
Pancreatic Cancer Surveillance in Carriers of a Germline Pathogenic Variant in CDKN2A
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
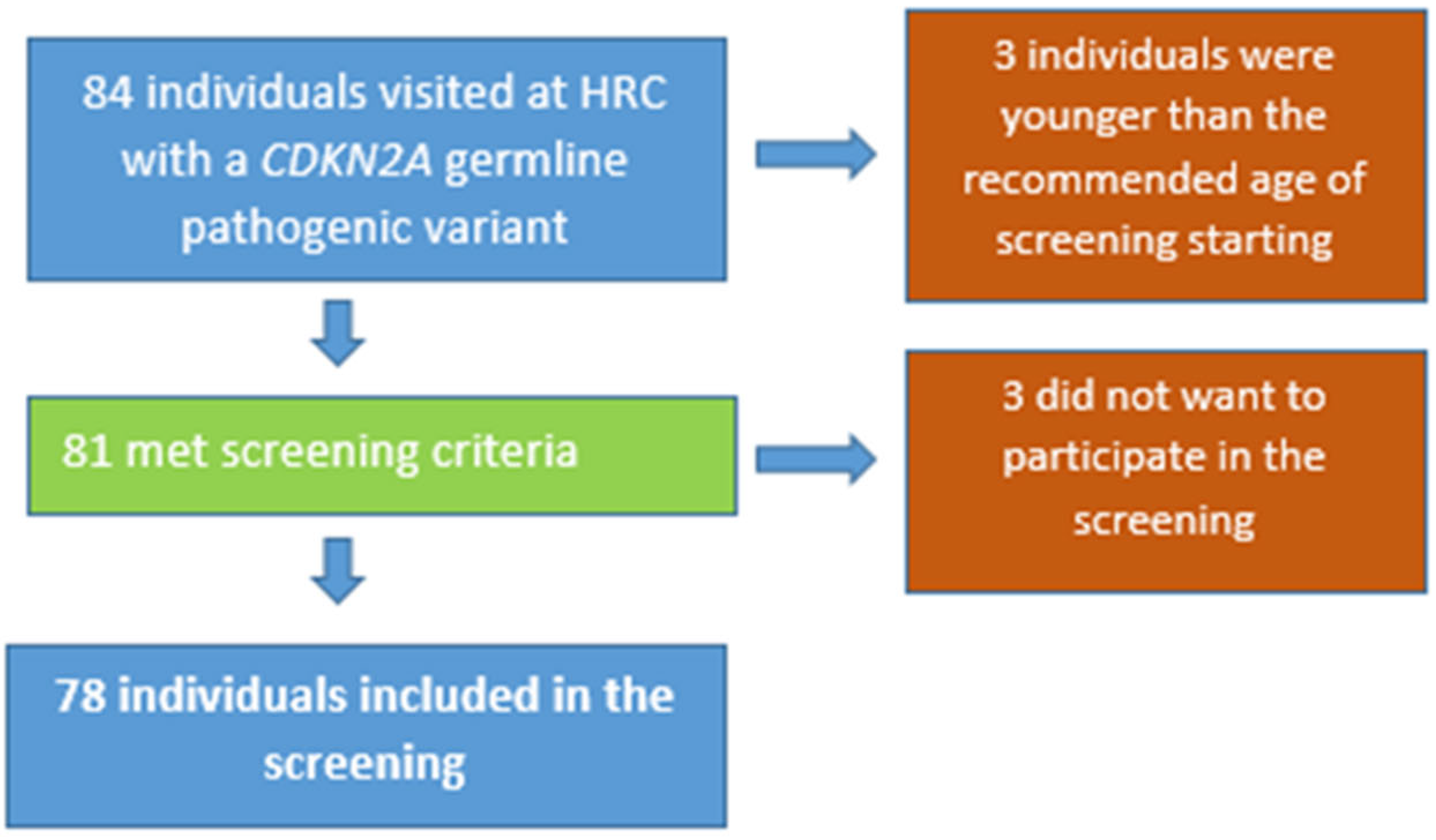
2.1. Study Population
2.2. Definition of Surveillance Program
2.3. Data Recording
- -
- Personal data such as age, gender, alcohol consumption (current consumption of >14 units/week; former drinkers (>10 years) were not considered), smoking habits (current or former, with at least 5 pack-years of smoking), and comorbidities were included, as well as oncologic personal history. If PDAC: location, histology, treatment performed (surgery, radiotherapy, chemotherapy), “TNM” stage, survival, recurrence, cause of death;
- -
- Molecular data: genetic study (description of pathogenic variant);
- -
- Family history of cancer (digestive and extra-digestive neoplasms, type of cancer, age and degree of relationship);
- -
- PDAC surveillance: type of test (EUS or MRI), periodicity, findings (normal, preneoplastic lesions, cancer);
- -
- Definition of pancreatic lesions:
- (a)
- High-risk pancreatic lesions [24]:
- (b)
- PDAC
- (c)
- Others (nonspecific lesions): IPMN o mucinous cystic neoplasm without high-risk criteria, nonspecific cyst, main pancreatic duct dilatation ≥10 mm, neuroendocrine tumor.
2.4. Statistical Methods for Data Analysis
3. Results
3.1. General Characteristics
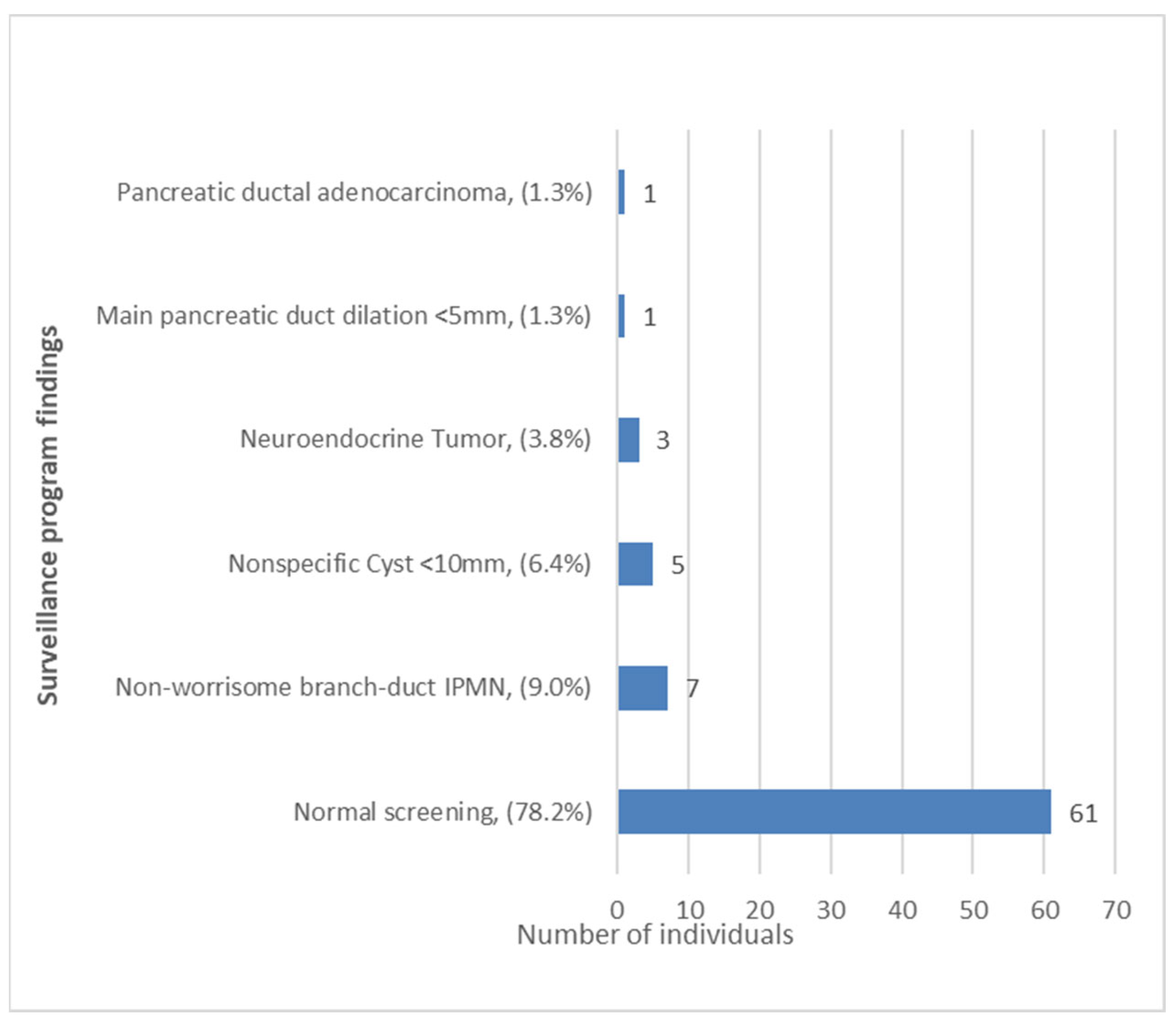
3.2. Pancreatic Cancer Surveillance Program: Characteristics and Findings
3.3. Risk Factors Associated with PDAC and Preneoplastic Lesions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Welinsky, S.; Lucas, A.L. Familial Pancreatic Cancer and the Future of Directed Screening. Gut Liver 2017, 11, 761–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, A.E.; Hernandez, Y.G.; Frucht, H.; Lucas, A.L. Pancreatic ductal adenocarcinoma: Risk factors, screening, and early detection. World J. Gastroenterol. 2014, 20, 11182–11198. [Google Scholar] [CrossRef]
- Llach, J.; Carballal, S.; Moreira, L. Familial Pancreatic Cancer: Current Perspectives. Cancer Manag. Res. 2020, 12, 743–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lier, M.G.; Wagner, A.; Mathus-Vliegen, E.M.; Kuipers, E.J.; Steyerberg, E.W.; van Leerdam, M.E. High cancer risk in Peutz-Jeghers syndrome: A systematic review and surveillance recommendations. Am. J. Gastroenterol. 2010, 105, 1258–1264, author reply 65. [Google Scholar] [CrossRef]
- De Snoo, F.A.; Bishop, D.T.; Bergman, W.; van Leeuwen, I.; van der Drift, C.; van Nieuwpoort, F.A.; Out-Luiting, C.J.; Vasen, H.F.; ter Huurne, J.A.; Frants, R.R.; et al. Increased risk of cancer other than melanoma in CDKN2A founder mutation (p16-Leiden)-positive melanoma families. Clin. Cancer Res. 2008, 14, 7151–7157. [Google Scholar] [CrossRef] [Green Version]
- Goggins, M.; Schutte, M.; Lu, J.; Moskaluk, C.A.; Weinstein, C.L.; Petersen, G.M.; Yeo, C.J.; Jackson, C.E.; Lynch, H.T.; Hruban, R.H.; et al. Germline BRCA2 gene mutations in patients with apparently sporadic pancreatic carcinomas. Cancer Res. 1996, 56, 5360–5364. [Google Scholar]
- Giardiello, F.M.; Offerhaus, G.J.; Lee, D.H.; Krush, A.J.; Tersmette, A.C.; Booker, S.V.; Kelley, N.C.; Hamilton, S.R. Increased risk of thyroid and pancreatic carcinoma in familial adenomatous polyposis. Gut 1993, 34, 1394–1396. [Google Scholar] [CrossRef] [Green Version]
- Kastrinos, F.; Mukherjee, B.; Tayob, N.; Wang, F.; Sparr, J.; Raymond, V.M.; Bandipalliam, P.; Stoffel, E.M.; Gruber, S.B.; Syngal, S. Risk of pancreatic cancer in families with Lynch syndrome. JAMA 2009, 302, 1790–1795. [Google Scholar] [CrossRef]
- Roberts, N.J.; Norris, A.L.; Petersen, G.M.; Bondy, M.L.; Brand, R.; Gallinger, S.; Kurtz, R.C.; Olson, S.H.; Rustgi, A.K.; Schwartz, A.G.; et al. Whole Genome Sequencing Defines the Genetic Heterogeneity of Familial Pancreatic Cancer. Cancer Discov. 2016, 6, 166–175. [Google Scholar] [CrossRef] [Green Version]
- Roberts, N.J.; Jiao, Y.; Yu, J.; Kopelovich, L.; Petersen, G.M.; Bondy, M.L.; Gallinger, S.; Schwartz, A.G.; Syngal, S.; Cote, M.L.; et al. ATM mutations in patients with hereditary pancreatic cancer. Cancer Discov. 2012, 2, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Lynch, H.T.; Fusaro, R.M.; Lynch, J.F.; Brand, R. Pancreatic cancer and the FAMMM syndrome. Fam. Cancer 2008, 7, 103–112. [Google Scholar] [CrossRef]
- Bishop, D.T.; Demenais, F.; Goldstein, A.M.; Bergman, W.; Bishop, J.N.; Bressac-de Paillerets, B.; Chompret, A.; Ghiorzo, P.; Gruis, N.; Hansson, J.; et al. Geographical variation in the penetrance of CDKN2A mutations for melanoma. J. Natl. Cancer Inst. 2002, 94, 894–903. [Google Scholar] [CrossRef] [Green Version]
- Ohtani, N.; Zebedee, Z.; Huot, T.J.G.; Stinson, J.A.; Sugimoto, M.; Ohashi, Y.; Sharrocks, A.D.; Peters, G.; Hara, E. Opposing effects of Ets and Id proteins on p16INK4a expression during cellular senescence. Nature 2001, 409, 1067–1070. [Google Scholar] [CrossRef]
- Lu, C.; Xu, C.F.; Wan, X.Y.; Zhu, H.T.; Yu, C.H.; Li, Y.M. Screening for pancreatic cancer in familial high-risk individuals: A systematic review. World J. Gastroenterol. 2015, 21, 8678–8686. [Google Scholar] [CrossRef]
- Canto, M.I.; Almario, J.A.; Schulick, R.D.; Yeo, C.J.; Klein, A.; Blackford, A.; Shin, E.J.; Sanyal, A.; Yenokyan, G.; Lennon, A.M.; et al. Risk of Neoplastic Progression in Individuals at High Risk for Pancreatic Cancer Undergoing Long-term Surveillance. Gastroenterology 2018, 155, 740–751.e2. [Google Scholar] [CrossRef] [Green Version]
- Canto, M.I.; Harinck, F.; Hruban, R.H.; Offerhaus, G.J.; Poley, J.-W.; Kamel, I.; Nio, Y.; Schulick, R.S.; Bassi, C.; Kluijt, I.; et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013, 62, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Goggins, M.; Overbeek, K.A.; Brand, R.; Syngal, S.; Del Chiaro, M.; Bartsch, D.K.; Bassi, C.; Carrato, A.; Farrell, J.; Fishman, E.K.; et al. Management of patients with increased risk for familial pancreatic cancer: Updated recommendations from the International Cancer of the Pancreas Screening (CAPS) Consortium. Gut 2020, 69, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Overbeek, K.A.; Levink, I.J.M.; Koopmann, B.D.M.; Harinck, F.; Konings, I.C.A.W.; Ausems, M.G.E.M.; Wagner, A.; Fockens, P.; van Eijck, C.H.; Koerkamp, B.G.; et al. Long-term yield of pancreatic cancer surveillance in high-risk individuals. Gut 2021, 71, 1152–1160. [Google Scholar] [CrossRef]
- Vasen, H.; Ibrahim, I.; Ponce, C.G.; Slater, E.P.; Matthäi, E.; Carrato, A.; Earl, J.; Robbers, K.; van Mil, A.M.; Potjer, T.; et al. Benefit of Surveillance for Pancreatic Cancer in High-Risk Individuals: Outcome of Long-Term Prospective Follow-Up Studies from Three European Expert Centers. J. Clin. Oncol. 2016, 34, 2010–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klatte, D.C.; Boekestijn, B.; Wasser, M.N.; Shahbazi, S.F.; Ibrahim, I.S.; Mieog, J.S.D.; Luelmo, S.A.; Morreau, H.; Potjer, T.P.; Inderson, A.; et al. Pancreatic Cancer Surveillance in Carriers of a Germline. J. Clin. Oncol. 2022, 40, 3267–3277. [Google Scholar] [CrossRef] [PubMed]
- Vangala, D.B.; Cauchin, E.; Balmaña, J.; Wyrwicz, L.; van Cutsem, E.; Güller, U.; Castells, A.; Carneiro, F.; Hammel, P.; Ducreux, M.; et al. Screening and surveillance in hereditary gastrointestinal cancers: Recommendations from the European Society of Digestive Oncology (ESDO) expert discussion at the 20th European Society for Medical Oncology (ESMO)/World Congress on Gastrointestinal Cancer, Barcelona, June 2018. Eur. J. Cancer 2018, 104, 91–103. [Google Scholar] [PubMed]
- European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms. Gut 2018, 67, 789–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoita, A.; Penman, I.D.; Williams, D.B. Review of screening for pancreatic cancer in high risk individuals. World J. Gastroenterol. 2011, 17, 2365–2371. [Google Scholar] [CrossRef]
- Kuo, E.J.; Salem, R.R. Population-level analysis of pancreatic neuroendocrine tumors 2 cm or less in size. Ann. Surg. Oncol. 2013, 20, 2815–2821. [Google Scholar] [CrossRef]
- Zhang, X.M.; Mitchell, D.G.; Dohke, M.; Holland, G.A.; Parker, L. Pancreatic cysts: Depiction on single-shot fast spin-echo MR images. Radiology 2002, 223, 547–553. [Google Scholar] [CrossRef]
- Kimura, W.; Nagai, H.; Kuroda, A.; Muto, T.; Esaki, Y. Analysis of small cystic lesions of the pancreas. Int. J. Pancreatol. 1995, 18, 197–206. [Google Scholar] [CrossRef]
- Overbeek, K.A.; Goggins, M.G.; Dbouk, M.; Levink, I.J.; Koopmann, B.D.; Chuidian, M.; Konings, I.C.; Paiella, S.; Earl, J.; Fockens, P.; et al. Timeline of Development of Pancreatic Cancer and Implications for Successful Early Detection in High-Risk Individuals. Gastroenterology 2022, 162, 772–785.e4. [Google Scholar] [CrossRef]
- Ho, A.S.; Huang, X.; Cao, H.; Christman-Skieller, C.; Bennewith, K.; Le, Q.-T.; Koong, A.C. Circulating miR-210 as a Novel Hypoxia Marker in Pancreatic Cancer. Transl. Oncol. 2010, 3, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Chhoda, A.; Lu, L.; Clerkin, B.M.; Risch, H.; Farrell, J.J. Current Approaches to Pancreatic Cancer Screening. Am. J. Pathol. 2019, 189, 22–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics of the Individuals Included (N = 78) | |
|---|---|
| Median age (years) at first test (median, IQR) | 53 (47–63) |
| Female, n (%) | 46 (59.0%) |
| Smoking habit (former or current smoker), n (%) | 31 (39.7%) |
| Alcohol consumption, n (%) | 5 (6.4%) |
| Diabetes mellitus type 2, n (%) | 7 (9.0%) |
Family history of PDAC, n (%)
| 17 (21.8%) 5 (6.4%) 12 (15.4%) |
Personal history of cancer
| 56 (71.8%) 2 (2.6%) 2 (2.6%) 1 (1.3%) 1 (1.3%) |
| Lesions Detected at the Surveillance Program (n = 17) | Test Performed During Follow-Up | Test that Detected the Lesion | ||
|---|---|---|---|---|
| EUS | MRI | EUS | MRI | |
| Main pancreatic duct dilation (5 mm) | Yes | Yes | Yes | No |
| IPMN | Yes | Yes | Yes | Yes |
| IPMN | Yes | Yes | Yes | Yes |
| IPMN | No | Yes | Not performed | Yes |
| IPMN | Yes | No | Yes | Not performed |
| IPMN | Yes | No | Yes | Not performed |
| IPMN | Yes | Yes | Yes | Yes |
| IPMN | Yes | Yes | Yes | No |
| Neuroendocrine tumor | Yes | Yes | Yes | No |
| Neuroendocrine tumor | Yes | Yes | Yes | Yes |
| Neuroendocrine tumor | Yes | Yes | Yes | Yes |
| Pancreatic cancer | Yes | No | Yes | Not performed |
| Nonspecific cyst | Yes | Yes | Yes | No |
| Nonspecific cyst | Yes | No | Yes | Not performed |
| Nonspecific cyst | Yes | Yes | Yes | Yes |
| Nonspecific cyst | Yes | No | Yes | Not performed |
| Nonspecific cyst | Yes | No | Yes | Not performed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llach, J.; Aguilera, P.; Sánchez, A.; Ginès, A.; Fernández-Esparrach, G.; Soy, G.; Sendino, O.; Vaquero, E.; Carballal, S.; Ausania, F.; et al. Pancreatic Cancer Surveillance in Carriers of a Germline Pathogenic Variant in CDKN2A. Cancers 2023, 15, 1690. https://doi.org/10.3390/cancers15061690
Llach J, Aguilera P, Sánchez A, Ginès A, Fernández-Esparrach G, Soy G, Sendino O, Vaquero E, Carballal S, Ausania F, et al. Pancreatic Cancer Surveillance in Carriers of a Germline Pathogenic Variant in CDKN2A. Cancers. 2023; 15(6):1690. https://doi.org/10.3390/cancers15061690
Chicago/Turabian StyleLlach, Joan, Paula Aguilera, Ariadna Sánchez, Angels Ginès, Glòria Fernández-Esparrach, Guillem Soy, Oriol Sendino, Eva Vaquero, Sabela Carballal, Fabio Ausania, and et al. 2023. "Pancreatic Cancer Surveillance in Carriers of a Germline Pathogenic Variant in CDKN2A" Cancers 15, no. 6: 1690. https://doi.org/10.3390/cancers15061690