and Patient Evaluation. Front. Oncol. 2022, 12, 1–12. [Google Scholar] [CrossRef]
- Zegers, C.M.L.; Van Elmpt, W.; Szardenings, K.; Kolb, H.; Waxman, A.; Subramaniam, R.M.; Moon, D.H.; Brunetti, J.C.; Srinivas, S.M.; Lambin, P.; et al. Repeatability of hypoxia PET imaging using [18F]HX4 in lung and head and neck cancer patients: A prospective multicenter trial. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1840–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, E.M.; Asselin, M.C.; Forster, D.; O’Connor, J.P.B.; Senra, J.M.; Williams, K.J. The Meaning, Measurement and Modification of Hypoxia in the Laboratory and the Clinic. Clin. Oncol. 2014, 26, 277–288. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | T-Stage | HPV Statut | T-Site |
|---|---|---|---|---|---|
| 1 | H | 64 | T2N3b | Positive | Oral cavity |
| 2 | H | 56 | T4aN0 | Negative | Oral cavity |
| 3 | H | 63 | T4aN0 | Negative | Oral cavity |
| 4 | H | 76 | T2N0 | Negative | Oropharynx |
| 5 | H | 60 | T3N0 | Negative | Oropharynx |
| 6 | H | 72 | T3N1 | Negative | Oropharynx |
| 7 | H | 59 | T4aNx | Negative | Oral cavity |
| 8 | H | 35 | T2N3b | Negative | Oral cavity |
| 9 | H | 54 | T4aN2b | Negative | Oropharynx |
| 10 | H | 70 | T4aN0 | Negative | Oral cavity |
| 11 | H | 78 | T3N0 | Negative | Oral cavity |
| 12 | H | 70 | T4aN3b | Negative | Oral cavity |
| 13 | H | 77 | T4aN2b | Negative | Oropharynx |
| 14 | H | 54 | T4aN1 | Negative | Oral cavity |
| 15 | F | 75 | T4aN3b | Negative | Oral cavity |
| 16 | F | 64 | T4aN0 | Negative | Oral cavity |
| Settings | DCE-MRI | T1 Mapping | T2 Mapping | DWI |
|---|---|---|---|---|
| Plane | Axial | Axial | Axial | Axial |
| TR (ms) | 8.4 | 15 | 1000 | 8091 |
| TE (ms) | 3.1 | 3 | 5.98–11.96–17.94–23.92–29.9–35.88–41.86–47.84 | 80.5 |
| Flip Angle (degrees) | 25 | 3–10–20–30 | 90 | 90 |
| Matrix size (pixels) | 256 × 256 | 128 × 128 | 128 × 128 | 256 × 256 |
| Slice thickness (mm) | 3.4 | 2 | 2 | 3 |
| Slice spacing (mm) | 0 | 0 | 0 | 0.3 |
| Pixel size (mm) | 0.9 × 0.9 | 1.01 × 1.00 | 1.01 × 1.01 | 0.94 × 0.94 |
| Patients | FDG SUVmax | MTV cm3 | TLG | FMISO SUVmax | HSv FDG cm3 | HSv MRI cm3 | HSv MRIuFDG cm3 | MRI Volume cm3 |
|---|---|---|---|---|---|---|---|---|
| 1 * | 8.4 | 2.2 | 10.78 | 2.64 | 0.0 | 0.0 | 0.0 | 2.63 |
| 2 | 15.4 | 71.54 | 676.77 | 2.08 | 2.03 | 2.25 | 2.25 | 162.89 |
| 3 | 10.43 | 13.42 | 77.43 | 2.51 | 0.86 | 1.22 | 1.22 | 29.1 |
| 4 | 13.32 | 7.82 | 66.08 | 2.24 | 1.2 | 1.76 | 2.22 | 10.92 |
| 5 | 14.67 | 18.75 | 204.19 | 2.46 | 2.59 | 4.3 | 4.84 | 49.96 |
| 6 | 10.87 | 11.86 | 92.98 | 2.12 | 0.2 | 0.2 | 0.46 | 10.48 |
| 7 | 10.86 | 17.29 | 135.21 | 1.75 | 0.17 | 0.83 | 0.83 | 59.19 |
| 8 | 11.32 | 4.4 | 26.62 | 2.79 | 0.66 | 1.71 | 2.98 | 7.01 |
| 9 * | 8.69 | 9.76 | 47.43 | 1.25 | 0.0 | 0.0 | 0.0 | 30.51 |
| 10 | 11.14 | 31.59 | 219.87 | 2.44 | 4.35 | 4.13 | 5.82 | 62.22 |
| 11 * | 7.81 | 1.8 | 8.17 | 1.92 | 0.0 | 0.0 | 0.0 | 1.33 |
| 12 | 5.74 | 12.22 | 48.02 | 2.3 | 0.4 | 0.0 | 0.51 | 6.72 |
| 13 | 14.18 | 20.12 | 179.47 | 3.56 | 5.75 | 21.49 | 26.16 | 93.59 |
| 14 | 9.52 | 7.09 | 38.71 | 1.84 | 0.37 | 0.76 | 0.76 | 15.49 |
| 15 | 34.9 | 12.23 | 237.87 | 3.26 | 4.01 | 3.55 | 4.91 | 21.8 |
| 16 | 9.25 | 2.01 | 15.74 | 2.28 | 0.15 | 0.0 | 0.15 | 1.76 |
| Mean | 12.3 | 15.3 | 130.3 | 2.3 | 1.4 | 2.6 | 3.3 | 35.3 |
| Median (q1; q3) | 10.9 (9.1; 13.5) | 12.1 (6.4; 17.6) | 71.8 (35.7; 185.6) | 2.3 (2; 2.5) | 0.5 (0.2; 2.2) | 1 (0; 2.6) | 1 (0.4; 3.4) | 18.6 (6.9; 52.3) |
| min; max | 5.7; 34.9 | 1.8; 71.5 | 8.2; 676.7 | 1.2; 3.6 | 0; 5.7 | 0; 21.5 | 0; 26.2 | 1.3; 162.9 |
| Hypoxic Volume not Measurable (n = 3) | Hypoxic Volume Measurable (n = 13) | p-Value | |
|---|---|---|---|
| FDG PET | |||
| SUV max | 0.01 | ||
| mean (±standard deviation) | 8.7 (±2.0) | 14.4 (±7.5) | |
| median (q1;q3) | 8.5 (8.0; 10.3) | 12.3 (10.6; 14.5) | |
| min; max | 5.7; 10.9 | 9.2; 34.9 | |
| SUV mean | 0.02 | ||
| mean (± standard deviation) | 5.6 (±1.7) | 8.9 (±4.1) | |
| median (q1;q3) | 4.9 (4.6; 7.1) | 8.1 (6.3; 9.3) | |
| min; max | 3.9; 7.8 | 5.5; 19.4 | |
| SUV peak | 0.05 | ||
| n (NA) | 4 (2) | 8 (2) | |
| mean (±standard deviation) | 7.3 (±2.2) | 12.7 (±5.6) | |
| median (q1;q3) | 7.6 (5.9; 9.0) | 11.6 (9.6; 13.3) | |
| min; max | 4.7; 9.3 | 7.6; 25.6 | |
| MTV | 0.26 | ||
| mean (±standard deviation) | 9.2 (±6.1) | 18.9 (±20.5) | |
| median (q1;q3) | 10.8 (4.1; 12.1) | 12.8 (7.3; 19.8) | |
| min; max | 1.8; 17.3 | 2.0; 71.5 | |
| TLG | 0.14 | ||
| mean (±standard deviation) | 57.1 (±49.2) | 174.3 (±196.1) | |
| median (q1;q3) | 47.7 (19.9; 81.7) | 128.4 (45.6; 215.9) | |
| min; max | 8.2; 135.2 | 15.7; 676.8 | |
| FMISO PET | |||
| Suv max | 0.05 | ||
| mean (±standard deviation) | 2.0 (±0.5) | 2.5 (±0.5) | |
| median (q1;q3] | 2.0 (1.8; 2.3] | 2.5 (2.2; 2.7] | |
| min; max | 1.2; 2.6 | 1.8; 3.6 | |
| MRI | |||
| Volume | 0.18 | ||
| mean (±standard deviation) | 18.5 (±22.6) | 45.5 (±50.2) | |
| median (q1;q3] | 8.6 (3.6; 25.5] | 25.5 (12.1; 59.1] | |
| min; max | 1.3; 59.2 | 1.8; 162.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gouel, P.; Callonnec, F.; Obongo-Anga, F.-R.; Bohn, P.; Lévêque, E.; Gensanne, D.; Hapdey, S.; Modzelewski, R.; Vera, P.; Thureau, S. Quantitative MRI to Characterize Hypoxic Tumors in Comparison to FMISO PET/CT for Radiotherapy in Oropharynx Cancers. Cancers 2023, 15, 1918. https://doi.org/10.3390/cancers15061918
Gouel P, Callonnec F, Obongo-Anga F-R, Bohn P, Lévêque E, Gensanne D, Hapdey S, Modzelewski R, Vera P, Thureau S. Quantitative MRI to Characterize Hypoxic Tumors in Comparison to FMISO PET/CT for Radiotherapy in Oropharynx Cancers. Cancers. 2023; 15(6):1918. https://doi.org/10.3390/cancers15061918
Chicago/Turabian StyleGouel, Pierrick, Françoise Callonnec, Franchel-Raïs Obongo-Anga, Pierre Bohn, Emilie Lévêque, David Gensanne, Sébastien Hapdey, Romain Modzelewski, Pierre Vera, and Sébastien Thureau. 2023. "Quantitative MRI to Characterize Hypoxic Tumors in Comparison to FMISO PET/CT for Radiotherapy in Oropharynx Cancers" Cancers 15, no. 6: 1918. https://doi.org/10.3390/cancers15061918