
Differentiation of Urothelial Carcinoma and Normal Bladder Tissues by Means of Fiber-Based ATR IR Spectroscopy
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Spectroscopy
2.3. Statistical Analysis
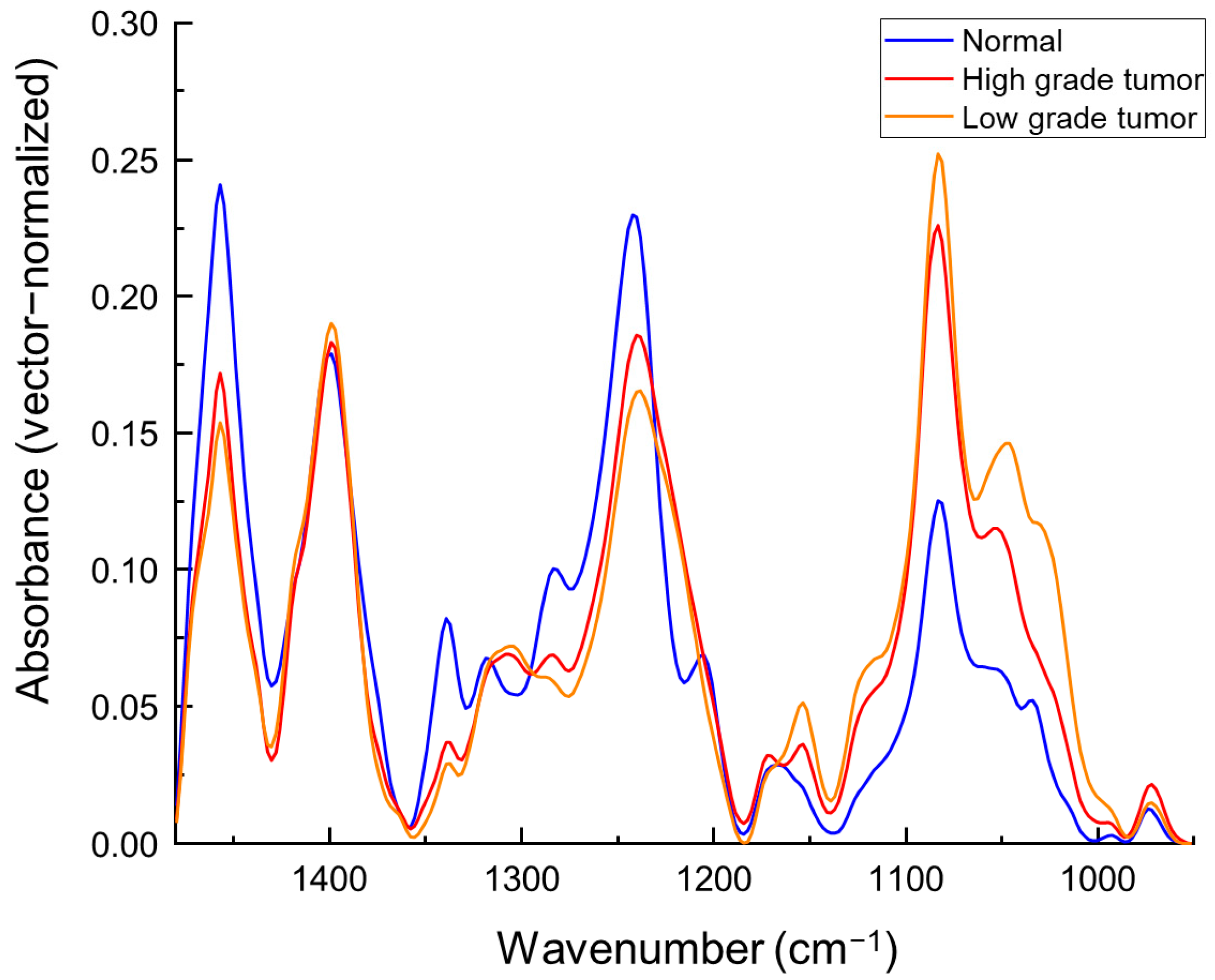
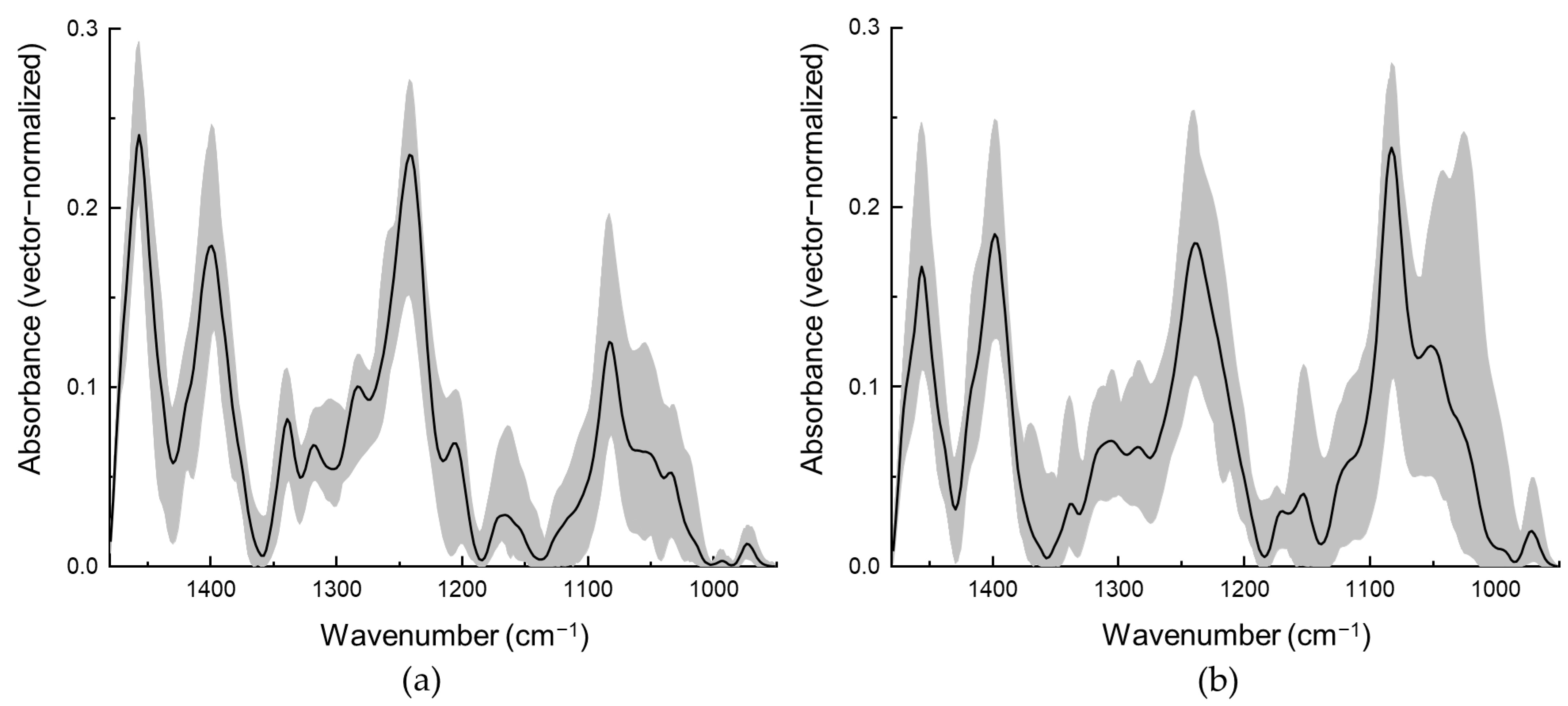
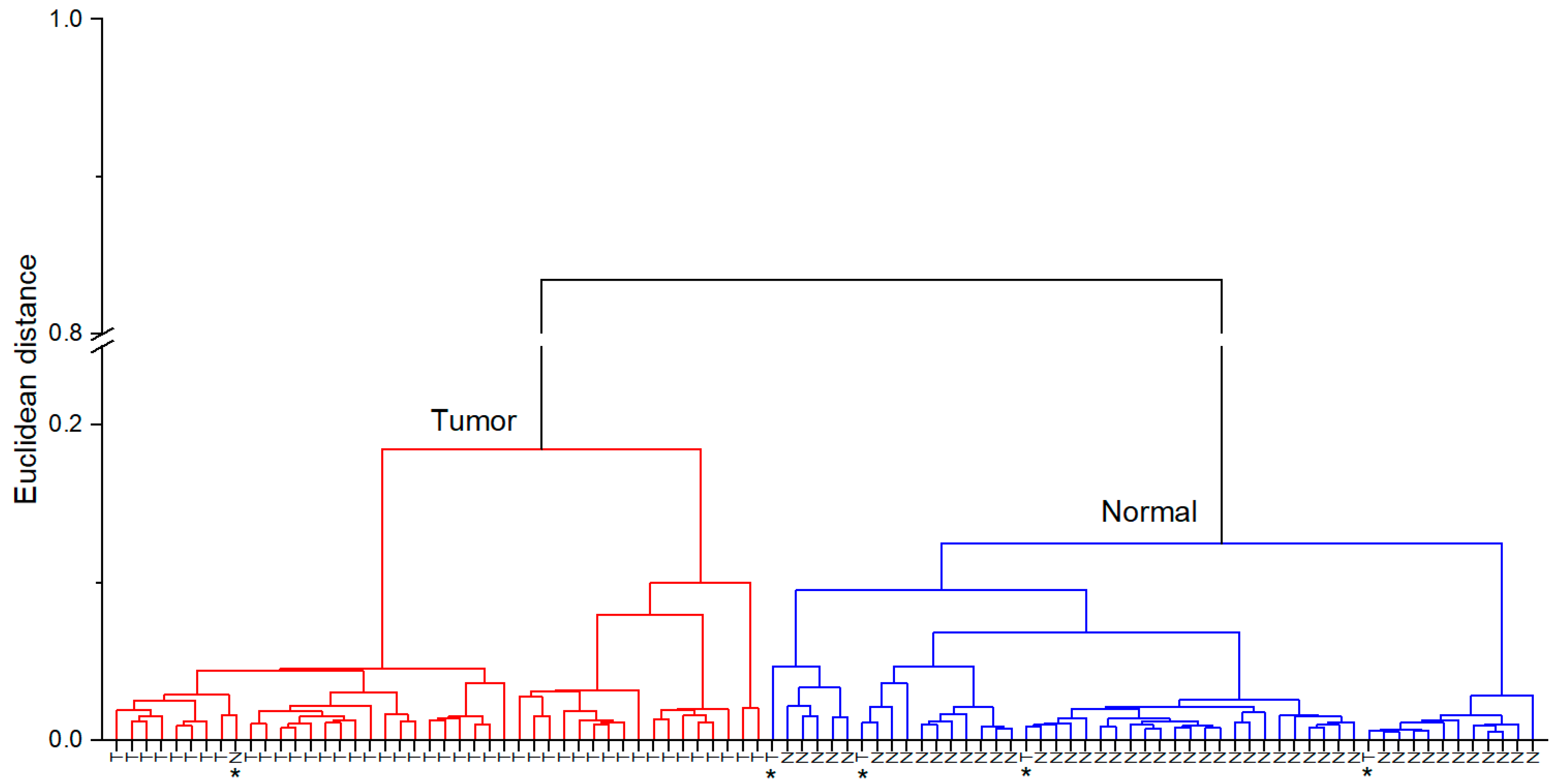
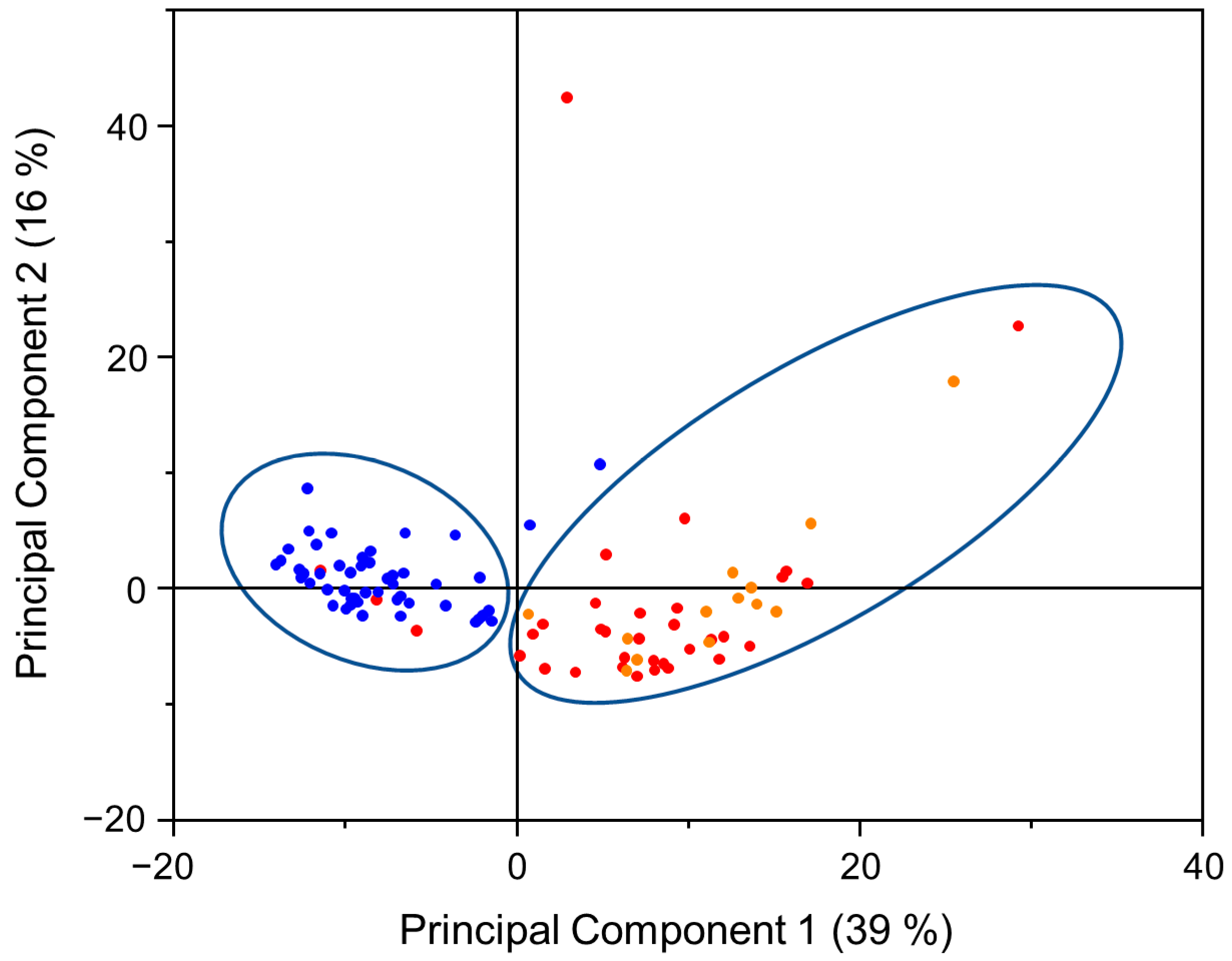
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Gotoh, D.; Shimada, K.; Tatsumi, Y.; Nakai, Y.; Anai, S.; Torimoto, K.; Aoki, K.; Tanaka, N.; Konishi, N.; et al. Exploration of risk factors predicting outcomes for primary T1 high-grade bladder cancer and validation of the Spanish Urological Club for Oncological Treatment scoring model: Long-term follow-up experience at a single institute. Int. J. Urol. 2015, 22, 541–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.J.; Kwon, C.S.; Forsythe, A.; Mamolo, C.M.; Masters, E.T.; Jacobs, I.A. Humanistic and Economic Burden of Non-Muscle Invasive Bladder Cancer: Results of Two Systematic Literature Reviews. Clinicoecon. Outcomes Res. 2020, 12, 693–709. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.I.; Sholklapper, T.N.; Cocci, A.; Broggi, G.; Caltabiano, R.; Smith, A.B.; Lotan, Y.; Morgia, G.; Kamat, A.M.; Witjes, J.A.; et al. Performance of Narrow Band Imaging (NBI) and Photodynamic Diagnosis (PDD) Fluorescence Imaging Compared to White Light Cystoscopy (WLC) in Detecting Non-Muscle Invasive Bladder Cancer: A Systematic Review and Lesion-Level Diagnostic Meta-Analysis. Cancers 2021, 13, 4378. [Google Scholar] [CrossRef]
- Daneshmand, S.; Bazargani, S.T.; Bivalacqua, T.T.; Holzbeierlein, J.M.; Willard, B.; Taylor J., M.; Liao, J.C.; Pohar, K.; Tierney, J.; Konety, B. Blue light cystoscopy for the diagnosis of bladder cancer: Results from the US prospective multicenter registry. Urol. Oncol.: Semin. Orig. Investig. 2018, 36, 361.e1. [Google Scholar] [CrossRef]
- Grossman, H.B.; Soloway, M.; Messing, E.; Katz, G.; Stein, B.; Kassabian, V.; Shen, Y. Surveillance for recurrent bladder cancer using a point-of-care proteomic assay. JAMA 2006, 295, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Kim, L.H.C.; Patel, M.I. Transurethral resection of bladder tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef]
- Song, P.H.; Cho, S.; Ko, Y.H. Decision based on narrow band imaging cystoscopy without a referential normal standard rather increases unnecessary biopsy in detection of recurrent bladder urothelial carcinoma early after intravesical instillation. Cancer Res. Treat. 2016, 48, 273–280. [Google Scholar] [CrossRef]
- Nagaya, T.; Nakamura, Y.A.; Choyke, P.L.; Kobayashi, H. Fluorescence-Guided Surgery. Front. Oncol. 2017, 7, 314. [Google Scholar] [CrossRef]
- Cui, S.; Zhang, S.; Yue, S. Raman Spectroscopy and Imaging for Cancer Diagnosis. J. Healthc. Eng. 2018, 2018, 8619342. [Google Scholar] [CrossRef]
- Desroches, J.; Jermyn, M.; Mok, K.; Lemieux-Leduc, C.; Mercier, J.; St-Arnaud, K.; Urmey, K.; Guiot, M.C.; Marple, E.; Petrecca, K.; et al. Characterization of a Raman spectroscopy probe system for intraoperative brain tissue classification. Biomed. Opt. Express 2015, 6, 2380–2397. [Google Scholar] [CrossRef] [Green Version]
- Benard, A.; Desmedt, C.; Smolina, M.; Szternfeld, P.; Verdonck, M.; Rouas, G.; Kheddoumi, N.; Rothé, F.; Larsimont, D.; Sotiriou, C.; et al. Infrared imaging in breast cancer: Automated tissue component recognition and spectral characterization of breast cancer cells as well as the tumor microenvironment. Analyst 2014, 139, 1044–1056. [Google Scholar] [CrossRef] [PubMed]
- Old, O.J.; Fullwood, L.M.; Scott, R.; Lloyd, G.R.; Almond, L.M.; Shepherd, N.A.; Stone, N.; Barr, H.; Kendall, C. Vibrational spectroscopy for cancer diagnostics. Anal. Methods 2014, 6, 3901–3917. [Google Scholar] [CrossRef]
- Fernandez, D.C.; Bhargava, R.; Hewitt, S.M.; Levin, I.W. Infrared spectroscopic imaging for histopathologic recognition. Nat. Biotechnol. 2005, 23, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Goormaghtigh, E. Infrared Imaging in Histopathology: Is a Unified Approach Possible? Biomed. Spectrosc. Imaging 2016, 5, 325–346. [Google Scholar] [CrossRef] [Green Version]
- Bhargava, R.; Madabhushi, A. Emerging Themes in Image Informatics and Molecular Analysis for Digital Pathology. Annu. Rev. Biomed. Eng. 2016, 18, 387–412. [Google Scholar] [CrossRef] [Green Version]
- Uckermann, O.; Juratli, T.A.; Galli, R.; Conde, M.; Wiedemuth, R.; Krex, D.; Geiger, K.; Temme, A.; Schackert, G.; Koch, E.; et al. Optical Analysis of Glioma: Fourier-Transform Infrared Spectroscopy Reveals the IDH1 Mutation Status. Clin. Cancer Res. 2018, 24, 2530–2538. [Google Scholar] [CrossRef] [Green Version]
- Notarstefano, V.; Sabbatini, S.; Conti, C.; Pisani, M.; Astolfi, P.; Pro, C.; Rubini, C.; Vaccari, L.; Giorgini, E. Investigation of human pancreatic cancer tissues by Fourier Transform Infrared Hyperspectral Imaging. J. Biophotonics 2020, 13, e201960071. [Google Scholar] [CrossRef]
- Pezzei, C.; Brunner, A.; Bonn, G.K.; Huck, C.W. Fourier transform infrared imaging analysis in discrimination studies of bladder cancer. Analyst 2013, 138, 5719–5725. [Google Scholar] [CrossRef]
- Hughes, C.; Iqbal-Wahid, J.; Brown, M.; Shanks, J.H.; Eustace, A.; Denley, H.; Hoskin, P.J.; West, C.; Clarke, N.W.; Gardner, P. FTIR microspectroscopy of selected rare diverse sub-variants of carcinoma of the urinary bladder. J. Biophotonics 2013, 6, 73–87. [Google Scholar] [CrossRef]
- Kujdowicz, M.; Placha, W.; Mech, B.; Chrabaszcz, K.; Okoń, K.; Malek, K. In Vitro Spectroscopy-Based Profiling of Urothelial Carcinoma: A Fourier Transform Infrared and Raman Imaging Study. Cancers 2021, 13, 123. [Google Scholar] [CrossRef]
- Sablinskas, V.; Bandzeviciute, R.; Velicka, M.; Ceponkus, J.; Urboniene, V.; Jankevicius, F.; Laurinavičius, A.; Dasevičius, D.; Steiner, G. Fiber attenuated total reflection infrared spectroscopy of kidney tissue during live surgery. J. Biophotonics 2020, 13, e202000018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandzeviciute, R.; Ceponkus, J.; Velicka, M.; Urboniene, V.; Jankevicius, F.; Zelvys, A.; Steiner, G.; Sablinskas, V. Fiber based infrared spectroscopy of cancer tissues. J. Mol. Struct. 2020, 1220, 128724. [Google Scholar] [CrossRef]
- Zacharovas, E.; Velička, M.; Platkevičius, G.; Čekauskas, A.; Želvys, A.; Niaura, G.; Šablinskas, V. Toward a SERS Diagnostic Tool for Discrimination between Cancerous and Normal Bladder Tissues via Analysis of the Extracellular Fluid. ACS Omega 2022, 7, 10539–10549. [Google Scholar] [CrossRef]
- MedCalc Statistical Calculators. Available online: https://www.medcalc.org/calc/diagnostic_test.php?fbclid=IwAR0P2pB8WaTor3OK_lYBg6jPzkMCz0X2obitS-sVYa3VwHsjXx7YedsiKMs (accessed on 22 December 2022).
- Talari, A.; Martinez, M.G.; Movasaghi, Z.; Rehman, S.; Rehman, I. Advances in Fourier transform infrared (FTIR) spectroscopy of biological tissues. Appl. Spectrosc. Rev. 2017, 52, 456–506. [Google Scholar] [CrossRef]
- Belbachir, K.; Noreen, R.; Gouspillou, G.; Petibois, C. Collagen types analysis and differentiation by FTIR spectroscopy. Anal. Bioanal. Chem. 2009, 395, 829–837. [Google Scholar] [CrossRef]
- Stevenson, K.K.; Kucich, U.; Whitbeck, C.; Levin, R.M.; Howard, P.S. Functional changes in bladder tissue from type III collagen-deficient mice. Mol. Cell Biochem. 2006, 283, 107–114. [Google Scholar] [CrossRef]
- Baba, A.; Câtoi, C. Chapter 3: Tumor Cell Morhology. In Comparative Oncology; The Publishing House of the Romanian Academy: Bucharest, Romania, 2007. Available online: https://www.ncbi.nlm.nih.gov/books/NBK9557/ (accessed on 14 September 2022).
- Bannasch, P. Sequential cellular changes during chemical carcinogenesis. J. Cancer Res. Clin. Oncol. 1984, 108, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Zois, C.E.; Favaro, E.; Harris, A.L. Glycogen metabolism in cancer. Biochem. Pharmacol. 2014, 92, 3–11. [Google Scholar] [CrossRef]
- Mowatt, G.; N’Dow, J.; Vale, L.; Nabi, G.; Boachie, C.; Cook, J.A.; Fraser, C.; Griffiths, T.R.; Aberdeen Technology Assessment Review (TAR) Group. Photodynamic diagnosis of bladder cancer compared with white light cystoscopy: Systematic review and meta-analysis. Int. J. Technol. Assess. Health Care 2011, 27, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue Type | Number of Samples |
|---|---|
| Normal tissue | 49 |
| Tumorous tissue | |
| High-grade tumor | 34 |
| Low-grade tumor | 13 |
| Patient characteristics | Number of patients |
| Tumor size during initial TURB | |
| <10 mm | 12 |
| 10–30 mm | 18 |
| >30 mm | 17 |
| Tumor count on initial TURB | |
| Single | 15 |
| Two to three | 15 |
| More than three | 17 |
| Additional information | |
| Number of patients Median patient age (years) | 54 70.5 |
| Spectral Band Position, cm−1 | Assignment | |
|---|---|---|
| Normal Tissue | Urothelial Carcinoma Tissue | |
| 972 | 972 | ν(PO4) of nucleic acids and proteins OCH3 of polysaccharides |
| Not present | 1028 | ν(C-O), ν(C-C), δ(C-O-H) of glycogen |
| 1033 | Not present | Collagen |
| 1050 | 1048 (low-grade) 1052 (high-grade) | ν(CO-O-C) ν(C-O), δ(C-O) of the C-OH of carbohydrates |
| 1082 | 1082 | ν(PO−2) of nucleic acids |
| Shoulder at 1121 | Shoulder at 1121 | ν(C-O), δ(C-O), δ(C-O-H), δ(C-O-C) phosphodiester stretching |
| Shoulder at 1154 | 1154 | ν(C-O) |
| 1163 | Not present | ν(C-O) |
| Shoulder at 1172 | 1172 | ν(C-O) |
| 1206 | Not present | Amide III |
| 1241 | 1239 | ν(PO−2), Amide III |
| 1282 | 1284 | Amide III |
| Not present | 1307 | ν(CH2) |
| 1317 | Shoulder at 1317 | Amide III |
| 1339 | 1339 | CH2 wagging |
| 1399 | 1399 | δ(CH3) |
| 1457 | 1457 | δ(CH3) |
| Method | ||||
|---|---|---|---|---|
| HCA | PCA | |||
| Value | 95% CI | Value | 95% CI | |
| Sensitivity | 91% | 80% to 98% | 91% | 80% to 98% |
| Specificity | 98% | 89% to 100% | 96% | 86% to 100% |
| PPV | 98% | 86% to 100% | 96% | 85% to 99% |
| NPV | 92% | 82% to 97% | 92% | 87% to 98% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandzevičiūtė, R.; Platkevičius, G.; Čeponkus, J.; Želvys, A.; Čekauskas, A.; Šablinskas, V. Differentiation of Urothelial Carcinoma and Normal Bladder Tissues by Means of Fiber-Based ATR IR Spectroscopy. Cancers 2023, 15, 499. https://doi.org/10.3390/cancers15020499
Bandzevičiūtė R, Platkevičius G, Čeponkus J, Želvys A, Čekauskas A, Šablinskas V. Differentiation of Urothelial Carcinoma and Normal Bladder Tissues by Means of Fiber-Based ATR IR Spectroscopy. Cancers. 2023; 15(2):499. https://doi.org/10.3390/cancers15020499
Chicago/Turabian StyleBandzevičiūtė, Rimantė, Gediminas Platkevičius, Justinas Čeponkus, Arūnas Želvys, Albertas Čekauskas, and Valdas Šablinskas. 2023. "Differentiation of Urothelial Carcinoma and Normal Bladder Tissues by Means of Fiber-Based ATR IR Spectroscopy" Cancers 15, no. 2: 499. https://doi.org/10.3390/cancers15020499