
Vulvar Cancer: 2021 Revised FIGO Staging System and the Role of Imaging

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Background
3. Genomics of Vulvar Cancer
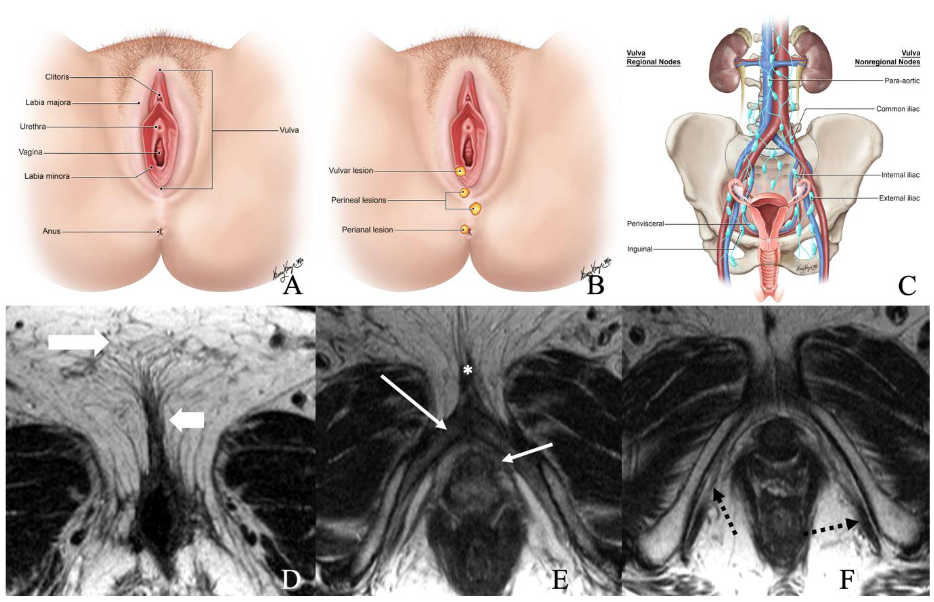
4. Role of Imaging in Vulvar Cancer
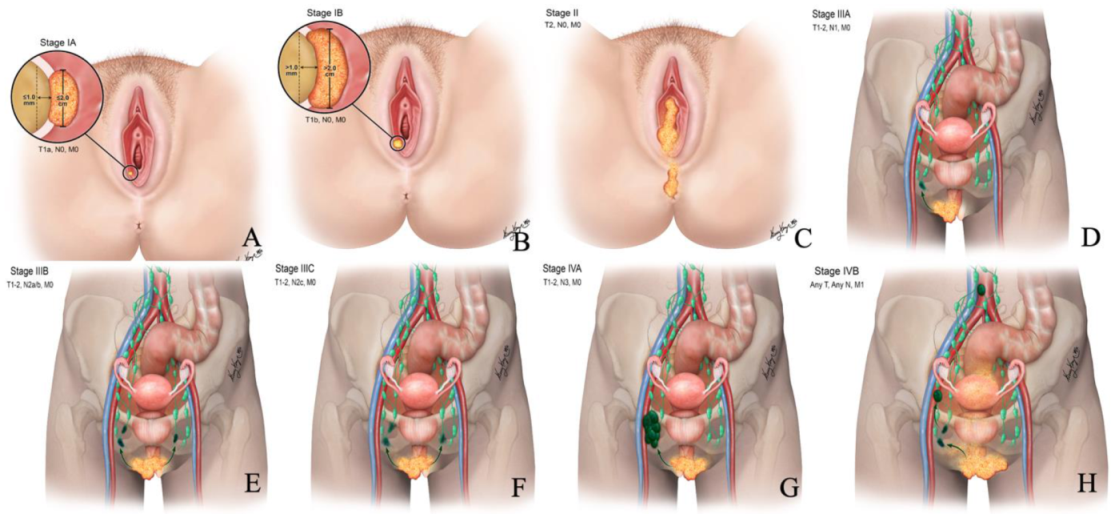
5. International Federation of Gynecology and Obstetrics Staging of Vulvar Cancer
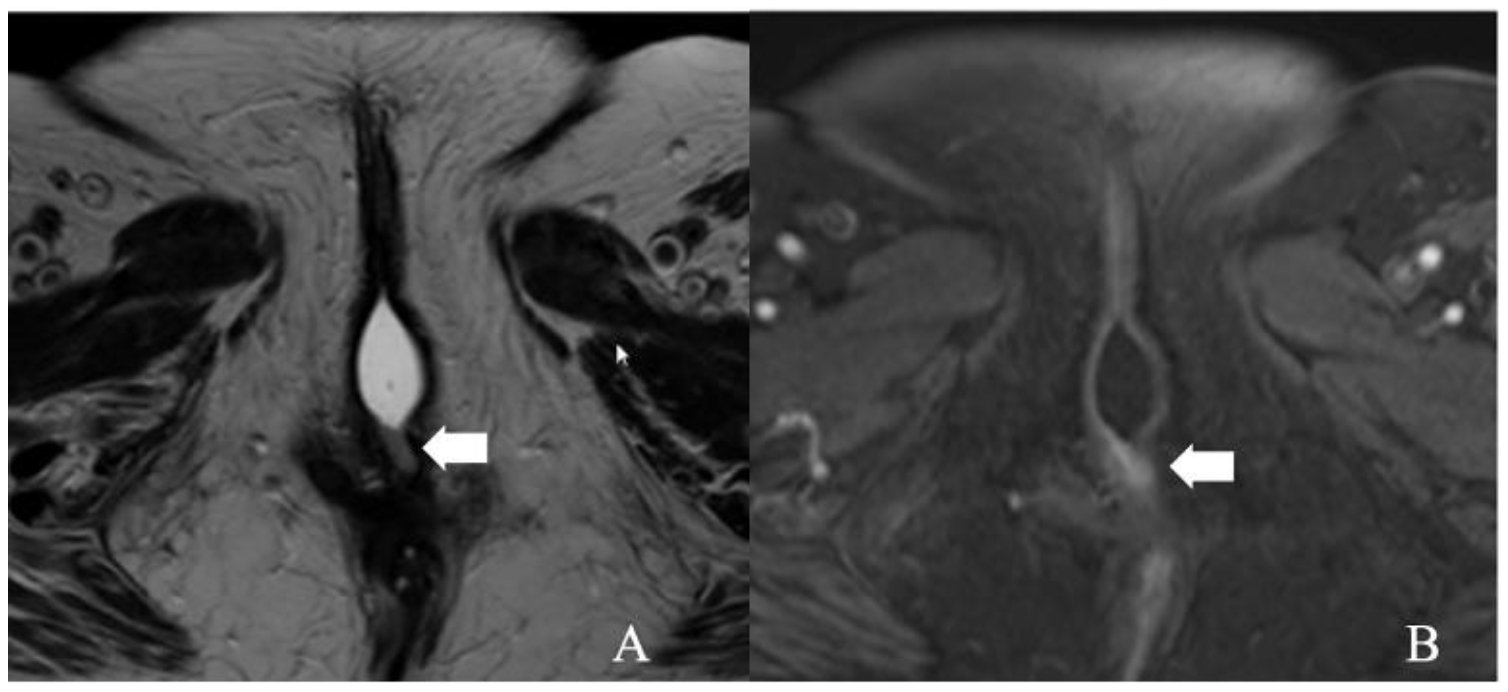
5.1. Stage I
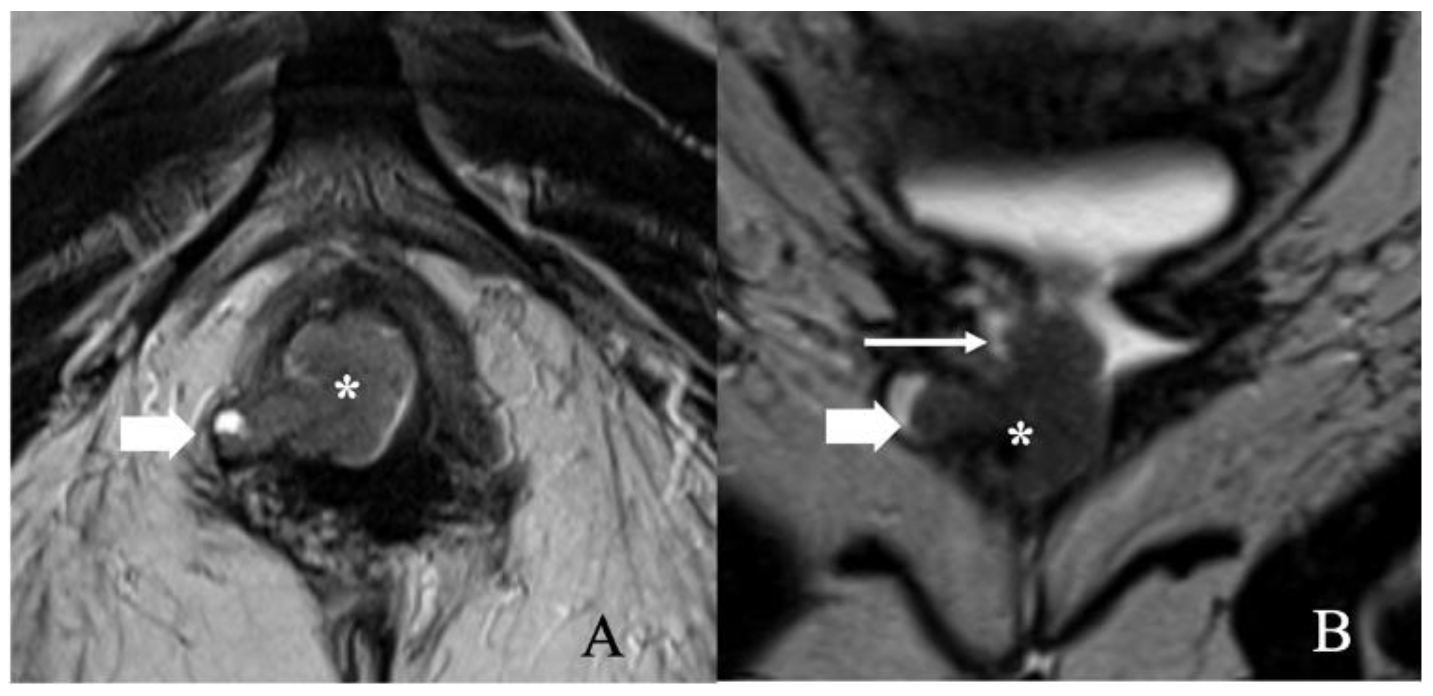
5.2. Stage II
5.3. Stage III
5.4. Stage IV
6. Treatment
7. Surveillance of Vulvar Cancer
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shetty, A.S.; Menias, C.O. MR Imaging of Vulvar and Vaginal Cancer. Magn. Reson. Imaging Clin. N. Am. 2017, 25, 481–502. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.; Tsui, B.Q.; Bahrami, S.; Masamed, R.; Memarzadeh, S.; Raman, S.S.; Patel, M.K. Gynecologic tumor board: A radiologist’s guide to vulvar and vaginal malignancies. Abdom. Radiol. 2021, 46, 5669–5686. [Google Scholar] [CrossRef] [PubMed]
- Merlo, A.S. Modern treatment of vulvar cancer. Radiol. Oncol. 2020, 54, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, D.; Gomez-Martinez, R.A. Vulvar cancer. Obstet. Gynecol. Clin. 2019, 46, 125–135. [Google Scholar] [CrossRef]
- Mitra, S.; Sharma, M.K.; Kaur, I.; Khurana, R.; Modi, K.B.; Narang, R.; Mandal, A.; Dutta, S. Vulvar carcinoma: Dilemma, debates, and decisions. Cancer Manag. Res. 2018, 10, 61. [Google Scholar] [CrossRef] [Green Version]
- A Cohen, P.; Anderson, L.; Eva, L.; Scurry, J. Clinical and molecular classification of vulvar squamous pre-cancers. Int. J. Gynecol. Cancer 2019, 29, 821–828. [Google Scholar] [CrossRef]
- Serrado, M.A.; Horta, M.; Cunha, T.M. State of the art in vulvar cancer imaging. Radiol. Bras. 2019, 52, 316–324. [Google Scholar] [CrossRef] [Green Version]
- Cobos, G.A.; Pomeranz, M.K. A General Approach to the Evaluation and the Management of Vulvar Disorders. Obstet. Gynecol. Clin. North Am. 2017, 44, 321–327. [Google Scholar] [CrossRef]
- Olawaiye, A.B.; Cuello, M.A.; Rogers, L.J. Cancer of the vulva: 2021 update. Int. J. Gynecol. Obstet. 2021, 155, 7–18. [Google Scholar] [CrossRef]
- Hoang, L.N.; Park, K.J.; Soslow, R.A.; Murali, R. Squamous precursor lesions of the vulva: Current classification and diagnostic challenges. Pathology 2016, 48, 291–302. [Google Scholar] [CrossRef] [Green Version]
- Bigby, S.M.; Eva, L.J.; Fong, K.L.; Jones, R.W. The natural history of vulvar intraepithelial neoplasia, differentiated type: Evidence for progression and diagnostic challenges. Int. J. Gynecol. Pathol. 2016, 35, 574–584. [Google Scholar] [CrossRef]
- Van de Nieuwenhof, H.P.; Massuger, L.F.; van der Avoort, I.A.; Bekkers, R.L.; Casparie, M.; Abma, W.; van Kempen, L.C.; de Hullu, J.A. Vulvar squamous cell carcinoma development after diagnosis of VIN increases with age. Eur. J. Cancer 2009, 45, 851–856. [Google Scholar] [CrossRef]
- Olawaiye, A.B.; Cotler, J.; Cuello, M.A.; Bhatla, N.; Okamoto, A.; Wilailak, S.; Purandare, C.N.; Lindeque, G.; Berek, J.S.; Kehoe, S.; et al. FIGO staging for carcinoma of the vulva: 2021 revision. Int. J. Gynecol. Obstet. 2021, 155, 43–47. [Google Scholar] [CrossRef]
- Rakislova, N.; Clavero, O.; Alemany, L.; Saco, A.; Quirós, B.; Lloveras, B.; Alejo, M.; Pawlita, M.; Quint, W.; Del Pino, M. Histological characteristics of HPV-associated and-independent squamous cell carcinomas of the vulva: A study of 1594 cases. Int. J. Cancer 2017, 141, 2517–2527. [Google Scholar] [CrossRef] [Green Version]
- Mooren, J.J.; Gültekin, S.E.; Straetmans, J.M.; Haesevoets, A.; Peutz-Kootstra, C.J.; Huebbers, C.U.; Dienes, H.P.; Wieland, U.; Ramaekers, F.C.; Kremer, B. P16INK4A immunostaining is a strong indicator for high-risk-HPV-associated oropharyngeal carcinomas and dysplasias, but is unreliable to predict low-risk-HPV-infection in head and neck papillomas and laryngeal dysplasias. Int. J. Cancer 2014, 134, 2108–2117. [Google Scholar] [CrossRef]
- Cheng, A.S.; Karnezis, A.N.; Jordan, S.; Singh, N.; McAlpine, J.N.; Gilks, C.B. p16 Immunostaining Allows for Accurate Subclassification of Vulvar Squamous Cell Carcinoma Into HPV-Associated and HPV-Independent Cases. Int. J. Gynecol. Pathol. 2016, 35, 385–393. [Google Scholar] [CrossRef]
- Lee, L.J.; Howitt, B.; Catalano, P.; Tanaka, C.; Murphy, R.; Cimbak, N.; DeMaria, R.; Bu, P.; Crum, C.; Horowitz, N.; et al. Prognostic importance of human papillomavirus (HPV) and p16 positivity in squamous cell carcinoma of the vulva treated with radiotherapy. Gynecol. Oncol. 2016, 142, 293–298. [Google Scholar] [CrossRef]
- Dasgupta, S.; Ewing-Graham, P.C.; Swagemakers, S.M.; van der Spek, P.J.; van Doorn, H.C.; Hegt, V.N.; Koljenović, S.; van Kemenade, F.J. Precursor lesions of vulvar squamous cell carcinoma—Histology and biomarkers: A systematic review. Crit. Rev. Oncol. 2020, 147, 102866. [Google Scholar] [CrossRef]
- Xing, D.; Fadare, O. Molecular events in the pathogenesis of vulvar squamous cell carcinoma. Semin. Diagn. Pathol. 2021, 38, 50–61. [Google Scholar] [CrossRef]
- He, C.; Li, L.; Guan, X.; Xiong, L.; Miao, X. Mutant p53 Gain of Function and Chemoresistance: The Role of Mutant p53 in Response to Clinical Chemotherapy. Chemotherapy 2017, 62, 43–53. [Google Scholar] [CrossRef]
- Griffin, N.; Grant, L.A.; Sala, E. Magnetic resonance imaging of vaginal and vulval pathology. Eur. Radiol. 2008, 18, 1269–1280. [Google Scholar] [CrossRef]
- Kataoka, M.Y.; Sala, E.; Baldwin, P.; Reinhold, C.; Farhadi, A.; Hudolin, T.; Hricak, H. The accuracy of magnetic resonance imaging in staging of vulvar cancer: A retrospective multi-centre study. Gynecol. Oncol. 2010, 117, 82–87. [Google Scholar] [CrossRef]
- Viswanathan, C.; Kirschner, K.; Truong, M.; Balachandran, A.; Devine, C.; Bhosale, P. Multimodality Imaging of Vulvar Cancer: Staging, Therapeutic Response, and Complications. Am. J. Roentgenol. 2013, 200, 1387–1400. [Google Scholar] [CrossRef]
- Nikolić, O.; e Sousa, F.A.; Cunha, T.M.; Nikolić, M.B.; Otero-García, M.M.; Gui, B.; Nougaret, S.; Leonhardt, H.; Fournier, L.; Bourgioti, C.; et al. Vulvar cancer staging: Guidelines of the European Society of Urogenital Radiology (ESUR). Insights into Imaging 2021, 12, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Hacker, N.F.; Barlow, E.L. Staging for vulvar cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 802–811. [Google Scholar] [CrossRef]
- Gui, B.; Persiani, S.; Miccò, M.; Pignatelli, V.; Rodolfino, E.; Avesani, G.; Di Paola, V.; Panico, C.; Russo, L.; Fragomeni, S.M.; et al. MRI Staging in Locally Advanced Vulvar Cancer: From Anatomy to Clinico-Radiological Findings. A Multidisciplinary VulCan Team Point of View. J. Pers. Med. 2021, 11, 1219. [Google Scholar] [CrossRef] [PubMed]
- Klapdor, R.; Länger, F.; Gratz, K.; Hillemanns, P.; Hertel, H. SPECT/CT for SLN dissection in vulvar cancer: Improved SLN detection and dissection by preoperative three-dimensional anatomical localisation. Gynecol. Oncol. 2015, 138, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Salani, R.; Khanna, N.; Frimer, M.; Bristow, R.E.; Chen, L.-M. An update on post-treatment surveillance and diagnosis of recurrence in women with gynecologic malignancies: Society of Gynecologic Oncology (SGO) recommendations. Gynecol. Oncol. 2017, 146, 3–10. [Google Scholar] [CrossRef]
- Hall, T.; Barton, D.; Trott, P.; Nasiri, N.; Shepherd, J.; Thomas, J.; Moskovic, E. The Role of Ultrasound-guided Cytology of Groin Lymph Nodes in the Management of Squamous Cell Carcinoma of the Vulva: 5-Year Experience in 44 Patients. Clin. Radiol. 2003, 58, 367–371. [Google Scholar] [CrossRef]
- Kim, K.W.; Shinagare, A.B.; Krajewski, K.M.; Howard, S.A.; Jagannathan, J.P.; Zukotynski, K.; Ramaiya, N.H. Update on Imaging of Vulvar Squamous Cell Carcinoma. Am. J. Roentgenol. 2013, 201, W147–W157. [Google Scholar] [CrossRef]
- Will, O.; Purkayastha, S.; Chan, C.; Athanasiou, T.; Darzi, A.W.; Gedroyc, W.; Tekkis, P.P. Diagnostic precision of nanoparticle-enhanced MRI for lymph-node metastases: A meta-analysis. Lancet Oncol. 2006, 7, 52–60. [Google Scholar] [CrossRef]
- McMahon, C.J.; Rofsky, N.M.; Pedrosa, I. Lymphatic Metastases from Pelvic Tumors: Anatomic Classification, Characterization, and Staging. Radiology 2010, 254, 31–46. [Google Scholar] [CrossRef]
- Crivellaro, C.; Guglielmo, P.; De Ponti, E.; Elisei, F.; Guerra, L.; Magni, S.; La Manna, M.; Di Martino, G.; Landoni, C.; Buda, A. 18F-FDG PET/CT in preoperative staging of vulvar cancer patients: Is it really effective? Medicine 2017, 96, e7943. [Google Scholar] [CrossRef]
- Rufini, V.; Garganese, G.; Ieria, F.P.; Pasciuto, T.; Fragomeni, S.M.; Gui, B.; Florit, A.; Inzani, F.; Zannoni, G.F.; Scambia, G.; et al. Diagnostic performance of preoperative [18F]FDG-PET/CT for lymph node staging in vulvar cancer: A large single-centre study. Eur. J. Pediatr. 2021, 48, 3303–3314. [Google Scholar] [CrossRef]
- Triumbari, E.K.; de Koster, E.J.; Rufini, V.; Fragomeni, S.M.; Garganese, G.; Collarino, A. 18F-FDG PET and 18F-FDG PET/CT in vulvar cancer: A systematic review and meta-analysis. Clin. Nucl. Med. 2021, 46, 125–132. [Google Scholar] [CrossRef]
- Albano, D.; Bonacina, M.; Savelli, G.; Ferro, P.; Busnardo, E.; Gianolli, L.; Camoni, L.; Giubbini, R.; Bertagna, F. Clinical and prognostic 18F-FDG PET/CT role in recurrent vulvar cancer: A multicentric experience. Jpn. J. Radiol. 2021, 40, 66–74. [Google Scholar] [CrossRef]
- Koh, W.-J.; Greer, B.E.; Abu-Rustum, N.R.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A.; Dizon, D.S. Vulvar cancer, version 1.2017, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 92–120. [Google Scholar] [CrossRef] [Green Version]
- Faul, C.M.; Mirmow, D.; Huang, Q.; Gerszten, K.; Day, R.; Jones, M.W. Adjuvant radiation for vulvar carcinoma: Improved local control. Int. J. Radiat. Oncol. Biol. Phys. 1997, 38, 381–389. [Google Scholar] [CrossRef]
- Hacker, N.F.; Berek, J.S.; Juillard, G.J.F.; Lagasse, L.D. Preoperative radiation therapy for locally advanced vulvar cancer. Cancer 1984, 54, 2056–2061. [Google Scholar] [CrossRef]
- Hassanzade, M.; Attaran, M.; Treglia, G.; Yousefi, Z.; Sadeghi, R. Lymphatic mapping and sentinel node biopsy in squamous cell carcinoma of the vulva: Systematic review and meta-analysis of the literature. Gynecol. Oncol. 2013, 130, 237–245. [Google Scholar] [CrossRef]
- Coleman, R.L.; Ali, S.; Levenback, C.F.; Gold, M.A.; Fowler, J.M.; Judson, P.L.; Bell, M.C.; De Geest, K.; Spirtos, N.M.; Potkul, R.K.; et al. Is bilateral lymphadenectomy for midline squamous carcinoma of the vulva always necessary? An analysis from Gynecologic Oncology Group (GOG) Gynecol. Oncol. 2013, 128, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Oonk, M.H.; van Hemel, B.M.; Hollema, H.; A de Hullu, J.; Ansink, A.C.; Vergote, I.; Verheijen, R.H.; Maggioni, A.; Gaarenstroom, K.N.; Baldwin, P.J.; et al. Size of sentinel-node metastasis and chances of non-sentinel-node involvement and survival in early stage vulvar cancer: Results from GROINSS-V, a multicentre observastional study. Lancet Oncol. 2010, 11, 646–652. [Google Scholar] [CrossRef]
- Radziszewski, J.; Kowalewska, M.; Jedrzejczak, T.; Kozlowicz-Gudzinska, I.; Nasierowska-Guttmejer, A.; Bidzinski, M.; Siedlecki, J.A. The accuracy of the sentinel lymph node concept in early stage squamous cell vulvar carcinoma. Gynecol. Oncol. 2010, 116, 473–477. [Google Scholar] [CrossRef]
- Selman, T.; Luesley, D.; Acheson, N.; Khan, K.; Mann, C. A systematic review of the accuracy of diagnostic tests for inguinal lymph node status in vulvar cancer. Gynecol. Oncol. 2005, 99, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I.; Schubert, M.; Garbrecht, N.; Weigel, M.T.; Jonat, W.; Mundhenke, C.; Günther, V. Vulvar cancer: Epidemiology, clinical presentation, and management options. Int. J. Women’s Health 2015, 7, 305. [Google Scholar] [CrossRef] [Green Version]
- Fukutome, M.; Maebayashi, K.; Nasu, S.; Seki, K.; Mitsuhashi, N. Enhancement of radiosensitivity by dual inhibition of the HER family with ZD1839 (“Iressa”) and trastuzumab (“Herceptin”). Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Van Der Zee, A.G.J.; Oonk, M.H.; De Hullu, J.A.; Ansink, A.C.; Vergote, I.; Verheijen, R.H.; Maggioni, A.; Gaarenstroom, K.; Baldwin, P.J.; Van Dorst, E.B.; et al. Sentinel node dissection is safe in the treatment of early-stage vulvar cancer. J. Clin. Oncol. 2008, 26, 884–889. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Series Number | Series Description | FOV | Slice Thickness | Spacing | Frequency Encoding | Freq × Phase |
|---|---|---|---|---|---|---|
| 1 | Coronal T2 (to include the kidneys) | 420 | 5 | 0 | S/I | 288 × 192 |
| 2 | Sagittal T2 | 240 | 5 | 0 | A/P | 320 × 224 |
| 3 | rFOV Sagittal b = 50,600 | 240 | 5 | 0 | S/I | 96 × 80 |
| 4 | Axial T2 | 240 | 5 | 0 | L/R | 320 × 224 |
| 5 | AxialT1 | 240 | 5 | 0 | L/R | 320 × 224 |
| 6 | Axial DWI b = 50,400,800 | 380+ | 5 | 0 | L/R | 96 × 160 |
| 7 | Axial 3D Pre | 240 | 5 | −2.5 | L/R | 320 × 224 |
| 8 | Axial Dynamic 115 | 240 | 5 | −2.5 | S/I | 256 × 224 |
| 9 | +C Sagittal 3D Immediate delay | 240 | 5 | −2.5 | L/R | 256 × 224 |
| MRI Report Findings |
|---|
| Tumor dimension: maximum diameter |
| Tumor location: lateral/midline/multifocal |
| Clitoris involvement |
| Extension to adjacent organs/structures: urethra and/or vagina with caudo-cranial extension specification; lower one-third or upper two-third; urethral meatus; bladder; fourchette area, anus/rectum |
| Lymph node involvement: inguinofemoral and/or pelvic and/or abdominal |
| Additional findings: uterus; adnexa; kidneys; and pelvic bones |
| Stage | Characteristics |
|---|---|
| I | Tumor confined to the vulva |
| IA—Tumor size ≤ 2 cm and stromal invasion ≤ 1 mm * | |
| IB—Tumor size > 2 cm or stromal invasion > 1 mm * | |
| II | Tumor of any size with extension to lower one-third of the urethra, lower one-third of the vagina, lower one-third of the anus with negative nodes |
| III | Tumor of any size with extension to the upper part of adjacent perineal structures or with any number of nonfixed, nonulcerated lymph nodes |
| IIIA—Tumor of any size with disease extension to upper two-thirds of the urethra, upper two-thirds of the vagina, bladder mucosa, rectal mucosa, or regional lymph node metastases ≤ 5 mm | |
| IIIB—Regional ** lymph node metastases > 5 mm | |
| IIIC—Regional ** lymph node metastases with extracapsular spread | |
| IV | Tumor of any size fixed to the bone or fixed, ulcerated lymph node metastases, or distant metastases |
| IVA—Disease fixed to the pelvic bone or fixed or ulcerated regional ** lymph node metastases | |
| IVB—Distant metastases |
| FIGO Staging System | II |
|---|---|
| 2009 | Tumor of any size with extension to the adjacent perineal structures (lower one-third of the urethra, lower one-third of vagina, anus) with no lymph node involvement |
| 2021 | Tumor of any size with extension to lower one-third of the urethra, lower one-third of the vagina, lower one-third of the anus with no lymph node involvement |
| FIGO Staging System | III | IIIA | IIIB | IIIC |
|---|---|---|---|---|
| 2009 | Tumor of any size, with/without extension to adjacent perineal structures (lower third of urethra, the lower third of vagina, anus) with positive inguinofemoral lymph nodes | With one lymph node metastases (≥5 mm) or with 1–2 lymph node metastases (<5 mm) | With two or more lymph node metastases (≥5 mm) or with three or more lymph node metastases (<5 mm) | With positive nodes with extracapsular spread |
| 2021 | Tumor of any size with extension to upper parts of adjacent perineal structures or with any number of nonfixed and nonulcerated lymph nodes | Tumor of any size with disease extension to upper two-thirds of the urethra, upper two-thirds of the vagina, bladder mucosa, or regional lymph node metastases ≤ 5 mm | Regional lymph node (inguinofemoral) metastases >5 mm | Regional lymph node (inguinofemoral) metastases with extracapsular spread |
| FIGO Staging System | IV | IVA | IVB |
|---|---|---|---|
| 2009 | Tumor invades adjacent structures or fixed and ulcerated lymph nodes or distant metastases | Upper urethral and/or vaginal mucosa, bladder mucosa, rectal mucosa, or is fixed to the pelvic bone Fixed or ulcerated inguinofemoral lymph nodes | Any distant metastases, including pelvic lymph nodes |
| 2021 | Tumor of any size fixed to the bone, or fixed and ulcerated lymph node metastases or distant metastases | Disease fixed to the pelvic bone or fixed or ulcerated regional (inguinofemoral) lymph node metastases | Distant metastases |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virarkar, M.; Vulasala, S.S.; Daoud, T.; Javadi, S.; Lall, C.; Bhosale, P. Vulvar Cancer: 2021 Revised FIGO Staging System and the Role of Imaging. Cancers 2022, 14, 2264. https://doi.org/10.3390/cancers14092264
Virarkar M, Vulasala SS, Daoud T, Javadi S, Lall C, Bhosale P. Vulvar Cancer: 2021 Revised FIGO Staging System and the Role of Imaging. Cancers. 2022; 14(9):2264. https://doi.org/10.3390/cancers14092264
Chicago/Turabian StyleVirarkar, Mayur, Sai Swarupa Vulasala, Taher Daoud, Sanaz Javadi, Chandana Lall, and Priya Bhosale. 2022. "Vulvar Cancer: 2021 Revised FIGO Staging System and the Role of Imaging" Cancers 14, no. 9: 2264. https://doi.org/10.3390/cancers14092264