
Isolated Pancreatic Metastases of Renal Cell Carcinoma—Clinical Particularities and Seed and Soil Hypothesis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methodology
Statistics
3. Results
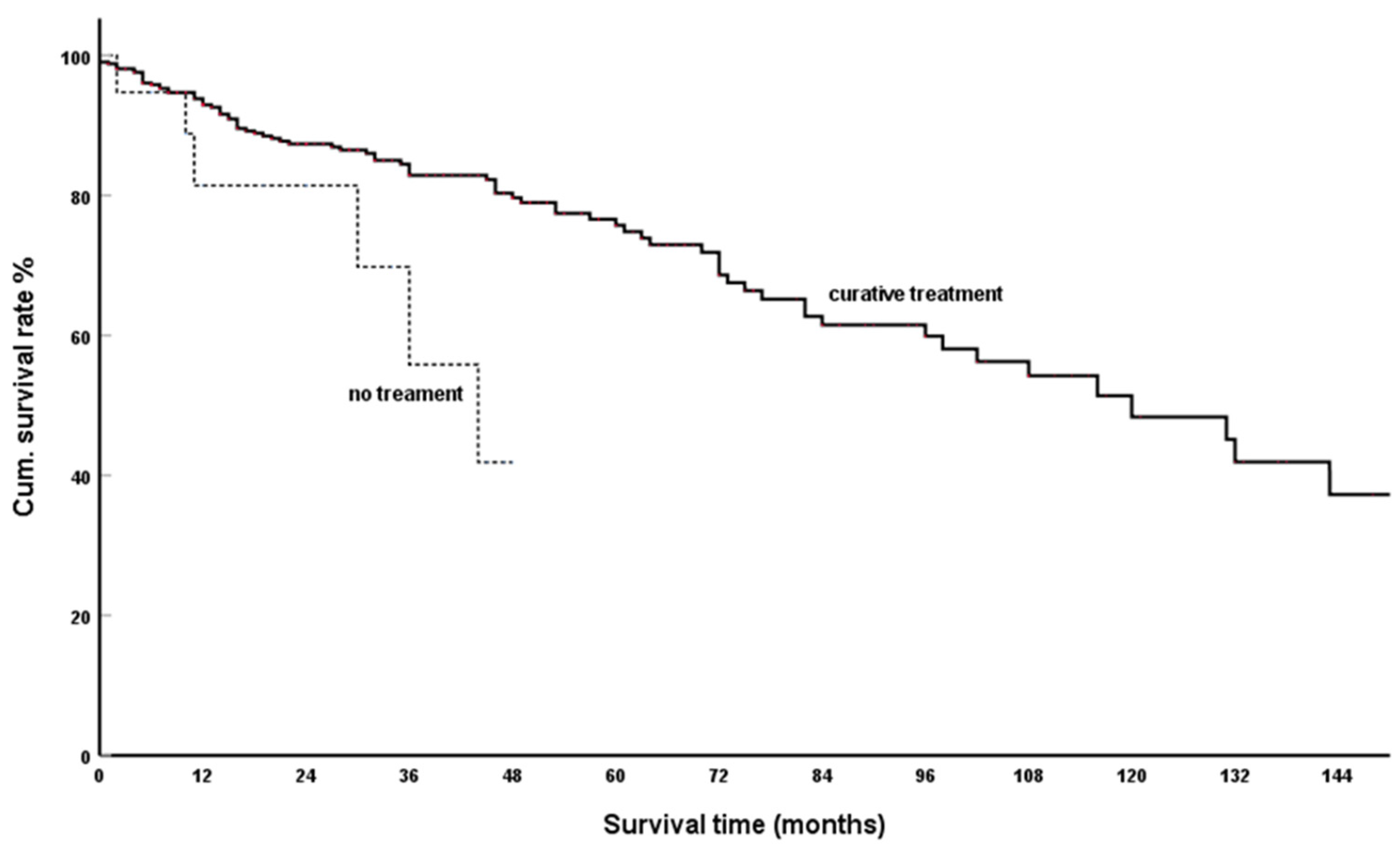
3.1. TreatmentOoutcomes
3.1.1. Surgical Therapy
3.1.2. Spontaneous Course of IsPMRCC
3.1.3. Systemic Treatment
3.2. Tumour Volume-Dependent Risk Factors
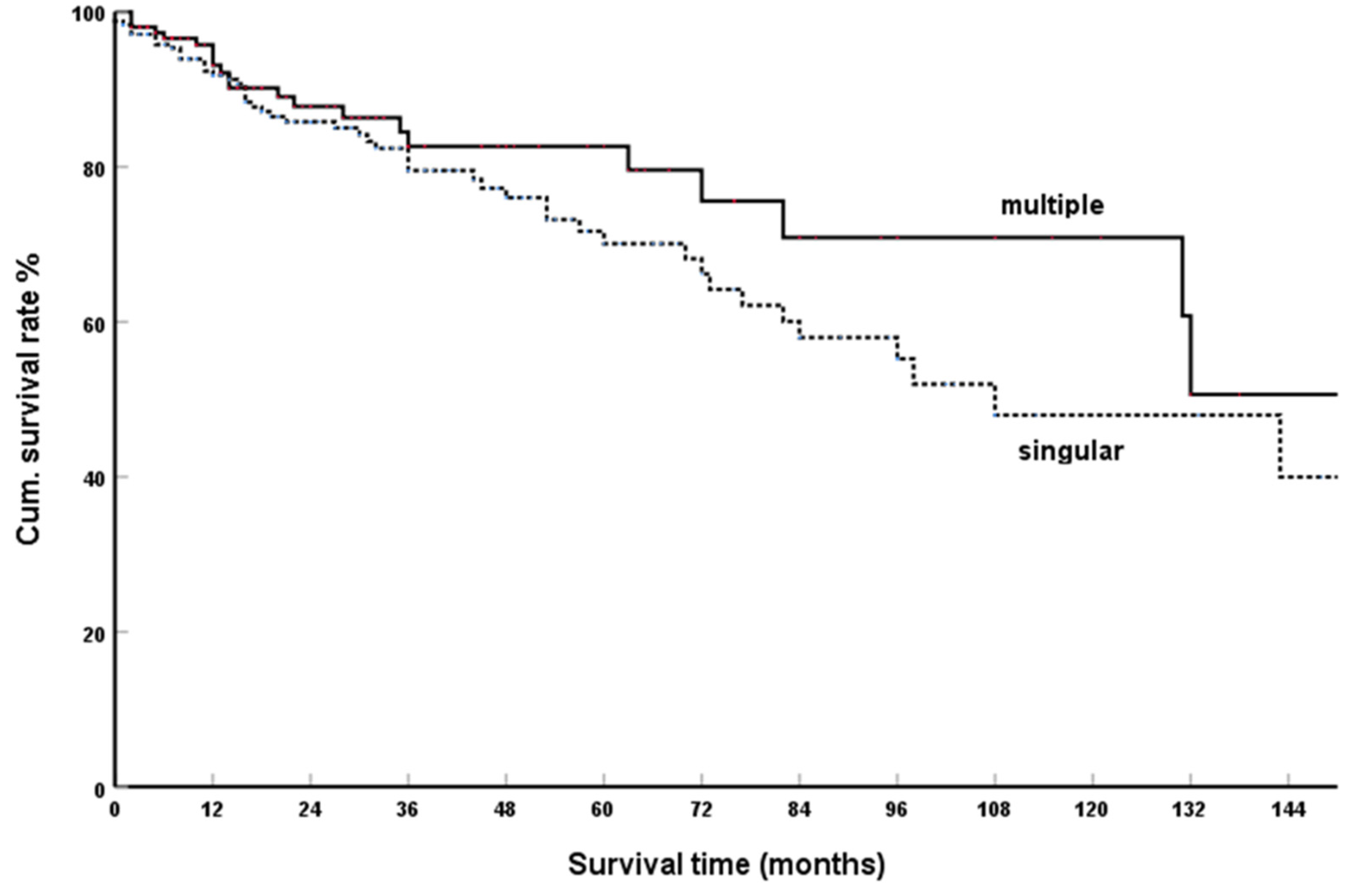
3.2.1. Single Versus Multiple Metastases
3.2.2. Number of Pancreatic Metastases
3.2.3. Size of PM
3.3. Risk Factors Related to the Time of PM Operation
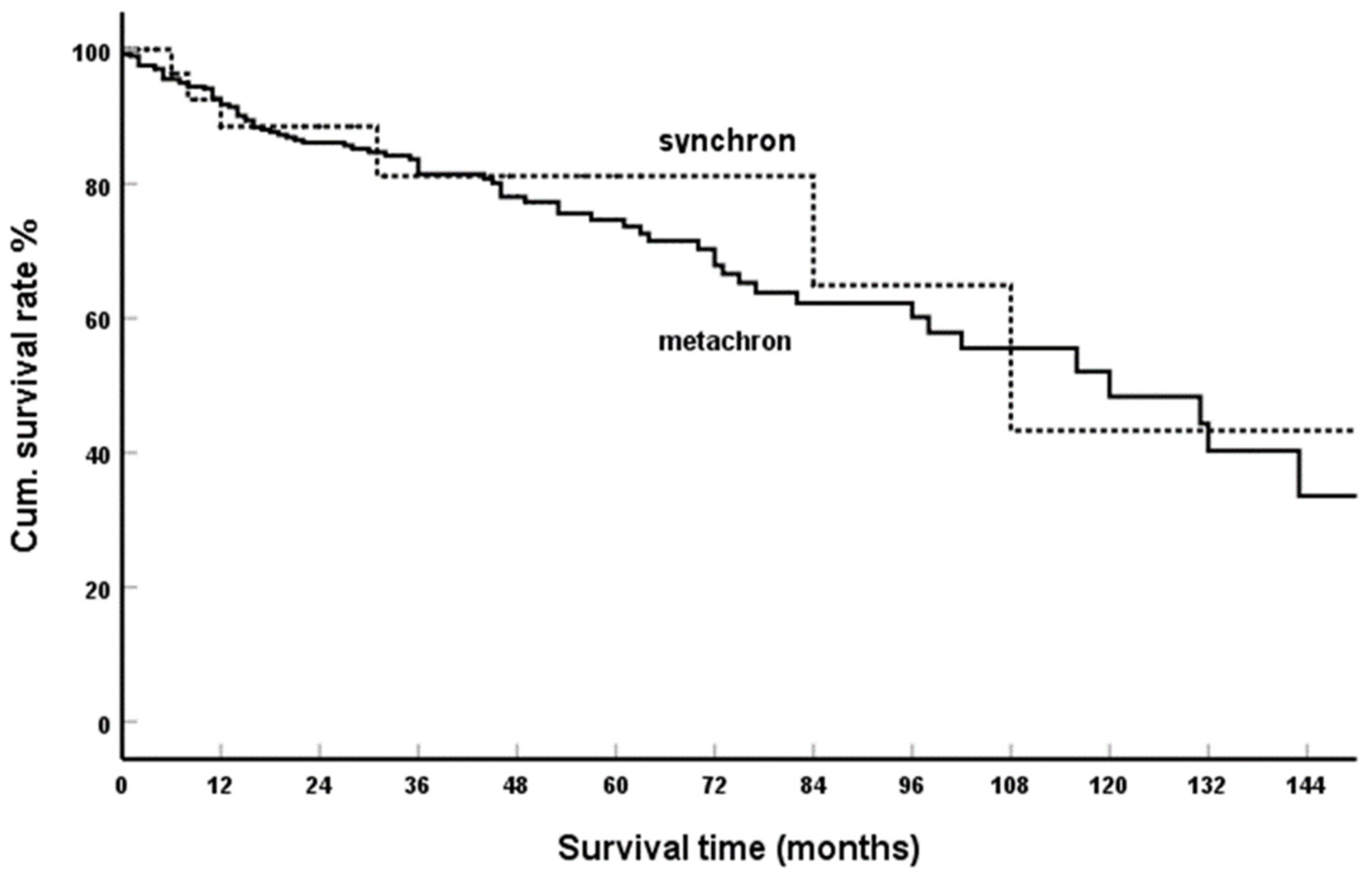
3.3.1. Synchronous Versus Metachronous Occurrence
3.3.2. Interval between Nephrectomy and PM Diagnosis
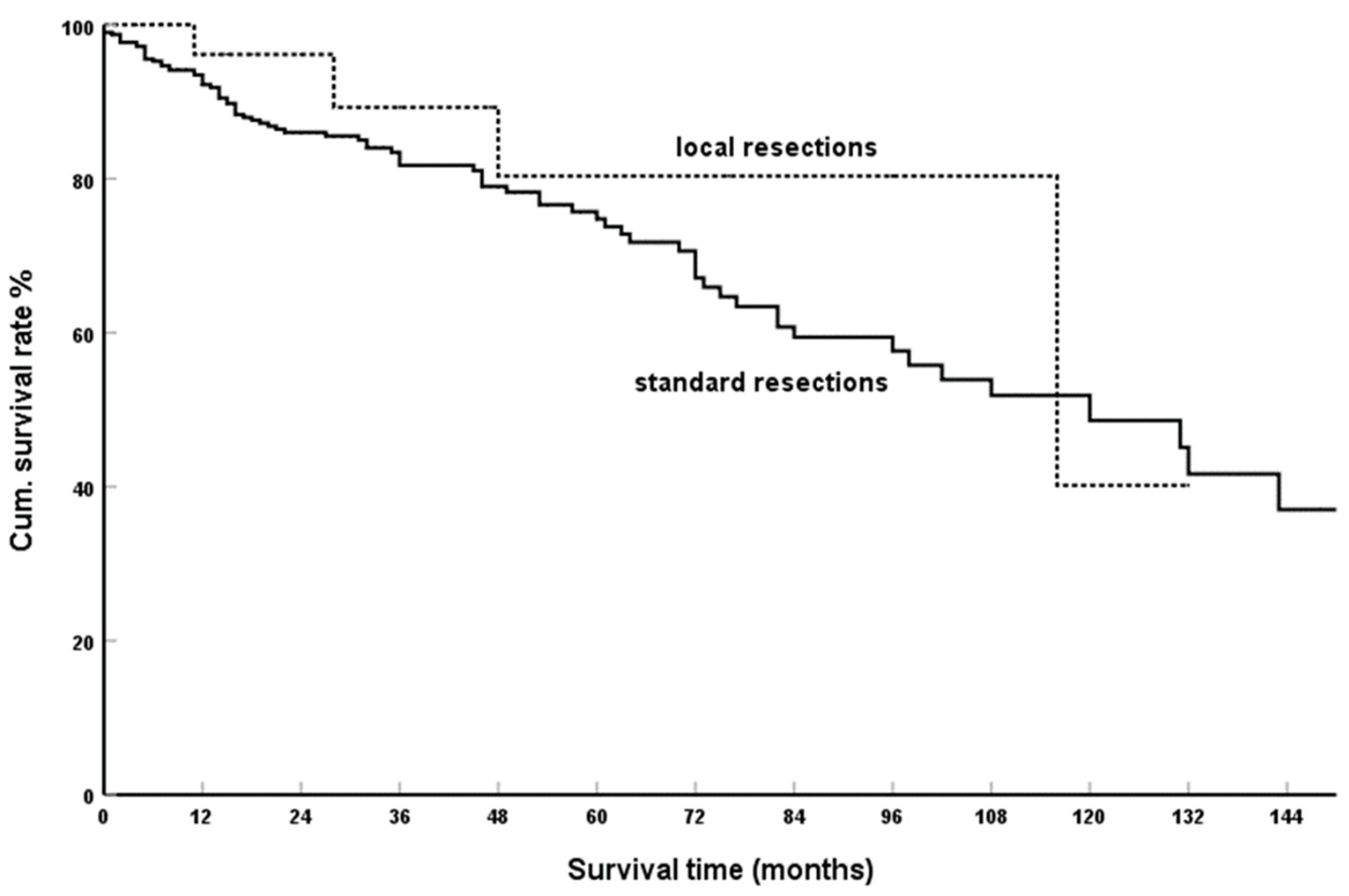
3.4. Extent of Resection
4. Discussion
4.1. Genetics/Epigenetics of isPMRCC
4.2. IsPMRCC and Risk Factors
4.3. IsPMRCC and Seed and Soil Mechanism
4.4. IsPMRCC and Organotropism
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jenssen, E. A metastatic hypernephroma to the pancreas. Acta Chir. Scand. 1952, 104, 177–180. [Google Scholar] [PubMed]
- Lawson, L.; Holt, L.; Rooke, H. Recurrent duodenal haemorrhage from renal carcinoma. Brit. J. Urol. 1966, 38, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, R.A.; Russo, J. Renal cell carcinoma metastatic to the pancreas thirteen years following nephrectomy. Mil. Med. 1969, 134, 200–203. [Google Scholar] [CrossRef]
- Marquand, J.; Giraud, B.; Maliakas, S. Pancreatic metastasis revealing a kidney neoplasm. J. Urol. Nephrol. 1971, 77, 595–601. [Google Scholar]
- Guttman, F.; Ross, M.; Lachance, C. Pancreatic metastasis of renal cell carcinoma treated by total pancreatectomy. Arch Surg. 1972, 105, 782–784. [Google Scholar] [CrossRef]
- Gillet, M.; Camelit, G.; Runser, G.; Clement, D. Duodenopancreatic metastasis of kidney cancer revealed by digestive hemorrhage treated by cephalic duodeno-pancreatectomy. Chirurgie 1974, 100, 226–230. [Google Scholar] [PubMed]
- Hermanutz, K.D.; Sonnenberg, G.E. Late metastasis of a hypernephroid kidney carcinoma to the pancreas with tumor invasion to the duodenum. Fortschr. Röntgenstr. 1977, 127, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Saxon, A.; Gottesman, J.; Doolas, A. Bilateral hypernephroma with solitary pancreatic metastasis. J. Surg. Oncol. 1980, 13, 317–322. [Google Scholar] [CrossRef]
- Yazaki, T.; Ishikawa, S.; Ogawa, Y.; Takahashi, S.; Nemoto, S.; Rinsho, K.; Kanoh, S.; Kitagawa, R. Silent pancreatic metastasis from renal cell carcinoma diagnosed at arteriography. Acta Urol. Jpn. 1981, 27, 1517–1522. [Google Scholar]
- Py, J.M.; Arnaud, J.P.; Cinqualbre, J.; Adloff, M.; Bollack, C. Pancreatic metastases of nephro-epitheliomas. Apropos of 2 cases. Acta Chir. Belg. 1984, 84, 117–121. [Google Scholar]
- Skaarup, P.; Jorgensen, T.; Larsen, S. Asynchronous metastasizing renal cell carcinoma associated with progressive immune complex glomerulonephritis and proteinuria. Scand. J. Urol. Nephrol. 1984, 18, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Audisio, R.A.; La Monica, G. Solitary pancreatic metastasis occurring 20 years after nephrectomy for carcinoma of the kidney. Tumori 1985, 71, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, H.; Niumra, Y.; Okamoto, K.; Tsuchie, K.; Yamase, H.; Maeda, S.; Kamija, J.; Hasagawa, H.; Hayakawa, N.; Yamamoto, M. A case of resected renal cell carcinoma with massive pancreatic metastasis. Jap. J. Cancer. Clin. 1985, 31, 91–96. [Google Scholar]
- Amamiya, H.; Iizumi, T.; Yazaki, T.; Waku, M.; Yasuda, H.; Takada, T.; Shikata, J.; Nagai, J. A solitary pancreatic metastasis from renal cell carcinoma. Hinyouki Geka 1988, 2, 167–170. [Google Scholar]
- Carini, M.; Selli, C.; Barbanti, G.; Bianchi, S.; Muraro, G. Pancreatic late recurrence of bilateral renal cell carcinoma after conservative surgery. Eur. Urol. 1988, 14, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Hirano, M.; Douden, K.; Bantou, H.; Sakatoku, M.; Saitoh, H.; Tachikawa, H.; Kitagawa, K.; Yamahata, T.; Hirano, A.; Kawaguchi, M.; et al. Solitary pancreatic metastasis occuring 10 years after nephrectomy for carcinoma of the kidney. Tan Sui 1988, 9, 233–237. [Google Scholar]
- Sharma, S.K.; Kumar, A.; Madhusoodnan, P.; Banerjee, C.; Suri, S.; Dhar, M. Solitary pancreatic metastasis from renal cell carcinoma. A rare metastatic site. Indian J. Cancer 1988, 25, 29–32. [Google Scholar]
- Guyenne, C.; Rat, P.; Haas, O.; Baudet, J.G.; Favre, J.P. Triple metastase pancreatique d´un cancer du rein traitee par duodenopancreatectomie subtotale. Presse Med. 1989, 18, 231. [Google Scholar]
- Iwanami, M.; Nakayoshi, A.; Yagi, H.; Shimizu, K.; Kimura, K.; Suzuki, K.; Matsumoto, K.; Kai, Y.; Heno, M.; Sagawa, F.; et al. A resected case of the asymptomatic pancreatic metastasis in the body and tail of the pancreas from renal cell carcinoma. J. Jpn. Panc. Soc. 1989, 4, 100–106. [Google Scholar]
- Roland, C.; van Heerden, J. Nonpancreatic primary tumors with metastasis to the pancreas. Surg. Gynecol. Obstet. 1989, 168, 345–347. [Google Scholar]
- Simpson, N.S.; Mulholland, C.K.; Lioe, T.; Spence, R. Late, solitary metastatic renal carcinoma in the pancreas. Ulster Med. J. 1989, 58, 198–199. [Google Scholar] [PubMed]
- Strijk, S.P. Pancreatic metastases of renal cell carcinoma: Report of two cases. Gastrointest. Radiol. 1989, 14, 123–126. [Google Scholar] [CrossRef]
- Temellini, F.; Bavosi, M.; Lamarra, M.; Quagliarini, P.; Giuliani, F. Pancreatic metastasis 25 years after nephrectomy for renal cancer. Tumori 1989, 75, 503–504. [Google Scholar] [CrossRef]
- Gohji, K.; Matsumoto, O.; Kamidono, S. Solitary pancreatic metastasis from renal cell carcinoma. Hinyokika Kiyo 1990, 36, 677–681. [Google Scholar] [PubMed]
- Terashima, M.; Abe, H.; Suga, K.; Matsuya, F.; Kobayashi, K.; Itoh, S.; Sasaki, R.; Kanno, S.; Saito, K.; Tomichi, N.; et al. Two cases of renal cell carcinoma metastasized to the pancreas and to the gallbladder. Jpn. J. Gastroenterol. Surg. 1990, 23, 1952–1956. [Google Scholar] [CrossRef]
- Furukawa, T.; Hattori, R.; Ohtake, H.; Souma, T.; Kinukawa, T.; Hirai, K.; Kimura, J.; Sakata, T.; Ishii, M.; Hayashi, N.; et al. A resectable case of pancreatic head metastasis from renal cell carcinoma. Hinyouki Geka 1991, 4, 111–114. [Google Scholar]
- Kubo, K.; Morita, J.; Mizoe, J.; Ogawa, H.; Irie, G. Renal cell carcinoma metastatic to the pancreas 8 years following nephrectomy. Jpn. J. Clin. Radiol. 1991, 36, 509–512. [Google Scholar]
- Nishida, O.; Matsunaga, Y.; Dekigai, H.; Um, S.; Hsieh, C.; Kimura, F. Three elderly cases of renal cell carcinoma with pancreatic metastasis. Nippon Ronen Igakkai Zasshi 1991, 28, 392–396. [Google Scholar] [CrossRef] [Green Version]
- Oka, H.; Hatayama, T.; Taki, Y.; Ueyama, H.; Hida, S.; Noguchi, M. A resected case of renal cell carcinoma with metastasis to the pancreas. Hinyokika Kiyo. 1991, 37, 1531–1534. [Google Scholar]
- Tabata, T.; Kuroda, Y.; Nishimatsu, S.; Satoh, Y. A resected case of pancreatic tumor metastasized from renal cell carcinoma. J. Jpn. Panc. Soc. 1991, 6, 245–250. [Google Scholar]
- Yamamoto, S.; Tobinaga, K.; Taketomi, K.; Kimino, K.; Ashizuka, S.; Kishikawa, M. Pancreatic metastasis of renal cell carcinoma occurring 17 years after nephrectomy. J. Jpn. Soc. Clin. Surg. 1991, 52, 3006–3011. [Google Scholar] [CrossRef] [Green Version]
- Fujii, M.; Kogawa, T.; Matsuyama, K.; Yamamoto, H.; Kaawahito, Y.; Iinuma, S.; Kokura, S.; Takemura, S.; Yoshikawa, T.; Kondo, M.; et al. A case of metastatic renal cell carcinoma to pancreas ten years after nephrectomy. J. Kyoto Pref. Univ. Med. 1992, 101, 589–596. [Google Scholar]
- Melo, C.R.; Melo, I.S.; Monteiro, A.Z.; de Mello, E.S. Pancreatic metastasis from renal cell carcinoma. Arq. Gastroenterol. 1992, 29, 110–112. [Google Scholar] [PubMed]
- Nakagawa, K.; Tsuchiya, T.; Momono, S.; Sasaki, Y.; Sato, T. A case of pancreatic metastasis of renal cell carcinoma. Jpn. J. Gastroenterol. Surg. 1992, 25, 2200–2204. [Google Scholar] [CrossRef] [Green Version]
- Rypens, F.; Van Gansbeke, V.; Lambilliotte, J.; Regemorter, V.; Verhest, A.; Struyven, J. Pancreatic metastasis from renal cell carcinoma. Br. J. Radiol. 1992, 65, 547–548. [Google Scholar] [CrossRef]
- Stankard, C.; Karl, R.C. The treatment of isolated pancreatic metastases from renal cell carcinoma: A surgical review. Am. J. Gastroenterol. 1992, 87, 1658–1660. [Google Scholar]
- Aikou, S.; Tokura, Y.; Yamafuji, K.; Takahashi, T.; Yoshibide, O.; Kishii, K.; Fujii, S.; Katsumata, K.; Tamiya, M.; Takahashi, T.; et al. A resected case of pancreatic metastasis from renal cell carcinoma presenting with acute duodenal bleeding. J. Jpn. Soc. Clin. Surg. 1993, 54, 2666–2672. [Google Scholar] [CrossRef] [Green Version]
- Calmes, J.M.; Meyer, A. Pancreatic hypernephroma manifested by a duodenal hemorrhage. Rev. Med. Suisse Rom. 1993, 113, 629–631. [Google Scholar]
- Ishikawa, T.; Horimi, T.; Majima, K. A resected case of pancreatic tumor metastasized from renal cell carcinoma. A review of 11 cases in the japanese and 13 cases in the foreign literature. J. Jpn. Soc. Clin. Surg. 1993, 51, 1642–1647. [Google Scholar]
- Kawaguchi, T.; Tsunoda, T.; Tanaka, Y.; Saika, Y.; Ohiani, H.; Fujii, R.; Zaitsu, Y.; Tanimura, H.; Takifuji, K.; Saika, Y.; et al. A case of resection of a solitary pancreatic metastasis of renal cell carcinoma occuring 5 years after nephrectomy. J. Jpn. Panc. Soc. 1993, 8, 189–195. [Google Scholar]
- Marcote-Valdivieso, E.; Arlandis, F.; Baltasar, A.; Martinez, C.; Vierna, G. Synchronous pancreatic metastasis of renal carcinoma. Rev. Esp. Enferm. Dig. 1993, 83, 471–473. [Google Scholar] [PubMed]
- Nan, Y.; Kuno, N.; Kurimoto, K.; Nakamura, T.; Kobayashi, S. A resected case of pancreatic tumor metastasized from renal cell carcinoma diagnosed by endoscopic biopsy through the main pancreatic duct. Gastroenterol. Endosc. 1993, 35, 1380–1385. [Google Scholar]
- Oda, K.; Itoh, J.; Hachisuka, K.; Yamaguchi, A.; Isogai, M.; Utsunomiya, H.; Osamura, Y.; Watanabe, K. Value of computer image analysis in improving ERCP images in metastatic tumor of the pancreas. AJR 1993, 161, 885–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reale, D.; Squillaci, S.; Guarino, M.; Milesi, F.; Forloni, B.; Vezzini, V.; Pascale, M.; Micoli, G.; Milesi, F.; Forloni, B.; et al. Late pancreatic metastasis of renal carcinoma. Description of 2 cases and review of literature. Minerva Urol. Nefrol. 1993, 45, 183–186. [Google Scholar] [PubMed]
- Sauvanet, A.; Barthes, T.; Levy, P.; Flejou, J.F. Late pancreatic metastasis from renal cell carcinoma. Pancreas 1993, 8, 742–746. [Google Scholar] [CrossRef]
- Takeuchi, H.; Konaga, E.; Harano, M.; Watanabe, K.; Takeuchi, Y.; Hara, M.; Mano, S. Solitary pancreatic metastasis from renal cell carcinoma. Acta Med. Okayama 1993, 47, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Vergara, V.; Marucci, M.; Marcarino, C.; Brunello, F.; Capussotti, L. Metastatic involvement of the pancreas from renal cell carcinoma treated by surgery. Ital. J. Gastroenterol. 1993, 25, 388–390. [Google Scholar]
- Yanagisawa, T.; Nakayama, K.; Kashiwagi, M.; Tanaka, J.; Kashiwagi, T.; Mizusaki, K.; Itoh, A.; Akimoto, H.; Takahashi, T.; Aoki, T.; et al. Three cases of resectable pancreatic metastases from renal cell carcinoma. Geka Shinryo 1993, 35, 651–655. [Google Scholar]
- Zugel, N.; Leipprand, F.; Weckermann, D.; Witte, J. Solitäre Pankreaskopfmetastase bei hypernephroidem Carcinom. Fortschr. Med. 1994, 112, 388–390. [Google Scholar]
- Dousset, B.; Andant, C.; Guimbaud, R.; Roseau, G.; Tulliez, M.; Gaudric, M.; Palazzo, L. Late pancreatic metastasis from renal cell carcinoma diagnosed by endoscopic ultrasonography. Surgery 1995, 117, 591–594. [Google Scholar] [CrossRef]
- Fabre, J.; Rounanet, P.; Dagues, F.; Blanc, F.; Baumel, H.; Domergue, J. Various features and surgical approach of solitary pancreatic metastasis from renal cell carcinoma. Eur. J. Surg. Oncol. 1995, 21, 683–686. [Google Scholar] [CrossRef] [PubMed]
- Onishi, T.; Ohishi, Y.; Iizuka, N.; Suzuki, Y.; Shirakawa, H.; Hatano, T.; Tomita, M. Clinical characteristics of 7 renal cell carcinoma patients developing a solitary pancreatic metastasis after nephrectomy. Nippon Hinyokika Gakkai Zasshi 1995, 86, 1538–1542. [Google Scholar] [PubMed] [Green Version]
- Orita, M.; Morita, N.; Hiraoka, H.; Noshima, S.; Takaimashi, T.; Esato, K. A case of resected pancreatic metastasis from renal cell carcinoma 14 years after radical nephrectomy. J. Jpn. Panc. Soc. 1995, 10, 63–68. [Google Scholar]
- Takashi, M.; Takagi, Y.; Sakata, T.; Shimoji, T.; Miyake, K. Surgical treatment of renal cell carcinoma metastases: Prognostic significance. Int. Urol. Nephrol. 1995, 27, 1–8. [Google Scholar] [CrossRef]
- Barras, J.P.; Baer, H.; Stenzl, A.; Czerniak, A. Isolated late metastasis of a renal cell cancer treated by radical distal pancreatectomy. HPB Surg. 1996, 10, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Hirota, T.; Tomida, T.; Iwasa, M.; Takahashi, K.; Kaneda, M.; Tamaki, H. Solitary pancreatic metastasis occurring eight years after nephrectomy for renal cell carcinoma. A case report and surgical review. Int. J. Pancreatol. 1996, 19, 145–153. [Google Scholar] [CrossRef]
- Palazzo, L.; Borotto, E.; Cellier, C.; Roseau, G.; Chaussade, S.; Couturier, D.; Paolaggi, J. Endosonographic features of pancreatic metastases. Gastrointest. Endosc. 1996, 44, 433–436. [Google Scholar] [CrossRef]
- Paz, A.; Koren, R.; Gal, R.; Wolloch, Y. Late solitary pancreatic metastasis from renal cell carcinoma. Isr. J. Med. Sci. 1996, 32, 1319–1321. [Google Scholar]
- Chambers, T.; Fishman, E.; Hruban, R. Pancreatic metastases from renal cell carcinoma in von Hippel-Lindau disease. Clin. Imaging 1997, 21, 40–42. [Google Scholar] [CrossRef]
- Harrison, L.E.; Merchant, N.; Cohen, A.M.; Brennan, M.F. Pancreaticoduodenectomy for nonperiampullary primary tumors. Am. J. Surg. 1997, 174, 393–395. [Google Scholar] [CrossRef]
- Robbins, E.G.; Franceschi, D.; Barkin, J. Solitary metastatic tumors to the pancreas: A case report and review of the literature. Am. J. Gastroenterol. 1997, 92, 914–915. [Google Scholar]
- Adem, C.; Chetritt, J.; Guymar, S.; Bellil, K.; Ladouch-Badre, A.; Benlagha, N.; Bedossa, P. Pancreatic metastasis of a renal adenocarcinoma. Apropos on 2 cases. Ann. Pathol. 1998, 18, 481–483. [Google Scholar]
- Altschuler, E.; Ray, A. Spontaneous regression of a pancreatic metastasis of a renal cell carcinoma. Arch. Fam. Med. 1998, 7, 516–517. [Google Scholar] [CrossRef]
- Butturini, G.; Bassi, C.; Falconi, M.; Salvia, R.; Caldiron, E.; Iannucci, A.; Zamboni, G.; Grazinai, R.; Procacci, C.; Pederzoli, P.; et al. Surgical treatment of pancreatic metastases from renal cell carcinomas. Dig. Surg. 1998, 15, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Lallu, S.; Delahunt, B. Fine-needle aspiration cytology of metastatic clear-cell renal carcinoma presenting as a solitary mass in the head of the pancreas. Diagn. Cytopathol. 1998, 19, 194–197. [Google Scholar] [CrossRef]
- Hashimoto, M.; Watanabe, G.; Matsuda, M.; Dohi, T.; Tsurumaru, M. Management of pancreatic metastases from renal cell carcinoma: Report of four resected cases. Hepatogastroenterology 1998, 45, 1150–1154. [Google Scholar] [PubMed]
- Jingu, K.; Watanabe, K.; Yamamoto, H.; Fujita, Y.; Honda, I.; Watanabe, S.; Nagata, M.; Sugimoto, K.; Watanabe, Y.; Fujita, Y.; et al. Surgical treatment of a solitary pancreatic metastasis from renal cell carcinoma: Report of a case. Surg. Today 1998, 28, 91–94. [Google Scholar] [CrossRef]
- Merkle, E.M.; Boaz, T.; Kolokythas, O.; Haaga, J.R.; Lewin, J.S.; Brambs, H.J. Metastases to the pancreas. Br. J. Radiol. 1998, 71, 1208–1214. [Google Scholar] [CrossRef]
- Sahin, M.; Foulis, A.A.; Poon, F.W.; Imrie, C.W. Late focal pancreatic metastasis of renal cell carcinoma. Dig. Surg. 1998, 15, 72–74. [Google Scholar] [CrossRef]
- Z´graggen, K.; Fernandez-del Castillo, C.; Rattner, D.; Sigala, H.; Warshaw, A. Metastases to the pancreas and their surgical extirpation. Arch. Surg. 1998, 133, 413–417. [Google Scholar] [CrossRef]
- Augustin, H.; Bacher, H.; Uggowitzer, M.; Ott, A.; Hubmer, G.; Mischinger, H. Pancreatic metastases from renal cell carcinoma mimicking insulinomas. BJU Int. 1999, 83, 140–141. [Google Scholar] [CrossRef] [PubMed]
- Carucci, L.; Siegelman, E.; Feldman, M. Pancreatic metastasis from clear cell renal carcinoma: Diagnosis with chemical shift MRI. J. Comput. Assist. Tomogr. 1999, 23, 934–936. [Google Scholar] [CrossRef]
- Eriguchi, N.; Aoyagi, S.; Hara, M.; Miyazaki, T.; Hashino, K.; Imamura, I.; Jimi, A.; Naito, H.; Miyazaki, T.; Hashimo, K.; et al. A resected case of pancreatic metastasis from primary renal cell carcinoma. Kurume Med. J. 1999, 46, 119–122. [Google Scholar] [CrossRef]
- Ng, C.S.; Loyer, E.M.; Iyer, R.B.; David, C.L.; DuBrow, R.A.; Charnsangavej, C. Metastases to the pancreas from renal cell carcinoma: Findings on three-phase contrast-enhanced helical CT. AJR 1999, 172, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, M.; Katsura, M.; Yamamoto, K.; Nouchi, W.; Abe, N.; Hatano, N.; Atomi, Y. Pancreatic metastasis from renal cell carcinoma causing massive gastrointestinal bleeding in von Hippel-Lindau disease. Hepatogastroenterology 1999, 46, 1199–1201. [Google Scholar] [PubMed]
- Yavaşçaoğlu, I.; Korun, N.; Oktay, B.; Simsek, U.; Ozyurt, M. Renal cell carcinoma with solitary synchronous pancreaticoduodenal and metachronous periprostatic metastases: Report of a case. Surg. Today 1999, 29, 364–366. [Google Scholar] [CrossRef]
- Fricke, P.; Schulz, H.U.; Buhtz, B.; Lippert, H. Multiple metachrone Metastasen eines Nierenzellkarzinoms im Pankreas. Fallbeschreibung und Literaturübersicht. Chirurg 2000, 71, 575–579. [Google Scholar] [CrossRef]
- Ghavamian, R.; Klein, K.A.; Stephens, D.H.; Welch, T.J.; LeRoy, A.J.; Richardson, R.L.; Burch, P.A.; Zincke, H. Renal cell carcinoma metastatic to the pancreas: Clinical and radiological features. Mayo Clin. Proc. 2000, 75, 581–585. [Google Scholar] [CrossRef]
- Kassabian, A.; Stein, J.; Jabbour, N.; Parsa, K.; Skinner, D.; Parekh, D.; Cosenza, C.; Selby, R. Renal cell carcinoma metastatic to the pancreas: A single institution series and review of the literature. Urology 2000, 56, 211–215. [Google Scholar] [CrossRef]
- Le Borgne, J.; Partensky, C.; Glemain, P.; Dupas, B.; de Kerviller, B. Pancreaticoduodenectomy for metastatic ampullary and pancreatic tumors. Hepatogastroenterology 2000, 47, 540–544. [Google Scholar]
- Mehta, N.; Volpe, C.; Haley, T.; Balos, L.; Bradley, E.L.; Doerr, R.J. Pancreaticoduodenectomy for metastatic renal cell carcinoma: Report of a case. Surg. Today 2000, 30, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.D.; Heffess, C.S. Renal cell carcinoma to the pancreas in surgical pathology material. Cancer 2000, 89, 1076–1089. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, R.; Rossi, R.; Rossi, R.; Rosenberg, H. Metachronous pancreatic metastasis of a renal cell carcinoma: 3 new cases. Rev. Med. Chil. 2001, 129, 86–90. [Google Scholar] [PubMed]
- Faure, J.P.; Tuech, J.J.; Richer, J.P.; Pessaux, P.; Arnaud, J.P.; Carretier, M. Pancreatic metastasis of renal cell carcinoma: Presentation, treatment and survival. J. Urol. 2001, 165, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Marusch, F.; Koch, A.; Dietrich, F.; Hoschke, B.; Gastinger, I. A singular late metastasis of renal cell carcinoma inside the pancreas. An uncommon pancreatic tumor. Zentralbl. Chir. 2001, 126, 391–395. [Google Scholar] [CrossRef]
- Ruibal Moldes, M.; Quintana de la Rosa, J.; Farina Perez, L.; Tardaguila, F.; Ortiz Rey, J.; Zungri Telo, E. Late pancreatic metastasis from renal carcinoma. Actas Urol. Esp. 2001, 25, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Scatarige, J.; Horton, K.; Sheth, S.; Fishman, E. Pancreatic parenchymal metastases: Observations on helical CT. Am. J. Roentenol. 2001, 176, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Sohn, T.A.; Yeo, C.J.; Cameron, J.L.; Nakeeb, A.; Lillemoe, K.D. Renal cell carcinoma metastatic to the pancreas: Results of surgical management. J. Gastrointest. Surg. 2001, 5, 346–351. [Google Scholar] [CrossRef]
- Tada, T.; Kobayashi, G.; Noda, Y.; Kimura, K.; Ito, K.; Fujita, N. A resected case with multiple pancreatic metastasis of renal cell carcinoma. Nippon Shokakibyo Gakkai Zasshi 2001, 98, 1368–1373. [Google Scholar]
- Béchade, D.; Palazzo, I.; Desramé, J.; Duvic, C.; Hérody, M.; Didelot, F.; Coutant, G.; Algayres, J. Pancreatic metastasis of renal carcinoma: Report of three cases. Rev. Med. Interne 2002, 23, 862–866. [Google Scholar] [CrossRef]
- Chao, K.; Hurley, J.; Neerhut, G.; Kiroff, G. Multiple pancreatic metastases from renal cell carcinoma. ANZ J. Surg. 2002, 72, 310–312. [Google Scholar] [CrossRef]
- Chou, Y.; Chiou, H.; Hong, T.; Tiu, C.; Chiou, S.; Su, C.; Tsay, S. Solitary metastasis from renal cell carcinoma presenting as diffuse pancreatic enlargement. J. Clin. Ultrasound 2002, 30, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Eloubeidi, M.A.; Jhala, D.; Chhieng, D.C.; Jhala, N.; Eltoum, I.; Wilcox, C.M. Multiple late asymptomatic pancreatic metastases from renal cell carcinoma: Diagnosis by endoscopic ultrasound-guided fine needle aspiration biopsy with immunocytochemical correlation. Dig. Dis. Sci. 2002, 47, 1839–1842. [Google Scholar] [CrossRef] [PubMed]
- Hiotis, S.; Klimstra, D.; Conlon, K.; Brennan, M. Results after pancreatic resection for metastatic lesions. Ann. Surg. Oncol. 2002, 9, 675–679. [Google Scholar] [CrossRef]
- Lisii, D.; Gaimant, A.; Sautereau, D.; Paraf, F.; Maubon, A. Duodenal bleeding revealing a renal cell carcinoma. Gastroenterol. Clin. Biol. 2002, 26, 1044–1046. [Google Scholar] [PubMed]
- Peschaud, F.; Cheynel, N.; Hagry, O.; Tremeaux, J.C.; Rat, P.; Favre, J.P. Surgical treatment of pancreatic metastases from renal carcinoma. Ann. Chir. 2002, 127, 527–531. [Google Scholar] [CrossRef]
- Roviello, F.; Nastri, G.; Hako, L.; Marrelli, D.; De Stefano, A.; Cioppa, T.; Pinto, E. Pancreatic metastasis from clear renal cell carcinoma: A clinical case. Chir. Ital. 2002, 54, 873–877. [Google Scholar] [PubMed]
- Yachida, S.; Fukushima, N.; Kanai, Y.; Nimura, S.; Shimada, K.; Yamamoto, J.; Sakamoto, M. Pancreatic metastasis from renal cell carcinoma extending into the main pancreatic duct: A case report. Jpn. J. Clin. Oncol. 2002, 32, 315–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassi, C.; Butturini, G.; Falconi, M.; Sargenti, W.; Mantovavi, W.; Pederzoli, P. High recurrence rate after atypical resection for pancreatic metastases from renal cell carcinoma. Br. J. Surg. 2003, 90, 555–559. [Google Scholar] [CrossRef]
- Giulini, S.; Portolani, N.; Bonardelli, S.; Baiocchi, G.; Zampatti, N.; Coniglio, A.; Baronchelli, C. Distal pancreatic resection with splenic preservation for metastasis of renal carcinoma diagnosed 24 years later from the nephrectomy. Ann. Ital. Chir. 2003, 74, 93–96. [Google Scholar]
- Hernandez, D.J.; Kavoussi, L.R.; Ellison, L. Laparoscopic distal pancreatectomy for metastatic renal cell carcinoma. Urology 2003, 62, 551. [Google Scholar] [CrossRef] [PubMed]
- Law, C.H.; Wei, A.C.; Hanna, S.S.; Al-Zahrani, M.; Taylor, B.R.; Greig, B.; Langer, B.; Gallinger, S.; Al-Zahrani, M.; Taylor, B.; et al. Pancreatic resection for metastatic renal cell carcinoma: Presentation, treatment and outcome. Ann. Surg. Oncol. 2003, 10, 922–926. [Google Scholar] [CrossRef] [PubMed]
- Nakagohri, T.; Konishi, M.; Inoue, K.; Nakamura, T.; Kinoshita, T. Partial pancreatic head resection for pancreatis metastasis from renal cell carcinoma. Hepatogastroenterology 2003, 50, 2236–2238. [Google Scholar]
- Pecchi, A.; Cesinaro, A.; Torricelli, P. Solitary pancreatic metastasis from renal cell carcinoma. A case report. Radiol. Med. 2003, 105, 386–390. [Google Scholar]
- Uemura, T.; Kurita, A.; Nishimura, R.; Ishizaki, M.; Takashima, S. Solitary pancreatic metastasis from renal cell carcinoma concomitant with early gastric cancer 17 years after nephrectomy. Report of a case. Surg. Today 2003, 33, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Sellner, F.; Tykalsky, N.; De Santis, M.; Pont, J.; Klimpfinger, M. Solitary and multiple isolated metastases of clear cell renal carcinoma: An indication for pancreatic surgery. Ann. Surg. Oncol. 2006, 13, 75–85. [Google Scholar] [CrossRef]
- Zacharoulis, D.; Asopa, V.; Karvounis, E.; Williamson, R.C. Resection of renal metastases to the pancreas: A surgical challenge. HPB. 2003, 5, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Kijvikai, K.; Ratana-olarn, K. Solitary pancreatic metastasis from renal cell carcinoma 14 years after nephrectomy: A case report. J. Med. Assoc. Thai. 2004, 87, 1123–1126. [Google Scholar]
- Kobayashi, A.; Yamaguchi, T.; Ishihara, T.; Tadenuma, H.; Nakamura, K.; Ohshimi, T.; Sakaue, N.; Baba, T.; Yoshikawa, M.; Saisho, H. Spontaneous rupture of pancreatic metastasis from renal cell carcinoma. Jpn. J. Clin. Onco. 2004, 34, 696–699. [Google Scholar] [CrossRef] [Green Version]
- Kornprat, P.; Bacher, H.; Hauser, H.; Cerwenka, H.; El-Shabrawi, A.; Lackner, C.; Mischinger, H.J. Renal cell carcinoma with metastasis to the pancreas: A case report and literature review. Eur. Surg. 2004, 36, 381–384. [Google Scholar] [CrossRef]
- Moussa, A.; Mitry, E.; Hammel, P.; Sauvanet, A.; Nassif, T.; Palazzo, L. Pancreatic metastasis: A multicentric study of 22 patients. Gastroenterol. Clin. Biol. 2004, 28, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Paparel, P.; Cotton, F.; Voiglio, E.; Decaussin, M.; Isaac, S.; Caillot, J.L. A case of late pancreatic metastasis from renal cell carcinoma. Prog. Urol. 2004, 14, 403–405. [Google Scholar]
- Ninan, S.; Jain, P.K.; Paul, A.; Menon, K.V. Synchronous pancreatic metastases from asymptomatic renal cell carcinoma. JOP 2005, 6, 26–28. [Google Scholar] [PubMed]
- Pekmezci, S.; Saribeyoglu, K.; Kahya, A.S.; Kapan, M.; Durgun, V. Pancreatic renal cell carcinoma metastasis presenting with upper gastrointestinal bleeding. Surgery 2005, 137, 386–387. [Google Scholar] [CrossRef]
- Sotiropoulos, G.C.; Lang, H.; Liu, C.; Brokalaki, E.I.; Molmenti, E.; Broelsch, C.E. Surgical treatment of pancreatic metastases of renal cell carcinoma. JOP 2005, 6, 339–343. [Google Scholar] [PubMed]
- Wente, M.N.; Kleef, J.; Esposito, I.; Hartel, M.; Müller, M.W.; Fröhlich, E.; Büchler, M.W.; Friess, H. Renal cancer cell metastasis into the pancreas: A single-center experience and overview of the literature. Pancreas 2005, 30, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Crippa, S.; Angelini, C.; Mussi, C.; Bonardi, C.; Romano, F.; Sartori, P.; Uggeri, F.; Bovo, G. Surgical treatment of metastatic tumors to the pancreas: A single center experience and review of the literature. World J. Surg. 2006, 30, 1536–1542. [Google Scholar] [CrossRef]
- Köhler, K.; Haroske, G.; Ludwig, K. Management of pancreatic metastases from renal cell carcinoma. Report of five cases. Zentralbl. Chir. 2006, 131, 425–428. [Google Scholar] [CrossRef]
- Shrikhande, S.V.; Büchler, P.; Esposito, I.; Loos, M.; Büchler, M.W.; Friess, H. Splenic and portal vein thrombosis in pancreatic metastasis from renal cell carcinoma. World. J. Surg. Oncol. 2006, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- Akatsu, T.; Shimazu, M.; Aiura, K.; Ito, Y.; Shinoda, M.; Kawachi, S.; Tanabe, M.; Ueda, M.; Kitajima, M.; Kitagawa, Y. Clinicopathological features and surgical outcome of isolated metastasis of renal cell carcinoma. Hepatogastroenterology 2007, 54, 1836–1840. [Google Scholar]
- Eidt, S.; Jergas, M.; Schmidt, R.; Siedek, M. Metastasis to the pancreas—An indication for pancreatic resection? Langenbecks Arch. Surg. 2007, 392, 539–542. [Google Scholar] [CrossRef]
- Goto, T.; Dohmen, T.; Yoneyama, K. Pancreatic metastasis from renal cell carcinoma. Clin. Gastroenterol. Hepatol. 2007, 5, A26. [Google Scholar] [CrossRef] [PubMed]
- Karimi, K.M.; McFadden, D.W. Pancreatic resection for metastatic renal cell carcinoma to the pancreas. Am. Surg. 2007, 73, 58–60. [Google Scholar] [CrossRef]
- Maeda, H.; Okabayashi, T.; Nishimori, I.; Kobayashi, M.; Sugimoto, T.; Kohsaki, T.; Onishi, S.; Hanazaki, K. Duodenum-preserving pancreatic head resection for pancreatic metastasis from renal cell carcinoma: A case report. Langenbecks Arch. Surg. 2007, 392, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Varker, K.A.; Muscarella, P.; Wall, K.; Ellison, C.; Bloomston, M. Pancreatectomy for non-pancreatic malignancies results in improved survival after R0 resection. World. J. Surg. Oncol. 2007, 5, 145. [Google Scholar] [CrossRef] [PubMed]
- Aimoto, T.; Uchida, E.; Yamahatsu, K.; Yoshida, H.; Hiroi, M.; Tajiri, T. Surgical treatment for isolated multiple pancreatic metastases from renal cell carcinoma: Report of a case. J. Nippon Med. Sch. 2008, 75, 221–224. [Google Scholar] [CrossRef] [Green Version]
- Bahra, M.; Jacob, D.; Langrehr, J.M.; Glanemann, M.; Schumacher, G.; Lopez-Hänninen, E.; Neuhaus, P. Metastasen im Pankreas. Wann ist eine Resektion sinnvoll? Chirurg 2008, 79, 241–248. [Google Scholar] [CrossRef]
- Kawakami, H.; Kuwatani, M.; Yamato, H.; Shinada, K.; Hirano, S.; Kondo, S.; Yonemori, A.; Matsuno, Y.; Asaka, M. Pancreatic metastasis from renal cell carcinoma with intraportal tumor thrombus. Inter. Med. 2008, 47, 1967–1970. [Google Scholar] [CrossRef] [Green Version]
- Matsutani, T.; Sasajima, K.; Miyamoto, M.; Yokoyama, T.; Maruyama, H.; Yanagi, K.; Matsuda, A.; Kashiwabara, M.; Suzuki, S.; Tajiri, T. Resection of pancreatic metastasis from renal cell carcinoma and an early gastric cancer. J. Nippon Med. Sch. 2008, 75, 41–45. [Google Scholar] [CrossRef] [Green Version]
- Koide, N.; Yokoyama, Y.; Oda, K.; Nishio, H.; Ebata, T.; Abe, T.; Igami, T.; Nimura, Y.; Nagino, M. Pancreatic metastasis from renal cell carcinoma. Results of the surgical management and pathologic findings. Pancreas 2008, 37, 104–107. [Google Scholar] [CrossRef]
- Schauer, M.; Vogelsang, H.; Siewert, J.R. Pancreatic resection for metastatic renal cell carcinoma: A single center experience and review of the literature. Anticancer Res. 2008, 28, 361–366. [Google Scholar] [PubMed]
- Shukla, R.C.; Pathak, R.; Senthil, S. Pancreatic metastases of renal cell carcinoma—Case report. Nepal. Med. Coll. J. 2008, 10, 275–277. [Google Scholar] [PubMed]
- Tuech, J.; Lefebure, R.; Bridoux, V.; Albouy, B.; Lermite, E.; Le Pessot, F.; Le Blanc-Louvry, I.; Michot, F. Combined resection of the pancreas and inferior vena cava for pancreatic metastasis from renal cell carcinoma. J. Gastrointest. Surg. 2008, 12, 612–615. [Google Scholar] [CrossRef]
- Zerbi, A.; Ortolano, E.; Balzano, G.; Borri, A.; Beneduce, A.A.; Di Carlo, V. Pancreatic metastasis from renal cell carcinoma: Which patients benefit from surgical resection? Ann. Surg. Oncol. 2008, 15, 1161–1168. [Google Scholar] [CrossRef]
- Deguchi, Y.; Shimada, K.; Nara, S.; Esaki, M.; Sakamoto, Y.; Kosuge, T.; Hiraoka, N. Pancreaticojejunostomy with invagination of the punched pancreatic remnant after medial pancreatectomy and enucleation for multiple metastases of renal cell carcinoma: Report of a case. Surg. Today 2009, 39, 1086–1090. [Google Scholar] [CrossRef]
- Machado, N.O.; Chopra, P. Pancreatic metastasis from renal carcinoma managed by Whipple resection. A case report and literature review of metastatic pattern, surgical management and outcome. JOP 2009, 10, 413–418. [Google Scholar] [PubMed]
- Tanis, P.J.; van der Gaag, N.A.; Busch, O.R.; van Gulik, T.M.; Gouma, D.J. Systematic review of pancreatic surgery for metastatic renal cell carcinoma. Br. J. Surg. 2009, 96, 579–592. [Google Scholar] [CrossRef]
- Volk, A.; Kersting, S.; Konopke, R.; Dobrowolski, F.; Franzen, S.; Ockert, D.; Grützmann, R.; Saeger, H.D.; Bergert, H. Surgical therapy of intrapancreatic metastasis from renal cell carcinoma. Pancreatology 2009, 9, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Akashi, Y.; Saiura, A.; Kishi, Y.; Koga, R.; Morimura, R.; Yoshioka, R.; Yamamoto, J.; Yamaguchi, T. Outcome after surgical resection of isolated metastases to the pancreas. Hepatogastroenterology 2010, 57, 1549–1552. [Google Scholar]
- Barbaros, U.; Sümer, A.; Demirel, T.; Karakullukçu, N.; Batman, B.; Içscan, Y.; Sariçam, G.; Serin, K.; Loh, W.L.; Dinççag, A.; et al. Single incision laparoscopic pancreas resection for pancreatic metastasis of renal cell carcinoma. JSLS. 2010, 14, 566–570. [Google Scholar] [CrossRef] [Green Version]
- Hijioka, S.; Hifumi, M.; Mekky, M.; Takekuma, Y.; Kawaguchi, T.; Yokomizo, H.; Sato, T. Total pancreatectomy for metastatic renal cell carcinoma with marked extension into the main pancreatic duct. Inter. Med. 2010, 49, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitasato, A.; Tajima, Y.; Kuroki, T.; Tsutsumi, R.; Tsuneoka, N.; Adachi, T.; Mishima, T.; Kanematsu, T. Limited pancreatectomy for metastatic pancreatic tumors from renal cell carcinoma. Hepatogastroenterology 2010, 57, 354–357. [Google Scholar] [PubMed]
- Konstantinidis, I.; Dursun, A.; Zheng, H.; Wargo, J.; Thayer, S.; Castillo, C.; Warshaw, A.; Ferrone, C. Metastatic tumors in the pancreas in the modern era. J. Am. Coll. Surg 2010, 211, 749–753. [Google Scholar] [CrossRef] [Green Version]
- Masetti, M.; Zanini, N.; Martuzzi, F.; Fabbri, C.; Mastrangelo, L.; Landolfo, G.; Fornelli, A.; Burzi, M.; Vezzelli, E.; Jovine, E. Analysis of prognostic factors in metastatic tumors of the pancreas: A single-center experience and review of the literature. Pancreas 2010, 39, 135–143. [Google Scholar] [CrossRef]
- Mourra, N.; Arrive, L.; Balladur, P.; Flejou, J.F.; Tiret, E.; Paye, F. Isolated metastatic tumors to the pancreas. Pancreas 2010, 39, 577–580. [Google Scholar] [CrossRef]
- Szabó, K.G.; Szentkereszty, Z.; Tóth, L.A.; Damjanovich, L.; Sápy, P. Distal pancreas resection for metastasis of clear cell renal cancer. Magy. Seb. 2010, 63, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Vujcic, T.; Brahm, J.; Buckel, E.; Ibarra, A.; Vial, M.T.; Fernández, M. Pancreatic metastasis from renal cell carcinoma: A case report. Rev. Med. Chile. 2010, 138, 738–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokonishi, T.; Ito, Y.; Osaka, K.; Komiya, A.; Kobayashi, K.; Sakai, N.; Noguchi, S.; Kishi, H.; Satomi, Y.; Mogaki, M.; et al. Tsuura Y.; Mizuno N.; Ikeda I. Pancreatic metastasis from renal cell carcinoma 25 years after radical nephrectomy. Hinyokika Kiyo. 2010, 56, 629–633. [Google Scholar]
- D’Ambra, M.; Ricci, C.; Casadei, R.; Minni, F. Pancreatic metastasis from renal cell carcinoma. Urologia 2011, 78 (Suppl. S18), 5–8. [Google Scholar] [CrossRef] [PubMed]
- Irigoin, R.R.; Entrenas, A.O.; Urbano, V.A.; Marin, J.G.; Salgado, T.P.; Zabal, J.M.; Adan, N.G. Solitary pancreatic metastasis from renal carcinoma. Gastroenterol. Hepatol. 2011, 34, 624–628. [Google Scholar] [CrossRef]
- Masago, T.; Watanabe, T.; Nemoto, R. Small renal cell carcinoma with pancreas metastasis: A case report. Hinyokika Kiyo. 2011, 57, 607–610. [Google Scholar]
- Miyao, N.; Naito, S.; Ozono, S.; Shinohara, N.; Masumori, N.; Igarashi, T.; Nakao, M.; Tsushima, T.; Senga, Y.; Horie, S.; et al. Late recurrence of renal cell carcinoma: Retrospective and collaborative study of the japanese society of renal cancer. Urology 2011, 77, 379–384. [Google Scholar] [CrossRef]
- Thadani, A.; Pais, S.; Savino, J. Metastasis of renal cell carcinoma to the pancreas 13 years postnephrectomy. Gastroenterol. Hepatol. 2011, 7, 697–699. [Google Scholar]
- Watanabe, T.; Morinaga, S.; Numata, M.; Mikayama, Y.; Tamura, S.; Tamagawa, H.; Yamamoto, N.; Shiozawa, M.; Ohkawa, S.; Kameda, Y.; et al. Pancreatic resection for metastatic tumors to the pancreas. Gan Kagaku Ryoho 2011, 38, 2068–2070. [Google Scholar]
- You, D.D.; Choi, D.W.; Choi, S.H.; Heo, J.S.; Kim, W.S.; Ho, C.Y.; Lee, H.G. Surgical resection of metastasis to the pancreas. J. Korean Surg. Soc. 2011, 80, 278–282. [Google Scholar] [CrossRef] [Green Version]
- Alzahrani, M.; Schmulewitz, N.; Grewal, S.; Lucas, F.; Turner, K.; McKenzie, J.; Sussman, J.; Ahmad, S. Metastases to the pancreas: The experience of. a high volume center and a review of the literature. J. Surg. Oncol. 2012, 105, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Çomunoğlu, C.; Altaca, G.; Demiralay, E.; Moray, G. Multiple metastatic renal cell carcinoma isolated to pancreas. Malays. J. Pathol. 2012, 34, 63–66. [Google Scholar] [PubMed]
- Firek, P.; Richter, S.; Jaekel, J.; Brehmer, B.; Heidenreich, A. Metastasectomy in renal cell cancer after neoadjuvant therapy with multi-tyrosine kinase inhibitors. Urologe 2012, 51, 398–402. [Google Scholar] [CrossRef]
- Gardini, A.; Morgagni, P.; Milandri, C.; Riccobon, A.; Ridolfi, R.; La Barba, G.; Saragoni, L.; Amadori, D.; Garcea, D. Pancreatic resection for metastases from renal cancer: Long term outcome after surgery and immunotherapy approach—Single center experience. Hepatogastroenterology 2012, 59, 687–690. [Google Scholar] [CrossRef]
- Hung, J.H.; Wang, S.E.; Shyr, Y.M.; Su, C.H.; Chen, T.H.; Wu, C.W. Resection for secondary malignancy of the pancreas. Pancreas. 2012, 41, 121–129. [Google Scholar] [CrossRef]
- Katsourakis, A.; Noussios, G.; Hadjis, I.; Alatsakis, M.; Chatzitheoklitos, E. Late solitary pancreatic metastasis from renal cell carcinoma: A case report. Case Rep. Med. 2012, 2012, 464808. [Google Scholar] [CrossRef] [PubMed]
- Yazbek, T.; Gayet, B. The place of enucleation and enucleo-resection in the treatment of pancreatic metastasis of renal cell carcinoma. JOP 2012, 13, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Zygulska, A.L.; Wójcik, A.; Richter, P.; Krzesiwo, K. Renal carcinoma metachronous metastases to the gall-bladder and pancreas--case report. Pol. Przegl. Chir. 2012, 84, 313–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hata, T.; Sakata, N.; Aoki, T.; Yoshida, H.; Kanno, A.; Fujishima, F.; Motoi, F.; Masamune, A.; Shimosegawa, T.; Unno, M. Repeated pancreatectomy for metachronous duodenal and pancreatic metastases of renal cell carcinoma. Case Rep. Gastroenterol. 2013, 7, 442–448. [Google Scholar] [CrossRef]
- Hoshino, Y.; Shinozaki, H.; Kimura, Y.; Masugi, Y.; Ito, H.; Terauchi, T.; Kimatam, M.; Furukawa, J.; Kobayashi, K.; Ogata, Y. Pancreatic metastases from renal cell carcinoma: A case report and literature review of the clinical and radiological characteristics. World J. Surg. Oncol. 2013, 11, 289. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, R.; Kumar, R.; Dey, P.; Mittal, B.R. A late recurrence of renal cell carcinoma as pancreatic metastases: A rare disease. BMJ Case Rep. 2013, 2013, bcr2013009314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markinez, I.; Jiménez, R.; Ruiz, I.; Villarreal, E.; Lizarazu, A.; Borda, N.; Arteaga, X.; Medrano, M.Á.; Guisasola, E.; Beguiristain, A.; et al. Pancreatic metastases due to renal carcinoma. Our cases and a literature review. Cir. Esp. 2013, 91, 90–95. [Google Scholar] [CrossRef]
- Mqirage, M.; Zabala Egurrola, J.; Rodríguez, J.; Pertusa Peña, C. Métastase pancréatique métachrone du cancer du rein: À propos d’un cas. Can. Urol. Assoc. J. 2013, 7, e460–e461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niess, H.; Conrad, C.; Kleespies, A.; Haas, F.; Bao, Q.; Jauch, K.W.; Graeb, C.; Bruns, C. Surgery for metastasis to the pancreas: Is it safe and effective? J. Surg. Oncol. 2013, 107, 859–864. [Google Scholar] [CrossRef]
- Simtniece, Z.; Kirsakmens, G.; Strumfa, I.; Vanaga, A.; Gardovskis, J. Delayed pancreatic metastasis of renal clear cell carcinoma. Acta Chir. Latv. 2013, 13, 79–80. [Google Scholar] [CrossRef]
- Yabe, N.; Murai, S.; Shimizu, H.; Kitasato, K.; Yoshikawa, T.; Oto, I.; Nakadai, J.; Hasegawa, H.; Kitagawa, Y. A case of pancreatic metastasis from renal cell carcinoma 27 years after nephrectomy. Gan Kagaku Ryoho. 2013, 40, 1897–1899. [Google Scholar]
- Yoshikawa, Y.; Murakami, M.; Shimizu, J.; Yasuyama, A.; Watase, C.; Kubota, M.; Miyake, Y.; Matsuura, Y.; Kim, H.M.; Hirota, M.; et al. A case of partial pancreatectomy for recurrent metastatic renal cell carcinoma in the remnant pancreas after subtotal stomach-preserving pancreaticoduodenectomy. Gan Kagaku Ryoho. 2013, 40, 1900–1902. [Google Scholar]
- Untsch, B.R.; Allen, P.J. Pancreatic metastasectomy: The Memorial Sloan-Kettering experience and a review of the literature. J. Surg. Oncol. 2014, 109, 28–30. [Google Scholar] [CrossRef]
- Espinoza, E.; Hassani, A.; Vaishampayan, U.; Shi, D.; Pontes, E.; Weaver, D. Surgical excision of duodenal/pancreatic metastatic renal cell carcin oma. Front Oncol 2014, 4, 218. [Google Scholar] [CrossRef] [Green Version]
- Lauro, S.; Onesti, E.C.; Righini, R.; Carbonetti, F.; Cremona, A.; Marchetti, P. A synchronous pancreatic metastasis from renal clear cell carcinoma, with unusual CT characteristics, completely regressed after therapy with sunitinib. Case Rep. Med. 2014, 2014, 473431. [Google Scholar] [CrossRef] [Green Version]
- Kimura, Y.; Keira, Y.; Imamura, M.; Ito, T.; Nobuoka, T.; Mizuguchi, T.; Masumori, N.; Hasegawa, T.; Hirata, K. Histopathological aspects of pancreatic metastases in renal cell carcinoma: Does the mode of invasion permit limited resections? Pancreat. Disord. Ther 2014, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Matsuki, M.; Ichihara, K.; Matsuda, Y.; Taguchi, K. Clinical features of six patients with pancreas metastasis from renal cell carcinoma. Hinyokika Kiyo. 2014, 60, 105–108. [Google Scholar] [PubMed]
- Macrì, A.; Fleres, F.; Putortì, A.; Lentini, M.; Ascenti, G.; Mastrojeni, C. Relapsed metachronous pancreatic metastasis from renal cell carcinoma (RCC): Report of a case and review of literature. Ann. Ital. Chir. 2014, 85, S2239253X1402283X. [Google Scholar]
- Minni, F.; Casadei, R.; Perence, B.; Greco, V.M.; Marrano, N.; Margiotta, A.; Marrano, D. Pancreatic metastases: Observations of three cases and review of the literature. Pancreatology. 2014, 4, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Moletta, L.; Milanetto, A.C.; Vincenzi, V.; Alaggio, R.; Pedrazzoli, S.; Pasquali, C. Pancreatic secondary lesions from renal cell carcinoma. World J. Surg. 2014, 38, 3002–3006. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, L.; Sauvanet, A.; Regenet, N.; Mabrut, J.Y.; Gigot, J.F.; Housseau, E.; Millat, B.; Ouaissi, M.; Gayet, B.; Fuks, D.; et al. Long-term survival after pancreatic resection for renal cell carcinoma metastasis. Ann. Surg. Oncol. 2014, 21, 4007–4013. [Google Scholar] [CrossRef] [PubMed]
- Takeshi, A.; Mitsuhiro, I.; Hiromitsu, A.; Naoyuki, Y.; Taiichiro, S.; Hiroki, S.; Takeaki, K.; Tatsuya, S.; Futoshi, O.; Hiroharo, S.; et al. Middle segment-preserving pancreatectomy for recurrent metastasis of renal cell carcinoma after pancreatoduodenenctomy: A case report. Case Rep. Surg. 2014, 2014, 648678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosoian, J.J.; Cameron, J.L.; Allaf, M.E.; Hruban, R.H.; Nahime, C.B.; Pawlik, T.M.; Pierorazio, P.M.; Reddy, S.; Wolfgang, C.L. Resection of isolated renal cell carcinoma metastases of the pancreas: Outcomes from the Johns Hopkins Hospital. J. Gastrointest. Surg. 2014, 18, 542–548. [Google Scholar] [CrossRef]
- Benhaim, R.; Oussoultzoglou, E.; Saeedi, Y.; Mouracade, P.; Bachellier, P.; Lang, H. Pancreatic metastasis from clear cell renal cell carcinoma: Outcome of an aggressive approach. Urology 2015, 85, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Liaw, C.; Chuang, C. The role of surgery in renal cell carcinoma with pancreatic metastasis. Biomed. J. 2015, 38, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Gajendra, S.; Sachdev, R.; Mohapatra, I.; Goel, R.; Goel, S. Metastatic renal cell carcinoma: An unusual cause of bleeding pancreatic mass. J. Clin. Diagn. Res. 2015, 9, ED15–ED17. [Google Scholar] [CrossRef]
- Kitade, H.; Yanagida, H.; Yamada, M.; Matsuura, T.; Yoshioka, K.; Satoi, S.; Matsui, Y.; Kon, M. Pylorus-preserving total pancreatectomy for metastatic renal cell carcinoma: A case report. J. Med. Case Rep. 2015, 9, 212. [Google Scholar] [CrossRef] [Green Version]
- Kusnierz, K.; Mrowiec, S.; Lampe, P. Results of surgical management of renal cell carcinoma metastatic to the pancreas. Contemp. Oncol. 2015, 19, 54–59. [Google Scholar] [CrossRef]
- Santoni, M.; Conti, A.; Partelli, S.; Porta, C.; Sternberg, C.N.; Procopio, G.; Bracarda, S.; Basso, U.; De Giorgi, U.; Derosa, L.; et al. Surgical resection does not improve survival in patients with renal metastases to the pancreas in the era of tyrosine kinase inhibitors. Ann. Surg. Oncol. 2015, 22, 2094–2100. [Google Scholar] [CrossRef]
- Wiltberger, G.; Bucher, J.N.; Kremnzien, F.; Atanasov, G.; Schemelzle, M.; Haum, H.M.; Bartels, M. Extended resection in pancratic metastases: Feasibility, frequency, and long-term-outcome: A retrospective analysis. BMC Surg. 2015, 15, 126. [Google Scholar] [CrossRef] [Green Version]
- Yuasa, T.; Inoshita, N.; Saiura, A.; Yamamoto, S.; Urakami, S.; Masusa, H.; Fujii, Y.; Fukui, I.; Ishikawa, Y.; Yonese, J. Clinical outcome of patients with pancreatic metastases from renal cell cancer. BMC Cancer 2015, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltazar, M.P.; Meirinha, A.; Joao, R.; Pina, M.J.; Pinheiro, H.; Fernandes, F.; Falcao, G.; Forte, J.P.; Carvalho, A.M.; Vigia, E.; et al. Obstructive jaundice as a rare presentation of metastatic renal cell carcinoma—Clinical case and literature review. Acta Urol. Port. 2016, 33, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Boussios, S.; Zerdes, J.; Batsi, O.; Papakostas, P.; Seraj, E.; Pentheroudakis, G.; Glantzounis, G. Pancreatic resection for renal cell carcinoma metastasis: An exceptionally rare coexistence. Int. J. Surg. Case Rep. 2016, 27, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Cong, L.; Zhang, T.P.; Zhao, Y.P. Pancreatic metastasis of renal cell carcinoma. Hepatobiliary Pancreat. Dis. Int. 2016, 15, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Fikatas, P.; Klein, F.; Andreou, A.; Schmuck, R.B.; Pratschke, J.; Bahra, M. Long-term survival after surgical treatment of renal cell carcinoma metastasis within the pancreas. Anticancer Res. 2016, 36, 4273–4278. [Google Scholar]
- Koga, C.; Murakami, M.; Shimizu, J.; Matsumara, T.; Kameda, C.; Kawabata, R.; Oda, N.; Hirota, M.; Yoshikawa, M.; Morishima, H.; et al. A case of multiple pancreatic metastases from renal cell carcinoma diagnosed using EUS-FNA. Gan Kagaku Ryoho 2016, 43, 2356–2358. [Google Scholar]
- Miura, T.; Nakamura, N.; Ogawa, K.; Watanabe, Y.; Yonekura, K.; Sanada, T.; Kuwabara, H.; Goseki, N. Resection of pancreatic metastasis from renal cell carcinoma 21 years after nephrectomy. Gan Kagaku Ryoho 2016, 43, 2187–2189. [Google Scholar]
- Nihei, K.; Sakamoto, K.; Suzuki, S.; Mishina, T.; Otaki, M. A case of pancreatic metastasis of renal cell carcinoma. Gan To Kagaku Ryoho. 2016, 43, 2274–2276. [Google Scholar]
- Rückert, F.; Distler, M.; Ollmann, D.; Lietzmann, A.; Birgin, E.; Teoule, P.; Grützmann, R.; Wilhelm, T.J. Retrospective analysis of survival after resection of pancreatic renal cell carcinoma metastases. Int. J. Surg. 2016, 26, 64–68. [Google Scholar] [CrossRef]
- Chatzizacharias, N.A.; Rosich-Medina, A.; Dajani, K.; Harper, S.; Huguet, E.; Liau, S.S.; Praseedom, R.K.; Jah, A. Surgical management of hepato-pancreatic metastasis from renal cell carcinoma. World J. Gastrointest. Oncol. 2017, 15, 70–77. [Google Scholar] [CrossRef]
- Garcia-Major Fernandez, R.L.; Fernandez-Gonzales, M. Diagnosis and treatment of isolated metastases from renal clear cell carcinoma: Report of a case and review of literature. Cr. Cir. 2017, 85, 436–439. [Google Scholar] [CrossRef] [Green Version]
- Ko, S.; Yun, S.; Kim, S.; Kim, T.; Seo, H. Pancreatic resection for renal cell carcinoma metastasis: A case review. Ann. Hepatobiliary Pancreat. Surg. 2017, 21, 176–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.R.; Gemenetzis, G.; Cooper, M.; Javed, A.A.; Cameron, J.L.; Wolfgang, C.L.; Eckhauser, F.E.; He, J.; Weiss, M.J. Long-term outcomes of 98 surgically resected metastatic tumors in the pancreas. Ann. Surg. Oncol. 2017, 24, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Shatveryan, G.A.; Chardarov, N.K.; Bagmet, N.N.; Ratnikova, N.P.; Bedzhanyan, A.L.; Petrenko, K.N.; Polishchuk, L.O.; Karagyozyan, G.A. Isolated pancreatic metastases of renal cell carcinoma. Khirurgiia 2017, 12, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Yagi, T.; Hashimoto, D.; Taki, K.; Yamamura, K.; Chikamoto, A.; Ohmuraya, M.; Beppu, T.; Baba, H. Surgery for metastatic tumors to the pancreas. Surg. Case Rep. 2017, 3, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zianne, M.; Takahashi, N.; Tsujibata, A.; Miwa, K.; Goto, Y.; Matano, Y. Asymptomatic pancreatic metastasis from renal cell carcinoma diagnosed 21 years after nephrectomy. Case Rep. Gastrointest. Med. 2017, 2017, 8765264. [Google Scholar] [CrossRef] [Green Version]
- Boni, A.; Cochetti, G.; Ascani, S.; Del Zingaro, M.; Quadrini, F.; Paladini, A.; Cocca, D.; Mearini, E. Robotic treatment of oligometastatic kidney tumor with synchronous pancreatic metastasis: Case report and review of the literature. BMC Surg. 2018, 18, 40. [Google Scholar] [CrossRef]
- Ito, T.; Takada, R.; Omoto, S.; Tsuda, M.; Masuda, D.; Kato, H.; Matsumoto, T.; Moriyama, I.; Okabe, Y.; Shiomi, H.; et al. Analysis of prognostic factors in pancreatic metastasis: A multicentre retrospective analysis. Pancreas 2018, 47, 1033–1039. [Google Scholar] [CrossRef]
- Kling, S.M.; Tannouri, S.; Jiang, W.; Yeo, C.J. Pancreatic mass in a patient with a history of resected renal cell carcinoma and resected adenocarcinoma of the ampulla of Vater: A case report. J. Pancreat. Cancer 2018, 4, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Limaiem, F.; Bouraoui, S. Metastasis of renal cell carcinoma to the pancreas 11 years postnephrectomy. Pan. Afr. Med. J. 2018, 30, 53. [Google Scholar] [CrossRef]
- Madkhali, A.; Shin, S.; Song, K.; Lee, J.; Hwang, D.; Paark, K.; Lee, Y.; Kim, S. Pancreatectomy for secondary metastasis to the pancreas. Medicine 2018, 97, e12653. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, M.; Dias, S.C.; Silva, A.C.; Pintob, J.; Machado, J. Solitary pancreatic renal cell carcinoma metastasis. Autops. Case Rep. 2018, 23, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, H.; Toyama, H.; Terai, S.; Mukubou, H.; Shirakawa, S.; Ishida, J.; Asakura, Y.; Shimizu, T.; Lee, D.; Tanaka, M.; et al. A patient with multiple pancreatic metastases undergoing total pancreatectomy 18 years after renal cell carcinoma resection. Gan Kagaku Ryoho. 2018, 45, 2214–2216. [Google Scholar]
- Yu, Q.; Kan, F.; Ma, Z.; Wang, T.; Lin, G.; Chen, B.; Zhao, W. CT Diagnosis for metastasis of clear cell renal cell carcinoma to the pancreas: Three case reports. Medicine 2018, 97, e13200. [Google Scholar] [CrossRef]
- Anderson, B.; Williams, G.; Sanford, D.E.; Lu, J.; Khan, A.S. A 22-year experience with pancreatic resection for metastatic renal cell carcinoma. HPB 2019. [Google Scholar] [CrossRef] [PubMed]
- Ayari, Y.; Ben Rhouma, S.; Boussaffa, H.; Chelly, B.; Hamza, K.; Sellami, A.; Jrad, M.; Nouira, Y. Metachronous isolated locally advanced pancreatic metastasis from chromophobe renal cell carcinoma. Int. J. Surg. Case Rep. 2019, 60, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Brozzetti, S.; Sterpetti, A.V. Unexpected prolonged survival after extended and emergent resection of pancreatic metastases from renal cell carcinoma. J. Gastrointest. Cancer 2019, 50, 1055–1058. [Google Scholar] [CrossRef] [PubMed]
- Chon, H.K.; Choi, K.H. Late metachronous isolated pancreatic metastasis from renal cell carcinoma mimicking a pancreatic neuroendocrine tumor. Turk. J. Gastroenterol. 2019, 30, 489–491. [Google Scholar] [CrossRef]
- Endo, Y.; Noda, H.; Watanabe, F.; Kato, T.; Kakizawa, N.; Ichida, K.; Kasahara, N.; Rikiyama, T. A retrospective analysis of preoperative evaluation and surgical resection for metastatic tumors of the pancreas. Indian J. Surg. Oncol. 2019, 10, 251–257. [Google Scholar] [CrossRef]
- Geramizadeh, B.; Kashkooe, A.; Nikeghbalian, S.; Malek-Hosseini, S. Metastatic tumors to the pancreas, a single center study. Arch. Iran. Med. 2019, 22, 50–52. [Google Scholar]
- Glinka, J.; Sanchez Claria, R.; Ardiles, V.; de Santibañes, E.; Pekolj, J.; de Santibañes, M.; Mazza, O. The pancreas as a target of metastasis from renal cell carcinoma: Results of surgical treatment in a single institution. Ann. Hepatobiliary Pancreat. Surg. 2019, 23, 240–244. [Google Scholar] [CrossRef]
- Huang, Q.; Zhou, H.; Liu, C.; Jin, K.; Fan, K.; Cheng, H.; Fan, Z.; Yang, C.; Liu, L.; Long, J.; et al. Surgical resection for metastatic tumors in the pancreas: A single-center experience and systematic review. Ann. Surg. Oncol. 2019, 26, 1649–1656. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.; Yang, I.S.; Song, S. Surgery for metastatic renal cell carcinoma in the pancreatic head: A case report and literature review. Ann. Hepatobiliary Pancreat. Surg. 2019, 23, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Yang, J.; Qin, K.; Zhou, Y.; Ying, X.; Yuan, F.; Shi, M.; Jin, J.; Wang, D.; Gu, J.; et al. Resection of pancreatic metastatic renal cell carcinoma: Experience and long-term survival outcome from a large center in China. Int. J. Clin. Oncol. 2019, 24, 686–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patyutko, Y.I.; Kotelnikov, A.G.; Kriger, A.G.; Prodkuryakov, I.S.; Galkin, G.V.; Polyakov, A.N.; Fainstein, I.A. Metastatic renal cell carcinoma in the pancreas: Experience of surgical treatment. Khirurgiia 2019, 9, 25–31. [Google Scholar] [CrossRef]
- Teranishi, R.; Hatanaka, N.; Hara, S.; Takayama, K.; Shimura, Y.; Ohashi, T.; Osawa, H.; Sakai, K.; Yasumasa, K.; Noro, H.; et al. Two cases of pancreatectomy for pancreatic metastasis from renal cell carcinoma. Gan Kagaku Ryoho. 2019, 46, 561–563. [Google Scholar]
- Yamaguchi, H.; Kimura, Y.; Nagayama, M.; Imamura, M.; Tanaka, S.; Yoshida, E.; Fujino, H.; Machiki, T.; Miyanishi, K.; Mizuguchi, T.; et al. Central pancreatectomy in portal annular pancreas for metastatic renal cell carcinoma: A case report. World J. Surg. Oncol. 2019, 17, 76. [Google Scholar] [CrossRef]
- Wakabayashi, T.; Uchida, T.; Oyama, H.; Shiozawa, T.; Kigawa, G.; Tanaka, K. A case of laparoscopic distal pancreatectomy for metachronous pancreatic metastasis from renal cell carcinoma. Nihon Rinsho Geka Gakkai Zasshi 2019, 80, 983–989. [Google Scholar] [CrossRef] [Green Version]
- Brozzetti, S.; Bini, S.; De Lio, N.; Lombardo, C.; Boggi, U. Surgical-only treatment of pancreatic and extra-pancreatic metastases from renal cell carcinoma—quality of life and survival analysis. BMC Surg. 2020, 20, 101. [Google Scholar] [CrossRef]
- Chikhladze, S.; Lederer, A.K.; ·Kühlbrey, C.M.; ·Hipp, J.; Sick, O.; Fichtner-Feigl, S.; Wittel, U.A. Curative-intent pancreas resection for pancreatic metastases: Surgical and oncological results. Clin. Exper. Metastasis 2020. [Google Scholar] [CrossRef]
- Choucair, K.; Parker, N.A.; Al-Obaidi, A.; Alderson, J.; Truong, P. Solitary, late metastatic recurrence of renal cell carcinoma to the pancreas: A case report. Cureus 2020, 12, e8521. [Google Scholar] [CrossRef]
- Di Franco, G.; Gianardi, D.; Palmeri, M.; Furbetta, N.; Guadagni, S.; Bianchini, M.; Bonari, F.; Sbrana, A.; Vasile, E.; Pollina, L.E.; et al. Pancreatic resections for metastases: A twenty-year experience from a tertiary care center. Eur. J. Surg. Oncol. 2020, 46, 825–831. [Google Scholar] [CrossRef]
- Fahlbusch, T.; Luu, A.M.; Braumann, C.; Lukas, C.; Uhl, W.; Künzli, B.M. Lipomatous pancreas facilitates late onset of renal cell carcinoma metastases. Acta Chir. Belg. 2020, 18, 1–6. [Google Scholar] [CrossRef]
- Janevska, V.; Shumkovski, A.; Nikolova, D.; Asani, L.; Pandilov, S.; Karanfilovski, V. Late onset of pancreatic metastases from renal cell carcinoma. A case report. Prilozi 2020, 41, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Milanetto, A.C.; Morelli, L.; Di Franco, G.; David, A.; Campra, D.; De Paolis, P.; Pasquali, C. A plea for surgery in pancreatic metastases from renal cell carcinoma: Indications and outcome from a multicenter surgical experience. J. Clin. Med. 2020, 9, 3278. [Google Scholar] [CrossRef]
- Rupert, K.; Kural, T.; Skalický, T.; Zeithaml, J.; Hess, O.; Třeška, V. Clear cell renal carcinoma metastases to the pancreas. Rozhl. Chir. 2020, 99, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Schammel, J.; Schammel, C.; Schammel, D.; Trocha, S.D. Renal cell carcinoma metastasis to the pancreas: The aggressive nature of synchronous presentation—Case report and comprehensive review of the literature. SN. Compr. Clin. Med. 2020, 2, 1272–1281. [Google Scholar] [CrossRef]
- Singla, N.; Xie, Z.; Zhang, Z.; Gao, M.; Yousuf, Q.; Onabolu, O.; McKenzie, T.; Tcheuyap, V.T.; Ma, Y.; Choi, J.; et al. McKay R, Christie A, Torras RO, Bowman IA, Margulis V, Pedrosa I, Przybycin C, Wang T, Kapur P, Rini B.; Brugarolas JP. Pancreatic tropism of metastatic renal cell carcinoma. JCI. Insight. 2020, 5, e134564. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.Y.; Li, X.Y.; Bai, C.M.; Zhou, Y.; Wu, X.; Yang, A.M.; Hua, S.R. The clinicopathologic features and prognostic analysis of pancreatic metastasis from clear cell renal cell carcinoma. Zhonghua Zhong Liu Za Zhi. 2020, 42, 44–49. [Google Scholar] [CrossRef]
- Zurimendi, G.G.; Ibarguren, R.L.; Castaños, D.L.; Pereda, R.F.; Olabarrieta, A.U.; Casasola-Rodriguez, G.G.; Egurrola, A.Z.; Amuza-Echevarria, A.A. Metastasis pancreaticas de tumor primario renal: Presentacion de una serie de casos y revision de la literatura. Arch. Esp. Urol 2020, 73, 147–154. [Google Scholar]
- Alayyaf, N.; AlQatari, A.A.; Altalib, A.; AlQattan, A.S.; AlShahrani, A.A. Management of very late pancreatic metastasis of renal cell carcinoma 8 years after radical nephrectomy: A report of a rare case. Am. J. Case Rep 2021, 22, e927921. [Google Scholar] [CrossRef] [PubMed]
- Bauschke, A.; Altendorf-Hofmann, A.; Deeb, A.A.; Kissler, H.; Tautenhahn, H.M.; Settmacher, U. Chirurgische Therapie von Leber und Pankreasmetastasen von Nierenzellkarzinomen. Chirurg 2021, 92, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Fernández, G.; Fondevila-Campo, C.; Sanjuanbenito, A.; Fabregat-Prous, J.; Secanella-Medayo, L.; Rotellar-Sastre, F.; Pardo-Sanchez, F.; Prieto-Calvo, M.; Marin-Ortega, H.; Sanchez-Cabus, S.; et al. Pancreatic metastases from renal cell carcinoma. Postoperative outcome after surgical treatment in a Spanish multicenter study. Eur. J. Surg. Oncol. 2022, 48, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Ksontini, F.; Khrouf, S.; Kacem, S.; Hadda, A.; Magherbi, H.; Chaker, Y.; Ayadi, M.; Ben Safta, Z. Pancreatic metastasis of renal cell carcinoma: A surgical indication for a disseminated disease. Case Rep. Med. 2021, 2021, 5579385. [Google Scholar] [CrossRef]
- Malleo, G.; Salvia, R.; Maggino, L.; Marchegiani, G.; D’Angelica, M.; DeMatteo, R.; Kingham, P.; Pulvirenti, A.; Sereni, E.; Jarnagin, W.R.; et al. Long-term outcomes after surgical resection of pancreatic metastases from renal clear-cell carcinoma. Ann. Surg. Oncol. 2021, 28, 3100–3108. [Google Scholar] [CrossRef]
- Matsui, S.; Ono, H.; Asano, D.; Ishikawa, Y.; Ueda, H.; Akahoshi, K.; Ogawa, K.; Kudo, A.; Tanaka, S.; Tanabe, M. Pancreatic metastasis from renal cell carcinoma presenting as gastrointestinal hemorrhage: A case report. J. Surg. Case Rep. 2021, 2021, rjab368. [Google Scholar] [CrossRef]
- Novotny, A.; Sell, E.; Mehrotra, S. Metastatic tumors to the pancreas, a 12-year single institution review. Diagn. Cytopathol. 2021, 49, 1233–1236. [Google Scholar] [CrossRef]
- Piskorz, Ł.; Mitura, K.; Olejniczak, W.; Misiak, P.; Jablonski, S. Atypical locations of renal cell carcinoma metastases to the pancreas and duodenum. Res. Rep. Urol. 2021, 13, 17–24. [Google Scholar] [CrossRef]
- Yamada, Y.; Sakai, A.; Abe, S.; Gonda, M.; Kobayashi, T.; Masusa, A.; Shiomi, H.; Sahirakawa, S.; Toyama, H.; Hyodo, T.; et al. Pancreatic metastasis of renal cell carcinoma filling into the duct of Santorini. Clin. J. Gastroenterol. 2021, 14, 905–909. [Google Scholar] [CrossRef]
- Yamawaki, M.; Takano, Y.; Noda, J.; Azami, T.; Kobayashi, T.; Niiya, F.; Maruoka, T.; Nagashama, M. A case of hemobilia caused by pancreatic metastasis of renal cell carcinoma treated with a covered metallic stent. Clin. J. Gastroenterol. 2022, 15, 210–215. [Google Scholar] [CrossRef]
- Cardoso, D.; Rosales, A.; Thiel, D.D.; Asbun, H.; Stauffer, J.A. Pancreatic metastasectomy of renal cell carcinoma: A single institution experience. Can. J. Urol. 2022, 29, 11020–11023. [Google Scholar]
- Itamoto, S.; Abe, T.; Oshita, A.; Hanada, K.; Nakahara, M.; Noriyuki, T. Repeat pancreatic resection for metachronous pancreatic metastasis from renal cell carcinoma: A case report. Int. J. Surg. Case Rep. 2022, 94, 107022. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.K.; Li, L.J.; He, Y.M.; Xu, Z.F. Misdiagnosis of pancreatic metastasis from renal cell carcinoma: A case report. World J. Clin. Cases 2022, 10, 9012–9019. [Google Scholar] [CrossRef] [PubMed]
- Yano, R.; Yokota, T.; Morita, M.; Amano, M.; Ochi, H.; Azemoto, N.; Mashiba, T.; Joko, K. A case of metastasis from renal cell carcinoma to ectopic pancreas diagnosed after resection. Intern. Med. 2022, 2022, 9731-22. [Google Scholar] [CrossRef]
- Sbitti, Y.; Debbagh, A.; Slimani, K.; Mahi, M.; Errihani, H.; Ichou, M. When tyrosine kinase inhibitor sunitinib can be discontinued in metastatic renal cell carcinoma to pancreas: A case report. J. Med. Case Rep. 2018, 20, 80. [Google Scholar] [CrossRef] [PubMed]
- Chara, L.; Rodriguez, B.; Holgado, E.; Ramirez, N.; Fernandez-Rañada, I.; Mohedano, N.; Arcediano, A.; Garcia, I.; Cassinello, J. An unusual metastatic renal cell carcinoma with maintained complete response to sunitinib treatment. Case Rep. Oncol. 2011, 4, 583–586. [Google Scholar] [CrossRef]
- Medioni, J.; Choueiri, T.K.; Zinzindohoué, F.; Cho, D.; Fournier, L.; Oudard, S. Response of renal cell carcinoma pancreatic metastasis to sunitinib treatment: A retrospective analysis. J. Urol. 2009, 181, 2470–2475. [Google Scholar] [CrossRef]
- Negishi, T.; Furubayashi, N.; Nakagawa, T.; Nishiyama, N.; Kitamura, H.; Hori, Y.; Kuroiwa, K.; Son, Y.; Seki, N.; Tomoda, T.; et al. Site specific response to Nivolumab in renal cell carcinoma. Anticancer Res. 2021, 41, 1539–1545. [Google Scholar] [CrossRef]
- Reddy, S.; Edil, B.H.; Cameron, J.L.; Pawlik, T.M.; Herman, J.M.; Gilson, M.M.; Campbell, K.A.; Schulick, R.D.; Ahuja, N.; Wolfgang, C.L. Pancreatic resection of isolated metastases from nonpancreatic primary cancers. Ann. Surg. Oncol. 2008, 15, 3199–3206. [Google Scholar] [CrossRef]
- Iacovelli, R.; Lanoy, E.; Albiges, L.; Escudier, B. Tumour burden is an independent prognostic factor in metastatic renal cell carcinoma. BJU Int. 2012, 110, 1747–1754. [Google Scholar] [CrossRef]
- Grassi, P.; Verzoni, E.; Mariani, L.; De Braud, F.; Coppa, J.; Mazzaferro, V.; Procopio, G. Prognostic role of pancreatic metastases from renal cell carcinoma: Results from an Italian center. Clin. Genitourin. Cancer 2013, 11, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Shaya, J.A.; Lin, X.; Weise, N.; Cabal, A.; Panian, J.; Derweesh, I.H.; McKay, R.R. Prognostic significance of pancreatic metastases in patients with advanced renal cell carcinoma treated with systemic therapy. Clin. Genitourin. Cancer 2021, 19, S1558–S7673. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.J.; Song, C.; Jeong, C.W.; Kwak, C.; Seo, S.; Kang, M.; Chung, J.; Hong, S.H.; Hwang, E.C.; Park, J.Y.; et al. Metastatic renal cell carcinoma to the pancreas: Clinical features and treatment outcome. J. Surg. Oncol. 2021, 123, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Dudani, S.; de Velasco, G.; Wells, J.C.; Gan, C.L.; Donskov, F.; Porta, C.; Pasini, F.; Lee, J.L.; Hansen, A.; Bjarnason, G.A.; et al. Evaluation of clear cell, papillary, and chromophobe renal cell carcinoma metastasis sites and association with survival. JAMA Netw. Open 2021, 4, e22021869. [Google Scholar] [CrossRef]
- Grassi, P.; Doucet, L.; Giglione, P.; Grünwald, V.; Melichar, B.; Galli, L.; De Giorgi, U.; Sabbatini, R.; Ortega, C.; Santoni, M.; et al. Clinical impact of pancreatic metastases from renal cell carcinoma: A multicenter retrospective analysis. PLoS ONE 2016, 11, e0151662. [Google Scholar] [CrossRef]
- Chrom, P.; Stec, R.; Bodnar, L.; Szczylik, C. Prognostic significance of pancreatic metastases from renal cell carcinoma in patients treated with tyrosine kinase inhibitors. Anticancer Res. 2018, 38, 359–365. [Google Scholar] [CrossRef] [Green Version]
- Kalra, S.; Atkinson, B.J.; Matrana, M.R.; Matin, S.F.; Wood, C.G.; Karam, J.A.; Tamboli, P.; Sircar, K.; Rao, P.; Corn, P.G.; et al. Prognosis of patients with metastatic renal cell carcinoma and pancreatic metastases. BJU Int. 2016, 117, 761–765. [Google Scholar] [CrossRef] [Green Version]
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of clear renal cell carcinoma. Nature 2013, 499, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Jonasch, E. Updates to the management of kidney cancers. J. Natl. Compr. Canc. Netw. 2018, 16, 639–641. [Google Scholar] [CrossRef]
- Mitchell, T.J.; Rossi, S.H.; Klatte, T.; Stewart, G.D. Genomics and clinical correlates of renal cell carcinoma. W. J. Urol. 2018, 36, 1899–1911. [Google Scholar] [CrossRef] [Green Version]
- Carlo, M.I.; Manley, B.; Patil, S.; Woo, K.M.; Coskey, D.T.; Redzematovic, A.; Arcila, M.; Ladanyi, M.; Lee, W.; Chen, Y.B.; et al. Genomic alterations and outcomes with VEGF-targeted therapy in patients with clear cell renal cell carcinoma. Kidney Cancer 2017, 1, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voss, M.H.; Reising, A.; Cheng, Y.; Patel, P.; Marker, M.; Kuo, F.; Chan, T.A.; Choueiri, T.K.; Hsieh, J.J.; Hakimi, A.A.; et al. Genomically annotated risk model for advanced renal-cell carcinoma: A retrospective cohort study. Lancet Oncol. 2018, 19, 1688–1698. [Google Scholar] [CrossRef] [PubMed]
- Turajlic, S.; Xu, H.; Litchfield, K.; Rowan, A.; Chambers, T.; Lopez, J.I.; Nicol, D.; O’Brien, T.; Larkin, J.; Horswell, S.; et al. Tracking cancer evolution reveals constrained routes to metastases: TRACERx Renal. Cell 2018, 173, 581–594. [Google Scholar] [CrossRef] [Green Version]
- Meacci, E.; Nachira, D.; Zanfrini, E.; Evangelista, J.; Triumbari, E.K.A.; Congedo, M.T.; Petracca Ciavarella, L.; Chiappetta, M.; Vita, M.L.; Schinzari, G.; et al. Prognostic factors affecting survival after pulmonary resection of metastatic renal cell carcinoma: A multicenter experience. Cancers 2021, 13, 3258. [Google Scholar] [CrossRef]
- Saricam, M. Factors Affecting Long-Term Survival Following Pulmonary Metastasectomy of Renal Cell Carcinoma. Urol. Oncol. 2020, 17, 492–496. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, J.; Li, C.; Fan, J.; Liu, L. Prognostic factors for overall survival after lung metastasectomy in renal cell cancer patients: A systematic review and meta-analysis. World J. Surg. 2017, 41, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Macherey, S.; Kauffmann, C.; Heidenreich, A.; Doerr, F.; Wahlers, T.; Hekmat, K. Pulmonary metastasectomy in renal cell carcinoma. Urologe A. 2017, 56, 1025–1030. [Google Scholar] [CrossRef]
- Piltz, S.; Meimarakis, G.; Wichmann, M.W.; Hatz, R.; Schildberg, F.W.; Fuerst, H. Long-term results after pulmonary resection of renal cell carcinoma metastases. Ann. Thorac. Surg. 2002, 73, 1082–1087. [Google Scholar] [CrossRef]
- Hau, H.M.; Thalmann, F.; Lübbert, C.; Morgul, M.H.; Schmelzle, M.; Atanasov, G.; Benzing, C.; Lange, U.; Ascherl, R.; Ganzer, R.; et al. The value of hepatic resection in metastasicrenal cancer in the era of tyrosinkinase inhibitor therapy. BMC Surg. 2016, 16, 49. [Google Scholar] [CrossRef] [Green Version]
- Aloia, T.A.; Adam, R.; Azoulay, D.; Bismuth, H.; Castaing, D. Outcome following hepatic resection of metastatic renal tumors: The Paul Brousse Hospital experience. HPB 2006, 8, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Hamada, S.; Ito, K.; Kuroda, K.; Sato, A.; Asakuma, J.; Horiguchi, A.; Seguchi, K.; Asano, T. Clinical characteristics and prognosis of patients with renal cell carcinoma and liver metastasis. Mol. Clin. Oncol. 2015, 3, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruys, A.T.; Tanis, P.J.; Nagtegaal, I.D.; van Duijvendijk, P.; Verhoef, C.; Porte, R.J.; van Gulik, T.M. Surgical treatment of renal cell cancer liver metastases: A population-based study. Ann. Surg. Oncol. 2011, 18, 1932–1938. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.C.; Yip, A.S.M. Prognostic factors of survival and a new scoring system for liver resection of colorectal liver metastasis. World J. Hepatol. 2022, 14, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Villard, C.; Abdelrafee, A.; Habib, M.; Ndegwa, N.; Jorns, C.; Sparrelid, E.; Allard, M.A.; Adam, R. Prediction of survival in patients with colorectal liver metastases- development and validation of a prognostic score model. Eur. J. Surg. Oncol. 2022, 48, 2432–2439. [Google Scholar] [CrossRef]
- Acciuffi, S.; Meyer, F.; Bauschke, A.; Croner, R.; Settmacher, U.; Altendorf-Hofmann, A. Solitary colorectal liver metastasis: Overview of treatment strategies and role of prognostic factors. J. Cancer Res. Clin. Oncol. 2022, 148, 657–665. [Google Scholar] [CrossRef]
- Fromer, M.W.; Scoggins, C.R.; Egger, M.E.; Philips, P.; McMasters, K.M.; Martin, R.C.G. Preventing futile liver resection: A risk-based approach to surgical selection in major hepatectomy for colorectal cancer. Ann. Surg. Oncol. 2022, 29, 905–912. [Google Scholar] [CrossRef]
- Viganò, L.; Gentile, D.; Galvanin, J.; Corleone, P.; Costa, G.; Cimino, M.; Procopio, F.; Torzilli, G. Very early recurrence after liver resection for colorectal metastases: Incidence, risk factors, and prognostic impact. J. Gastrointest. Surg. 2022, 26, 570–582. [Google Scholar] [CrossRef]
- Ren, W.; Sell, N.M.; Ferrone, C.R.; Tanabe, K.K.; Lillemoe, K.D.; Qadan, M. Size of the largest colorectal liver metastasis Is an independent prognostic factor in the neoadjuvant setting. J. Surg. Res. 2021, 259, 253–260. [Google Scholar] [CrossRef]
- Moro, A.; Mehta, R.; Tsilimigras, D.I.; Sahara, K.; Paredes, A.Z.; Bagante, F.; Guglielmi, A.; Alexandrescu, S.; Poultsides, G.A.; Sasaki, K.; et al. Prognostic factors differ according to KRAS mutational status: A classification and regression tree model to define prognostic groups after hepatectomy for colorectal liver metastasis. Surgery 2020, 168, 497–503. [Google Scholar] [CrossRef]
- Carvajal, C.; Facundo, H.; Puerto, P.; Carreño, J.; Beltrán, R. Lung metastasectomy from colorectal cancer, 10-year experience in a South American cancer center. Front. Surg. 2022, 9, 913678. [Google Scholar] [CrossRef]
- Gössling, G.C.L.; Chedid, M.F.; Pereira, F.S.; da Silva, R.K.; Andrade, L.B.; Peruzzo, N.; Saueressig, M.G.; Schwartsmann, G.; Parikh, A.R. Outcomes and prognostic factors of patients with metastatic colorectal cancer who underwent pulmonary metastasectomy with curative intent: A brazilian experience. Oncologist 2021, 26, e1581–e1588. [Google Scholar] [CrossRef] [PubMed]
- Okumura, T.; Boku, N.; Hishida, T.; Ohde, Y.; Sakao, Y.; Yoshiya, K.; Higashiyama, M.; Hyodo, I.; Mori, K.; Kondo, H. Surgical outcome and prognostic stratification for pulmonary metastasis from colorectal cancer. Ann. Thorac. Surg. 2017, 104, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Ohtaki, Y.; Okumura, T.; Boku, N.; Horio, H.; Takenoyama, M.; Yamashita, M.; Hyodo, I.; Mori, K.; Kondo, H. Outcomes and prognostic factors after pulmonary metastasectomy in patients with colorectal cancer with previously resected hepatic metastases. J. Thorac. Cardiovasc. Surg. 2019, 157, 2049–2057. [Google Scholar] [CrossRef]
- Brozzetti, S.; Carati, M.; Sterpetti, A. Systematic review and metanalysis of clinical outcomes after enucleation of pancreatic metastases from renal cell carcinoma. Dig. Surg. 2022, in press.
- Saitoh, H.; Kobayashi, N.; Yochida, K.; Suwata, L.; Uchijima, Y.; Nakame, Y. Possible metastatic routes via portocaval shunts in renal adenocarcinoma with liver metastasis. Urology 1997, 37, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Lore, J.; Madden, J.; Gerold, F. Pre-exisiting portocaval shunts: A hypothesis for bizarre metastases of some carcinomas. Cancer 1958, 11, 24–27. [Google Scholar] [CrossRef]
- Sellner, F. Isolated pancreatic metastases from renal cell carcinoma: An outcome of a special metastatic pathway or of a specific tumor cell selection? Clin. Exp. Metastasis 2018, 35, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Jaen-Torrejimeno, I.; Rojas-Holguin, A.; Lopez-Querra, D.; Ramia, J.M.; Blanco-Fernandez, Q. Pancreatic resection for metastatic renal cell carcinoma. A systematic review. HPB 2020, 22, 479–486. [Google Scholar] [CrossRef]
- Sellner, F. Isolated pancreatic metastases of renal cell carcinoma—A paradigm of a seed and soil mechanism: A literature analysis of 1034 observations. Front. Oncol. 2020, 10, 709. [Google Scholar] [CrossRef]
- Sellner, F.; Thalhammer, S.; Klimpfinger, M. Isolated pancreatic metastases of renal cell cancer: Genetics and epigenetics of an unusual tumour entity. Cancers 2022, 14, 1539. [Google Scholar] [CrossRef]
- Paget, S. The distribution of secondary growths in cancer of the breast. Lancet 1889, 133, 571–573. [Google Scholar] [CrossRef] [Green Version]
- Akhtar, M.; Haider, A.; Rashid, S.M.; Al-Naber, A.D. Paget’s "Seed and Soil" theory of cancer metastasis: An idea whose time has come. Adv. Anat. Pathol. 2019, 26, 69–74. [Google Scholar] [CrossRef]
- Chambers, A.; Varghese, H.; Nadkarni, K.; MacDonald, I.; Groom, A. Critical steps in hematogenous metastasis: An overview. Surg. Oncol. Clin. N. Am. 2001, 10, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Hunter, K. Host genetics and tumour metastasis. Br. J. Cancer 2004, 90, 752–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, S.P.; Cabrera, R.M.; Segall, J.E. Tumor cell intravasation. Am. J. Physiol. Cell Physiol. 2016, 311, C1–C14. [Google Scholar] [CrossRef] [Green Version]
- Obenauf, A.C.; Massague, J. Surviving at a distance: Organ-specific metastasis. Trends Cancer 2015, 1, 76–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Summers, M.A.; McDonald, M.M.; Croucher, P.I. Cancer cell dormancy in metastasis. Cold Spring Harb. Perspect. Med. 2020, 10, a037556. [Google Scholar] [CrossRef] [Green Version]
- Endo, H.; Inoue, M. Dormancy in cancer. Cancer Sci. 2019, 110, 474–480. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Zhang, H.; Jiang, X.; Qian, C.; Liu, Z.; Luo, D. Factors involved in cancer metastases: A better understanding to “seed and soil” hypothesis. Mol. Cancer 2017, 16, 176. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Bado, I.; Wang, H.; Zhang, W.; Rosen, J.M.; Zhang, X.H. Metastasis organotropism: Redefining the congenial soil. Dev. Cell 2019, 49, 375–391. [Google Scholar] [CrossRef]
- Nan, X.; Wang, J.; Liu, H.N.; Wong, S.T.; Zhao, H. Epithelial-mesenchymal plasticity in organotropism metastasis and tumor immune escape. J. Clin. Med. 2019, 8, 747. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Ding, Y.; Guo, N.; Wang, S. MDSCs: Key criminals of tumor pre-metastatic niche formation. Front. Immunol. 2019, 10, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Pan, J.; Barsky, L.; Jacob, J.C.; Zheng, Y.; Gao, C.; Wang, S.; Zhu, W.; Sun, H.; Lu, L.; et al. Characteristics of pre-metastatic niche: The landscape of molecular and cellular pathways. Mol. Biomed. 2021, 2, 3. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.N.; Riba, R.D.; Zacharoulis, S.; Bramley, A.H.; Vincent, L.; Costa, C.; MacDonald, D.D.; Jin, D.K.; Shido, K.; Kerns, S.A.; et al. VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 2005, 438, 820–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sceneay, J.; Smyth, M.; Möller, A. The pre-metastatic niche: Finding common ground. Cancer Metastasis Rev. 2013, 32, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Cao, X. Characteristics and significance of the pre-metastatic niche. Cancer Cell. 2016, 30, 668–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talmadge, J.E.; Fidler, I.J. AACR centennial series: The biology of cancer metastasis: Historical perspective. Cancer Res. 2010, 70, 5649–5669. [Google Scholar] [CrossRef] [Green Version]
- Grange, C.; Brossa, A.; Bussolatti, B. Extracellular vesicles and carried miRNAs in the progression of renal cell carcinoma. Int. J. Mol. Sci. 2019, 20, 1832. [Google Scholar] [CrossRef] [Green Version]
- Gai, C.; Pomatto, M.A.; Grange, C.; Deregibus, M.C.; Camussi, G. Extracellular vesicles in onco-nephrology. Exp. Mol. Med. 2019, 51, 29. [Google Scholar] [CrossRef] [Green Version]
- Wortzel, I.; Dror, S.; Kenific, C.M.; Lyden, D. Exosome-mediated metastasis: Communication from a distance. Dev. Cell. 2019, 49, 347–360. [Google Scholar] [CrossRef]
- Deguchi, A.; Maru, Y. Inflammation-associated premetastatic niche formation. Inflamm. Regen. 2022, 42, 22. [Google Scholar] [CrossRef] [PubMed]
- Grange, C.; Tapparo, M.; Collino, F.; Vitillo, L.; Damasco, C.; Deregibus, M.C.; Tetta, C.; Bussolati, B.; Camussi, G. Microvesicles released from human renal cancer stem cells stimulate angiogensis and formation of lung premetastatic niche. Cancer Res. 2011, 71, 5346–5356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walenkamp, A.M.; Lapa, C.; Herrmann, K.; Wester, H.J. CXCR4 ligands: The next big hit? J. Nucl. Med. 2017, 58, 77S–82S. [Google Scholar] [CrossRef]
- DiNatale, A.; Castelli, M.S.; Nash, B.; Meucci, O.; Fatatis, A. Regulation of tumor and metastasis initiation by chemokine receptors. J. Cancer 2022, 13, 3160–3176. [Google Scholar] [CrossRef] [PubMed]
- Schild, T.; Low, V.; Blenis, J.; Gomes, A.P. Unique metabolic adaptations dictate distal organ-specific metastatic colonization. Cancer Cell. 2018, 33, 347–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebert, D.; Haller, R.G.; Walton, M.E. Energy contribution of octanoate to intact rat brain metabolism measured by 13C nuclear magnetic resonance spectroscopy. J. Neurosci. 2003, 23, 5928–5935. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, R.P.; Nissim, I.; Brosnan, J.T. Creatine synthesis: Hepatic metabolism of guanidinacetate and creatine in the rat in vitro and in vivo. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E256–E261. [Google Scholar] [CrossRef]
- Mashimo, T.; Pichumani, K.; Vemireddy, V.; Hatanpaa, K.J.; Singh, D.K.; Sirasanagandla, S.; Nannepaga, S.; Piccirillo, S.G.; Kovacs, Z.; Foong, C.; et al. Acetate is a bioenergetic substrate for human glioblastoma and brain metastases. Cell 2014, 159, 1603–1614. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Lee, H.J.; Wu, X.; Huo, L.; Kim, S.J.; Xu, L.; Wang, Y.; He, J.; Bollu, L.R.; Gao, G.; et al. Gain of glucose-independent growth upon metastasis of breast cancer cells to the brain. Cancer Res. 2015, 75, 554–565. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Luo, D. The metabolic adaptation mechanism of metastatic organotropism. Exp. Hematol. Oncol. 2021, 10, 30. [Google Scholar] [CrossRef]
- Bloom, H.J. Hormone induced and spontaneous regression of metastatic renal cancer. Cancer 1973, 32, 1666. [Google Scholar] [CrossRef]
- Snow, R.M.; Schellhammer, P.F. Spontaneous regression of metastatic renal cell carcinoma. Urology 1982, 20, 177. [Google Scholar] [CrossRef] [PubMed]
- Elhilali, M.M.; Gleave, M.; Fradet, Y.; Venner, D.; Saad, F.; Klotz, L.; Moore, R.; Paton, E. Placebo-associated remissions in a multicentre, randomized, double-blind trial of interferon γ-1b for the treatment of metastatic renal cell carcinoma. BJU. Int. 2000, 86, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Battle, D.; Figlin, R.A.; George, D.J.; Hammers, H.; Hutson, T.; Jonasch, E.; Joseph, R.W.; McDermott, D.F.; Motzer, R.J.; et al. The society for immunotherapy of cancer consensus statement on immunotherapy for the treatment of advanced renal cell carcinoma (RCC). J. Immunother. Cancer 2019, 7, 354. [Google Scholar] [CrossRef] [Green Version]
- Flippot, R.; Escudier, B.; Albiges, L. Immune checkpoint inhibitors: Toward new paradigms in renal cell carcinoma. Drugs 2018, 78, 1443–1457. [Google Scholar] [CrossRef]
- Chang, A.J.; Zhao, L.; Zhu, Z.; Boulanger, K.; Xiao, H.; Wakefield, M.R.; Bai, Q.; Fang, Y. The past, present and future of immunotherapy for metastatic renal cell carcinoma. Anticancer Res. 2019, 39, 2683–2687. [Google Scholar] [CrossRef]
- Wang, T.; Lu, R.; Kapur, P.; Jaiswal, B.S.; Hannan, R.; Zhang, Z.; Pedrosa, I.; Luke, J.J.; Zhang, H.; Goldstein, L.D.; et al. An empirical approach leveraging tumorgrafts to dissect the tumor microenvironment in renal cell carcinoma identifies missing link to prognostic inflammatory factors. Cancer Discov. 2018, 8, 1142–1155. [Google Scholar] [CrossRef] [Green Version]
- Laruelle, A.; Manini, C.; Iñarra, E.; López, J.I. Metastasis, an example of evolvability. Cancers 2021, 13, 3653. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sellner, F.; Thalhammer, S.; Klimpfinger, M. Isolated Pancreatic Metastases of Renal Cell Carcinoma—Clinical Particularities and Seed and Soil Hypothesis. Cancers 2023, 15, 339. https://doi.org/10.3390/cancers15020339
Sellner F, Thalhammer S, Klimpfinger M. Isolated Pancreatic Metastases of Renal Cell Carcinoma—Clinical Particularities and Seed and Soil Hypothesis. Cancers. 2023; 15(2):339. https://doi.org/10.3390/cancers15020339
Chicago/Turabian StyleSellner, Franz, Sabine Thalhammer, and Martin Klimpfinger. 2023. "Isolated Pancreatic Metastases of Renal Cell Carcinoma—Clinical Particularities and Seed and Soil Hypothesis" Cancers 15, no. 2: 339. https://doi.org/10.3390/cancers15020339