
Deep Learning Approach to Classify Cutaneous Melanoma in a Whole Slide Image


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Cases and Histopathological Records
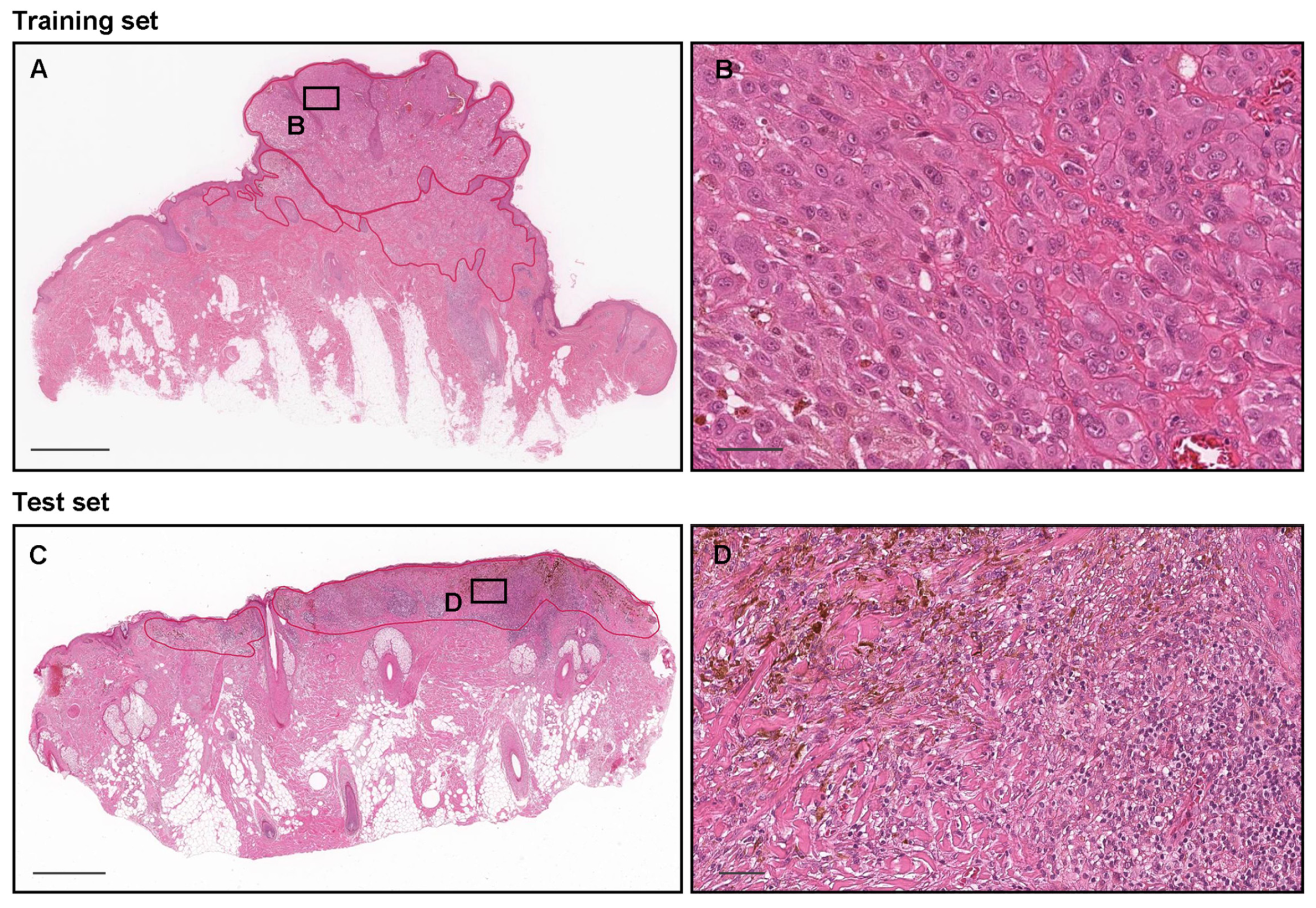
2.2. Annotation
2.3. Deep Learning Models
2.4. Software and Statistical Analysis
3. Results
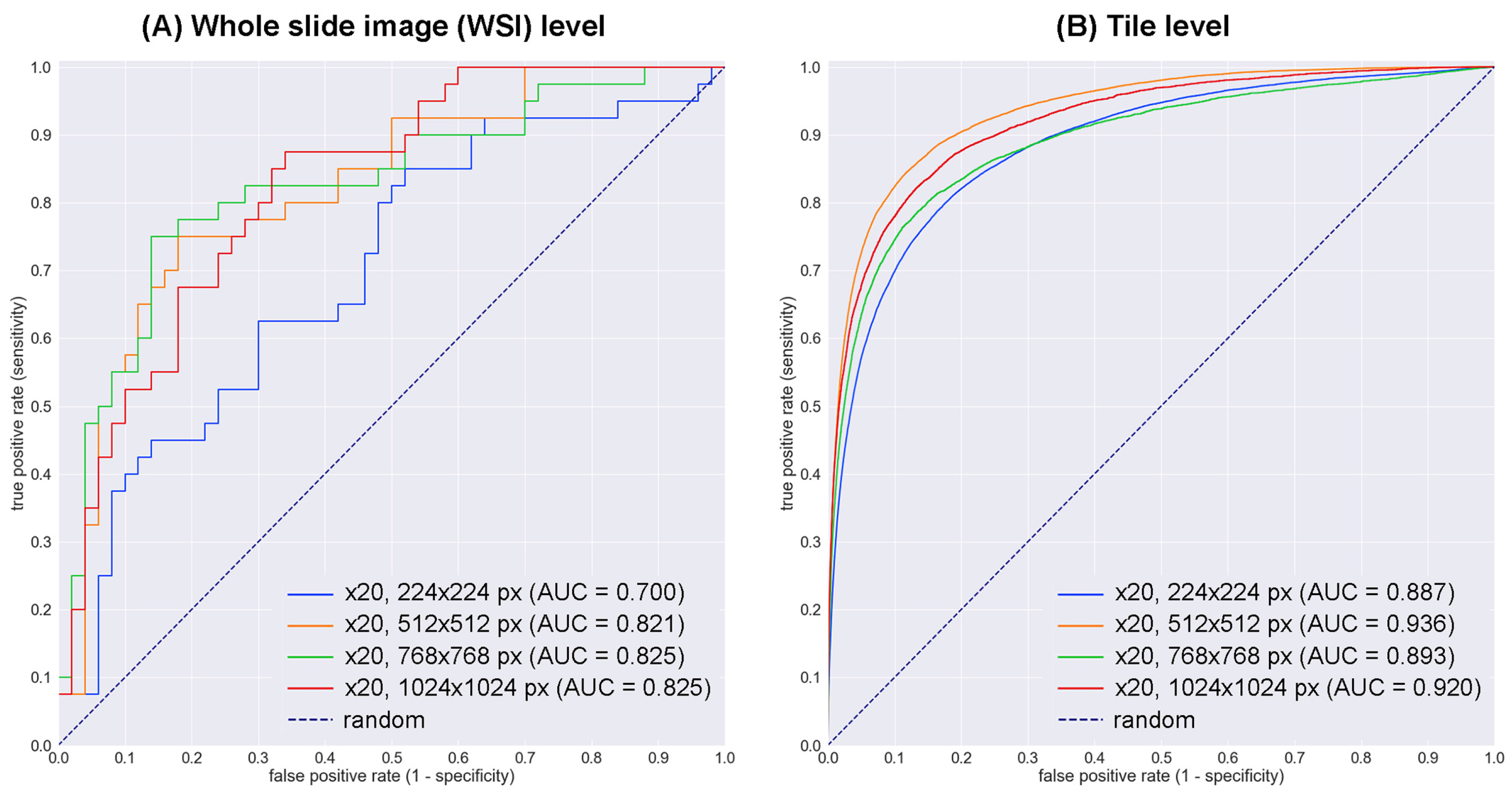
3.1. High ROC–AUC Performance of Melanoma WSI and Tile-Level Evaluation
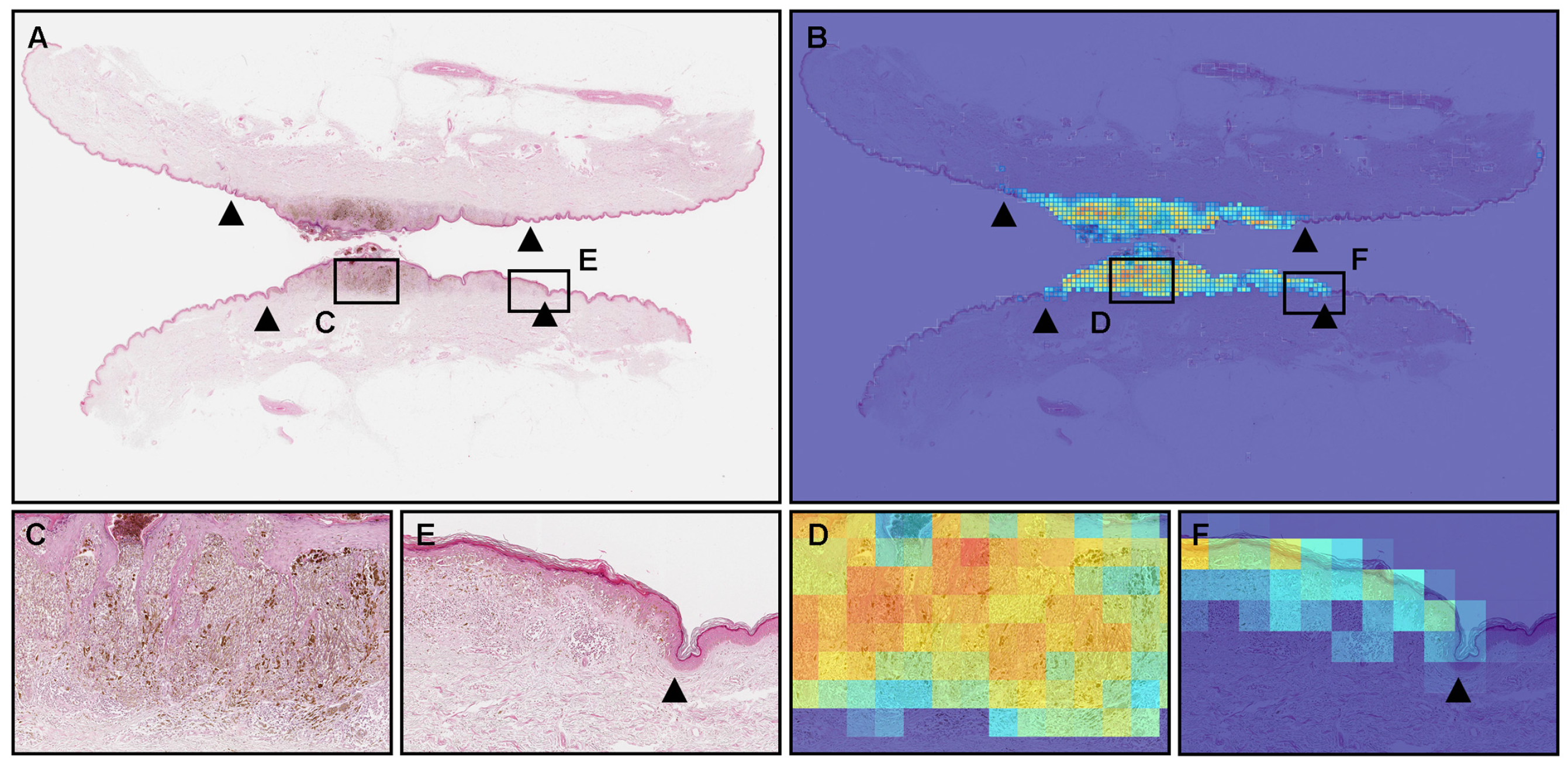
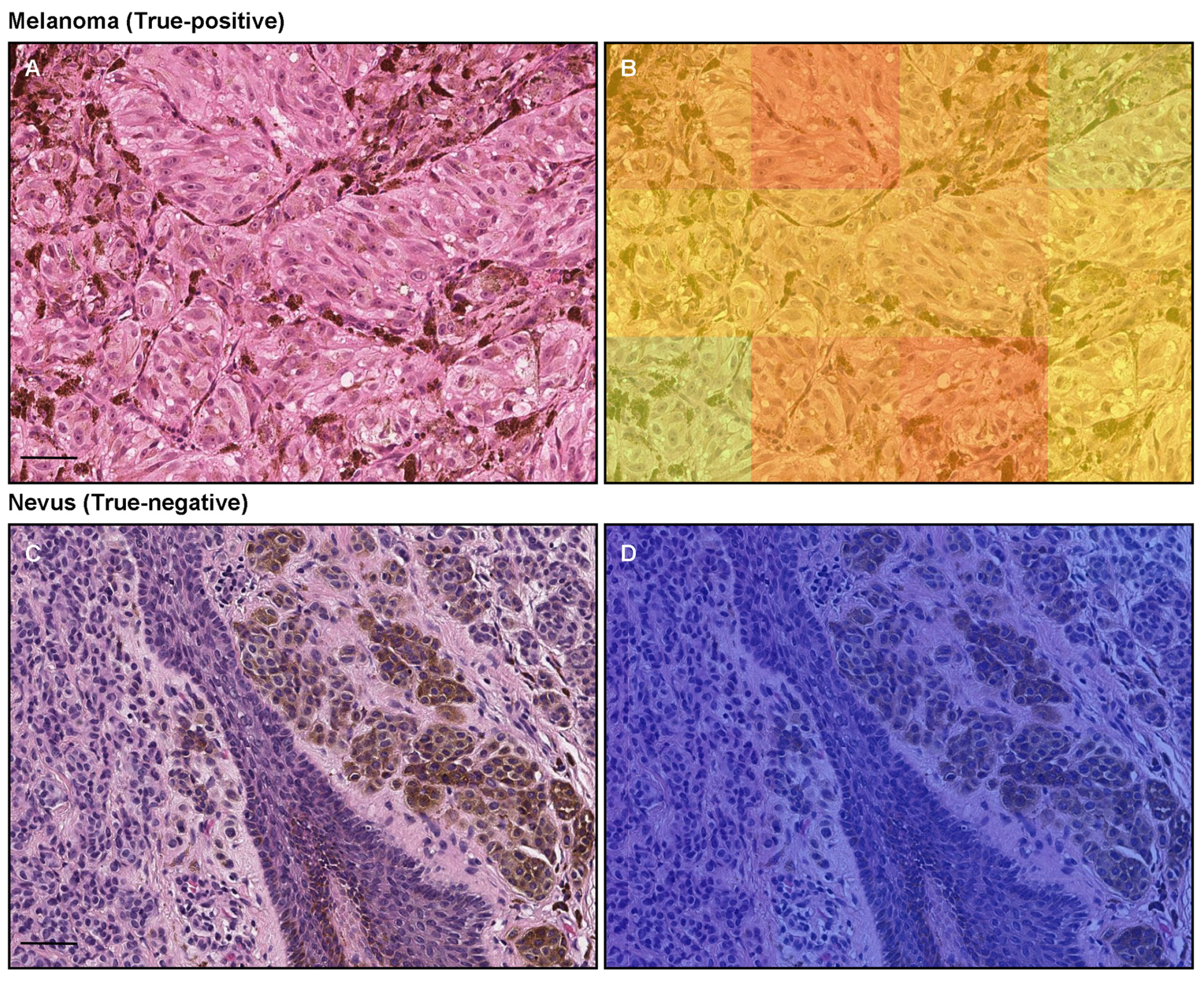
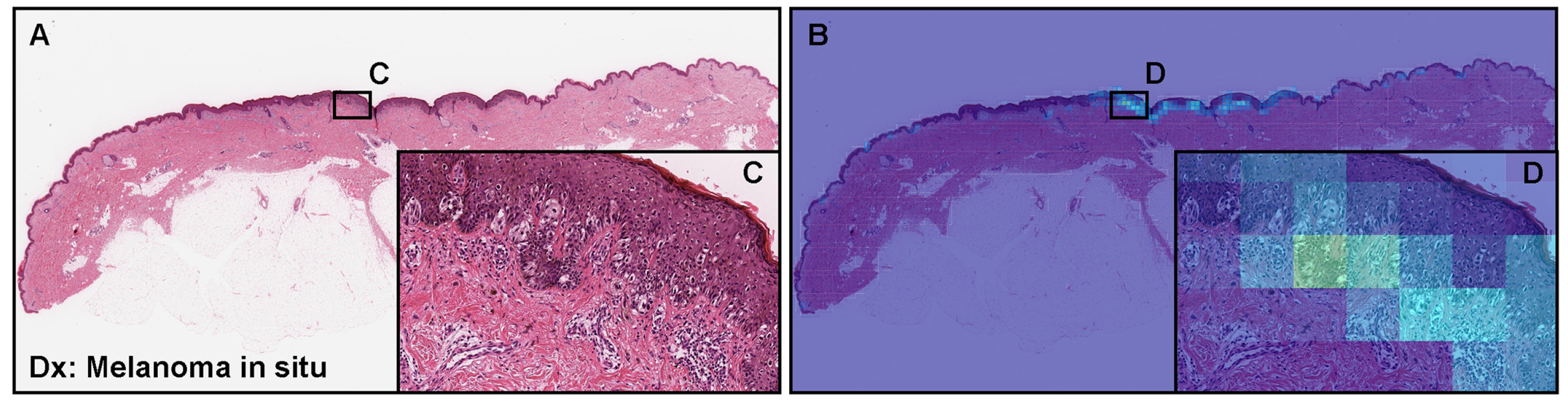
3.2. True Positive Prediction
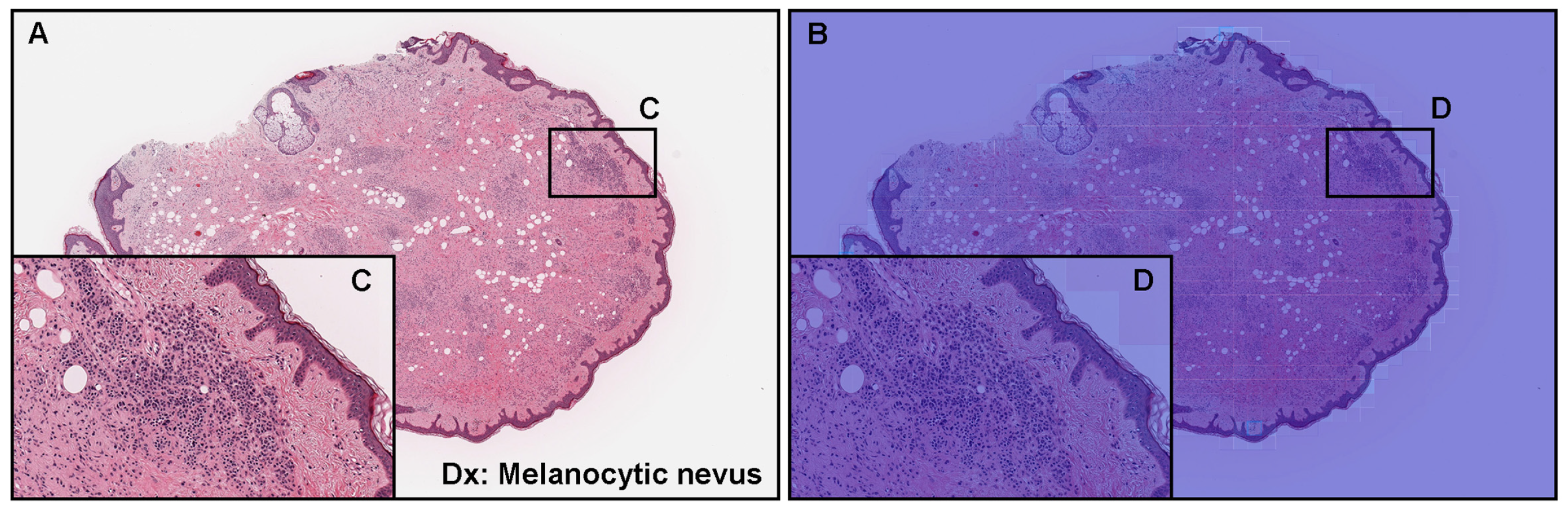
3.3. True Negative Prediction
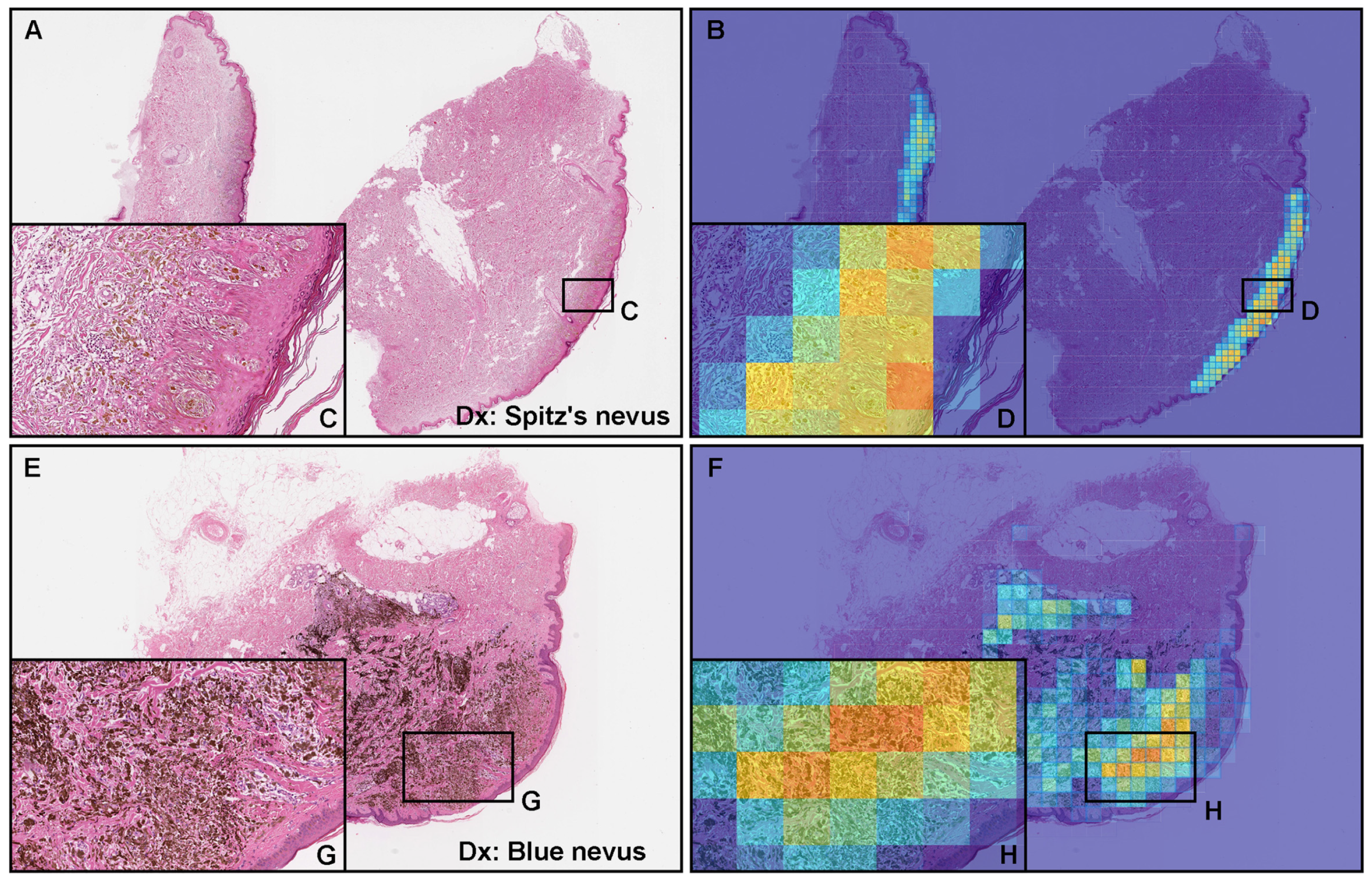
3.4. False Positive Prediction
3.5. False Negative Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Rigel, D.S.; Russak, J.; Friedman, R. The evolution of melanoma diagnosis: 25 years beyond the ABCDs. CA Cancer J. Clin. 2010, 60, 301–316. [Google Scholar] [CrossRef]
- Namikawa, K.; Yamazaki, N. Targeted therapy and immunotherapy for melanoma in Japan. Curr. Treat. Opt. Oncol. 2019, 20, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Tomizuka, T.; Namikawa, K.; Higashi, T. Characteristics of melanoma in Japan: A nationwide registry analysis 2011–2013. Melanoma Res. 2017, 27, 492–497. [Google Scholar] [CrossRef]
- Dessinioti, C.; Geller, A.C.; Stratigos, A.J. A review of nevus-associated melanoma: What is the evidence? J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1927–1936. [Google Scholar] [CrossRef]
- Skender-Kalnenas, T.M.; English, D.R.; Heenan, P.J. Benign melanocytic lesions: Risk markers or precursors of cutaneous melanoma? J. Am. Acad. Dermatol. 1995, 33, 1000–1007. [Google Scholar] [CrossRef]
- Saida, T. Histogenesis of cutaneous malignant melanoma: The vast majority do not develop from melanocytic nevus but arise de novo as melanoma in situ. J. Dermatol. 2019, 46, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.L. Histopathologic and molecular diagnosis of melanoma. Clin. Plast. Surg. 2021, 48, 587–598. [Google Scholar] [CrossRef]
- Barnhill, R.; Mihm, M., Jr. The histopathology of cutaneous malignant melanoma. Semin. Diagn. Pathol. 1993, 10, 47–75. [Google Scholar]
- Banerjee, S.S.; Harris, M. Morphological and immunophenotypic variations in malignant melanoma. Histopathology 2000, 36, 387–402. [Google Scholar] [CrossRef]
- Magro, C.M.; Crowson, A.N.; Mihm, M.C. Unusual variants of malignant melanoma. Mod. Pathol. 2006, 19, S41–S70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, A.S.; Wu, H.; Shyr, Y. Monster cells in malignant melanoma. Am. J. Dermatopathol. 2005, 27, 208–210. [Google Scholar] [CrossRef]
- Hanson, I.; Banerjee, S.S.; Menasce, L.P.; Prescott, R. A study of eleven cutaneous malignant melanomas in adults with small-cell morphology: Emphasis on diagnostic difficulties and unusual features. Histopathology 2002, 40, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Al-Talib, R.; Theaker, J. Signet-ring cell melanoma: Light microscopic, immunohistochemical and ultrastructural features. Histopathology 1991, 18, 572–575. [Google Scholar] [CrossRef]
- Sheibani, K.; Battifora, H. Signet-ring cell melanoma: A rare morphologic variant of malignant melanoma. Am. J. Surg. Pathol. 1988, 12, 28–34. [Google Scholar] [CrossRef]
- Abbott, J.J.; Amirkhan, R.H.; Hoang, M.P. Malignant melanoma with a rhabdoid phenotype: Histologic, immunohistochemical, and ultrastructural study of a case and review of the literature. Arch. Pathol. Lab. Med. 2004, 128, 686–688. [Google Scholar] [CrossRef]
- Borek, B.T.; McKee, P.H.; Freeman, J.A.; Maguire, B.; Brander, W.L.; Calonje, E. Primary malignant melanoma with rhabdoid features: A histologic and immunocytochemical study of three cases. Am. J. Dermatopathol. 1998, 20, 123–127. [Google Scholar] [CrossRef]
- Chang, E.S.; Wick, M.R.; Swanson, P.E.; Dehner, L.P. Metastatic malignant melanoma with “rhabdoid” features. Am. J. Clin. Pathol. 1994, 102, 426–431. [Google Scholar] [CrossRef]
- Kao, G.F.; Helwig, E.B.; Graham, J.H. Balloon cell malignant melanoma of the skin. A clinicopathologic study of 34 cases with histochemical, immunohistochemical, and ultrastructural observations. Cancer 1992, 69, 2942–2952. [Google Scholar] [CrossRef]
- Gong, H.Z.; Zheng, H.Y.; Li, J. Amelanotic melanoma. Melanoma Res. 2019, 29, 221–230. [Google Scholar] [CrossRef]
- Waqar, S.; George, S.; Jean-Baptiste, W.; Ali, A.Y.; Inyang, B.; Koshy, F.S.; George, K.; Poudel, P.; Chalasani, R.; Goonathilake, M.R.; et al. Recognizing Histopathological Simulators of Melanoma to Avoid Misdiagnosis. Cureus 2022, 14, e26127. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S.; Feldman, M.D.; Abels, E.; Ashfaq, R.; Beltaifa, S.; Cacciabeve, N.G.; Cathro, H.P.; Cheng, L.; Cooper, K.; Dickey, G.E.; et al. Whole slide imaging versus microscopy for primary diagnosis in surgical pathology: A multicenter blinded randomized noninferiority study of 1992 cases (pivotal study). Am. J. Surg. Pathol. 2018, 42, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malarkey, D.E.; Willson, G.A.; Willson, C.J.; Adams, E.T.; Olson, G.R.; Witt, W.M.; Elmore, S.A.; Hardisty, J.F.; Boyle, M.C.; Crabbs, T.A.; et al. Utilizing whole slide images for pathology peer review and working groups. Toxicol. Pathol. 2015, 43, 1149–1157. [Google Scholar] [CrossRef] [Green Version]
- Tsuneki, M. Deep learning models in medical image analysis. J. Oral Biosci. 2022, 64, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Snyder, A.N.; Zhang, D.; Dreesen, S.L.; Baltimore, C.A.; Lopez-Garcia, D.R.; Akers, J.Y.; Metts, C.L.; Madory, J.E.; Chang, P.D.; Doan, L.T.; et al. Histologic Screening of Malignant Melanoma, Spitz, Dermal and Junctional Melanocytic Nevi Using a Deep Learning Model. Am. J. Dermatopathol. 2022, 44, 650–657. [Google Scholar] [CrossRef]
- Alheejawi, S.; Berendt, R.; Jha, N.; Maity, S.P.; Mandal, M. Detection of malignant melanoma in H&E-stained images using deep learning techniques. Tissue Cell 2021, 73, 101659. [Google Scholar] [CrossRef]
- Kanavati, F.; Toyokawa, G.; Momosaki, S.; Rambeau, M.; Kozuma, Y.; Shoji, F.; Yamazaki, K.; Takeo, S.; Iizuka, O.; Tsuneki, M. Weakly-supervised learning for lung carcinoma classification using deep learning. Sci. Rep. 2020, 10, 9297. [Google Scholar] [CrossRef]
- Abadi, M.; Agarwal, A.; Barham, P.; Brevdo, E.; Chen, Z.; Citro, C.; Corrado, G.S.; Davis, A.; Dean, J.; Devin, M.; et al. TensorFlow: Large-Scale Machine Learning on Heterogeneous Systems. 2015. Available online: https:///www.tensorflow.org (accessed on 2 March 2021).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; CRC Press: Boca Raton, FL, USA, 1994. [Google Scholar]
- Yeh, I.; Busam, K.J. Spitz melanocytic tumours—A review. Histopathology 2022, 80, 122–134. [Google Scholar] [CrossRef]
- Kamino, H. Spitzoid melanoma. Clin. Dermatol. 2009, 27, 545–555. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S.W.; Scolyer, R.A. Pitfalls and important issues in the pathologic diagnosis of melanocytic tumors. Ochsner J. 2010, 10, 66–74. [Google Scholar] [PubMed]
- Gonzalez-Campora, R.; Galera-Davidson, H.; Vazquez-Ramirez, F.; Diaz-Cano, S. Blue nevus: Classical types and new related entities: A differential diagnostic review. Pathol.-Res. Pract. 1994, 190, 627–635. [Google Scholar] [CrossRef]
- Busam, K.J. Metastatic melanoma to the skin simulating blue nevus. Am. J. Surg. Pathol. 1999, 23, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Wieselthier, J.S.; White, W.L. Cutaneous metastasis of ocular malignant melanoma: An unusual presentation simulating blue nevi. Am. J. Dermatopathol. 1996, 18, 289–295. [Google Scholar] [CrossRef]
- Cook, M.; Robertson, I. Melanocytic dysplasia and melanoma. Histopathology 1985, 9, 647–658. [Google Scholar] [CrossRef]
- McGovern, V.J.; Shaw, H.; Milton, G. Histogenesis of malignant melanoma with an adjacent component of the superficial spreading type. Pathology 1985, 17, 251–254. [Google Scholar] [CrossRef]
- Okamura, J.M.; Barr, R.J.; Cantos, K.A. Benign atypical junctional melanocytic hyperplasia associated with intradermal nevi: A common finding that may be confused with melanoma in situ. Mod. Pathol. 2000, 13, 857–860. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subtype | Site | WSI | Subtype | Site | WSI |
|---|---|---|---|---|---|
| Melanoma in-situ | Head and neck | 4 | NOS | Head and neck | 3 |
| Upper extremity | 4 | Trunk | 3 | ||
| Lower extremity | 6 | Upper extremity | 2 | ||
| Nodular | Head and neck | 3 | Lower extremity | 3 | |
| Trunk | 5 | Amelanotic | Head and neck | 4 | |
| Upper extremity | 7 | Trunk | 3 | ||
| Lower extremity | 8 | Upper extremity | 5 | ||
| Lentigo maligna | Head and neck | 5 | Lower extremity | 4 | |
| Upper extremity | 1 | ||||
| Superficial spreading | Head and neck | 2 | |||
| Trunk | 3 | ||||
| Upper extremity | 2 | ||||
| Lower extremity | 1 |
| Subtype | Site | WSI | Subtype | Site | WSI |
|---|---|---|---|---|---|
| Compound nevus | Head and neck | 6 | Spitz’s nevus | Head and neck | 5 |
| Trunk | 4 | Lower extremity | 1 | ||
| Upper extremity | 6 | Congenital nevus | Head and neck | 1 | |
| Lower extremity | 5 | Upper extremity | 1 | ||
| Junctional nevus | Head and neck | 5 | Normal skin | Head and neck | 3 |
| Trunk | 3 | Trunk | 3 | ||
| Upper extremity | 5 | Upper extremity | 4 | ||
| Lower extremity | 4 | Lower extremity | 3 | ||
| Intradermal nevus | Head and neck | 3 | Non-melanocytic benign | Head and neck | 3 |
| Trunk | 1 | Trunk | 4 | ||
| Upper extremity | 2 | Upper extremity | 3 | ||
| Lower extremity | 3 | Lower extremity | 4 | ||
| Blue nevus | Head and neck | 2 | |||
| Trunk | 1 | ||||
| Upper extremity | 1 | ||||
| Lower extremity | 2 |
| Melanoma | Non-Melanoma | |
|---|---|---|
| Training | 33 | 33 |
| Validation | 5 | 5 |
| Test | 40 | 50 |
| Total | 78 | 88 |
| Evaluation | ||
|---|---|---|
| WSI Level | Tile Level | |
| ×20, 224 × 224 px | ||
| ROC–AUC | 0.700 [0.587–0.808] | 0.887 [0.885–0.890] |
| Log-loss | 0.666 [0.642–0.686] | 0.328 [0.327–0.329] |
| Accuracy | 0.644 [0.544–0.744] | 0.833 [0.831–0.837] |
| Sensitivity | 0.850 [0.705–0.933] | 0.788 [0.783–0.793] |
| Specificity | 0.480 [0.366–0.647] | 0.835 [0.834–0.837] |
| ×20, 512 × 512 px | ||
| ROC–AUC | 0.821 [0.712–0.890] | 0.936 [0.935–0.938] |
| Log-loss | 0.532 [0.472–0.618] | 0.151 [0.149–0.153] |
| Accuracy | 0.778 [0.667–0.844] | 0.881 [0.880–0.882] |
| Sensitivity | 0.725 [0.538–0.844] | 0.844 [0.839–0.849] |
| Specificity | 0.820 [0.691–0.902] | 0.883 [0.882–0.884] |
| ×20, 768 × 768 px | ||
| ROC–AUC | 0.825 [0.763–0.930] | 0.893 [0.888–0.898] |
| Log-loss | 0.568 [0.435–0.651] | 0.171 [0.165–0.174] |
| Accuracy | 0.811 [0.767–0.911] | 0.860 [0.858–0.862] |
| Sensitivity | 0.750 [0.667–0.920] | 0.786 [0.777–0.798] |
| Specificity | 0.860 [0.786–0.964] | 0.865 [0.863–0.867] |
| ×20, 1024 × 1024 px | ||
| ROC–AUC | 0.825 [0.752–0.916] | 0.920 [0.918–0.924] |
| Log-loss | 0.577 [0.383–0.704] | 0.186 [0.180–0.192] |
| Accuracy | 0.756 [0.667–0.844] | 0.863 [0.860–0.865] |
| Sensitivity | 0.875 [0.755–0.961] | 0.823 [0.817–0.835] |
| Specificity | 0.660 [0.523–0.800] | 0.865 [0.863–0.868] |
| WSI Level | Tile Level | ||||
|---|---|---|---|---|---|
| Predicted Label | Predicted Label | ||||
| Melanoma | Non-Melanoma | Melanoma | Non-Melanoma | ||
| ×20, 224 × 224 px | |||||
| True label | Melanoma | 34 | 6 | 22,241 | 5990 |
| Non-melanoma | 26 | 24 | 70,527 | 358,037 | |
| ×20, 512 × 512 px | |||||
| True label | Melanoma | 29 | 11 | 18,706 | 3471 |
| Non-melanoma | 9 | 41 | 39,055 | 294,926 | |
| ×20, 768 × 768 px | |||||
| True label | Melanoma | 30 | 10 | 1287 | 653 |
| Non-melanoma | 7 | 43 | 46,007 | 38,460 | |
| ×20, 1024 × 1024 px | |||||
| True label | Melanoma | 35 | 5 | 5621 | 1206 |
| Non-melanoma | 17 | 33 | 12,996 | 83,448 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Abe, M.; Nakano, S.; Tsuneki, M. Deep Learning Approach to Classify Cutaneous Melanoma in a Whole Slide Image. Cancers 2023, 15, 1907. https://doi.org/10.3390/cancers15061907
Li M, Abe M, Nakano S, Tsuneki M. Deep Learning Approach to Classify Cutaneous Melanoma in a Whole Slide Image. Cancers. 2023; 15(6):1907. https://doi.org/10.3390/cancers15061907
Chicago/Turabian StyleLi, Meng, Makoto Abe, Shigeo Nakano, and Masayuki Tsuneki. 2023. "Deep Learning Approach to Classify Cutaneous Melanoma in a Whole Slide Image" Cancers 15, no. 6: 1907. https://doi.org/10.3390/cancers15061907