
Multimodal Deep Learning-Based Prognostication in Glioma Patients: A Systematic Review
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
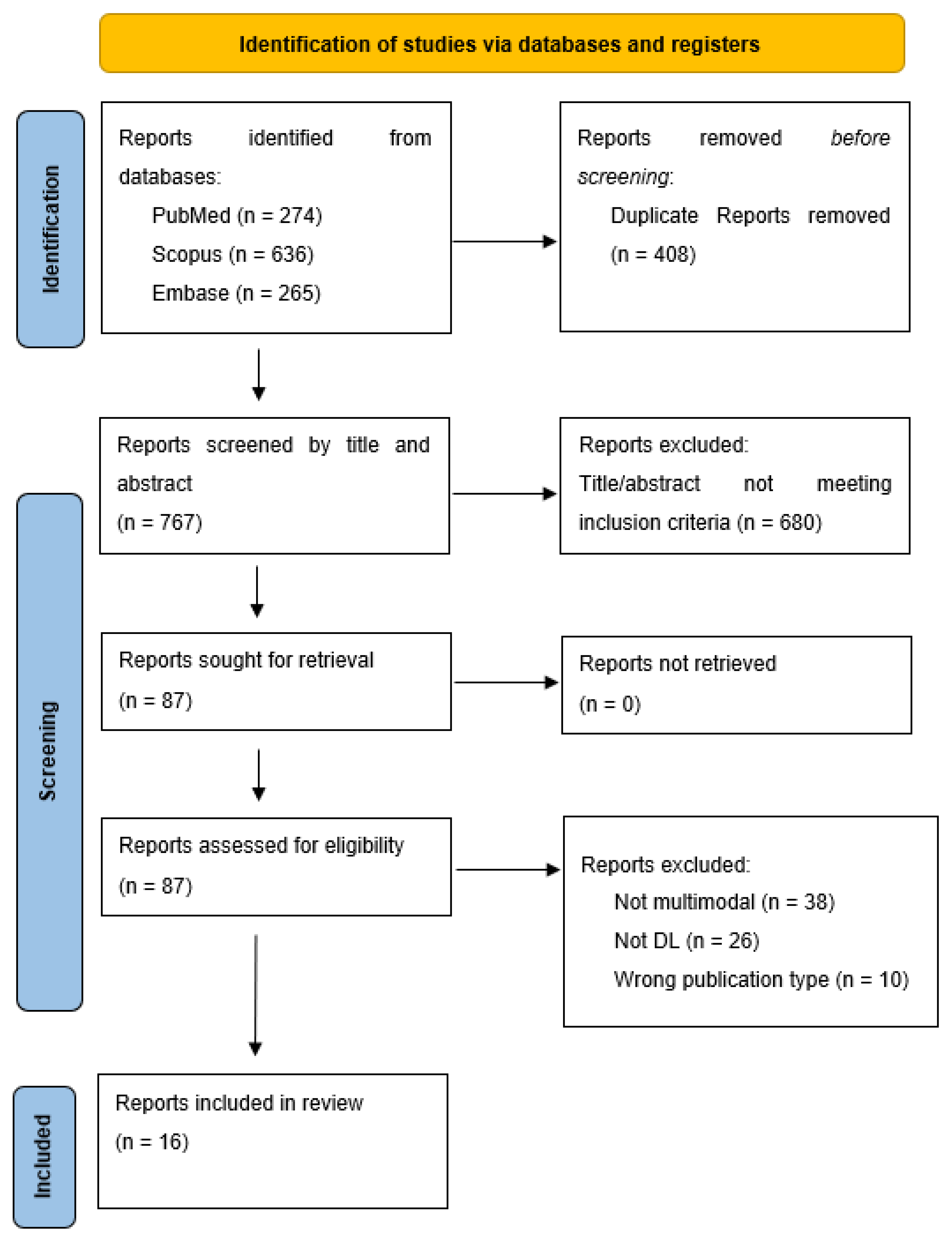
2. Methods
3. Results
Integrated Multimodal Data Types
4. Discussion
4.1. Applications of Multimodal DL
4.2. Use in the Clinical Workflow
4.3. Challenges for Implementation in Clinical Workflow
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, A.P.; Fisher, J.L.; Nichols, E.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Abraha, H.N.; Agius, D.; Alahdab, F.; Alam, T.; et al. Global, regional, and national burden of brain and other CNS cancer, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 376–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.D.; Ostrom, Q.T.; Kruchko, C.; Patil, N.; Tihan, T.; Cioffi, G.; Fuchs, H.E.; Waite, K.A.; Jemal, A.; Siegel, R.L.; et al. Brain and other central nervous system tumor statistics, 2021. CA Cancer J. Clin. 2021, 71, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Shlobin, N.A.; Lam, S.K.; DeCuypere, M. Artificial Intelligence Applications in Pediatric Brain Tumor Imaging: A Systematic Review. World Neurosurg. 2022, 157, 99–105. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Huang, J.; Shlobin, N.A.; DeCuypere, M.; Lam, S.K. Deep Learning for Outcome Prediction in Neurosurgery: A Systematic Review of Design, Reporting, and Reproducibility. Neurosurgery 2022, 90, 16–38. [Google Scholar] [CrossRef]
- Kelly, C.J.; Karthikesalingam, A.; Suleyman, M.; Corrado, G.; King, D. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019, 17, 195. [Google Scholar] [CrossRef] [Green Version]
- Vulli, A.; Srinivasu, P.N.; Sashank, M.S.K.; Shafi, J.; Choi, J.; Ijaz, M.F. Fine-Tuned DenseNet-169 for Breast Cancer Metastasis Prediction Using FastAI and 1-Cycle Policy. Sensors 2022, 22, 2988. [Google Scholar] [CrossRef]
- El-Sappagh, S.; Ali, F.; Abuhmed, T.; Singh, J.; Alonso, J.M. Automatic detection of Alzheimer’s disease progression: An efficient information fusion approach with heterogeneous ensemble classifiers. Neurocomputing 2022, 512, 203–224. [Google Scholar] [CrossRef]
- Pei, L.; Vidyaratne, L.; Rahman, M.M.; Iftekharuddin, K.M. Context aware deep learning for brain tumor segmentation, subtype classification, and survival prediction using radiology images. Sci. Rep. 2020, 10, 19726. [Google Scholar] [CrossRef]
- Shboul, Z.A.; Alam, M.; Vidyaratne, L.; Pei, L.; Elbakary, M.I.; Iftekharuddin, K.M. Feature-Guided Deep Radiomics for Glioblastoma Patient Survival Prediction. Front. Neurosci. 2019, 13, 966. [Google Scholar] [CrossRef]
- Schneider, L.; Laiouar-Pedari, S.; Kuntz, S.; Krieghoff-Henning, E.; Hekler, A.; Kather, J.N.; Gaiser, T.; Fröhling, S.; Brinker, T.J. Integration of deep learning-based image analysis and genomic data in cancer pathology: A systematic review. Eur. J. Cancer. 2022, 160, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 372, n71. [Google Scholar] [CrossRef]
- Wolff, R.F.; Moons, K.G.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; PROBAST Group. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Alex, V.; Safwan, M.; Krishnamurthi, G. Automatic segmentation and overall survival prediction in gliomas using fully convolutional neural network and texture analysis. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2018; Volume 10670, pp. 216–225. [Google Scholar] [CrossRef] [Green Version]
- Asthana, P.; Hanmandlu, M.; Vashisth, S. Brain tumor detection and patient survival prediction using U-Net and regression model. Int. J. Imaging Syst. Technol. 2022, 32, 1801–1814. [Google Scholar] [CrossRef]
- Chaddad, A.; Daniel, P.; Zhang, M.; Rathore, S.; Sargos, P.; Desrosiers, C.; Niazi, T. Deep radiomic signature with immune cell markers predicts the survival of glioma patients. Neurocomputing 2022, 469, 366–375. [Google Scholar] [CrossRef]
- Han, W.; Qin, L.; Bay, C.; Chen, X.; Yu, K.H.; Li, A.; Xu, X.; Young, G.S. Integrating deep transfer learning and radiomics features in glioblastoma multiforme patient survival prediction. In Medical Imaging 2020: Image Processing; SPIE: Bellingham, WA, USA, 2020; Volume 11313. [Google Scholar] [CrossRef]
- Kao, P.Y.; Ngo, T.; Zhang, A.; Chen, J.W.; Manjunath, B.S. Brain tumor segmentation and tractographic feature extraction from structural MR images for overall survival prediction. In International MICCAI Brainlesion Workshop; Springer: Berlin/Heidelberg, Germany, 2019; Volume 11384, pp. 128–141. [Google Scholar] [CrossRef] [Green Version]
- Tang, Z.; Xu, Y.; Jiao, Z.; Lu, J.; Jin, L.; Aibaidula, A.; Wu, J.; Wang, Q.; Zhang, H.; Shen, D. Pre-operative overall survival time prediction for glioblastoma patients using deep learning on both imaging phenotype and genotype. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019; Volume 11764, pp. 415–422. [Google Scholar] [CrossRef]
- Islam, M.; Wijethilake, N.; Ren, H. Glioblastoma multiforme prognosis: MRI missing modality generation, segmentation and radiogenomic survival prediction. Comput. Med. Imaging Graph. 2021, 2021, 91. [Google Scholar] [CrossRef]
- Sun, L.; He, Y. Survival prediction of LGG patients based on deep learning of MRI data and genomic data integration. In Proceedings of the 2021 China Automation Congress (CAC), Hangzhou, China, 22–24 October 2021; pp. 6473–6477. [Google Scholar] [CrossRef]
- Wijethilake, N.; Islam, M.; Ren, H. Radiogenomics model for overall survival prediction of glioblastoma. Med. Biol. Eng. Comput. 2020, 58, 1767–1777. [Google Scholar] [CrossRef]
- Jiang, S.; Zanazzi, G.J.; Hassanpour, S. Predicting prognosis and IDH mutation status for patients with lower-grade gliomas using whole slide images. Sci. Rep. 2021, 11, 16849. [Google Scholar] [CrossRef]
- Braman, N.; Gordon, J.W.H.; Goossens, E.T.; Willis, C.; Stumpe, M.C.; Venkataraman, J. Deep Orthogonal Fusion: Multimodal Prognostic Biomarker Discovery Integrating Radiology, Pathology, Genomic, and Clinical Data. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September 2022–1 October 2022; Springer: Berlin/Heidelberg, Germany, 2021; Volume 12905, pp. 667–677. [Google Scholar] [CrossRef]
- Choi, Y.; Nam, Y.; Jang, J.; Shin, N.Y.; Lee, Y.S.; Ahn, K.J.; Hong, Y.G. Radiomics may increase the prognostic value for survival in glioblastoma patients when combined with conventional clinical and genetic prognostic models. Eur. Radiol. 2021, 31, 2084–2093. [Google Scholar] [CrossRef]
- Fathi Kazerooni, A.; Saxena, S.; Toorens, E.; Tu, D.; Bashyam, V.; Akbari, H.; Davatzikos, C. Clinical measures, radiomics, and genomics offer synergistic value in AI-based prediction of overall survival in patients with glioblastoma. Sci. Rep. 2022, 12, 8784. [Google Scholar] [CrossRef]
- Jeong, J.W.; Lee, M.H.; John, F.; Robinette, N.L.; Amit-Yousif, A.J.; Barger, G.R.; Juhász, C. Feasibility of Multimodal MRI-Based Deep Learning Prediction of High Amino Acid Uptake Regions and Survival in Patients With Glioblastoma. Front. Neurol. 2019, 10, 1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.Z.; Liu, P.F.; An, T.T.; Yang, H.C.; Zhang, W.; Wang, J.X. Construction of a prognostic immune signature for lower grade glioma that can be recognized by MRI radiomics features to predict survival in LGG patients. Transl. Oncol. 2021, 14, 101065. [Google Scholar] [CrossRef] [PubMed]
- Mi, E.; Mauricaite, R.; Pakzad-Shahabi, L.; Chen, J.; Ho, A.; Williams, M. Deep learning-based quantification of temporalis muscle has prognostic value in patients with glioblastoma. Br. J. Cancer 2022, 126, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Kuenzi, B.M.; Park, J.; Fong, S.H.; Sanchez, K.S.; Lee, J.; Kreisberg, J.F.; Ideker, T. Predicting Drug Response and Synergy Using a Deep Learning Model of Human Cancer Cells. Cancer Cell 2020, 38, 672–684. [Google Scholar] [CrossRef]
- Mu, W.; Jiang, L.; Zhang, J.; Shi, Y.; Gray, J.E.; Tunali, I.; Schabath, M.B. Non-invasive decision support for NSCLC treatment using PET/CT radiomics. Nat. Commun. 2020, 11, 5228. [Google Scholar] [CrossRef]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Shetty, S. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Jiang, Y.; Yang, M.; Wang, S.; Li, X.; Sun, Y. Emerging role of deep learning-based artificial intelligence in tumor pathology. Cancer Commun. 2020, 40, 154–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Zhang, J.; Sheng, Y.; Chang, Y.; Yin, F.F.; Ge, Y.; Wang, C. Automatic IMRT planning via static field fluence prediction (AIP-SFFP): A deep learning algorithm for real-time prostate treatment planning. Phys. Med. Biol. 2020, 65, 175014. [Google Scholar] [CrossRef]
- Vale-Silva, L.A.; Rohr, K. Long-term cancer survival prediction using multimodal deep learning. Sci. Rep. 2021, 11, 13505. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country | Disease | Procedure | Outcome | Predictors | Data Source | Size | Model Type | Key Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Alex | 2018 | India | Glioma (LGG, HGG) | Patients treated independently | Overall Survival Time | Radiomic, clinical data | BRaTS | 241 | FCNN | After using FCNN for segmentation the BraTS 2017 validation data and test data, the regressor accuracy was 52% and 47%, respectively. |
| Asthana | 2022 | India | Glioma (LGG, HGG) | Patients treated independently | Overall survival | Radiomic, clinical data | BRaTS | 989 | U-net | U-Net-based semantic segmentation of tumors and the pervasive learning model to calculate the weights of the regression model had accuracies of 64.2% on Brats 2018, 59.8% on Brats 2019, and 60.5% on Brats 2020 datasets. |
| Braman | 2021 | United States | Glioma (LGG, GBM) | Patients treated independently | Overall survival with predicted risk score | Radiomic, histologic, genomic, and clinical data | TCIA | 176 | Deep Orthogonal Fusion model, multiple-input CNN, SNN, pre-trained VGG-19 | The multimodal deep orthogonal full fusion model (rad, path, genetics and clinical data) outperformed various combinations of unimodal, pairwise and triple fusion models (except for the rad, path and genetics triple fusion MMO loss). |
| Chaddad | 2022 | Canada | Glioma (LGG, GBM) | Patients treated independently | Overall survival | Radiomic, clinical data | The Cancer Imaging Archive (TCIA) | 151 | 3D CNN | Combining DRFs (using 3D CNN), clinical features and immune cell markers as input to a random forest classifier discriminated between short and long survival outcomes. |
| Choi | 2021 | South Korea | Glioblastoma | Patients treated independently | Overall survival via iAUC | Radiomic, genetic, clinical data | Institutional | 120 | CNN | When CNN radiomics was combined with clinical and genetic prognostic models for overall survival and progression free survival in glioblastoma patients, the prognostic value increased. |
| Fathi | 2022 | United States | Glioblastoma | Preoperative mpMRI followed by surgical resection | Overall survival | Radiomic, genomic, MGMT methylation, clinical data | MRI scans from the hospital of the University of Pennsylvania between 2006–2018 | 516 | VGG-16 CNN | The survival prediction performance was highest in the fusion model, combining clinical data, MGMT methylation, radiomics, and genomics, with a c-index of 0.75 and an IBS reduction of 24.8% |
| Han | 2020 | United States | Glioblastoma | Maximal surgical resection and radiation therapy (w/temozolomide or bevacizumab) | Overall survival | Radiomic, clinical data | World Health Organization IV GBM, TCGA | 178 | CNN (VGG-19 for deep features) | Using radiomics and CNN deep learning features extracted from GBM MRIs for a machine learning-based statistical analysis allowed for discrimination between short and long-term survivors. |
| Islam | 2021 | Singapore | Glioblastoma | Patients treated independently | Overall survival | Radiomics, genomic data | TCGA-GBM | 285 | FCN, cGAN, SVM, ANN | Performance almost doubled after fusing genomic features with radiomic and SVM model outperforms ANN model. |
| Jeong | 2019 | United States | Glioblastoma | Resection and subsequent chemoradiation | Progression free survival | Radiomics, clinical data | PET database at Children’s Hospital of Michigan | 21 | U-net | Glioma delineation by PET-based deep learning and clinical multimodal MRI data achieved the highest AUC (0.66) for survival outcome prediction. |
| Jiang | 2021 | United States | Glioma (grades 2 and 3) | Patients treated independently | IDH mutational status and overall survival | Histologic, genetic, clinical data | TCGA | 296 | End-to-end deep learning models (Resnet18) | The performance of the deep learning model, based on only WSIs, is better than the model based on the primary diagnosis and some demographic variables, such as race and gender, but not as good as age at diagnosis. |
| Kao | 2019 | United States | Glioma | Patients treated independently | Overall survival | Radiomic, clinical data | TCIA | 347 | Deep neural networks, hard negative mining, patch-based 3D U-nets, DeepMedic, SVM classifier with linear kernal | The use of normalized brain parcellation data and tractography data achieved a survival prediction accuracy of ~0.7 on the training data set. |
| Li | 2021 | China | Glioma (LGG) | Patients treated independently | Immunotherapy response risk score | Radiomics, immune molecular biomarkers, genetic, clinical data | TCGA | 665 | Neural network deep learning | Patients at lower risk were more likely to be predicted in the low IMriskScore risk group by the imagingomics deep learning model and have higher survival rates |
| Mi | 2022 | United Kingdom | Glioblastoma | Patients treated independently | Overall survival | Radiomic, clinical data | 45 from in house glioblastoma data set, 51 from TCGA-GBM data set | 132 | 2D U-net CNN | U-net trained with DL had highest performance and was better than BCEL and HDL for temporalis segmentation to determine cross sectional measurements. |
| Sun | 2021 | China | Glioma (LGG) | Patients treated independently | Overall survival | Radiomic, genomic data | TCIA, TCGA | 44 | Combining MRI and gene expression data in DNN led to more accurate disease specific survival statistics for LGG patients than when tested separately. | |
| Tang | 2019 | United States | Glioblastoma | Patients treated independently | Overall survival and tumor genotype prediction | Radiomic, genomic biomarker, clinical data | Department of Radiology at University of North Carolina at Chapel Hill | 120 | Integrated multitask CNN | The combination of imaging phenotype and genotype data input to CNN for OS time prediction for GBM outperformed the mono-task CNN-based and radiomics-based random forest methods. |
| Wijethilake | 2020 | Singapore | Glioblastoma | Patients treated independently | Overall survival | Radiomics, genomics | TCGA | 59 | Hypercolumn-based convolutional network, ANN | Hypercolumn-based CNN Radiogenomic data achieved higher survival prediction accuracies than just radiomic or genomic data alone when predicted using ANN, SVM and linear regression models. |
| ROB | Applicability | Overall | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Participants | Predictors | Outcomes | Analysis | Participants | Predictors | Outcomes | ROB | Applicability |
| Alex | 2018 | ? | + | + | - | + | + | + | - | - |
| Asthana | 2022 | ? | ? | ? | ? | ? | ? | ? | ? | ? |
| Braman | 2021 | + | + | + | ? | + | + | + | ? | ? |
| Chaddad | 2022 | + | + | + | - | + | + | + | - | - |
| Choi | 2021 | + | + | + | + | + | + | + | + | + |
| Fathi | 2022 | + | + | + | + | + | + | + | + | + |
| Han | 2020 | ? | + | + | - | + | + | + | - | - |
| Islam | 2021 | ? | + | + | - | + | + | + | - | - |
| Jeong | 2019 | + | + | + | - | + | + | + | - | - |
| Jiang | 2021 | + | + | + | + | + | + | + | + | + |
| Kao | 2019 | + | + | + | + | + | + | + | + | + |
| Li | 2021 | + | + | + | + | + | + | + | + | + |
| Mi | 2022 | + | + | + | + | + | + | + | + | + |
| Sun * | 2021 | ? | ? | ? | - | ? | ? | ? | - | - |
| Tang | 2019 | ? | + | + | ? | + | + | + | ? | ? |
| Wijethilake | 2020 | ? | + | + | + | + | + | + | + | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alleman, K.; Knecht, E.; Huang, J.; Zhang, L.; Lam, S.; DeCuypere, M. Multimodal Deep Learning-Based Prognostication in Glioma Patients: A Systematic Review. Cancers 2023, 15, 545. https://doi.org/10.3390/cancers15020545
Alleman K, Knecht E, Huang J, Zhang L, Lam S, DeCuypere M. Multimodal Deep Learning-Based Prognostication in Glioma Patients: A Systematic Review. Cancers. 2023; 15(2):545. https://doi.org/10.3390/cancers15020545
Chicago/Turabian StyleAlleman, Kaitlyn, Erik Knecht, Jonathan Huang, Lu Zhang, Sandi Lam, and Michael DeCuypere. 2023. "Multimodal Deep Learning-Based Prognostication in Glioma Patients: A Systematic Review" Cancers 15, no. 2: 545. https://doi.org/10.3390/cancers15020545